Introduction
Ingrown toenail, also known as onychocryptosis or paronychia, is a common nail problem encountered in podiatry, general family practice, and dermatology, accounting for approximately 20% of foot problems seen in primary care clinics (see Image. Ingrown Toenail).[1] An ingrown toenail occurs when the nail plate grows into the periungual skin, causing inflammation and may lead to infection. This may be the medial, lateral, or proximal nail folds. An ingrown toenail causes considerable pain, discomfort, and disability if left untreated.
An ingrown toenail may present at any age, but commonly affects teenagers and young adults (see Images. Ingrown Toenail, Adolescent Type, and Neonatal Ingrown Nails). The hallux nail unit is the most common anatomic site for ingrown toenails, accounting for approximately 80% of cases (see Image. Ingrowing Nail, Medial Border of the Left Hallux).[2] Management options range from conservative treatments and minor procedures to more invasive surgical interventions, depending on the severity and the stage of the condition.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Improper nail trimming and inadequate foot hygiene represent the most common etiologic factors in the development of ingrown toenails, as they may result in the formation of a nail spicule that penetrates adjacent periungual soft tissue, predisposing to localized inflammation and secondary bacterial infection.[2][3] Other predisposing factors for ingrown toenails include tight-fitting shoes, hyperhidrosis, trauma, digital deformities, eg, hallux valgus (also known as bunions), and hammertoes with increased interdigital pressure, incurvated nail shape either from genetic or underlying bone developments (eg, subungual exostoses), and some medications (eg, epidermal growth factor receptor inhibitors and chemotherapy medications (gefitinib, cetuximab)).[4] Obesity can potentially exacerbate onychocryptosis by contributing to greater soft tissue mass throughout the body, particularly in the lower extremities. This can mimic periungual hypertrophy and exacerbate constriction from footwear. Similarly, diabetes, as well as thyroid, cardiac, and renal disorders, can increase lower extremity edema mimicking the effect of obesity on the nail unit.[5]
The possible involvement of intrinsic risk factors in the pathogenesis of ingrown toenails, eg, abnormal nail shape and anatomical abnormalities, has been widely debated. Some studies have found that pincer-nail deformity (see Image. Pincer Nails in a Female Patient), wide nail plates, congenital malalignment of the toenails, and thickening of the nail plate are possible risk factors for ingrown toenails.[3][6] Other literature suggests that bony abnormalities that increase internal pressure within the ankle, foot, or toe might contribute to the development of ingrown toenails.[1][7] However, more recent studies suggest no difference in the prevalence of anatomical abnormalities between patients with ingrown toenails and controls when proper footwear accommodation is implemented.[8]
Epidemiology
Few investigations of the epidemiology of ingrown toenails have been conducted. Previous studies have reported a prevalence of 2.5% to 5%.[7] The incidence and prevalence of ingrown toenails have increased in recent years, likely due to enhanced health literacy, and may also be related to lifestyle changes, eg, increased physical activity.
The incidence peaks in adolescence and early adulthood, with a clear male predominance, characterized by an approximate male-to-female ratio of 2:1. Ingrown toenails predominantly affect the hallux nail matrix and can involve 1 or more nail edges. Involvement of the lateral nail fold occurs approximately twice as frequently as the medial aspect, likely secondary to repetitive interdigital friction and compressive forces between adjacent toes.[7][9]
Pathophysiology
Many theories have been proposed to explain the onset of ingrown toenails. One assumption is that ingrown toenails are related to excess hypertrophic skin surrounding the nail. This is explained by wide lateral tissue tending to bulge around the nail, leading to pressure and necrosis (see Image. Ingrown Toenail, Necrosis).[10] However, the most widely accepted theory is that an ingrown toenail occurs when the nail plate edge grows into the overlapping lateral nail fold, with hyperkeratosis or hypertrophic changes in the skin, causing painful inflammation and the formation of hypergranulation tissue, often referred to as a pyogenic granuloma.[9][10] Reactive ground forces from athletic activity, obesity, warm and humid environments, and constricting footwear may increase the risk of ingrown nails.[2]
Histopathology
Histopathologic evaluation of ingrown toenails demonstrates epithelial disruption at the lateral nail fold with penetration of a nail spicule into the periungual soft tissue. This inciting mechanical insult results in an acute inflammatory infiltrate composed predominantly of neutrophils, often accompanied by edema and focal ulceration of the overlying epidermis. In chronicity, granulation tissue development is characterized by capillary proliferation, fibroblast activation, and a mixed inflammatory cell infiltrate. Long-standing lesions may additionally demonstrate epithelial hyperplasia and fibrosis of the surrounding nail fold.[11]
History and Physical
Patients with ingrown toenails most commonly present with localized pain along the lateral nail fold, exacerbated by shoe wear, ambulation, or direct pressure. The history frequently includes improper nail trimming, recent trauma, repetitive athletic activity, or the use of constrictive footwear. Patients may also report progressive swelling, erythema, drainage, or prior similar episodes. In advanced cases, symptoms of secondary infection, eg, purulent discharge or malodor, may be present.[9]
Physical examination typically demonstrates tenderness to palpation along the affected nail border, with visible penetration of the nail plate into the periungual soft tissue. Early findings include mild erythema and edema of the lateral nail fold. As the condition progresses, granulation tissue, hypertrophy of the nail fold, and seropurulent drainage may be observed. Assessment should also evaluate for surrounding cellulitis, fluctuance suggestive of abscess, and risk factors, eg, diabetes or peripheral vascular disease.
