Introduction
The ulnar nerve is one of the 5 terminal branches of the brachial plexus, arising from the medial cord. The nerve provides motor and sensory innervation to the upper extremity. The ulnar nerve originates from contributions of the ventral rami of the C8 and T1 nerve roots. The nerve courses along the medial aspect of the arm and forearm, then innervates the wrist, hand, and digits.[1][2][3]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The ulnar nerve provides motor innervation to part of the forearm and most of the hand. The ulnar nerve supplies sensory cutaneous innervation to the medial forearm, medial wrist, and medial 1.5 digits. The ulnar nerve and its branches send motor innervation to the flexor carpi ulnaris and flexor digitorum profundus in the forearm and to the hypothenar muscles, including the opponens digiti minimi, abductor digiti minimi, and flexor digiti minimi brevis. In the hand, the ulnar nerve provides motor innervation to the third and fourth lumbricals, dorsal interossei, palmar interossei, adductor pollicis, flexor pollicis brevis, and palmaris brevis.
Nerves
The ulnar nerve carries both sensory and motor fibers from the C8 and T1 ventral rami. The nerve courses along the medial arm from the anterior to the posterior compartment through the medial intermuscular septum, also called the arcade of Struthers. The arcade is formed by the medial head of the triceps, medial intermuscular septum, and internal brachial ligament. The ulnar nerve then passes posterior to the medial epicondyle of the humerus, giving off its first branch, which provides proprioception to the elbow joint. At the distal elbow, the ulnar nerve passes underneath the Osborne ligament, the retinaculum between the 2 heads of the flexor carpi ulnaris muscle. The nerve continues through the flexor and pronator muscles of the forearm and into the wrist, superficial to the flexor retinaculum. The ulnar nerve enters the hand through Guyon canal, a fibroosseous tunnel formed by the pisiform and hook of the hamate. In the hand, the ulnar nerve branches to give rise to the palmar cutaneous branch (nerve of Henle) and dorsal cutaneous branch. The dorsal cutaneous nerve then bifurcates into radial and ulnar branches, providing sensation to the dorsal hand.[4][5]
Muscles
The ulnar nerve innervates the flexor muscles of the forearm, including the flexor carpi ulnaris and flexor digitorum profundus. The nerve also innervates the intrinsic muscles of the hand, including the palmaris brevis, lumbricals, hypothenar muscles, and interossei muscles. In the hand, the superficial branch of the ulnar nerve innervates the palmaris brevis muscle and provides sensory innervation to the hypothenar muscles, fourth common digital nerve, and ulnar proper nerve. The deep branch innervates the hypothenar muscles, opponens digiti minimi, interosseous muscles, third and fourth lumbricals, adductor pollicis, and medial head of the flexor pollicis brevis.
Physiologic Variants
Anatomical variants are important to identify for prompt, accurate diagnosis of nerve dysfunction and to prevent delayed treatment. Two nerve variations include Martin-Gruber and Riche-Cannieu anastomoses.[6] Martin-Gruber anastomosis is a communication between the median and ulnar nerves in the forearm at any point distal to the medial epicondyle. With this anatomical variant, the motor nerves innervating the intrinsic ulnar muscles are carried by the anterior interosseous branch of the median nerve. In the midforearm, these fibers leave the anterior interosseous nerve to join the ulnar nerve. Therefore, patients with this variant can present with functional intrinsic hand muscle strength despite ulnar nerve dysfunction.
Riche-Cannieu anastomosis occurs when the median and ulnar nerves connect in the palm. This variant manifests as motor fibers typically carried by the median nerve being instead carried by the ulnar nerve to the hand, then crossing over in the palm. Riche-Cannieu anastomosis is clinically significant in the setting of carpal tunnel syndrome. Patients with advanced median nerve pathology could have normal function of the standard median nerve distribution.
Surgical Considerations
The most common site of ulnar nerve entrapment is at the elbow in the cubital tunnel. Cubital tunnel decompression with possible ulnar nerve transposition is a relatively common orthopedic procedure. The cubital tunnel is composed of the Osborne ligament (cubital tunnel retinaculum) and the deep layer of the aponeurosis of the 2 heads of the flexor carpi ulnaris muscle. Osborne ligament is the proximal roof of the cubital tunnel and prevents subluxation of the nerve with elbow flexion. During surgical decompression for cubital tunnel syndrome, Osborne fascia is incised to relieve pain and paresthesia caused by nerve injury. Transposition of the nerve from the arcade of Struthers to the flexor carpi ulnaris is also one of the recommended surgical treatments. The arcade of Struthers is formed by the internal brachial ligament, medial head of the triceps, and medial intermuscular septum just proximal to the medial epicondyle of the humerus. The arcade of Struthers is another possible site of ulnar nerve compression.[7][8][9]
Another surgical consideration includes incidental ulnar nerve damage during carpal tunnel release procedures. During surgical intervention for carpal tunnel syndrome, a small incision is made near the wrist crease. The surgeon dissects through the soft tissues of the wrist down to the transverse carpal ligament to relieve compression of the median nerve. Damage to the deep motor branch of the ulnar nerve can occur during this dissection because the branch courses just medial to the carpal tunnel along the hamate carpal bone. Although ulnar nerve damage is a rare complication of carpal tunnel release procedures, the incision should remain in line with the radial border of the fourth digit.
