Introduction
The trachea is a flexible, midline cylindrical conduit serving as the primary passageway for airflow during inspiration and expiration. As the most proximal structure of the lower respiratory tract, the trachea is structurally adapted to support essential physiologic functions. Organization of the cartilaginous framework, smooth muscle, mucosal lining, and submucosal glands maintains airway patency, enables mucociliary clearance, protects against aspiration, supports the cough reflex, facilitates phonation, and contributes to innate immune defense (see Image. Anatomy of the Tracheobronchial Tree).
A clear understanding of the relationship between tracheal structure and function is critical. Disruption of embryonic development may result in significant pathology, including esophageal atresia, tracheoesophageal fistula (TEF), tracheal atresia, and tracheomalacia. These conditions illustrate how deviations from normal development directly impair physiologic function. Given the proximity of the trachea to critical mediastinal and cervical structures, detailed knowledge of tracheal anatomy is essential for safe surgical planning. This activity examines structural components of the trachea, correlates structure with function, and explores clinical and surgical consequences arising from developmental failure or anatomic alteration.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The trachea is part of the lower respiratory system and allows the passage of gases, such as oxygen, between the external environment and the lungs. In infants, tracheal length measures approximately 5 to 6 cm and reaches approximately 10 to 13 cm in adulthood. Anatomically, the trachea is positioned anterior to the esophagus, arises immediately inferior to the larynx at the level of the cricoid cartilage and the 6th cervical vertebra, and terminates at the bifurcation into the primary bronchi at the carina at the level of the 4th to 5th thoracic vertebrae (see Image. Digestive and Respiratory Structures Anatomically Related to the Esophagus).
Structurally, the trachea consists of 4 layers (see Image. Transverse Section of the Tracheal Wall). The innermost mucosa contains pseudostratified ciliated columnar epithelium and an underlying lamina propria. The submucosa lies beneath the mucosa and is composed of connective tissue containing blood vessels, nerves, lymphatic plexuses, collagen, and elastin, providing structural support and elasticity. The musculocartilaginous layer consists of 16 to 20 C-shaped hyaline cartilage rings along the anterior and lateral walls, preventing collapse during inspiration.[1] The outermost adventitia anchors the trachea to surrounding tissues.
The pseudostratified ciliated columnar (respiratory) epithelium lining the innermost mucosa consists of goblet, pseudostratified ciliated columnar, basal, and neuroendocrine cells. Each epithelial cell type performs specialized functions.
Goblet cells are nonciliated columnar cells containing mucin-rich secretory granules, releasing mucus via exocytosis. The mucus contains electrolytes (sodium, chloride, bicarbonate), immunoglobulin A, lysozyme, lactoferrin, and peroxidase, contributing to lubrication, enhanced immune defense, and protection against mechanical and chemical injury. Ciliated columnar cells possess long motile cilia that propel particulate matter entrapped in mucus toward the oropharynx, a process known as mucociliary clearance.[2] Basal cells function as progenitor cells capable of differentiating into epithelial cell types and replacing damaged cells.[3] Neuroendocrine cells secrete serotonin and calcitonin gene-related peptides. These mediators regulate mucus secretion, ciliary rhythmic activity, and smooth muscle tone, and respond to environmental stimuli such as hypoxia.[4] The trachealis muscle bridges the posterior ends of the C-shaped tracheal cartilage rings.
The trachea receives arterial supply primarily from the inferior thyroid and bronchial arteries. Venous drainage primarily empties into the inferior thyroid and bronchial veins. Parasympathetic innervation is provided by the vagus nerve (cranial nerve X) and its branch, the recurrent laryngeal nerve (RLN), whereas sympathetic innervation arises from the cervical and upper thoracic sympathetic ganglia.
Several important anatomical structures surround the trachea. Anterior relations include the inferior thyroid veins and the left brachiocephalic vein. Posteriorly, the trachea is related to the esophagus, with the RLNs ascending within the tracheoesophageal grooves. Lateral relations, particularly near the 6th tracheal ring, include the thyroid gland lateral lobes and the carotid sheaths, containing the common carotid artery, internal jugular vein, and vagus nerve (see Image. Lymphatics and Neurovascular Relations of the Trachea).
Embryology
During the 3rd week of gestation, gastrulation transforms the bilaminar embryonic disc into a trilaminar disc composed of ectoderm, mesoderm, and endoderm. Respiratory system development begins during the 4th week of gestation from the endoderm-derived primitive foregut. A ventral outpouching, the laryngotracheal diverticulum, forms at the level of the laryngotracheal orifice. As elongation proceeds caudally, paired mesoderm-derived longitudinal tracheoesophageal folds develop and subsequently fuse to form the tracheoesophageal septum. Formation of this septum separates the primitive foregut into a ventral trachea and a dorsal esophagus. Failure of proper septal formation or fusion results in congenital anomalies discussed below (see Physiologic Variants).
