 Fetal Heart Rate Tracing: Assessment and Clinical Interpretation
Fetal Heart Rate Tracing: Assessment and Clinical Interpretation
Introduction
Adverse neonatal outcomes result from a complex interplay of intrapartum events, antepartum complications, placental function or dysfunction, and uterine perfusion.[1] Electronic fetal monitoring, or cardiotocography, is widely utilized during labor or as a component of antenatal fetal surveillance to assess fetal status and to prevent adverse neonatal outcomes, eg, fetal asphyxia or cerebral palsy. Unfortunately, a high intraobserver and interobserver variability exists when interpreting fetal heart rate tracings. In one study, obstetricians interpreted fetal heart rate tracings similarly in only 29% of cases.[2]
Electronic fetal monitoring can be used alone or in conjunction with real-time ultrasonography and monitoring maternal perception of fetal movements to detect potential uteroplacental compromise. Therefore, additional indications for electronic fetal monitoring other than labor can include maternal (eg, chronic hypertension, diabetes, and obesity), fetal (eg, intrauterine growth restriction, decreased fetal movement, and multiple gestations), or obstetric (eg, history of intrauterine fetal demise and postterm pregnancy) factors.[3] Please see StatPearls' companion resource, "Antenatal Fetal Surveillance," for further information.
In 2008, terminology and nomenclature for electronic fetal monitoring were standardized at a workshop sponsored by the American College of Obstetricians and Gynecologists, the Society for Maternal-Fetal Medicine, and the Eunice Kennedy Shriver National Institute of Child Health and Human Development (see Image. Fetal Heart Rate Terminology).[4] This workshop divided fetal heart tracings into 3 categories based on the risk of fetal acidemia. During labor, if fetal heart tracings are abnormal or concerning, various interventions are available to potentially alleviate the underlying causes and allow the patient to continue toward a vaginal delivery.
Fetal Heart Rate Terminology
Baseline fetal heart rate
The baseline fetal heart rate is the mean fetal heart rate over 10 minutes, present for at least 2 minutes within that 10 minutes, rounded to increments of 5 beats per minute (bpm). Additional definitions that guide interpretation include:
- The baseline fetal heart rate excludes episodic or period changes, periods where variability is marked, and segments where the baseline differs by 25 beats per minute or more
- A normal baseline is 110 to 160 beats per minute
- A baseline over 160 bpm is considered tachycardia
- A baseline less than 110 bpm is considered bradycardia [5]
Baseline variability
Baseline variability is the fluctuations in baseline fetal heart rate, irregular in amplitude and frequency, quantified visually in bpm from peak to trough. The following definitions are used to characterize baseline variability:
- Absent: amplitude range is undetectable
- Minimal: detectable, but the amplitude range is 5 or fewer bpm
- Moderate: "normal" range of amplitude of 6 to 25 bpm
- Marked: range of amplitude is greater than 25 bpm [5]
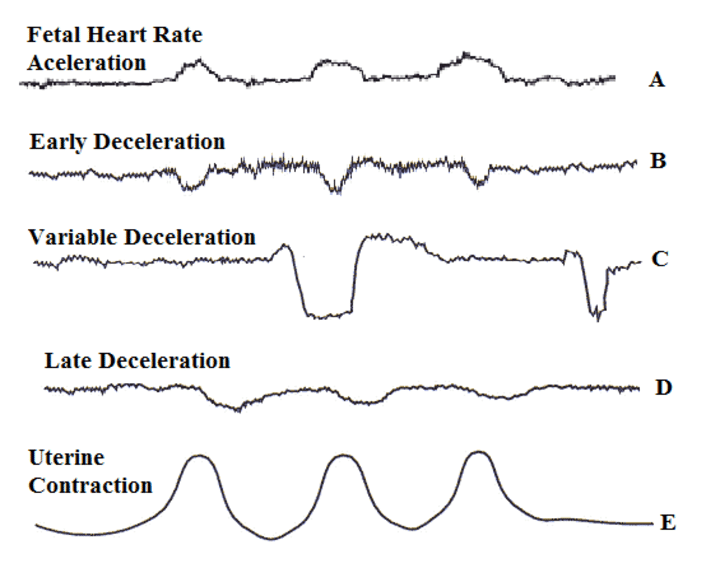
Fetal heart rate acceleration
An acceleration is an abrupt, visually apparent increase in the fetal heart rate, with an onset-to-peak duration of less than 30 seconds. The following criteria define accelerations:
- At and after 32 weeks of gestational age, the peak must occur at 15 beats per minute or more above baseline and last for 15 seconds or more (but less than 2 minutes) from onset to return to baseline.
- Before 32 weeks of gestational age, the peak must occur at 10 beats per minute or more above baseline and last for 10 seconds or more (but less than 2 minutes) from onset to return to baseline.
- An acceleration is considered prolonged if it lasts for 2 minutes or more, but less than 10 minutes.
- An acceleration that lasts for 10 minutes or more is considered a change in baseline.[5]
Early deceleration
An early deceleration is a gradual decrease below, and return to, the fetal heart rate baseline that is visually apparent, usually symmetrical, and is associated with a uterine contraction. The following criteria define early decelerations:
- Early decelerations are gradual, with the decrease in fetal heart rate from onset to nadir taking 30 seconds or more.
- The depth of an early deceleration is calculated from the onset to nadir.
- The nadir of an early deceleration occurs at the same time as the peak of the associated uterine contraction.
- Usually, the onset, nadir, and recovery of an early deceleration coincide with the beginning, peak, and end of the associated contraction, respectively.[5]
Late deceleration
A late deceleration is similar to an early deceleration in that this tracing shows a gradual decrease below, and return to, the fetal heart rate baseline that is visually apparent, usually symmetrical, and is associated with a uterine contraction. However, a late deceleration differs in its timing in relation to the associated uterine contraction. The following criteria define late decelerations:
- Late decelerations are gradual, with the decrease in fetal heart rate from onset to nadir taking 30 seconds or more.
- The depth of a late deceleration is calculated from onset to nadir.
- The timing of a late deceleration is delayed, and the deceleration's nadir occurs after the peak of the associated uterine contraction.
