 Anatomy, Shoulder and Upper Limb, Hand Volar Arch Arteries
Anatomy, Shoulder and Upper Limb, Hand Volar Arch Arteries
Introduction
Blood supply to the volar surface of the hand arises from the radial and ulnar arteries (see Image. Palmar Arterial Anatomy). After crossing the wrist and entering the palm, these vessels anastomose to form the superficial and deep volar arches. The arches and their branches create an extensive arterial network that delivers oxygenated blood to all musculoskeletal structures of the hand and digits.[1]
The wide range of hand functions—grasping, force application, and complex multidirectional movements—requires reliable perfusion across all tissue planes. Extensive collateral pathways preserve arterial flow during mechanical stress, positional changes, or functional loading.[2]
The volar arterial system holds clinical importance because disruptions in either the radial or ulnar artery can lead to digital ischemia when collateral pathways are insufficient. Surgical procedures involving these arteries demand precise appreciation of arterial configuration to minimize neurovascular complications. A detailed understanding of arterial anatomy and physiology in this region enables accurate evaluation of collateral flow, early recognition of vascular variants, and informed selection of operative approaches.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The arteries of the volar surface of the hand comprise the superficial and deep volar arches. These arches and their branches establish an extensive collateral network that delivers oxygenated blood to all regions of the hand and digits.[3]
The superficial volar arch serves as the dominant vascular structure of the palm. This arch arises primarily from the ulnar artery with additional contribution from the superficial branch of the radial artery (see Image. Forearm Artery Dissection). The ulnar artery enters the hand superficial to the flexor retinaculum through the ulnar (Guyon) canal and terminates in the superficial volar arch, where an anastomosis forms with the superficial radial branch (see Image. Guyon Canal Zones). The superficial radial branch courses superficial to the flexor retinaculum to complete the arch. The superficial volar arch lies superficial to the flexor tendons and deep to the palmar aponeurosis, extending from the 1st webspace to the hook of the hamate and reaching a more distal level than the deep volar arch.
Branches of the superficial volar arch include 3 common palmar digital arteries that traverse the palm between the finger webs. Each common palmar digital artery divides at the webspace into 2 proper palmar digital arteries that supply the opposing sides of digits 2, 3, 4, as well as the lateral aspect of the 5th digit. The medial surface of the 5th digit receives arterial supply from an additional branch of the superficial volar arch.[4]
The deep volar arch forms from the dorsal radial artery and the deep palmar branch of the ulnar artery. Before reaching the flexor retinaculum, the radial artery gives off the superficial branch of the radial artery and then continues as the dorsal radial artery. The dorsal radial artery continues its course by curving around to enter the dorsal aspect of the hand while passing the scaphoid and trapezium through the floor of the anatomical snuffbox.[5] From there, the blood vessel passes between the 2 heads of the 1st dorsal interosseous muscle to reenter the palmar aspect of the hand.[6] On the palmar side, the radial artery turns medially and terminates in the deep volar arch, where it anastomoses with the deep palmar branch of the ulnar artery.
The deep palmar branch of the ulnar artery completes the deep volar arch. The deep volar arch is localized deep to the flexor tendons of the hand. This arterial arch lies between the flexor tendons and the metacarpal bones and is proximal to the superficial volar arch.
Arising from the deep volar arch are 3 palmar metacarpal arteries that anastomose with the common palmar digital arteries from the superficial volar arch. The deep volar arch also provides arterial supply to the thumb and the lateral side of the index finger. The radial artery gives off 2 branches—the princeps pollicis and radialis indicis arteries—as it turns onto the palmar aspect of the hand. The princeps pollicis artery runs along the palmar aspect of the 1st metacarpal and bifurcates distally into 2 palmar digital arteries that supply each side of the thumb. The radialis indicis artery courses along the 1st dorsal interosseous muscle to supply the lateral side of the index finger.[7]
Embryology
The current theory of embryonic development of the hand arterial pattern proposes a combined process of vasculogenesis and remodeling. At stage 12, an initial capillary network arises from the dorsal aorta and expands into the developing limb bud. Simultaneously, the proximal segments of this network begin to enlarge, and arterial walls start differentiating by stage 13.
From stages 13 to 21, differentiation proceeds in a proximal-to-distal sequence, beginning with the ulnar, interosseous, and median arteries.[8] The radial artery develops at stage 18 and reaches its final differentiated morphology by stage 21. By this stage, the definitive arterial pattern of the hand, including the palmar arches, is established.