Endoderm gives rise to the epithelial lining of the respiratory tract. Within the trachea, endoderm differentiates into pseudostratified ciliated columnar epithelium, goblet cells, and submucosal mucus glands. Structural components of the airway, including cartilage, smooth muscle, and connective tissue, derive from mesoderm, with laryngeal and tracheal cartilages arising from mesenchyme of the 4th and 6th pharyngeal arches at 10 weeks of gestation.[5]
Blood Supply and Lymphatics
The trachea is anatomically divided into cervical and thoracic segments. The cervical, or upper, segment measures approximately 2 to 4 cm in length and transitions into the thoracic segment at approximately the level of the 6th tracheal cartilage ring. Cervical tracheal arterial supply arises primarily from branches of the thyrocervical trunk, a vessel originating from the subclavian artery. The thyrocervical trunk typically gives rise to multiple tracheoesophageal branches supplying the posterior tracheal wall. The 1st tracheoesophageal branch provides the predominant arterial supply to the cervical trachea, whereas the remaining branches contribute mainly to the esophagus and thyroid gland, respectively. The inferior thyroid artery anastomoses with the superior thyroid artery, arising from the external carotid artery, near the level of the thyroid isthmus. This vascular connection reinforces arterial supply to the cervical trachea.
In contrast to the complex vascular supply of the cervical trachea, the thoracic trachea receives arterial supply from bronchial arteries arising from the thoracic aorta at the level of the 5th and 6th thoracic vertebrae. Venous drainage of the cervical trachea occurs via the inferior thyroid venous plexus, which empties into the brachiocephalic veins. Venous drainage of the thoracic trachea occurs into the azygos, hemiazygos, and pulmonary veins.
Lymphatic drainage of the trachea is segmental, reflecting its cervical and thoracic divisions. The cervical trachea drains primarily through the pretracheal and paratracheal lymph nodes, located laterally within the tracheoesophageal groove, with subsequent drainage into the deep cervical lymph nodes. On the right, lymph from the paratracheal nodes empties into the right lymphatic duct, whereas on the left, drainage proceeds into the thoracic duct. Lymph from the thoracic trachea drains into the superior tracheobronchial and posterior mediastinal lymph nodes, which communicate with the bronchomediastinal trunks and ultimately terminate in the right lymphatic duct on the right and the thoracic duct on the left, mirroring the lymphatic drainage of the cervical trachea.
The lymphatic network plays a critical role in immune surveillance by transporting inhaled pathogens, particulate matter, and antigen-presenting cells to regional lymph nodes for immunologic processing and clearance. At the same time, lymphatic channels may serve as routes for the dissemination of malignant cells, making lymphatic involvement an important determinant in staging, progression, and prognosis of respiratory tract malignancies.[6]
Nerves
The RLNs, branches of the vagus nerves, innervate the trachea. The left RLN loops around the aortic arch, lateral to the ligamentum arteriosum, before ascending within the left tracheoesophageal groove. In contrast, the right RLN courses around the right subclavian artery and ascends medially within the right tracheoesophageal groove. Both RLNs contribute parasympathetic fibers and sensory innervation to the trachea and adjacent airway structures. Parasympathetic stimulation promotes airway smooth muscle contraction and increased glandular secretion, thereby increasing intraluminal pressure and facilitating protective reflexes such as coughing. Sympathetic innervation arises from the cervical and upper thoracic ganglia of the sympathetic trunk and produces relaxation of airway smooth muscle, contributing to airway dilation and modulation of vascular tone. Autonomic pathways regulate tracheal vascular tone, glandular secretion, and trachealis muscle activity while coordinating protective airway reflexes.
Muscles
The trachealis is a smooth muscle attached to the posterior ends of the C-shaped tracheal cartilage rings. Contraction of this smooth muscle reduces tracheal diameter, increases intraluminal pressure, and facilitates expulsive airflow during coughing, an important mechanism for clearance of foreign particles. Relaxation of the trachealis muscle allows the posterior membranous wall of the trachea to move posteriorly, permitting esophageal expansion during swallowing. This configuration facilitates passage of a food bolus while maintaining airway patency through the supportive C-shaped cartilage rings.
The trachealis muscle is under autonomic nervous system control, with parasympathetic innervation derived from the vagus nerve via the RLNs. Parasympathetic stimulation causes trachealis contraction and narrowing of the tracheal lumen. Postganglionic fibers from the cervical and upper thoracic sympathetic ganglia provide sympathetic innervation. Sympathetic stimulation causes relaxation and widening of the airway.
Physiologic Variants
Failure of proper formation or fusion of the tracheoesophageal septum results in a spectrum of defects that disrupt normal separation between the ventral trachea and dorsal esophagus, leading to significant respiratory and feeding difficulties. These anomalies occur in approximately 1 in 3,000 live births worldwide.[7] Tracheoesophageal defects discussed in this activity include esophageal atresia, TEF, laryngeal tracheoesophageal cleft, tracheomalacia, and tracheal atresia.
Esophageal atresia is defined as an interruption of esophageal continuity, with or without an abnormal communication with the trachea. A TEF is an aberrant connection between the esophagus and trachea. Five anatomical variants are recognized. Type A consists of esophageal atresia without a TEF. Type B involves a proximal TEF with distal esophageal atresia. Type C consists of proximal esophageal atresia with distal TEF. Type D includes both proximal and distal TEFs with esophageal atresia. Type E, also known as the H-type, represents an isolated TEF without esophageal atresia (see Image. Types of Tracheoesophageal Fistulas). Type C is the most common variant, accounting for approximately 82% to 85% of cases. More than 67% of esophageal atresia cases are nonisolated and associated with other congenital anomalies, most commonly within the VACTERL association, which includes vertebral, anal, cardiovascular, tracheoesophageal, renal, and limb defects.[8]
Laryngeal tracheoesophageal clefts occur when the primitive foregut fails to separate into distinct tracheal and esophageal lumens, typically at the level of the larynx. This defect results in a persistent midline communication between the esophagus and the posterior wall of the larynx and trachea.