- Usually, the onset, nadir, and recovery of a late deceleration occur after the beginning, peak, and end of the associated uterine contraction, respectively.[5]
Variable deceleration
A variable deceleration is a visually apparent, abrupt decrease in fetal heart rate (see Image. Variable Decelerations) and is defined by the following criteria:
- A variable deceleration is abrupt, with the onset-to-nadir interval of less than 30 seconds.
- The depth of a variable deceleration is calculated from onset to nadir.
- The decrease of the fetal heart rate from baseline is at least 15 beats per minute and lasts at least 15 seconds (but less than 2 minutes).
- A variable deceleration can be periodic or episodic.
- When associated with contractions, the onset, depth, and duration of variable decelerations typically vary with successive contractions.[5]
Additional terminology
The following terms are used to characterize fetal heart rate tracings:
- Prolonged deceleration: a visually apparent fetal heart rate decrease from baseline that lasts 2 minutes or longer (but less than 10 minutes)
- Decrease from baseline is at least 15 beats per minute
- If the deceleration lasts 10 minutes or longer, it is considered a change in baseline
- Sinusoidal pattern: smooth, visually apparent, sine wave-like undulation in the fetal heart rate baseline
- The pattern persists for 20 minutes or more
- Cycle frequency is 3-5 per minute
- Normal uterine activity: 5 or fewer uterine contractions in 10 minutes when averaged over a period of 30 minutes
- Tachysystole: more than 5 uterine contractions in 10 minutes when averaged over a period of 30 minutes; presence or absence of fetal heart rate decelerations should be documented
- Recurrent: decelerations present with 50% of uterine contractions
- Periodic: associated with a uterine contraction
- Episodic: not associated with a uterine contraction [5]
Categorization of Fetal Heart Rate Tracings
Fetal heart rate tracings are categorized into the following 3 tiers:
- Category I: fetal acid/base status likely normal
- Baseline is normal (110-160 beats per minute)
- Baseline variability is moderate
- No late or variable decelerations
- Early decelerations can be absent or present
- Accelerations can be absent or present [5]
- Category II: any tracings that are not category I or category III; association with fetal acidemia is uncertain
- Baseline can be tachycardic or bradycardic without absent variability
- Variability can be minimal or marked, or absent without recurrent decelerations
- Accelerations are absent despite attempts to induce with fetal stimulation
- Periodic or episodic decelerations that do not qualify as category III
- Recurrent variable decelerations, but variability is minimal or moderate
- Recurrent late decelerations, but variability is moderate
- Variable decelerations have other characteristics (overshoots, shoulders, slow return to baseline)
- Prolonged decelerations lasting more than 2 minutes but less than 10 minutes [5]
- Category III: associated with fetal acidemia
- Baseline variability is absent, and one of the following is present:
- recurrent late decelerations
- recurrent variable decelerations
- bradycardia
- Sinusoidal pattern [5]
- Baseline variability is absent, and one of the following is present:
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
In general, the fetus is well-adapted to life inside the uterus. The structure of fetal hemoglobin differs from that of adult hemoglobin. The fetus exhibits a more pronounced Bohr effect, allowing a greater amount of oxygen to bind and unbind in response to oxygen tension in the fetal circulation. The fetus also has high basal blood flow to its organs and vascular shunts that preferentially deliver oxygenated blood to the heart and brain. Because of these adaptations, the fetus has a surplus of oxygen, which, in turn, allows it to maintain oxidative metabolism even during mild or moderate reductions in oxygen supply, eg, during uterine contractions.[6][7]
In utero, the fetus depends on several factors to maintain oxygenation. The first is maternal respiration and circulation. Secondly, the placenta plays a key role. Both perfusion of the placenta and gas exchange across the placenta are important for fetal oxygenation. Lastly, umbilical and fetal circulations are key to fetal oxygenation. Decreased oxygen concentrations in fetal arterial blood (hypoxemia) and in fetal tissues (hypoxia) can occur if any of these factors are disrupted. Some degree of hypoxemia is expected during labor. However, each fetus varies in their ability to cope with the intensity, duration, and repetition of events that impact oxygenation. This ultimately determines the severity of any resultant hypoxia.[8]
When hypoxia occurs, anaerobic metabolism can maintain energy production in fetal cells for a limited time. This process, however, produces much less energy and results in lactic acid accumulation within fetal cells and its dispersal through the fetal circulation. Metabolic acidemia is the resultant increase in hydrogen ions in the fetal circulation. Metabolic acidemia closely parallels hydrogen ion concentration; thus, the terms "metabolic acidosis" and "metabolic acidemia" are often used synonymously. As hydrogen ions are buffered by circulating bases, eg, bicarbonate, these buffering agents are depleted. Depletion of buffers, represented by increasing base deficit, is a sign of the fetus's growing inability to neutralize circulating hydrogen ions. Continued hydrogen ion production ultimately leads to disruptions in enzyme systems in cells and tissue injury.[8]
The fetal cardioregulatory center (CRC) is responsible for maintaining homeostasis and ensuring optimum oxygen delivery. The CRC is located in the medulla oblongata and determines fetal heart rate baseline, pattern, and variability. It receives input from various afferent nerves that have receptors in the peripheral nervous system. These include baroreceptors in the aortic arch and bifurcation of the carotid. They detect stretch from changes in fetal blood pressure. Increased blood pressure leads to decreased heart rate, and vice versa. Chemoreceptors are sensitive to pH and oxygen saturation. Central chemoreceptors are present in the medulla oblongata, and peripheral chemoreceptors are located in the carotid bodies and the aortic arch. Central chemoreceptor stimulation leads to increased sympathetic output, hypertension, and tachycardia. On the other hand, peripheral chemoreceptor stimulation results in parasympathetic output and the opposite effects. The CRC also receives input from acoustic, temperature, and vibratory receptors.[9]
Baseline Fetal Heart Rate
Fetal heart rate baseline is determined by parasympathetic output, primarily through the vagus nerve, as well as sympathetic output. The parasympathetic system matures as the fetus matures. This results in a higher baseline heart rate early in pregnancy, which then falls as the pregnancy progresses.[9]
Tachycardia is usually a physiologic response to increased metabolic demand, decreased parasympathetic tone, or increased sympathetic tone. Tachycardia can be a sign of fever, infection, or low volume status. Additionally, tachycardia can represent an arrhythmia. If fetal tachycardia is a result of oxygen debt, it usually manifests late in the process. Central chemoreceptors detect hypoxemia and increase heart rate to maintain cerebral perfusion.[9]
Bradycardia can be seen in multiple physiologic and pathologic situations. For example, bradycardia can be seen in fetuses with heart block. "Terminal bradycardia" describes a low fetal heart rate just before delivery. Terminal bradycardia could be caused by prolonged stimulation of the vagus nerve due to rapid fetal descent and resultant head compression. Fetal bradycardia, in a more worrisome scenario, can represent prolonged hypoxia and acidosis. If initial physiologic responses, eg, tachycardia, do not meet the fetus's oxygen requirements, cardiac hypoxia results. This, in turn, leads to myocardial depression and subsequent bradycardia.[9]
Uterine Contractions
Contractions cause compression of maternal blood vessels coursing within the muscle of the uterus (myometrium), thus decreasing perfusion across the placenta. In spontaneous labor, up to 90 seconds are believed to be required after a contraction for fetal oxygenation to be restored.[8] Thus, if excessive uterine contractions are suspected of impacting the fetus negatively, interventions may be needed.