Ingrown Toenail Staging
Clinical staging is most commonly performed using the following Heifetz classification system:
- Stage I: mild erythema, edema, and pain without purulence
- Stage II: increased inflammation with drainage and infection
- Stage III: chronic inflammation with granulation tissue formation and hypertrophy of the lateral nail fold [12][13]
The following additional classification system has been described by Kline et al:
- Stage 1: local irritation; no infection, pus, or granulation tissue
- Stage 2: infection without a history of onychocryptosis; pus and/or granulation tissue are present
- Stage 3: Infection with a history of more than one episode of onychocryptosis; pus and granulation tissue are present
- Stage 4: Infective onychocryptosis with partial onycholysis of a single nail border
- Stage 5: Infective onychocryptosis with partial onycholysis of both nail borders [14]
Evaluation
The diagnosis of an ingrown toenail is classically based on clinical features, but may require bacterial culture or standard radiographic evaluation if deeper infection of soft tissue or underlying bone is suspected. If physical examination reveals an abnormal nail shape consistent with subungual pathology, an x-ray examination may be used to rule out subungual or periungual exostosis. In rare cases, if the standard radiograph reveals bone pathology consistent with infection, an MRI may be ordered to rule out concomitant osteomyelitis.
Treatment / Management
The natural history of untreated ingrown toenails is poorly supported by data, and no consensus on the best treatment technique exists.
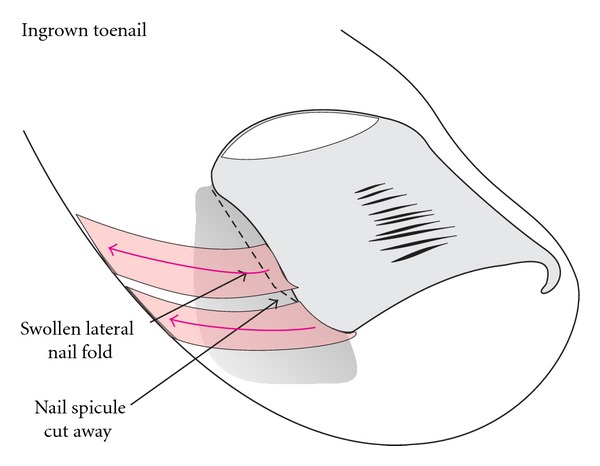
General Conservative Measures
General measures for ingrown toenails include education on proper footwear and correct nail debridement: avoiding aggressive cutting of the lateral and distal margins of the nail plate (see Images. Schematic illustration of Taping, Ingrown Toenail, Packing, and Ingrown Toenail, Gutter Treatment). Simple nonsurgical palliative measures include correcting inappropriate footwear, managing hyperhidrosis and onychomycosis, soaking the affected toe, followed by applying a mid- to high-potency topical steroid, and placing wisps of cotton or dental floss under the ingrown lateral nail edge (see Images. Lateral Ingrown Toenail With Granulation, and Toenails, Onychogryphosis and Malalignment).[15] The application of topical steroids to hypertrophic granulation tissue may decrease inflammation.[10][16] Granulomatous tissue may also be treated with silver nitrate to reduce hypergranulation and excessive bleeding.