Tracheomalacia has an estimated incidence of approximately 1 in 2,100 children. The condition results from inadequate development and structural weakness of the C-shaped hyaline cartilage tracheal rings, producing a soft, excessively compliant airway.[9] Dynamic airway collapse occurs during forced expiration when intrapleural pressure becomes positive and exceeds intraluminal airway pressure. In the presence of weakened cartilage, this pressure gradient leads to excessive narrowing of the tracheal lumen.
Tracheal atresia is characterized by partial or segmental obliteration of the tracheal lumen. The anomaly occurs during the 4th week of gestation and results from failure of proper tracheal recanalization. This condition produces severe airway obstruction at birth and is often incompatible with life without immediate intervention.[10]
Surgical Considerations
A thorough understanding of tracheal anatomy and surrounding structures is essential for safe planning and performance of surgical interventions. Surgical considerations discussed in this activity include tracheostomy and tracheal tumor resection.
Tracheostomy
Tracheotomy is a surgical procedure in which an opening into the trachea, also termed a "tracheostomy," is created (see Image. Anatomy and Airway Framework of the Neck). Indications for tracheotomy include acute airway obstruction when tracheal intubation is not feasible, chronic upper airway obstructive conditions, prolonged mechanical ventilation, and planned airway management for head and neck surgeries.[11] The procedure may be performed under general anesthesia in the operating room or local anesthesia in the intensive care unit.
Cervical hyperextension is achieved by placement of a cushion under the shoulders to optimize exposure. A 3- to 4-cm horizontal arcuate incision is made approximately 2 cm above the sternal notch, traversing the skin, subcutaneous tissue, and platysma muscle. The incision is extended through the infrahyoid muscle fascia, where the anterior jugular veins may be visualized. The superficial and deep infrahyoid muscles are separated vertically until the anterior aspect of the thyroid isthmus is identified. Absence of pulsatile vessels corresponding to a high-riding brachiocephalic arterial trunk must be confirmed.
The thyroid isthmus is divided using electrocautery or scissors, with careful avoidance of excessive lateral dissection to prevent injury to the RLNs. The tracheostomy is ideally performed at the level of the 3rd and 4th tracheal rings. The 1st and 2nd tracheal rings should not be incised to avoid cannula-induced tracheitis and subsequent stricture or stenosis. The tracheostomy tube is then inserted, and the skin is approximated on each side of the cannula.
Percutaneous tracheotomy is contraindicated in cases of an enlarged thyroid isthmus (eg, goiter), malignant tumors involving the area, uncorrected coagulation disorders, inability to achieve adequate cervical extension, disruption of normal landmark anatomy (eg, in trauma), and palpation of pulsatile vessels within the tracheotomy field.[12]
Special considerations apply when performing tracheostomy in pediatric patients due to anatomical and physiological differences compared with adults. In children, the larynx is positioned higher (approximately C3–C4 rather than C4–C5), and the hyoid bone is proportionally larger than the thyroid cartilage, whereas the opposite relationship is observed in adults. The pediatric trachea is narrower and more compliant, increasing susceptibility to tracheomalacia. The supraglottis and epiglottis are more compliant in infants, increasing susceptibility to edema, and the thyrohyoid membrane is shorter. These differences make tracheal access and palpation of anatomical landmarks more challenging in pediatric patients.
Tracheal Tumor Resection
Tracheal resections are approached according to anatomical location. Lesions in the proximal 2/3 of the trachea are approached via a cervical collar incision, whereas lesions in the distal 1/3 are approached through a right thoracotomy. In the cervical collar approach, tracheal exposure is achieved through careful anterior cervical dissection following the same principles described for open tracheotomy. Before resection, a small endotracheal tube is advanced distal to the obstruction to secure ventilation.
Circumferential mobilization of the trachea is performed once the tumor or stenotic segment is identified, with avoidance of excessive lateral dissection to prevent injury to the RLNs. After resection of the involved segment, proximal and distal tracheal ends are approximated in a primary end-to-end anastomosis. Anastomosis must be tension-free to minimize the risk of dehiscence and airway compromise. A laryngeal release maneuver may be performed if additional mobilization is required, although this step is reserved for select cases due to temporary postoperative swallowing impairment of up to 3 weeks. The endotracheal tube is then advanced across the distal segment to maintain airway control during completion of the anastomosis. Final bronchoscopy is performed to inspect the anastomotic site, with revision indicated if deficiencies are identified.[13]
Accurate assessment of the location and severity of the stenosis is critical before tracheal resection. Multiplanar computed tomography scanning and rigid bronchoscopy are used to identify the lesion and define its longitudinal extent.[14] Computed tomography evaluates the relationship of the tumor to surrounding structures, while rigid bronchoscopy allows direct visualization and precise measurement from fixed landmarks such as the cricoid cartilage and carina. Measurement of proximal and distal tumor margins relative to these landmarks permits accurate calculation of tracheal length requiring resection, while ensuring sufficient residual tracheal length for a tension-free anastomosis. Knowledge of adjacent anatomy is essential, as RLNs ascend in the tracheoesophageal grooves and pass posterior to the cricoid cartilage. Therefore, complete cricoid resection is not feasible without risking bilateral nerve injury and loss of protective laryngeal function.