Early Decelerations
Several theories have been posited regarding the physiology of early decelerations. Most commonly, early decelerations are thought to represent an autonomic response to the changes in cerebral blood flow and intracranial pressure that occur during a contraction. Classical teaching holds that head compression stimulates the vagus nerve, triggering a parasympathetic response and the characteristic slowing of the fetal heart rate.[10] Alternatively, early decelerations may be mediated through the Cushing response. This is a decrease in the heart rate due to intracranial pressure so high that the cerebral blood flow is reduced.[9] Yet another theory posits that early decelerations are a response to pressure by scalp receptors.[9]
Despite the uncertainty regarding their exact etiology, early decelerations are considered benign. As such, no interventions are usually indicated if early decelerations are seen on a fetal heart tracing. However, given the possibility that they are not entirely benign, care must be taken to monitor the clinical situation for other signs warranting concern. Care must also be taken to distinguish early decelerations from late decelerations, as they can appear similar to inexperienced observers.
Variable Decelerations
Variable decelerations can be seen resulting from fetal movement if the fetus is premature.[11] In the term fetus, variable decelerations result from vagus nerve-mediated parasympathetic effects on the heart. Several theories regarding the pathway that leads to this vagal stimulation have been proposed.
Traditionally, variable decelerations are attributable to transient compression of the umbilical cord. During a contraction, the umbilical vein may initially be the only vessel to undergo compression, leading to decreased fetal blood return and subsequent baroreceptor-mediated acceleration. This activity appears to create a “shoulder” on the tracing.[12] Complete umbilical cord occlusion increases fetal arterial blood pressure, and the resulting baroreceptor-triggered activation of the vagus nerve leads to rapid deceleration of fetal heart rate. When this sequence reverses with the resolution of the contraction, the variable deceleration also resolves.[13]
Alternatively, variable decelerations may result from chemoreceptor responses to hypoxia. The physiology of the uterus and placenta is such that, when the uterus contracts, uteroplacental perfusion is impaired. If the resulting hypoxemia is mild, the fetus may switch to quiet sleep or reduce movement and breathing to decrease oxygen consumption. However, at a certain threshold of hypoxemia, the peripheral chemoreflex is triggered. This reflex leads to the rapid increase in sympathetic and parasympathetic activity, which in turn promotes the centralization of perfusion to critical organs, hypertension, and peripheral vasoconstriction. Because the increased parasympathetic activity overrides the sympathetic activity in the heart, rapid deceleration is triggered.[6]
Late Deceleration
Late decelerations are associated with reduced fetal oxygenation. While the fetus usually tolerates the brief reduction in oxygenation that occurs during uterine contractions, situations occur in which the fetus may not be able to adapt as well. If oxygenation is already borderline or low, further loss of oxygenation may trigger vasoconstriction to shunt blood and oxygen to vital organs. Baroreceptors detect this increase in fetal blood pressure and lower the heart rate, usually via the vagus nerve.[9]
When associated with true placental insufficiency, interventions are indicated. This is especially true when other nonreassuring findings are present. Care must be taken to distinguish true late decelerations from late variable decelerations. While either may indicate the need for action, the resuscitation methods for each type of deceleration will vary.
Prolonged Deceleration
The prolonged deceleration is most likely due to a sudden, sustained reduction in oxygen delivery. Initially, the physiologic responses are likely vagal, as seen with late or variable decelerations. As impairment of gas exchange continues, direct myocardial depression may manifest in a prolonged deceleration. Experts have speculated that the decrease in heart rate is an attempt to conserve oxygen when the debt is severe.[9]
Epidemiology
Electronic fetal monitoring is utilized in approximately 85% of live births in the United States, making electronic fetal monitoring the most common procedure in obstetrics.[1] This frequency has increased since 1980, when electronic fetal monitoring was used in only about 45% of women in labor.[1] Intermittent, variable decelerations, defined as decelerations occurring in fewer than half of contractions, are the most common fetal heart rate abnormality in labor.[5] Intermittent variable decelerations are generally not associated with adverse perinatal outcomes, and they often do not require treatment. Recurrent variable decelerations, where the decelerations occur with 50% or more of the contractions, are less common and more concerning. Late decelerations are thought to represent poor oxygenation and are also concerning.
Pathophysiology
Fetal heart rate tracings reflect the response of the fetal cardioregulatory center, located in the medulla oblongata, to input from chemoreceptors and baroreceptors. These detect changes in blood pressure, pH, and oxygen saturation. The CRC responds with parasympathetic output via the vagus nerve and sympathetic release of catecholamines. Various inputs, eg, fever, head compression, or umbilical cord compression, can trigger physiologic responses that are reflected in the fetal heart tracing as changes in baseline or decelerations.[9]
History and Physical
Clinical History
The patient's history is important to consider when interpreting fetal monitoring.