The precise mechanisms guiding arterial development are incompletely understood. One hypothesis emphasizes the roles of oxygenation, nutrient supply, and hemodynamic forces. An alternative hypothesis proposes a genetic component in determining the arterial pattern.[9]
Blood Supply and Lymphatics
The superficial and deep volar arterial arches are each accompanied by paired venae comitantes, forming the superficial and deep palmar venous arches. These veins drain deoxygenated blood from the hand and fingers along pathways corresponding to the branches of the arterial arches. The common palmar digital veins receive blood from the proper palmar digital veins and empty into the superficial palmar venous arch, which ultimately drains into the radial vein. The palmar metacarpal veins, collecting blood from the metacarpal region, drain into the deep palmar venous arch. Certain branches of the palmar metacarpal veins communicate with the dorsal metacarpal veins and terminate in the radial veins, as well as the superficial veins on the dorsum of the wrist.
Lymphatic drainage of the hand similarly divides into superficial and deep systems. Superficial lymphatic vessels course adjacent to major superficial veins, whereas deep lymphatic vessels follow the trajectories of the principal deep veins.[10]
Nerves
Sympathetic fibers provide innervation to the arteries of the hand, with the 2nd and 3rd thoracic ganglia serving as the primary sources of sympathetic input.[11] Arterioles constrict to reduce blood flow to the superficial tissues and distal phalanges in response to cold exposure, thereby minimizing heat loss.
Muscles
The hand contains an extensive network of collateral vessels, ensuring delivery of oxygenated blood to all muscular structures of the hand and digits.[12] Injury to a single vessel does not necessarily compromise perfusion, as anastomotic connections maintain blood flow. This collateral network preserves oxygen delivery to regions at risk of ischemia following vascular injury.
Physiologic Variants
The arteries of the hand form a highly branched and anastomosed network, resulting in numerous anatomic variations of arterial patterns. These variants are classified as either complete or incomplete, affecting the superficial or deep arches.[13] An arch is considered complete when an anastomosis exists between its contributing vessels, and incomplete when such a connection is absent. Advances in hand microsurgery have increased the clinical significance of understanding these vascular variations. A recent meta-analysis reported a complete superficial volar arch in 81.3% of cases. Seven distinct types of complete superficial volar arches and 5 types of incomplete superficial volar arches have been documented. The deep volar arch exhibits less variability, with a complete arch observed in 95.2% of cases.[14]
Surgical Considerations
The radial artery is frequently utilized for blood gas sampling, arterial line placement, catheterization, and grafting in coronary revascularization. Anastomoses between the ulnar and radial arteries, forming the deep and superficial volar arches, generally preserve hand perfusion if an artery becomes occluded during such procedures. Complications, including distal ischemia and limb compromise, can occur when collateral circulation is insufficient to maintain adequate flow.[15] Therefore, assessment of collateral blood flow is essential to ensure sufficient perfusion following intervention. The Allen test and modified Allen test provide reliable methods for evaluating collateral circulation prior to procedures.[16][17]
Clinical Significance
The arterial supply of the hand and fingers is critical for maintaining tissue viability. Collateral circulation typically preserves perfusion if the ulnar or radial artery is occluded or damaged. However, patients with anatomic vascular variations may develop digital ischemia and limb compromise when collateral flow is insufficient. Awareness and documentation of significant vascular variants are essential to prevent adverse outcomes.
Raynaud syndrome is an idiopathic disorder characterized by intermittent digital ischemia, frequently accompanied by paresthesia and pain. Episodes are usually triggered by cold exposure or emotional stress.[18] Cervicodorsal presynaptic sympathectomy provides an effective surgical treatment, involving excision of a segment of the sympathetic chain to dilate digital arteries.
Other Issues
Traumatic hand injuries frequently involve the common digital arteries. Surgical repair of transected common digital arteries may be achieved by mobilizing the superficial palmar arch distally to reestablish arterial continuity and restore perfusion.[19]
Media
(Click Image to Enlarge)
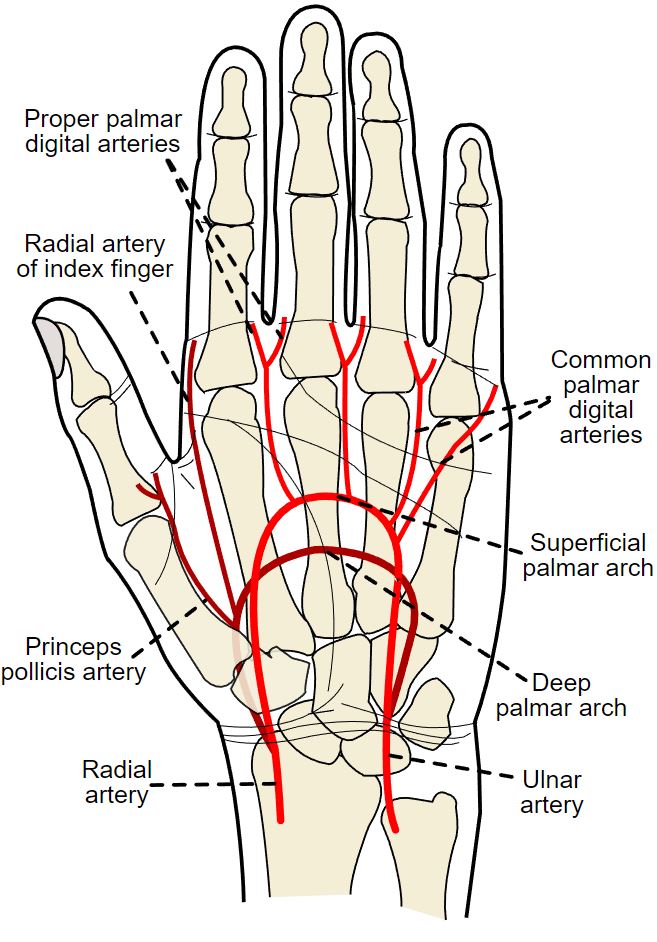
Palmar Arterial Anatomy. The diagram illustrates the radial and ulnar arteries, their contributions to the palmar arches, and the digital branches within the hand.