In cases of minor infection, including associated cellulitis or abscess formation, and in patients with high-risk comorbidities (eg, diabetes, immunosuppression), antibiotics (oral or topical) should be administered. Recent studies have concluded that polymicrobial infection/colonization is present in most ingrown nails in the fingers and toes. The most commonly cultured microorganisms were Enterococcus faecalis (14%), Staphylococcus aureus (12%), Candida albicans (9%), Enterobacter cloacae (8%), and Klebsiella pneumoniae (7%). Most cultured bacteria belonged to the Enterobacteriaceae family (36%), while other cultured bacteria included Staphylococci (26%), Enterococci (16%), Candida species (14%), and gram-negative non-fermenting bacilli (8%).[17]
The color of the nail may assist in antibiotic treatment, with green often associated with Pseudomonas species. The most common antibiotics used to treat would include gram-positive coverage with some gram-negative coverage. A history of resistant bacterial infection may guide antibiotic coverage. Topical mupirocin or oral methicillin-resistant Staphylococcus aureus (MRSA) coverage would be indicated in these cases.
Patient history of diabetes, peripheral vascular disease, or autoimmune dysfunction should be taken into consideration. Use of topical or oral anti-inflammatories, a short course of oral non-steroidal anti-inflammatory drugs (NSAIDs), or steroids may help reduce the hyperinflammatory component of this condition, with or without surgical intervention. Pulsed dye laser (PDL) therapy at 595 nm, with vascular-targeting and anti-inflammatory effects, may serve as an effective adjunctive treatment.[18]
Surgical Techniques
Surgical procedures for ingrown toenails are performed under local anesthesia. Various techniques for local anesthesia exist, including digital block and metatarsal blocks. Local anesthetics (lidocaine and marcaine are most commonly used) in 0.25% to 2% concentrations can be used alone or in combination. Indications for local anesthesia depend mainly on the type of procedure and the clinician's preference. Epinephrine may be added to the local anesthetic solution to minimize bleeding; commonly used concentrations include 1:200,000 or 1:400,000, prepared by combining a plain anesthetic agent with a formulation containing premixed epinephrine.
Surgical options for ingrown toenails include:
- Spicule excision and partial surgical matricectomy: This consists of excising the affected nail portion with a partial mechanical matricectomy.[19] (B2)
- Chemical partial matricectomy: Chemical matricectomy is commonly performed using 89% phenol (care must be taken, as this agent is highly flammable and will affect any skin surface). This procedure demonstrates a higher success rate and is less painful than mechanical/surgical matricectomy, and its success depends on good hemostasis. Other chemical agents, eg, sodium hydroxide and trichloroacetic acid, can be employed.[20] (A1)
- Wedge resection of the toenail and nail fold: This approach consists of the excision of the affected portion of the nail plate, partial matrixectomy, and wedge dissection of the nail bed and the hypertrophic nail fold. Clinicians should generally avoid this technique unless other methods have failed (see Image. Wedge Excisions).
- Excision of the affected nail and total matricectomy: This is a more invasive treatment for ingrown toenails and includes excision of the affected nail and nail bed, with a total matricectomy (chemical or mechanical/surgical). This procedure is indicated for stage IV ingrown toenails, onychogryphosis, onychodystrophy, and recurrence.
- Soft-tissue nail fold excision technique: This procedure does not touch the nail; the nail is theorized not to be the causative factor in developing ingrown toenails. This procedure consists of a wide excision of the soft tissue on the medial and/or lateral nail folds.[21][22] (B2)
- Other techniques: Newer techniques, including electrocautery, radiofrequency ablation, and carbon dioxide laser ablation, have become the newest form of ingrown toenail management.[3][10][23]
Surgical treatment options for ingrown toenails are numerous, and little consensus exists on the technique of choice, except that removal of enough nail and tissue to ensure a low rate of recurrence is preferred. The ideal procedure should lead to the best functional and aesthetic outcome (see Images. Fusiform Excision, Matrix Horn Resection, Lateral Matrix Horns, Lateral Matrix Horn Phenolization, and Phenolization, Lateral Matrix Horn).
Prior studies have concluded that antibiotic treatment and simple nail avulsions, partial or complete without matrixectomy, lead to high recurrence rates, while phenol or surgical matrixectomy has shown greater success. Ultimately, the patient and treating clinician must weigh the benefits of any treatment plan together. Consideration of microscopic biopsy analysis is advisable in any recurrent or nonhealing case.