Gestational age
The gestational age of the fetus can impact the fetal heart tracing. This includes aspects, eg, the expected baseline, the presence and definition of accelerations, and the presence/significance of variable decelerations. Postterm pregnancy is associated with worsening placental function, which can manifest as fetal heart rate decelerations during labor.
Maternal history
Many maternal health problems can impact the fetal heart tracing. Maternal systemic illness may lead to fetal tachycardia. Maternal systemic lupus can lead to antibodies crossing the placenta to the fetus, with a resultant fetal bradycardia from complete atrioventricular block. Use of buprenorphine or methadone for substance use disorder may impact the fetal heart rate variability.
Factors, eg, maternal smoking, uncontrolled hypertension, diabetes, use of cocaine or amphetamines, and others, can lead to placental damage. This damage can result in poor fetal growth, which impacts fetal tolerance of labor and may manifest as abnormalities in the heart tracing. Placental damage can also lead to decreased amniotic fluid volume, resulting in variable decelerations due to umbilical cord compression. Additionally, maternal hyperthyroidism may lead to fetal tachycardia.
Clinicians should elicit any symptoms consistent with rupture of membranes (eg, leaking fluid and constant wetness) as low amniotic fluid may contribute to decelerations. Rupture of membranes may also lead to intra-amniotic infection if diagnosis or delivery is delayed, leading to fever and decreased variability. Other sources of infection that may lead to fetal tachycardia may present with a systemic illness that can be elicited from the history.
Uncontrolled diabetes can also lead to increased amniotic fluid (polyhydramnios) when the amniotic sac ruptures, before or during labor, and umbilical cord prolapse can occur. Fetal bradycardia or variable decelerations may be seen in these cases. A history of polyhydramnios, breech presentation, advanced cervical dilation, or high fetal station before the rupture of membranes may raise suspicion for a prolapsed umbilical cord.
Prior uterine surgeries are relevant to labor, including previous cesarean section (low transverse or classical) and myomectomy. Deep, recurrent variable decelerations may precede bradycardia in cases of uterine rupture. In a patient who presents in labor with an abnormal fetal heart rate tracing, a history of a prior classical cesarean section or previous uterine rupture would warrant immediate evaluation.
Fetal conditions
Known fetal structural defects can lead to heart tracing abnormalities, eg, a lower baseline. Fetal renal or urinary tract anomalies can lead to amniotic fluid abnormalities. Low amniotic fluid can be reflected in the fetal heart tracing as variable decelerations. In some instances, the presence of a nuchal cord can be identified on ultrasound. A nuchal cord may increase the risk of umbilical cord compression during uterine contractions. Monoamniotic twins are at risk of umbilical cord entanglement, which may manifest as fetal heart rate decelerations.
Physical Examination
During prenatal care, the initial exam of a pregnant patient must include identification of the number of fetuses. If multiple fetuses are present, identification of chorionicity and amnionicity is essential. When fetuses share an amniotic sac, umbilical cord entanglement can occur.
Physical exam intrapartum should include an examination of the cervix for dilation, station, and presence of a prolapsed umbilical cord. Amniotic fluid leakage can be identified on exam. Palpation of the abdomen, especially if the contraction monitor is insufficient, may identify the presence of excessive uterine activity or unrelenting uterine contraction.
Vital signs are a crucial part of the physical exam. Maternal obesity can make fetal monitoring difficult, especially at early gestational ages. The presence of a fever, tachycardia, or low blood pressure may indicate systemic illness; this, in turn, can be reflected in the fetal heart tracing. Exam findings, eg, dry mucous membranes or poor capillary refill, along with tachycardia, may indicate maternal dehydration. Maternal dehydration may contribute to fetal tachycardia.
Evaluation
During electronic fetal monitoring, a finding of category II fetal heart tracings requires further evaluation.
An initial evaluation requires first understanding the entire clinical scenario, including the relevant clinical history, and performing a targeted physical exam. (Please refer to the History and Physical section for more information on these findings.)
Intermittent Variable Decelerations
Variable decelerations with less than 50% of the contractions are the most common abnormality of the fetal heart rate during labor. Variable decelerations are usually associated with normal outcomes. If variable decelerations are not recurrent and resolve spontaneously, no further evaluation is indicated.
Recurrent Variable Decelerations
Initial evaluation includes characterization of the decelerations themselves, including their frequency, depth, and duration.[5] Assessing the uterine contraction pattern and the other fetal heart tracing characteristics is also important. A cervical exam to assess dilation and fetal station and evaluate for a prolapsed umbilical cord can be useful both for identifying possible etiologies of concerning fetal heart rate tracings and for informing management. In the antepartum setting, variable decelerations may also indicate the need for further evaluation. Assessment of the amniotic fluid volume may be recommended, along with continued monitoring.
Recurrent Late Decelerations
As late decelerations reflect transient or chronic uteroplacental insufficiency, evaluation focuses on identifying causes of poor perfusion or oxygenation. Maternal blood pressure should be checked, and maternal position should be observed. Lying supine may compress the inferior vena cava, leading to hypotension. An epidural may also result in maternal hypotension, especially right after placement.
The tracing should be examined for excessive uterine activity. A physical examination of the maternal abdomen may also help identify uterine tachysystole. Additionally, maternal pulse oximetry may help identify maternal hypoxia.[5]
Fetal Tachycardia
Evaluation is focused on identifying underlying causes, including:
- Infection: intrauterine infection, pyelonephritis, other maternal infections
- Medications: terbutaline, cocaine, other stimulants
- Maternal medical disorders: hyperthyroidism
- Obstetric conditions: placental abruption, fetal bleeding
- Fetal tachyarrythmias: associated with heart rate>200 bpm [5]
Fetal Scalp Stimulation
Because the presence of moderate variability or accelerations is considered a reassuring sign of normal acid/base status, the evaluation of category II fetal tracings may involve attempts to induce accelerations. The fetus can be stimulated directly during a cervical examination by using the examining fingers or a device to rub the fetal scalp. The desired result is an acceleration on the fetal tracing. Other techniques can also be used to elicit acceleration, eg, a vibroacoustic stimulation device. If stimulation leads to an acceleration, this may be taken as one point of evidence in favor of continuing labor. Lack of an appropriate fetal response, characterized by the absence of acceleration following stimulation, may serve as evidence supporting the need to facilitate delivery via cesarean section.