Clinical Significance
A thorough understanding of upper airway and tracheal anatomy is critical for recognizing life-threatening conditions and guiding safe clinical interventions. Foreign body aspiration (FBA) often produces tracheobronchial obstruction and is primarily a clinical diagnosis, as chest radiographs may appear normal within the first 24 hours, and many aspirated objects are radiolucent. Clinically, FBA presents with coughing, wheezing, and unilaterally diminished breath sounds, reflecting asymmetric bronchial obstruction. This pattern is explained by airway anatomy. The right main bronchus is wider, shorter, and more vertical than the left, making the right main bronchus the most frequent site of impaction.
In children, additional anatomical and physiological features increase the risk and severity of obstruction, including a higher laryngeal position, a smaller tracheal diameter, a weaker cough reflex, immature swallowing coordination, and a relatively wider right main bronchus.[15] Recognition of these anatomical relationships allows rapid localization of obstruction, even when imaging is inconclusive. Timely bronchoscopy is facilitated by accurate localization and prevents hypoxia or respiratory failure. This anatomic configuration also explains the higher incidence of inadvertent right mainstem intubation in pediatric patients.[16]
Another clinically important manifestation of airway compromise is stridor, a high-pitched sound generated by turbulent airflow through a narrowed lumen. Stridor is typically inspiratory but may become biphasic or expiratory in severe obstruction.[17] In mild cases, stridor may occur only during increased respiratory effort, such as crying or physical exertion. Persistent biphasic stridor, loud stridor, abdominal retractions, or sudden decreases in lung volumes indicate fixed obstruction at the level of the glottis, subglottis, or trachea and require urgent evaluation.[18] FBA and stridor both illustrate how anatomical knowledge enables rapid recognition of airway compromise, facilitating timely intervention prior to imaging confirmation.