Differential Diagnosis
Differential diagnosis includes hallux extensus (ski jump hallux at the interphalangeal joint), subungual exostosis, osteochondroma, and tumors of the nail bed or nail folds (benign and malignant). If suspected, an x-ray examination that reveals the subungual bony proliferation can confirm the diagnosis of subungual bone tumor or distant trauma with hypertrophic remodeling. Malignant tumors to consider are subungual melanoma, including amelanotic melanoma and subungual squamous cell carcinoma, which can be locally aggressive.[2][10][24][25][26][27][28][29][30]
Prognosis
Recurrences can occur following all the abovementioned procedures; they result from incomplete matricectomy and regrowth of a spicule from the lateral horn. Simple nail avulsion has the highest recurrence rate (70%). Chemical matricectomy and laser matricectomy showed lower recurrence rates than mechanical matricectomy.[13]
Complications
Secondary infection of the nail fold, paronychia, and scarring of the nail fold are essential to consider and treat.
Deterrence and Patient Education
By far the most important part of education is informing the patient as to the etiology and pathogenesis of the condition. The most common form of ingrown nail is distal ingrowing. The pathogenesis is usually a wide, relatively markedly curved nail plate, the distal lateral corners of which have been cut obliquely, leaving a tiny spicule that digs into the lateral nail groove and finally pierces the epidermis when the nail grows forward.
This causes a foreign-body reaction with inflammation, granulation tissue, secondary bacterial colonization, and, eventually, infection. Precipitating factors include narrow, pointed shoes, tight socks, hyperhidrosis, juvenile diabetes mellitus, and more. In the most common form, ingrowing usually starts at the distal end of one or both of the lateral nail grooves. The tip of the toe is compressed in a narrow-tipped shoe, and when the nail is cut short or the distal corner has been cut off, the distal nail bed is allowed to shrink so that not enough space is present for the regrowing wide nail. It pushes on the soft tissue, which may first react with a circumscribed, usually painful hyperkeratosis called onychophosis. The patient tries to relieve the discomfort by cutting more of the nail corner; however, to cut the nail smoothly, the patient would have to insert the tip of the scissors deeper, which would require piercing the soft tissue. This is painful and, therefore, typically not done, leaving a hook-like piece of the lateral border. When the nail grows out, the hook pierces into the nail groove, causing even more pain. A vicious cycle of pain, attempts to relieve it, wrong nail cutting, and aggravating the condition is initiated.[23]
Finally, letting the patient know that the clinician wants to help and that they are welcome to return for treatment reduces hesitancy about treatment and the incidence of future ingrown nails.
Enhancing Healthcare Team Outcomes
Ingrown toenail, or onychocryptosis, is a common nail disorder in which the nail plate penetrates the periungual soft tissue, resulting in inflammation, pain, infection, and functional impairment. The condition most frequently affects the hallux and commonly develops due to improper nail trimming, constrictive footwear, trauma, hyperhidrosis, obesity, or structural nail abnormalities. Clinical findings range from mild erythema and edema to granulation tissue formation, hypertrophy of the nail fold, purulent drainage, and recurrent infection. Evaluation relies primarily on clinical examination and staging systems that guide treatment selection, while imaging or microbiologic studies may be indicated when osteomyelitis, abscess formation, or subungual pathology is suspected. Management includes conservative measures, topical or systemic therapies, and surgical interventions such as partial matricectomy or phenolization to reduce recurrence and preserve nail function.
Interprofessional collaboration improves outcomes by promoting timely diagnosis, coordinated treatment, prevention of complications, and longitudinal follow-up. Physicians, podiatrists, dermatologists, primary care clinicians, and advanced practitioners perform diagnostic evaluation, determine disease severity, manage comorbidities, and select appropriate medical or surgical interventions. Nurses reinforce wound care instructions, monitor healing, identify signs of infection, and support patient adherence to preventive strategies. Pharmacists optimize antimicrobial and anti-inflammatory therapy, assess for medication interactions, and counsel patients regarding appropriate medication use. Radiologists and laboratory personnel assist with diagnostic imaging and culture interpretation when deeper infection or atypical pathology is suspected. Coordinated communication among team members supports shared decision-making, timely referral for recurrent or severe disease, risk factor modification, and the prevention of complications such as chronic infection, nail deformity, cellulitis, or osteomyelitis.
Media
(Click Image to Enlarge)

Ingrown Toenail. An ingrown toenail occurs when the nail plate grows into the periungual skin and causes inflammation and infection. It can cause considerable pain, discomfort, and disability if left untreated.