Rhcastilhos, Public Domain, via Wikimedia Commons
{kind=link}
(Click Image to Enlarge)
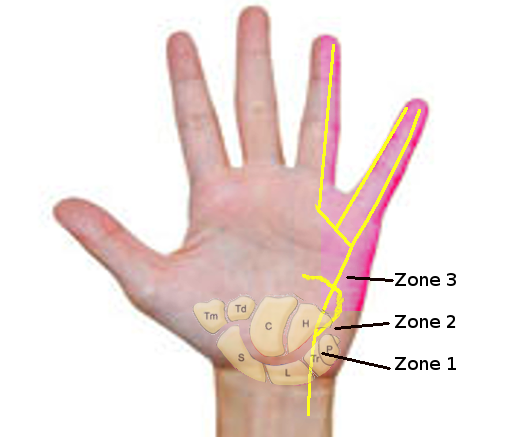
Guyon Canal Zones. This illustration shows the zones of ulnar nerve compression in the Guyon canal. Zone 1 represents the area proximal to the ulnar nerve bifurcation into sensory and motor branches. Zone 2 encompasses the area of the deep motor branch of the ulnar nerve. Zone 3 represents the area of the superficial sensory branch.
Contributed by S Bhimji, MD
(Click Image to Enlarge)
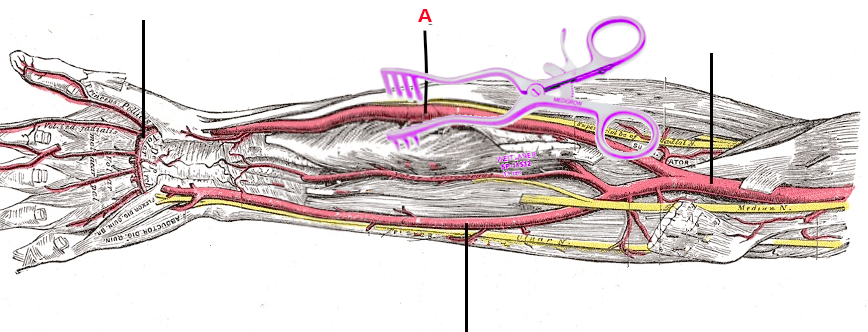
Forearm Artery Dissection. This image displays an anatomical dissection of the forearm, highlighting the radial artery at point A, the course of the median nerve, and the surrounding flexor muscles. The pointers in other locations, from proximal to distal, indicate the brachial, ulnar, and superficial palmar arteries.