Tension pneumothorax is another critical airway-related emergency. Increased intrapleural pressure collapses the affected lung and shifts mediastinal structures, producing contralateral compression, hemodynamic instability, and tracheal deviation (see Image. Right Tension Pneumothorax Radiograph). Clinical signs, including hypoxia, respiratory distress, unilaterally absent breath sounds, and jugular venous distention, reflect mediastinal displacement. These findings often precede radiographic confirmation, making prompt recognition based on physical examination and anatomical understanding essential. Delays in diagnosis, particularly in mechanically ventilated patients, are associated with significantly increased mortality. Current guidelines recommend emergent needle or tube thoracostomy for suspected tension pneumothorax prior to imaging, emphasizing symptom-based assessment in life-threatening scenarios.[19]
Anatomical knowledge is essential for safe surgical airway procedures. The first 2 tracheal rings should be avoided during tracheostomy, as incision at this level may cause subglottic stenosis or strictures secondary to cannula-induced tracheitis. In addition, the RLNs ascend within the tracheoesophageal grooves and pass posterior to the cricoid cartilage, requiring dissection to remain strictly midline and below the C6 level. Injury to these nerves may result in dysphagia and hoarseness if unilateral, or severe airway compromise with loss of protective laryngeal reflexes if bilateral.
These examples demonstrate that detailed knowledge of tracheal and mediastinal anatomy is essential for timely diagnosis, accurate localization of pathology, and safe surgical management. From foreign body obstruction and stridor to tension pneumothorax and operative airway procedures, anatomical understanding enables rapid interpretation of symptoms and effective intervention.
Media
(Click Image to Enlarge)
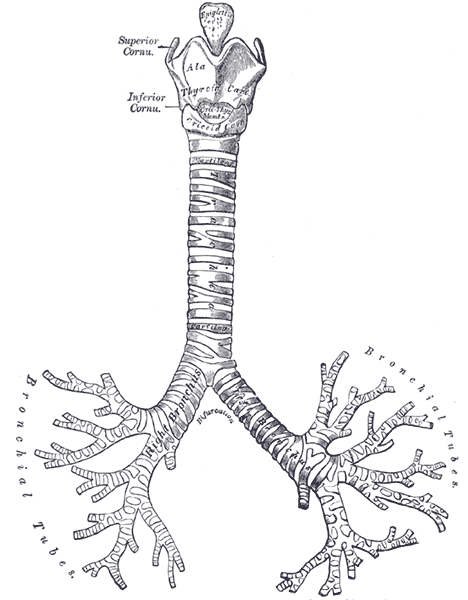
Anatomy of the Tracheobronchial Tree. This anterior view illustrates the continuity of the respiratory passage from the larynx to the distal bronchial tubes. Labels identify the thyroid and cricoid cartilages, the C-shaped tracheal rings, and the bifurcation into the right and left primary bronchi.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
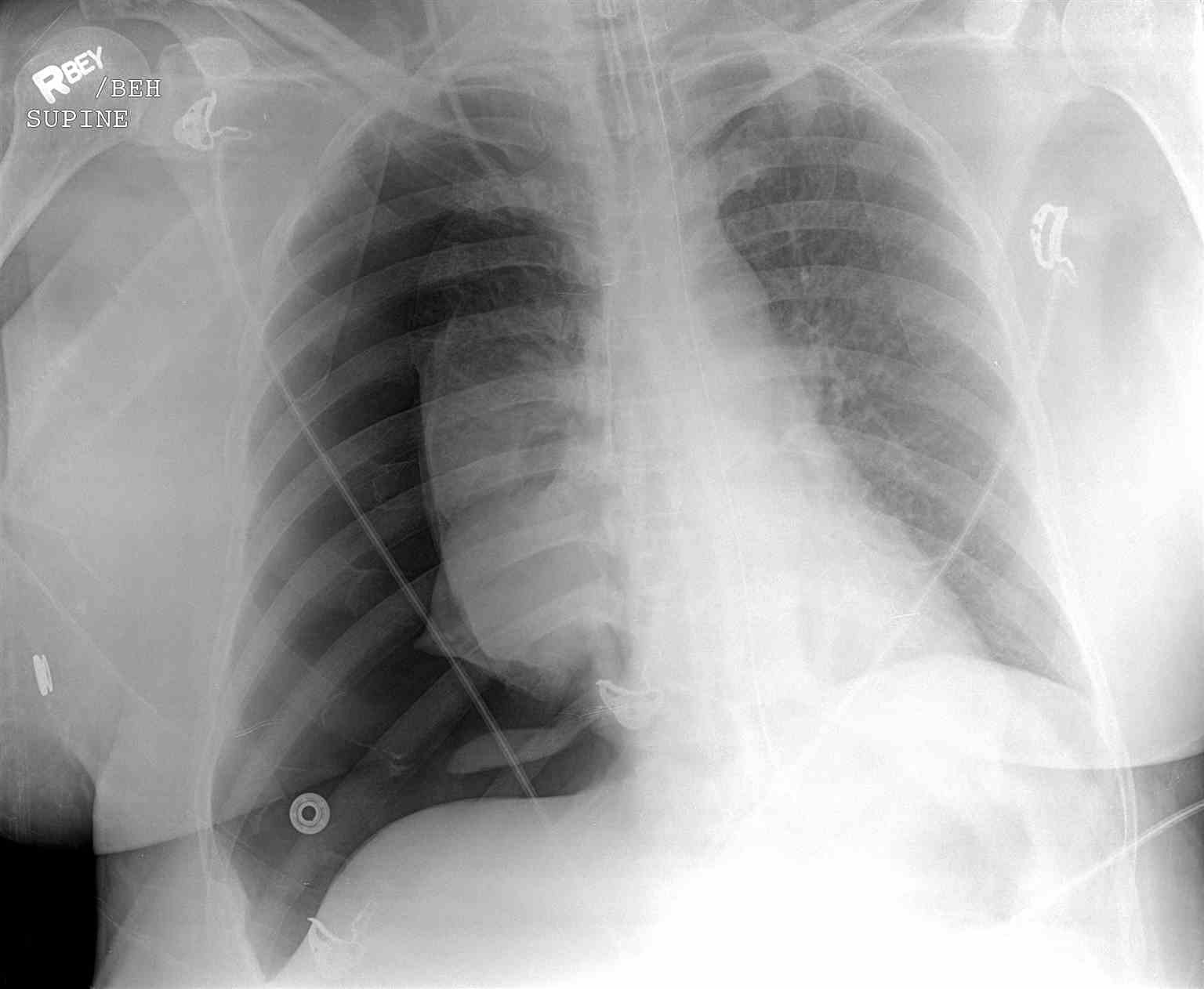
Right Tension Pneumothorax Radiograph. This image shows absent lung markings on the lateral side of the right pleural cavity and a collapsed right lung. The trachea and heart are displaced toward the left, indicating a mediastinal shift.
