Introduction
The uterine arteries are the main blood vessels that supply blood to the uterus. These arteries give off branches that supply different portions of the uterus and play an important role in maintaining blood supply during physiological processes, such as the altered endometrium during the menstrual cycle and growth of the uterus during pregnancy. During its course, the uterine artery passes anterior to the distal ureter; some refer to this as water under the bridge.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
There are two uterine arteries, one on each side (left and right). The uterine artery is a branch of the internal iliac artery, also called the hypogastric artery. The right uterine artery is a branch of the right anterior division of the internal iliac artery. The uterine artery courses from lateral to the medial direction through the bottom part of the broad ligament, also called the cardinal ligament. At the uterine isthmus level, the uterine artery is divided into ascending and descending branches.[1][2][3]
After the bifurcation, the ascending artery further rises superiorly next to the uterus and runs a tortuous course with the lateral side of the uterus. The ascending artery, in multiparous women, becomes much more convoluted and tortuous in size and shape. The ascending branch of the uterine artery anastomoses to the ovarian artery. The ovarian artery is a direct branch of the abdominal aorta. The ovarian artery supplies oxygenated blood to the ovary, fallopian tube, and uterus. In the myometrium, the uterine artery further branches out to the arcuate artery, radial artery, spiral artery, and basal artery.
The descending branch supplies blood to the uterine cervix and vagina. The arcuate artery around the cervix is also called the circular artery of the cervix. The uterine artery also branches towards the fallopian tube and ureter as it passes across them. Cervicovaginal branches anastomose with vaginal arteries to create the azygos arteries of the vagina.
The arcuate arteries of the uterus supply blood to the smooth musculature of the uterus called the myometrium. The arcuate arteries penetrate throughout the circumference of the myometrium and supply blood to the anterior and posterior walls of the uterus. The arcuate artery terminates in the spiral artery, which supplies the endometrium, decidua, and placenta during pregnancy. The rhythmic contraction and relaxation of these vessels help to maintain endometrial stability and necessary control of blood supply. These vessels are usually demonstrated in the late luteal phase. Before the beginning of menses and during menses, these vessels are less apparent. Estrogen increases the size and number of these vessels and increases blood flow. Estrogen is responsible for the proliferation of the uterine endometrium during the proliferative phase of the menstrual cycle.
The spiral arteries supply blood to the endometrium of the uterus, more specifically, the functional zone, which sheds during menstruation. In histology, identification of spiral arteries helps to make the diagnosis of the luteal phase of the menstrual cycle. The basal arteries supply blood to the endometrium, specifically the basal zone. The basal zone starts the regeneration of the denuded endometrium after menstruation. This regeneration happens under the influence of estrogen during the proliferative phase of the menstrual cycle. Maintenance of the stroma is supported by progesterone.[4]
Surgical Considerations
In pathological conditions like a fibroid uterus, the course of the uterine artery and its branches is significantly distorted. Uterine fibroids are the most common uterine tumors in the reproductive age of a woman. The uterine artery supplies blood to the growing fibroids, and this blood supply facilitates the growth of the fibroid. Most of the fibroids are benign and asymptomatic. Symptomatic fibroids may cause severe pelvic pain, dysmenorrhea, menorrhagia, and iron deficiency anemia. Symptomatic fibroids are the most common indication for hysterectomy in the United States. Symptomatic fibroids are usually treated by surgery. After reproductive age, uterine fibroids may be treated with gonadotropin-releasing hormone to shrink them. Uterine artery embolization blocks blood flow to fibroids, reducing their size; this radiological procedure may improve symptoms in many patients. It is not recommended during the reproductive period as it may cause atrophy of the ovaries leading to menopausal symptoms.[5]
During a hysterectomy, it is important to isolate the descending ureter from the uterine artery to avoid injury to the ureter. A surgical injury to the lower ureter happens during a difficult surgery, such as in cases of a tubo-ovarian abscess, pelvic mass, or various malignant conditions of pelvic organs. Many times, injuries of the ureter are missed during surgery. Postoperative cystoscopy and visualization of dye freely flowing from both ureters may confirm intact ureters.[6] During a cesarean delivery, there may be excessive bleeding during the surgery. Suturing or compressing the uterus or medical management may not succeed. In this situation, bilateral uterine artery ligation may stop bleeding. Recanalization of uterine vessels automatically takes place after recovery.
Clinical Significance
Pregnancy is a physiological state in which uterine smooth muscles and blood vessels proliferate continuously. During pregnancy, there is a considerable decrease in uterine vascular and muscular tone and an increase in uterine blood flow. Increased levels of steroid hormones during pregnancy, such as estrogen, progesterone, and cortisol, affect the uterine vasculature and musculature. Estrogen is a major factor in the increased size of the uterus and thickening of the uterine wall.[4]
The myometrium, the middle layer of the uterine wall, mainly consists of smooth muscle cells. The myometrium greatly enlarges during pregnancy. There is a lack of uterine contractions during the normal gestational period. The prevention of contraction is done through progesterone inhibition of myocytes. During pregnancy, the myocytes undergo continuous stretching, hypertrophy, and remodeling. These physiological changes are necessary for a successful pregnancy. During early pregnancy, extravillous cytotrophoblasts invade the decidualized endometrium and myometrium. The spiral arteries transform into large, low-resistance vessels, accompanied by a gradual loss of the normal musculo-elastic structure of the arterial wall. In preeclampsia or fetal growth retardation, the trophoblastic invasion and spiral artery dysfunction deter normal physiological changes.