Contributed by S Bhimji, MD
References
Tan RES, Lahiri A. Vascular Anatomy of the Hand in Relation to Flaps. Hand clinics. 2020 Feb:36(1):1-8. doi: 10.1016/j.hcl.2019.08.001. Epub [PubMed PMID: 31757342]
Brzezinski M, Luisetti T, London MJ. Radial artery cannulation: a comprehensive review of recent anatomic and physiologic investigations. Anesthesia and analgesia. 2009 Dec:109(6):1763-81. doi: 10.1213/ANE.0b013e3181bbd416. Epub [PubMed PMID: 19923502]
Tian R, Tai H, Chen J, Zhang Y, Zhang S, Li J, Li X, Linghu Y, Li Y. Morphological study of the superficial palmar arch and its significance in clinical operation. Folia morphologica. 2024:83(4):830-844. doi: 10.5603/fm.98591. Epub 2024 Apr 3 [PubMed PMID: 38567937]
Gnanasekaran D, Veeramani R. Newer insights in the anatomy of superficial palmar arch. Surgical and radiologic anatomy : SRA. 2019 Jul:41(7):791-799. doi: 10.1007/s00276-019-02223-w. Epub 2019 Mar 28 [PubMed PMID: 30923841]
Hallett Reid S, Jozsa F, Ashurst JV. Anatomy, Shoulder and Upper Limb: Hand Anatomical Snuff Box. StatPearls. 2025 Jan:(): [PubMed PMID: 29489241]
Valenzuela M, Bordoni B. Anatomy, Shoulder and Upper Limb, Hand Dorsal Interossei Muscle. StatPearls. 2025 Jan:(): [PubMed PMID: 30725607]
Singh S, Lazarus L, De Gama BZ, Satyapal KS. An anatomical investigation of the superficial and deep palmar arches. Folia morphologica. 2017:76(2):219-225. doi: 10.5603/FM.a2016.0050. Epub 2016 Sep 26 [PubMed PMID: 27665957]
Cole P, Kaufman Y, Hatef DA, Hollier LH Jr. Embryology of the hand and upper extremity. The Journal of craniofacial surgery. 2009 Jul:20(4):992-5. doi: 10.1097/SCS.0b013e3181abb18e. Epub [PubMed PMID: 19553860]
Rodríguez-Niedenführ M, Burton GJ, Deu J, Sañudo JR. Development of the arterial pattern in the upper limb of staged human embryos: normal development and anatomic variations. Journal of anatomy. 2001 Oct:199(Pt 4):407-17 [PubMed PMID: 11693301]
Valenzuela M, Bordoni B. Anatomy, Shoulder and Upper Limb, Hand Palmar Interosseous Muscle. StatPearls. 2025 Jan:(): [PubMed PMID: 30725850]
Coveliers HM, Hoexum F, Nederhoed JH, Wisselink W, Rauwerda JA. Thoracic sympathectomy for digital ischemia: a summary of evidence. Journal of vascular surgery. 2011 Jul:54(1):273-7. doi: 10.1016/j.jvs.2011.01.069. Epub 2011 Jun 8 [PubMed PMID: 21652164]
Picasso R, Zaottini F, Pistoia F, Perez MM, Macciò M, Bianco D, Rinaldi S, Pansecchi M, Rossi G, Tovt L, Martinoli C. Ultrasound of the palmar aspect of the hand: normal anatomy and clinical applications of intrinsic muscles imaging. Journal of ultrasonography. 2023 Sep:23(94):e122-e130. doi: 10.15557/jou.2023.0021. Epub 2023 Sep 11 [PubMed PMID: 37732107]
Dawani P, Mahajan A, Vasudeva N, Mishra S. Variations in the Pattern of the Deep Palmar Arch of the Hand and Its Surgical Importance. Cureus. 2022 Jan:14(1):e20873. doi: 10.7759/cureus.20873. Epub 2022 Jan 2 [PubMed PMID: 35145780]
Zarzecki MP, Popieluszko P, Zayachkowski A, Pękala PA, Henry BM, Tomaszewski KA. The surgical anatomy of the superficial and deep palmar arches: A Meta-analysis. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2018 Nov:71(11):1577-1592. doi: 10.1016/j.bjps.2018.08.014. Epub 2018 Aug 24 [PubMed PMID: 30245020]
Level 1 (high-level) evidenceHabib J, Baetz L, Satiani B. Assessment of collateral circulation to the hand prior to radial artery harvest. Vascular medicine (London, England). 2012 Oct:17(5):352-61. doi: 10.1177/1358863X12451514. Epub 2012 Jul 19 [PubMed PMID: 22814998]
Beutel BG, Worley C, Zisquit J, Nedeff N. Allen Test. StatPearls. 2025 Jan:(): [PubMed PMID: 29939593]
Moon J, Lee GH, Park TJ, Ki SH. Is the Modified Allen's Test a Useful Tool for Evaluating the Vascular Dominance of the Forearm? Journal of Korean medical science. 2025 Sep 15:40(36):e230. doi: 10.3346/jkms.2025.40.e230. Epub 2025 Sep 15 [PubMed PMID: 40955611]
Nawaz I, Nawaz Y, Nawaz E, Manan MR, Mahmood A. Raynaud's Phenomenon: Reviewing the Pathophysiology and Management Strategies. Cureus. 2022 Jan:14(1):e21681. doi: 10.7759/cureus.21681. Epub 2022 Jan 28 [PubMed PMID: 35242466]
Korambayil PM. Use of superficial palmar arch for bridging the gap in digital revascularisation. Indian journal of plastic surgery : official publication of the Association of Plastic Surgeons of India. 2011 Sep:44(3):511-6. doi: 10.4103/0970-0358.90844. Epub [PubMed PMID: 22279293]
Level 3 (low-level) evidence