Contributed by S Dulebohn, MD
(Click Image to Enlarge)
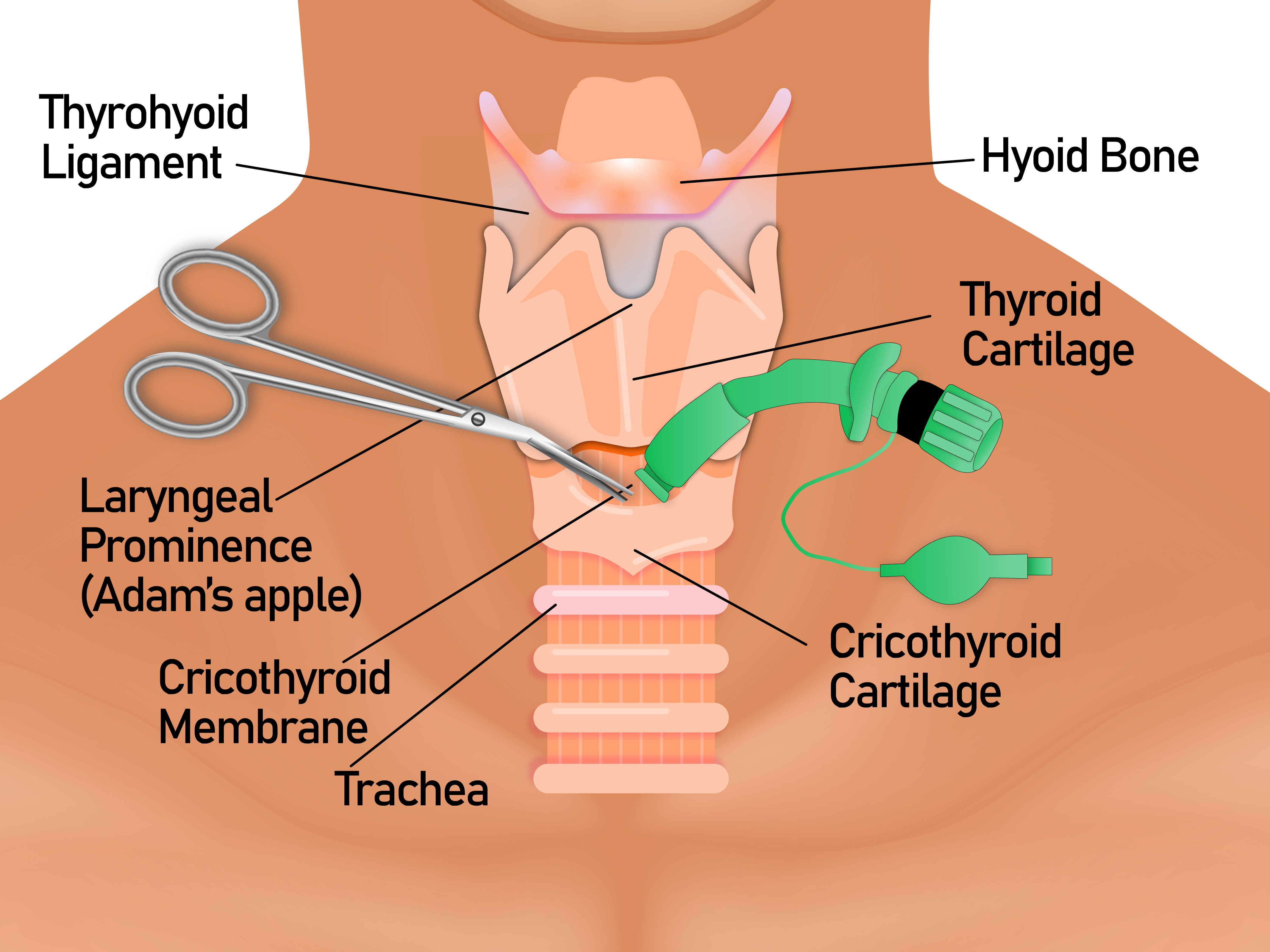
Anatomy and Airway Framework of the Neck. This image illustrates the anatomy and the framework of the airway in the neck region. The cricothyroid membrane is located between the thyroid cartilage superiorly and the cricoid cartilage inferiorly. The cricothyroid membrane must be identified by palpation of the surrounding cartilaginous structures.
Contributed by A Tariq, MD
(Click Image to Enlarge)
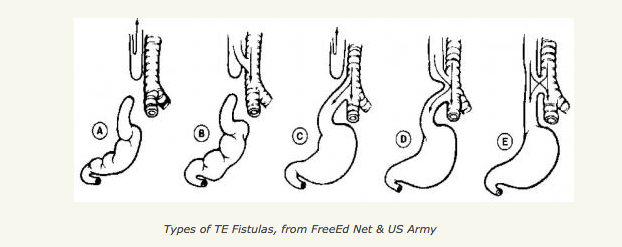
Types of Tracheoesophageal Fistulas. This image illustrates the anatomical differences between various tracheoesophageal fistula subtypes and associated esophageal atresia configurations. The 5 labeled diagrams (A-E) detail connections between the upper pouch, lower pouch, trachea, and the presence or absence of a central fistula.
Free-Ed.Net & The US Army
(Click Image to Enlarge)
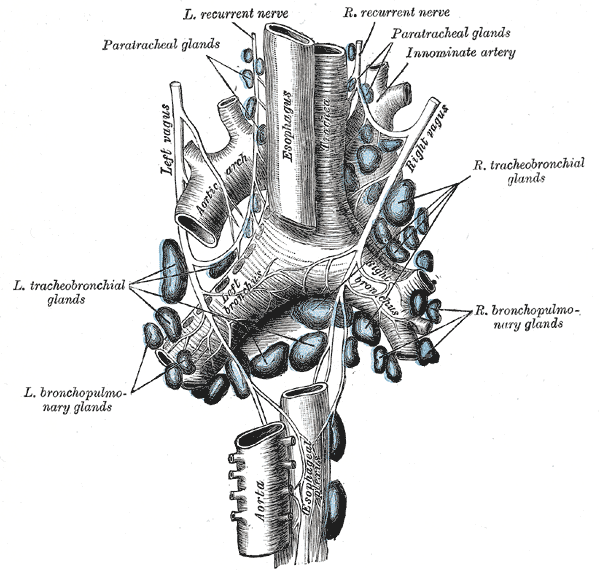
Lymphatics and Neurovascular Relations of the Trachea. This illustration details the extensive lymphatic network of the airway, including the paratracheal, tracheobronchial, and bronchopulmonary glands. The image also identifies the spatial relationship between these nodes and major structures such as the aortic arch, innominate artery, esophagus, and the left and right vagus and recurrent nerves. Other labeled structures include the descending aorta and the branching of the trachea into the left and right primary bronchi.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
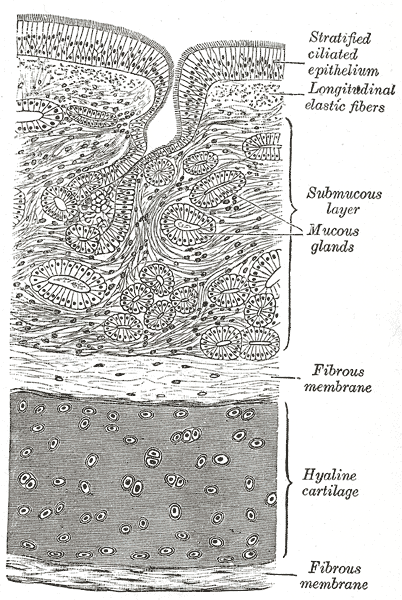
Transverse Section of the Tracheal Wall. This histological illustration delineates the various layers of the trachea, beginning with the luminal stratified ciliated epithelium and underlying longitudinal elastic fibers. The deep structure includes the submucous layer containing mucous glands, supported by a thick band of hyaline cartilage between 2 layers of fibrous membrane.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
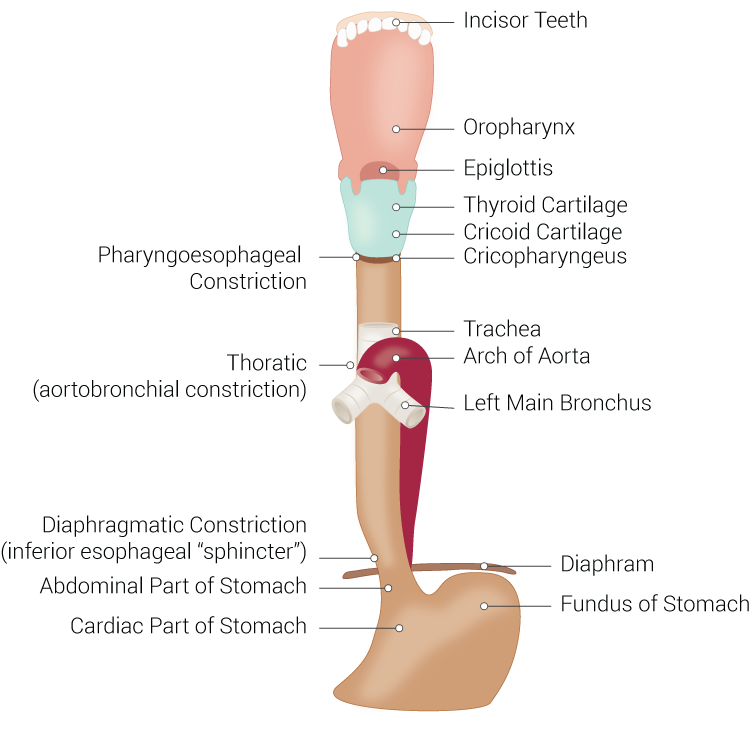
Digestive and Respiratory Structures Anatomically Related to the Esophagus. This illustration shows the esophagus and adjacent digestive and respiratory structures, including the incisors, oropharynx, laryngeal cartilages, trachea, aortic arch, bronchi, diaphragm, stomach, and esophageal constrictions.
Illustrated by B Palmer
References
McCullagh KL, Shah RN, Huang BY. Anatomy of the Larynx and Cervical Trachea. Neuroimaging clinics of North America. 2022 Nov:32(4):809-829. doi: 10.1016/j.nic.2022.07.011. Epub [PubMed PMID: 36244725]