During pregnancy, a uterine artery Doppler study may be used to scan uterine artery flow. This study shows the amount of uterine artery obstruction. In cases of fetal growth retardation, diabetes, hypertensive disorders, and preeclampsia, there is dysfunction of blood flow to the placenta and fetus. Uterine artery color imaging and pulsed-wave Doppler ultrasound studies may be helpful for evaluating uterine artery flow, mean arterial pressure, and the uterine artery resistance index. Pregnant patients with elevated mean arterial pressure but a normal uterine artery resistance index may expect a favorable pregnancy outcome. Those with increased mean arterial pressure with an abnormal uterine artery resistance index may have an unfavorable outcome.
Increased uteroplacental blood flow is necessary for a normal pregnancy outcome. This is accomplished through systematic growth and remodeling of the uterine circulation and formation of the placenta. During pregnancy, the diameter of the main uterine artery approximately doubles in size. There is no thickening of the arterial wall during the enlargement of the arterial diameter.
In postmenopausal women, calcifications may be found in the wall of arcuate arteries. These calcified patches are echogenic and appear as linear echoes with shadowing. This is a normal aging process which may be increased in diabetic patients. These calcified lesions are distinctive from calcified fibroids.
Media
(Click Image to Enlarge)
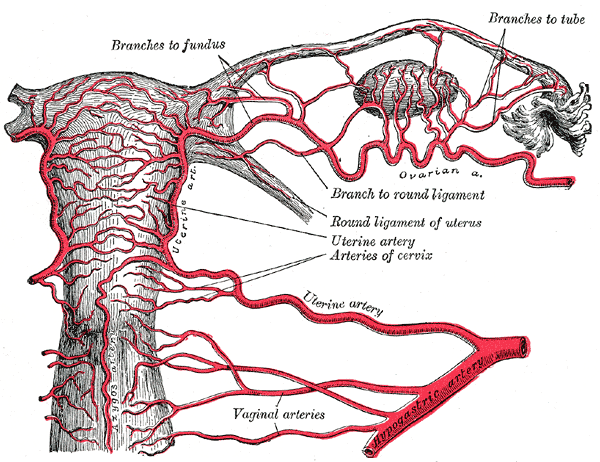
Vaginal Artery and its Branches. This illustration depicts the vaginal artery and its branches, the branches to the fundus, the branches to the tube, the arteries of the cervix, and the hypogastric artery.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Guida M, Maffucci D, Iannuzzi G, Giordano M, Luciano G, Di Benedetto L, Cantarella R, Rescigno A, Giugliano L. Successful pregnancy after uterine artery embolization for uterine arterovenous malformation: a rare case report. International journal of women's health. 2018:10():745-750. doi: 10.2147/IJWH.S182131. Epub 2018 Nov 21 [PubMed PMID: 30538584]
Level 3 (low-level) evidenceCraig ME, Sudanagunta S, Billow M. Anatomy, Abdomen and Pelvis: Broad Ligaments. StatPearls. 2026 Jan:(): [PubMed PMID: 29763118]
Dias T, Patabendige, M, Herath RPP, Garvik TI, Liland F, Arulkumaran S. Blood flow changes in pelvic vessels associated with the application of an abdominal compression belt in healthy postpartum women. The Ceylon medical journal. 2017 Dec 26:62(4):228-32 [PubMed PMID: 29393607]
Hwuang E, Vidorreta M, Schwartz N, Moon BF, Kochar K, Tisdall MD, Detre JA, Witschey WRT. Assessment of uterine artery geometry and hemodynamics in human pregnancy with 4d flow mri and its correlation with doppler ultrasound. Journal of magnetic resonance imaging : JMRI. 2019 Jan:49(1):59-68. doi: 10.1002/jmri.26229. Epub 2018 Nov 3 [PubMed PMID: 30390347]
Anton K, Rosenblum NG, Teefey P, Dayaratna S, Gonsalves CF. The Enlarged Fibroid Uterus: Aberrant Arterial Supply via the Omental Artery. Cardiovascular and interventional radiology. 2019 Apr:42(4):615-619. doi: 10.1007/s00270-018-2087-9. Epub 2018 Oct 15 [PubMed PMID: 30324267]
Liu Z, Wang Y, Yan J, Li J, Liu X, Zhang L, Cheng L. Uterine artery embolization versus hysterectomy in the treatment of refractory postpartum hemorrhage: a systematic review and meta-analysis. The journal of maternal-fetal & neonatal medicine : the official journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstetricians. 2020 Feb:33(4):693-705. doi: 10.1080/14767058.2018.1497599. Epub 2018 Oct 24 [PubMed PMID: 30354858]
Level 1 (high-level) evidence