Treatment / Management
In 2013, researchers proposed an algorithm for managing category II fetal heart tracings.[14] The initial step involves determining the presence of accelerations or moderate variability. The subsequent step focuses on identifying significant decelerations. Significant decelerations were defined as follows:
- Variable decelerations reaching a nadir of more than 60 beats per minute below the baseline and lasting longer than 60 seconds
- Variable decelerations reaching a nadir of fewer than 60 beats per minute, regardless of baseline, and lasting longer than 60 seconds
- Any late deceleration
- Any prolonged deceleration (lasting 2 minutes or longer) [14]
Management Algorithm
The management algorithm for category II fetal heart tracings begins with assessment of variability, accelerations, and the presence of significant decelerations.
When moderate variability or accelerations are present alongside significant decelerations occurring with 50% or more of contractions for 1 hour, the following management depends on the stage of labor:
- During the latent phase, cesarean delivery is recommended.
- In the active phase, observation remains appropriate with normal labor progress, whereas a lack of progress warrants cesarean delivery.
- During the second stage of labor, observation is appropriate with normal progress, while abnormal progress necessitates cesarean or operative vaginal delivery.[14]
Observation also remains appropriate when moderate variability or accelerations are present without significant decelerations in 50% or more of contractions for 1 hour.
Absence of moderate variability or accelerations with significant decelerations occurring in 50% or more of contractions for 30 minutes warrants cesarean delivery or operative vaginal delivery. When moderate variability or accelerations remain absent, and significant decelerations do not occur with 50% or more of contractions for 30 minutes, observation for 1 hour is appropriate. A persistent pattern of an absence of moderate variability or accelerations without significant decelerations with 50% or more of contractions for 30 minutes supports cesarean or operative vaginal delivery. However, resolution of this pattern allows continued management according to the algorithm.
Targeted Interventions
Based on the suspected etiology of underlying fetal heart tracing abnormalities, the following intrauterine resuscitative measures have been developed that can alleviate these abnormalities:
- Promote fetal oxygenation; improve blood flow through the placenta and uterus.
- Reduced fetal oxygenation is associated with recurrent late decelerations, prolonged decelerations, bradycardia, and minimal or absent variability.
- Perform lateral repositioning, left or right.
- Administer maternal oxygen. [5]
- Reduce uterine activity.
- Increased uterine activity is associated with tachysystole and fetal heart rate abnormalities.
- Discontinue cervical ripening agent or oxytocin.
- Administer tocolytic medication, eg, terbutaline.
- Alleviate the compression of the umbilical cord.
- This procedure is associated with recurrent variable decelerations, prolonged decelerations, or bradycardia.
- Administer amnioinfusion (reintroduce fluid into the uterine cavity with an intrauterine pressure catheter).
- If the exam shows a prolapsed umbilical cord, elevate the presenting part and prepare for emergent cesarean delivery.[5]
The 2012 Cochrane Review for amnioinfusion for umbilical cord compression showed not only an improvement in cesarean section and decelerations, but also in 5-minute Apgar scores, postpartum endometritis, maternal hospital stay, and mean umbilical artery pH.[15] More recent research has called into question the benefit of maternal oxygen supplementation as a technique for intrauterine resuscitation. Randomized controlled trials have shown no improvement in umbilical cord gases or other adverse outcomes. Meta-analyses have shown no improvement in umbilical artery pH or a reduction in cesarean delivery rates. Additionally, some evidence shows adverse outcomes in neonates with excessive in utero oxygen exposure, including lower umbilical artery pH and the presence of reactive oxygen species.[16] While caution should be used when deciding whether to use maternal oxygen supplementation, this strategy is still a reasonable option if objective data indicate maternal hypoxemia. (A1)
In specific clinical scenarios that may result in concerning decelerations, management should be guided by the underlying etiology. For example, in the second stage of labor, maternal pushing efforts may also lead to variable decelerations. Depending on the presence or absence of other reassuring signs of fetal status, the patient might be advised not to push with every contraction to allow adequate fetal recovery between pushes. Furthermore, if a patient is being monitored for preterm prelabor rupture of membranes, recurrent variable decelerations may be a sign of worsening fetal and maternal status. In the setting of preterm prelabor rupture of membranes, delivery is necessary with nonreassuring fetal status, intraamniotic infection, or placental abruption.
Ultimately, if the fetal heart tracing is persistently abnormal, facilitating delivery is indicated. In the term, laboring patient, an operative vaginal delivery may be considered. If the patient is remote from delivery, cesarean delivery may be indicated. In a patient with preterm prelabor rupture of membranes, induction or augmentation of labor may be the next step if the fetus is in the vertex presentation. Alternatively, cesarean delivery may be indicated if the fetus is in the breech presentation.
Differential Diagnosis
Recurrent Variable Decelerations
The differential diagnosis for recurrent variable decelerations includes:
- Intrauterine umbilical cord compression
- Maternal/fetal positioning
- Low fluid or oligohydramnios
- Nuchal cord or other cord entanglements
- True knot or short umbilical cord
- Uterine tachysystole
- Pushing efforts during the second stage of labor
- Increasing fetal acidemia
- Umbilical cord prolapse
- Uterine rupture
Late Decelerations
The differential diagnosis for late decelerations includes:
- Hypotension
- Maternal positioning
- Epidural
- Medications/drugs
- Uteroplacental insufficiency
- Antepartum placental damage
- Placental abruption
- Maternal conditions impacting blood flow to the fetus
- Preeclampsia/eclampsia
- Infection
- Anemia
- Dehydration
- Fetal hypoxia
Fetal heart rate decelerations may be confused with one another. While the definitions of each type of deceleration are clear, poor intraobserver and interobserver reproducibility is noted in the interpretation of fetal heart tracings.[2] Because the management of various decelerations differs, distinguishing among them is critical.