Bustamante-Marin XM, Ostrowski LE. Cilia and Mucociliary Clearance. Cold Spring Harbor perspectives in biology. 2017 Apr 3:9(4):. doi: 10.1101/cshperspect.a028241. Epub 2017 Apr 3 [PubMed PMID: 27864314]
Level 3 (low-level) evidenceHawkins FJ, Suzuki S, Beermann ML, Barillà C, Wang R, Villacorta-Martin C, Berical A, Jean JC, Le Suer J, Matte T, Simone-Roach C, Tang Y, Schlaeger TM, Crane AM, Matthias N, Huang SXL, Randell SH, Wu J, Spence JR, Carraro G, Stripp BR, Rab A, Sorsher EJ, Horani A, Brody SL, Davis BR, Kotton DN. Derivation of Airway Basal Stem Cells from Human Pluripotent Stem Cells. Cell stem cell. 2021 Jan 7:28(1):79-95.e8. doi: 10.1016/j.stem.2020.09.017. Epub 2020 Oct 23 [PubMed PMID: 33098807]
Shivaraju M, Chitta UK, Grange RMH, Jain IH, Capen D, Liao L, Xu J, Ichinose F, Zapol WM, Mootha VK, Rajagopal J. Airway stem cells sense hypoxia and differentiate into protective solitary neuroendocrine cells. Science (New York, N.Y.). 2021 Jan 1:371(6524):52-57. doi: 10.1126/science.aba0629. Epub [PubMed PMID: 33384370]
Panda N, Auchincloss HG. Anatomy of the Trachea. Thoracic surgery clinics. 2025 Feb:35(1):1-10. doi: 10.1016/j.thorsurg.2024.08.003. Epub 2024 Oct 15 [PubMed PMID: 39515887]
Sah B, Jaiswal LS. Foreign body aspiration with iatrogenic right bronchus perforation - A case report and literature review. International journal of surgery case reports. 2024 Mar:116():109404. doi: 10.1016/j.ijscr.2024.109404. Epub 2024 Feb 15 [PubMed PMID: 38364753]
Level 3 (low-level) evidenceEdwards NA, Shacham-Silverberg V, Weitz L, Kingma PS, Shen Y, Wells JM, Chung WK, Zorn AM. Developmental basis of trachea-esophageal birth defects. Developmental biology. 2021 Sep:477():85-97. doi: 10.1016/j.ydbio.2021.05.015. Epub 2021 May 21 [PubMed PMID: 34023332]
Galarreta CI, Vaida F, Bird LM. Patterns of malformation associated with esophageal atresia/tracheoesophageal fistula: A retrospective single center study. American journal of medical genetics. Part A. 2020 Jun:182(6):1351-1363. doi: 10.1002/ajmg.a.61582. Epub 2020 Apr 6 [PubMed PMID: 32250545]
Level 2 (mid-level) evidenceDurkin N, De Coppi P. Anatomy and embryology of tracheo-esophageal fistula. Seminars in pediatric surgery. 2022 Dec:31(6):151231. doi: 10.1016/j.sempedsurg.2022.151231. Epub 2022 Nov 17 [PubMed PMID: 36459913]
Pfeifer M, Rehder H, Gerykova Bujalkova M, Bartsch C, Fritz B, Knopp C, Beckers B, Dohle F, Meyer-Wittkopf M, Axt-Fliedner R, Beribisky AV, Hofer M, Laccone F, Schoner K. Tracheal agenesis versus tracheal atresia: anatomical conditions, pathomechanisms and causes with a possible link to a novel MAPK11 variant in one case. Orphanet journal of rare diseases. 2024 Mar 12:19(1):114. doi: 10.1186/s13023-024-03106-z. Epub 2024 Mar 12 [PubMed PMID: 38475835]