Clinical Significance
Ulnar nerve injury can be caused by several mechanisms, depending on the injury location along the course of the nerve, most commonly at the elbow. Proximal injury to the lower trunk of the brachial plexus can result in Klumpke palsy. Injury at the elbow may result in cubital tunnel syndrome, and compression at the Guyon canal of the wrist can manifest as motor and sensory deficits in the hand.[10]
Klumpke palsy is the manifestation of a lower trunk injury to the brachial plexus. Most commonly, lower trunk injuries result from an upward force on an infant’s arm or upward traction on the arm in an adult. Injury can also result from traumatic vaginal delivery with traction on an infant’s abducted arm due to a large infant birth weight or small birth canal. Klumpke palsy causes a functional deficit of the intrinsic hand muscles, presenting clinically with a complete claw hand. Clinically, findings include hyperextension of the metacarpophalangeal (MCP) joints due to loss of flexors, radial deviation of the wrist due to loss of flexor carpi ulnaris, and wasting of intrinsic hand muscles (lumbricals, interossei, thenar muscles, and hypothenar muscles) with flexion of the distal interphalangeal and proximal interphalangeal joints. Klumpke palsy is also known as strap-hanger syndrome. Horner syndrome (ptosis, miosis, and anhidrosis) can result from loss of sympathetic input from T1. Pupil constriction results from unopposed parasympathetic input to the eye.
The most common site of ulnar nerve injury is near the elbow. Nerve pathology can be caused by anatomic damage from fracture of the medial epicondyle, osteophyte formation, infection, soft tissue mass, or synovitis at the elbow joint. The nerve may also be damaged by compression from prolonged elbow flexion during activities such as sleep, exercise, driving, typing, or talking on the phone. Cubital tunnel syndrome is a peripheral neuropathy due to chronic compression or repetitive trauma of the ulnar nerve at the elbow between the medial epicondyle of the humerus and the olecranon process of the ulna.
Congenital laxity of the cubital tunnel retinaculum can occur, resulting in hypermobility of the ulnar nerve. Hypermobility can lead to repetitive subluxation and possible anterior dislocation when the elbow is flexed. Repetitive trauma at this location may result in inflammation from recurrent friction over the medial epicondyle.
Ulnar nerve impingement can also occur at the wrist due to compression through Guyon canal, local trauma, ganglion cysts, and external nerve compression. The ulnar nerve and artery enter Guyon canal, a fibroosseous tunnel formed by the pisiform and hook of the hamate. The ulnar nerve bifurcates within the canal into superficial and deep branches. Nerve compression at the wrist can also be caused by excess handlebar pressure in cyclists and prolonged compression while typing at a desk. Diagnosis of ulnar nerve injury can be made with a thorough history and musculoskeletal and neurological physical examination. However, electromyography (EMG) and nerve conduction studies can be used as adjuncts for diagnosing and localizing the lesion.
Media
(Click Image to Enlarge)
{kind=link}
(Click Image to Enlarge)
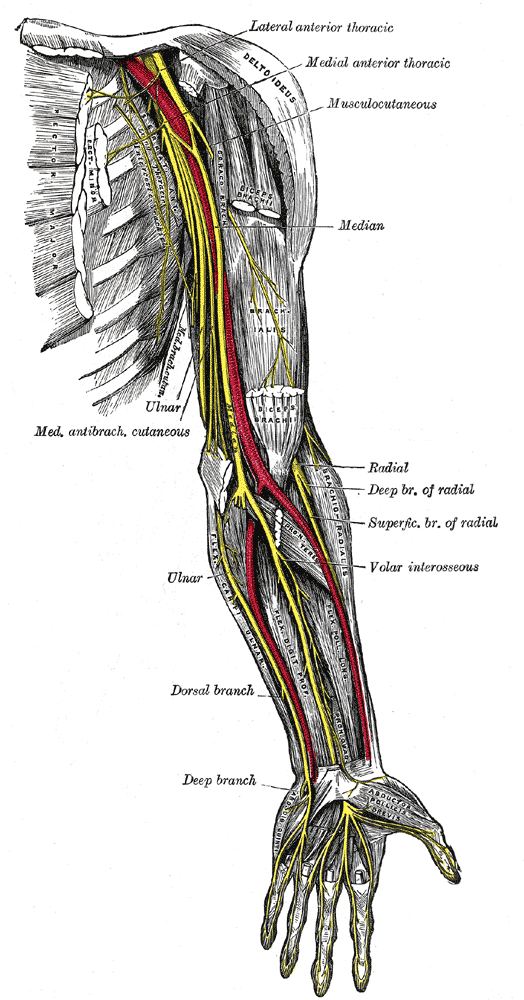
Nerves and Blood Vessels of the Arm and Forearm, Anterior View. This anatomical illustration depicts the nerves and arteries of the upper limb, highlighting the brachial artery (in red) running along the arm and forearm, with its major branches including the deep brachial artery, radial artery, and ulnar artery. Key nerves include the musculocutaneous, median, radial (with deep and superficial branches), and ulnar nerves, as well as the medial antebrachial cutaneous and dorsal branch of the ulnar nerve. The course of these nerves illustrates their anatomical relations with muscles such as the biceps brachii and brachialis and their distribution into the hand and digits.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)

Ulnar Nerve Compression.