Medication Effects
Medications given during the intrapartum period can influence fetal heart rate patterns. These changes are usually transient. Sometimes they will lead to intervention by the healthcare team.[1]
Epidural analgesia containing local anesthetic agents, eg, lidocaine or bupivacaine, can lead to sympathetic blockade, hypotension, and transient uteroplacental insufficiency that may be reflected in the fetal heart rate tracing. Parenteral narcotics can also impact the fetal heart rate. Fetal heart rate decelerations and decreased variability are present.[1]
Butorphanol can lead to a transient sinusoidal pattern and a slightly increased baseline heart rate. Cocaine has been found to decrease long-term variability. Magnesium sulfate decreases short-term variability, inhibits the increase in accelerations observed at later gestational ages, and may decrease the baseline, though not significantly. Terbutaline has been found to increase the fetal heart rate baseline, even causing tachycardia. Corticosteroids may reduce variability, particularly with betamethasone. With steroids, a loss of diurnal fetal rhythms is also seen. These effects are more pronounced when gestational age exceeds 29 weeks.[1]
Prognosis
Electronic fetal monitoring has the ultimate goal of preventing adverse perinatal outcomes, eg, hypoxic-ischemic encephalopathy, cerebral palsy, and death. The efficacy of continuous electronic fetal monitoring, however, is debated. Continuous electronic fetal monitoring has been shown to increase the rates of cesarean delivery and operative vaginal delivery and decrease neonatal seizures. However, continuous electronic fetal monitoring has not been shown to reduce perinatal mortality or the risk of cerebral palsy.[1]
Intermittent variable decelerations and early decelerations are usually benign and do not lead to adverse perinatal outcomes. Category III fetal heart tracings are associated with abnormal fetal acid/base status and acidemia. In some clinical scenarios with category II fetal heart tracings, eg, recurrent variable decelerations, tracings do correlate with poor outcomes, including neonatal acidemia.[17][18] The peripheral chemoreflex response to hypoxemia is a tailored response, so an increasing severity of hypoxemia leads to deeper decelerations.[6] Hypoxemia and fetal acidosis have correlations with the following conditions:
- Meconium aspiration
- Metabolic and hematologic disturbances
- Cognitive dysfunction
- Hypoxic-ischemic encephalopathy
- Cerebral palsy
- Death
The presence of category II heart tracing does not always indicate a poor prognosis. For example, if the fetal heart tracing also demonstrates moderate variability and accelerations, the fetal acid-base status may still be normal.[1] Also, if the category II heart tracing is identified, evaluated, and managed appropriately (including proceeding with cesarean delivery if indicated), the prognosis is favorable.
Complications
In addition to increasing the cesarean delivery rate, intra- and interobserver variability in the interpretation of fetal heart rate tracings is high. In one study, obstetricians reviewed cardiotocographs and agreed only 22% of the time; 2 months later, they reviewed the same tracings and interpreted them differently in 21% of cases.[19] The positive predictive value and false positive rate of electronic fetal monitoring are also poor. Nonreassuring fetal heart rate patterns predict cerebral palsy only 0.14% of the time, and they have a false positive rate of greater than 99%.[1] Future advancements in fetal monitoring, as well as collaboration across the healthcare spectrum to standardize evidence-based care, are hoped to counteract these shortcomings and improve health outcomes for babies and mothers.[20]
Consequences of Hypoxia
Low pH in fetal cells and inadequate energy production due to hypoxia and acidosis may compromise cell function and lead to cell death. Most babies born with metabolic acidosis will recover quickly and not have complications. If the hypoxia and acidosis are sufficiently severe in intensity and duration to cause dysfunction of important fetal organs and systems, the newborn is at risk of long-term morbidity or death.[8]
The short-term neurologic dysfunction that results from hypoxia/acidosis during labor, or other predelivery insults, is called hypoxic-ischemic encephalopathy (HIE). This diagnosis is given only if metabolic acidosis is confirmed, Apgar scores are low, early imaging shows evidence of cerebral edema, and changes in sucking movements, muscle tone, seizures, or coma are apparent within the first 48 hours after birth. Neonatal encephalopathy also has other causes, which is why umbilical artery or newborn laboratory documentation of metabolic acidosis within the first minutes of life is important. HIE can be accompanied by dysfunction of the renal, cardiovascular, gastrointestinal, pulmonary, or hematologic systems.[8]
HIE is divided into 3 grades using the Sarnat classification:
- Grade 1: no seizures; most newborns do not develop any major long-term sequelae
- Grade 2: seizures; associated with a risk of death or major neurologic sequelae of 20% to 30%
- Grade 3: coma; the majority of newborns develop long-term neurologic sequelae or suffer a demise [8]
Cerebral palsy of the dyskinetic or spastic quadriplegic type is a long-term neurologic sequelae that is associated more commonly with intrapartum hypoxia/acidosis in term deliveries. In high-resource settings, only 10% to 20% of cerebral palsy is caused by birth asphyxia. The majority of cases are due to other causes, eg, congenital disease, infection, metabolic disease, antepartum or postnatal hypoxia, coagulation disorders, complications associated with childbirth, and prematurity.[8]
Avoiding adverse outcomes related to hypoxia/acidosis is the main goal of fetal monitoring during labor; avoiding unnecessary intervention is equally important. When evaluating and managing category II fetal heart tracings, following guidelines and protocols that balance the risks and benefits of continuing labor versus cesarean delivery is important. A systems-based approach is needed to reduce avoidable harms associated with fetal monitoring.[21]
Deterrence and Patient Education
Patients require education regarding the purpose of electronic fetal monitoring, their options for continuous or intermittent monitoring, and the potential consequences of monitoring, eg, cesarean section. Additionally, the potential benefits of fetal monitoring warrant a review. When pregnancy complications or diagnoses that may affect patient care are identified, they should be addressed in the office before hospital admission. For example, patients with low fluid can be told their diagnosis and then allowed adequate time across subsequent appointments for adequate patient counseling regarding expectations during labor. Some patients may desire intermittent fetal monitoring but are not candidates due to maternal or fetal complications and conditions.
Interventions for fetal heart tracing abnormalities may be initiated quickly and require multiple healthcare team members to perform. This can be alarming to patients. If interventions can be anticipated or discussed in advance, this may help alleviate some patients' fears. As interventions are occurring, explaining to the patient what is happening and why is essential, as patient autonomy and education are always crucial. When interventions are urgent or emergent, conducting a debrief with the patient after the acute episode has passed is important. This allows for explanation of the events and interventions that occurred, answering patient questions, and providing anticipatory guidance for the course of care moving forward.