Level 3 (low-level) evidenceRosero EB, Corbett J, Mau T, Joshi GP. Intraoperative Airway Management Considerations for Adult Patients Presenting With Tracheostomy: A Narrative Review. Anesthesia and analgesia. 2021 Apr 1:132(4):1003-1011. doi: 10.1213/ANE.0000000000005330. Epub [PubMed PMID: 33369928]
Level 3 (low-level) evidenceGaubert N, Crambert A, Malgras B. Surgical tracheotomy. Journal of visceral surgery. 2021 Feb:158(1):69-74. doi: 10.1016/j.jviscsurg.2020.10.002. Epub 2020 Oct 22 [PubMed PMID: 33268320]
Saetti R, Ronzani G, Meneghesso S, Silvestrini M. Operative technique: Tracheal resection and anastomosis in a revision surgery. Head & neck. 2023 Oct:45(10):2730-2734. doi: 10.1002/hed.27468. Epub 2023 Jul 21 [PubMed PMID: 37477351]
Allen MS. Surgery of the Trachea. The Korean journal of thoracic and cardiovascular surgery. 2015 Aug:48(4):231-7. doi: 10.5090/kjtcs.2015.48.4.231. Epub 2015 Aug 5 [PubMed PMID: 26290833]
Sai Akhil R, Priya TG, Behera BK, Biswal B, Swain SK, Rath D, Mohanty MD, Choudhury J. Clinico-Radiological Profile and Outcome of Airway Foreign Body Aspiration in Children: A Single-Center Experience From a Tertiary Care Center in Eastern India. Cureus. 2022 Feb:14(2):e22163. doi: 10.7759/cureus.22163. Epub 2022 Feb 13 [PubMed PMID: 35308662]
Zidar N, Gale N. Update from the 5th Edition of the World Health Organization Classification of Head and Neck Tumors: Hypopharynx, Larynx, Trachea and Parapharyngeal Space. Head and neck pathology. 2022 Mar:16(1):31-39. doi: 10.1007/s12105-021-01405-6. Epub 2022 Mar 21 [PubMed PMID: 35312977]
Pfleger A, Eber E. Assessment and causes of stridor. Paediatric respiratory reviews. 2016 Mar:18():64-72. doi: 10.1016/j.prrv.2015.10.003. Epub 2015 Oct 23 [PubMed PMID: 26707546]
Patnaik S, Zacharias G, Jain MK, Samantaray KK, Surapaneni SP. Etiology, Clinical Profile, Evaluation, and Management of Stridor in Children. Indian journal of pediatrics. 2021 Nov:88(11):1115-1120. doi: 10.1007/s12098-021-03722-8. Epub 2021 Mar 17 [PubMed PMID: 33728566]
Roberts DJ, Leigh-Smith S, Faris PD, Ball CG, Robertson HL, Blackmore C, Dixon E, Kirkpatrick AW, Kortbeek JB, Stelfox HT. Clinical manifestations of tension pneumothorax: protocol for a systematic review and meta-analysis. Systematic reviews. 2014 Jan 4:3():3. doi: 10.1186/2046-4053-3-3. Epub 2014 Jan 4 [PubMed PMID: 24387082]
Level 1 (high-level) evidence