Contributed by S Bhimji, MD
(Click Image to Enlarge)

Claw Hand. Clinical presentation of claw hand deformity in a patient with ulnar nerve injury, characterized by hyperextension at the 4th and 5th metacarpophalangeal joints and flexion at the corresponding proximal interphalangeal and distal interphalangeal joints.
Mcstrothe, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
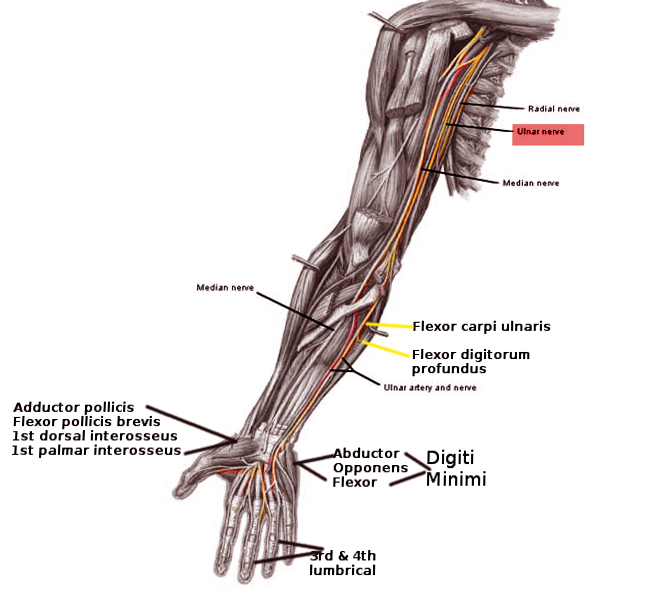
Ulnar Nerve Pathway. Anterior view illustrating the course of the ulnar nerve from the shoulder to the hand.
Image courtesy O.Chaigasame
References
Ramage JL, Varacallo MA. Anatomy, Shoulder and Upper Limb, Hand Guyon Canal. StatPearls. 2026 Jan:(): [PubMed PMID: 30521235]
Valenzuela M, Varacallo MA. Anatomy, Shoulder and Upper Limb, Hand Interossei Muscles. StatPearls. 2026 Jan:(): [PubMed PMID: 30521193]
Koziej M, Trybus M, Banach M, Bednarek M, Chrapusta A, Szuścik M, Piątek-Koziej K, Tomaszewski K. Comparison of Patient-Reported Outcome Measurements and Objective Measurements after Cubital Tunnel Decompression. Plastic and reconstructive surgery. 2018 May:141(5):1171-1181. doi: 10.1097/PRS.0000000000004291. Epub [PubMed PMID: 29697615]
Bains KNS, Lappin SL. Anatomy, Shoulder and Upper Limb, Elbow Cubital Fossa. StatPearls. 2026 Jan:(): [PubMed PMID: 29083694]
Hilgersom NFJ, van Deurzen DFP, Gerritsma CLE, van der Heide HJL, Malessy MJA, Eygendaal D, van den Bekerom MPJ. Nerve injuries do occur in elbow arthroscopy. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA. 2018 Jan:26(1):318-324. doi: 10.1007/s00167-017-4719-z. Epub 2017 Sep 20 [PubMed PMID: 28932881]
Patel M, Iwanaga J, Oskouian RJ, Tubbs RS. Variant Distal Ulnar Nerve Loop: A Previously Undescribed Anatomical Finding. Cureus. 2018 May 10:10(5):e2604. doi: 10.7759/cureus.2604. Epub 2018 May 10 [PubMed PMID: 30013868]
Lleva JMC, Munakomi S, Sun CE, Chang KV. Ulnar Neuropathy. StatPearls. 2026 Jan:(): [PubMed PMID: 30480959]
Andrews K, Rowland A, Pranjal A, Ebraheim N. Cubital tunnel syndrome: Anatomy, clinical presentation, and management. Journal of orthopaedics. 2018 Sep:15(3):832-836. doi: 10.1016/j.jor.2018.08.010. Epub 2018 Aug 16 [PubMed PMID: 30140129]
Briggs MS, Rethman KK, Lopez MT. CLINICAL DECISION MAKING AND DIFFERENTIAL DIAGNOSIS IN A CYCLIST WITH UPPER QUARTER PAIN, NUMBNESS, AND WEAKNESS: A CASE REPORT. International journal of sports physical therapy. 2018 Apr:13(2):255-268 [PubMed PMID: 30090684]
Level 3 (low-level) evidenceAleksenko D, Varacallo MA. Guyon Canal Syndrome. StatPearls. 2026 Jan:(): [PubMed PMID: 28613717]