Pearls and Other Issues
Intrapartum fetal heart rate tracings are divided into 3 categories. Each category is associated with a different level of reassurance or concern regarding fetal status. The following management is delineated for each category:
- Category I: Normal finding; no action is required.
- Baseline 110 to 160 beats per minute
- Moderate variability
- No late or variable decelerations
- Early decelerations may be present or absent
- Accelerations may be present or absent
- Category II: Indeterminate finding; evaluation, intervention, and surveillance are indicated.
- All tracings that are not category I or category III
- Category III: Abnormal finding; prompt delivery may be indicated.
- Absent variability and one of the following:
- Recurrent late decelerations
- Recurrent variable decelerations
- Bradycardia
- Sinusoidal pattern [5]
- Absent variability and one of the following:
Enhancing Healthcare Team Outcomes
Electronic fetal monitoring is widely used during labor to assess fetal oxygenation and reduce the risk of adverse neonatal outcomes such as hypoxia, acidemia, and neurologic injury. Fetal heart rate tracings reflect the interplay between uteroplacental perfusion, fetal compensatory mechanisms, and cardioregulatory responses to stress. Abnormal patterns, including variable or late decelerations and reduced variability, may signal impaired oxygen delivery and an increased risk of metabolic acidosis. Timely evaluation requires systematic interpretation using standardized criteria, with frequent reassessment based on clinical risk. In uncomplicated labor, tracings are reviewed every 30 minutes in the first stage and every 15 minutes in the second stage, with more frequent monitoring in high-risk patients. Management focuses on identifying underlying causes and initiating targeted intrauterine resuscitative measures or expediting delivery when indicated.
Interprofessional collaboration is essential to ensure accurate interpretation, timely intervention, and optimal outcomes. Physicians oversee diagnosis, risk stratification, and operative decision-making, while nurses provide continuous monitoring, early recognition of abnormalities, and prompt communication of concerns. Advanced practitioners support clinical assessment and implementation of management strategies. Pharmacists contribute by optimizing medication use, including oxytocin adjustments or tocolytics, to reduce uterine tachysystole. Neonatal specialists prepare for potential resuscitation when concerning patterns persist. Structured communication, shared decision-making with the patient, and coordinated team responses improve safety, reduce delays in care, and enhance consistency in evidence-based management, ultimately promoting better maternal and neonatal outcomes.
Media
(Click Image to Enlarge)
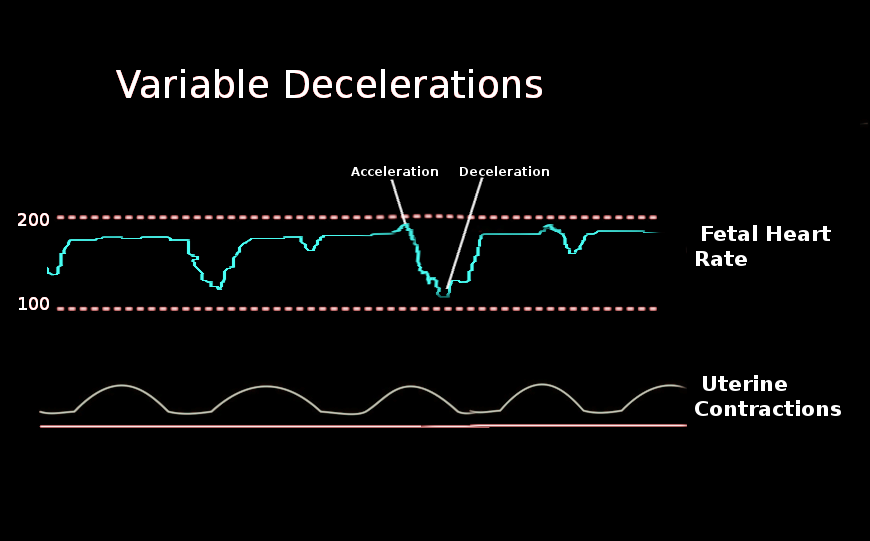
Variable Decelerations. A variable deceleration is a visually apparent, abrupt decrease in fetal heart rate.
Contributed by O Chaigasame, MD
(Click Image to Enlarge)
Fetal Heart Rate Terminology. The American College of Obstetricians and Gynecologists standardized terminology for electronic fetal monitoring.
Contributed by J Choe, MA
References
. ACOG Practice Bulletin No. 106: Intrapartum fetal heart rate monitoring: nomenclature, interpretation, and general management principles. Obstetrics and gynecology. 2009 Jul:114(1):192-202. doi: 10.1097/AOG.0b013e3181aef106. Epub [PubMed PMID: 19546798]
Level 1 (high-level) evidenceBeaulieu MD, Fabia J, Leduc B, Brisson J, Bastide A, Blouin D, Gauthier RJ, Lalonde A. The reproducibility of intrapartum cardiotocogram assessments. Canadian Medical Association journal. 1982 Aug 1:127(3):214-6 [PubMed PMID: 7104902]
David AL, Spencer RN. Clinical Assessment of Fetal Well-Being and Fetal Safety Indicators. Journal of clinical pharmacology. 2022 Sep:62 Suppl 1(Suppl 1):S67-S78. doi: 10.1002/jcph.2126. Epub [PubMed PMID: 36106777]
Macones GA, Hankins GD, Spong CY, Hauth J, Moore T. The 2008 National Institute of Child Health and Human Development workshop report on electronic fetal monitoring: update on definitions, interpretation, and research guidelines. Obstetrics and gynecology. 2008 Sep:112(3):661-6. doi: 10.1097/AOG.0b013e3181841395. Epub [PubMed PMID: 18757666]
American College of Obstetricians and Gynecologists. Practice bulletin no. 116: Management of intrapartum fetal heart rate tracings. Obstetrics and gynecology. 2010 Nov:116(5):1232-40. doi: 10.1097/AOG.0b013e3182004fa9. Epub [PubMed PMID: 20966730]
Lear CA, Westgate JA, Ugwumadu A, Nijhuis JG, Stone PR, Georgieva A, Ikeda T, Wassink G, Bennet L, Gunn AJ. Understanding Fetal Heart Rate Patterns That May Predict Antenatal and Intrapartum Neural Injury. Seminars in pediatric neurology. 2018 Dec:28():3-16. doi: 10.1016/j.spen.2018.05.002. Epub 2018 Jun 20 [PubMed PMID: 30522726]
Level 3 (low-level) evidenceJia YJ, Ghi T, Pereira S, Gracia Perez-Bonfils A, Chandraharan E. Pathophysiological interpretation of fetal heart rate tracings in clinical practice. American journal of obstetrics and gynecology. 2023 Jun:228(6):622-644. doi: 10.1016/j.ajog.2022.05.023. Epub [PubMed PMID: 37270259]
Ayres-de-Campos D, Arulkumaran S, FIGO Intrapartum Fetal Monitoring Expert Consensus Panel. FIGO consensus guidelines on intrapartum fetal monitoring: Physiology of fetal oxygenation and the main goals of intrapartum fetal monitoring. International journal of gynaecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics. 2015 Oct:131(1):5-8. doi: 10.1016/j.ijgo.2015.06.018. Epub [PubMed PMID: 26433399]
Level 3 (low-level) evidenceHeuser CC. Physiology of Fetal Heart Rate Monitoring. Clinical obstetrics and gynecology. 2020 Sep:63(3):607-615. doi: 10.1097/GRF.0000000000000553. Epub [PubMed PMID: 32618597]
Ball RH, Parer JT. The physiologic mechanisms of variable decelerations. American journal of obstetrics and gynecology. 1992 Jun:166(6 Pt 1):1683-8; discussion 1688-9 [PubMed PMID: 1615975]
Timor-Tritsch IE, Dierker LJ, Zador I, Hertz RH, Rosen MG. Fetal movements associated with fetal heart rate accelerations and decelerations. American journal of obstetrics and gynecology. 1978 Jun 1:131(3):276-80 [PubMed PMID: 665735]
Lee CY, Di Loreto PC, O'Lane JM. A study of fetal heart rate acceleration patterns. Obstetrics and gynecology. 1975 Feb:45(2):142-6 [PubMed PMID: 1118084]
Lear CA, Galinsky R, Wassink G, Yamaguchi K, Davidson JO, Westgate JA, Bennet L, Gunn AJ. The myths and physiology surrounding intrapartum decelerations: the critical role of the peripheral chemoreflex. The Journal of physiology. 2016 Sep 1:594(17):4711-25. doi: 10.1113/JP271205. Epub 2016 May 27 [PubMed PMID: 27328617]
Clark SL, Nageotte MP, Garite TJ, Freeman RK, Miller DA, Simpson KR, Belfort MA, Dildy GA, Parer JT, Berkowitz RL, D'Alton M, Rouse DJ, Gilstrap LC, Vintzileos AM, van Dorsten JP, Boehm FH, Miller LA, Hankins GD. Intrapartum management of category II fetal heart rate tracings: towards standardization of care. American journal of obstetrics and gynecology. 2013 Aug:209(2):89-97. doi: 10.1016/j.ajog.2013.04.030. Epub 2013 Apr 27 [PubMed PMID: 23628263]
Hofmeyr GJ, Lawrie TA. Amnioinfusion for potential or suspected umbilical cord compression in labour. The Cochrane database of systematic reviews. 2012 Jan 18:1(1):CD000013. doi: 10.1002/14651858.CD000013.pub2. Epub 2012 Jan 18 [PubMed PMID: 22258939]
Level 1 (high-level) evidenceBurd J, Raghuraman N. Intrapartum Oxygen for Fetal Resuscitation: State of the Science. Current obstetrics and gynecology reports. 2023 May 18:():1-5. doi: 10.1007/s13669-023-00363-w. Epub 2023 May 18 [PubMed PMID: 37360259]
Cahill AG, Roehl KA, Odibo AO, Macones GA. Association and prediction of neonatal acidemia. American journal of obstetrics and gynecology. 2012 Sep:207(3):206.e1-8. doi: 10.1016/j.ajog.2012.06.046. Epub [PubMed PMID: 22939728]
Level 2 (mid-level) evidenceRimsza RR, Frolova AI, Kelly JC, Carter EB, Cahill AG, Raghuraman N. Intrapartum electronic fetal monitoring features associated with a clinical diagnosis of nonreassuring fetal status. American journal of obstetrics & gynecology MFM. 2023 Sep:5(9):101068. doi: 10.1016/j.ajogmf.2023.101068. Epub 2023 Jun 26 [PubMed PMID: 37380056]
Nielsen PV, Stigsby B, Nickelsen C, Nim J. Intra- and inter-observer variability in the assessment of intrapartum cardiotocograms. Acta obstetricia et gynecologica Scandinavica. 1987:66(5):421-4 [PubMed PMID: 3425243]
Lovers A, Daumer M, Frasch MG, Ugwumadu A, Warrick P, Vullings R, Pini N, Tolladay J, Petersen OB, Lederer C, Yang L, Djurić PM, Abtahi F, Holzmann M, Boudet S, de l'Aulnoit AH, Georgieva A. Advancements in Fetal Heart Rate Monitoring: A Report on Opportunities and Strategic Initiatives for Better Intrapartum Care. BJOG : an international journal of obstetrics and gynaecology. 2025 Jun:132(7):853-866. doi: 10.1111/1471-0528.18097. Epub 2025 Feb 19 [PubMed PMID: 39971749]
Kelly S, Lamé G, Dixon-Woods M, Liberati E, Kyriacou H, Dunn H, Egerton A, Kok ZK, Jones K, Zheng XN, Kuhn I, Draycott TJ, Winter C, Burt J. Influences on safety of intrapartum electronic fetal heart rate monitoring practices: a scoping review. BMJ open. 2024 Dec 22:14(12):e085827. doi: 10.1136/bmjopen-2024-085827. Epub 2024 Dec 22 [PubMed PMID: 39806617]
Level 2 (mid-level) evidence