(Click Image to Enlarge)
Ingrown Toenail, Adolescent Type. Schematic illustration of the adolescent type of ingrown nail. (a) Oblique view. (b) Dorsal view.
Haneke E. Controversies in the treatment of ingrown nails Dermatol Res Pract. 2012;2012:783924. doi: 10.1155/2012/783924.
(Click Image to Enlarge)
Neonatal Ingrown Nails.
Haneke E. Controversies in the treatment of ingrown nails. Dermatol Res Pract. 2012;2012:783924. doi: 10.1155/2012/783924.
(Click Image to Enlarge)

Ingrowing Nail, Medial Border of the Left Hallux. The image shows an ingrowing nail on the medial border of the left hallux.
Contributed by MA Dreyer, DPM, FACFAS
(Click Image to Enlarge)

Pincer Nails in a Female Patient. (a) Frontal view, (b) Dorsal view, (c), X-ray dorsal view of the distal phalanges shows the lateral deviation of the terminal phalanges and the medial hook-like exostoses at the base of the bone. (d), X-ray lateral view demonstrates the distal dorsal traction osteophyte.
Haneke E. Controversies in the treatment of ingrown nails. Dermatol Res Pract. 2012;2012:783924. doi: 10.1155/2012/783924.
(Click Image to Enlarge)

Ingrown Toenail, Necrosis. Image of a 16-year-old boy 4 years after a wedge excision, which had been complicated by infection and necrosis of the lateral nail fold. There is considerable malalignment to the side of the necrosis.
Haneke E. Controversies in the treatment of ingrown nails. Dermatol Res Pract. 2012;2012:783924. doi: 10.1155/2012/783924.
(Click Image to Enlarge)
Schematic illustration of Taping.
Haneke E. Controversies in the treatment of ingrown nails. Dermatol Res Pract. 2012;2012:783924. doi: 10.1155/2012/783924.
(Click Image to Enlarge)
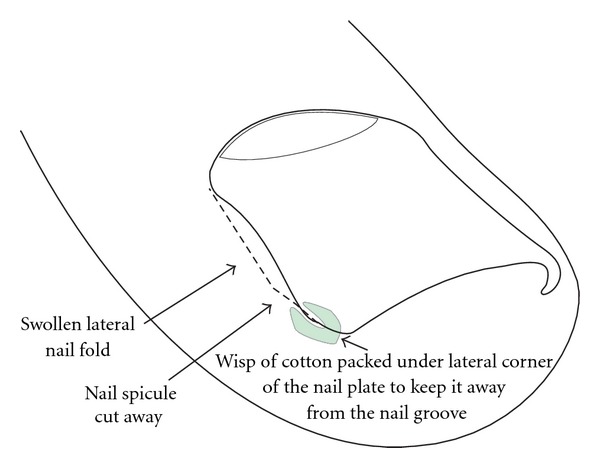
Ingrown Toenail, Packing.
Haneke E. Controversies in the treatment of ingrown nails. Dermatol Res Pract. 2012;2012:783924.
(Click Image to Enlarge)
Ingrown Toenail, Gutter Treatment.
Haneke E. Controversies in the treatment of ingrown nails. Dermatol Res Pract. 2012;2012:783924. doi: 10.1155/2012/783924.
(Click Image to Enlarge)

Lateral Ingrown Toenail With Granulation. This image is a laterally ingrown nail with granulation tissue in a 15-year-old male patient.
Haneke E. Controversies in the treatment of ingrown nails. Dermatol Res Pract. 2012;2012:783924. doi: 10.1155/2012/783924.
(Click Image to Enlarge)

Toenails, Onychogryphosis and Malalignment. Toenails of a 38-year-old female patient, 16 years after bilateral wedge excisions for ingrown nails, showing onychogryphosis and malalignment. (a) Right foot, (b) Left foot.
Haneke E. Controversies in the treatment of ingrown nails. Dermatol Res Pract. 2012;2012:783924. doi: 10.1155/2012/783924.
(Click Image to Enlarge)
Wedge Excisions. Schematic illustration of how wedge excisions are most commonly performed. The wedge is wide in the middle of the lateral nail fold, but the lateral matrix horn is not completely excised. (a) transverse section at the level of the midnail bed, (b) transverse section at the level of the matrix horns.
Haneke E. Controversies in the treatment of ingrown nails. Dermatol Res Pract. 2012;2012:783924. doi: 10.1155/2012/783924.
(Click Image to Enlarge)
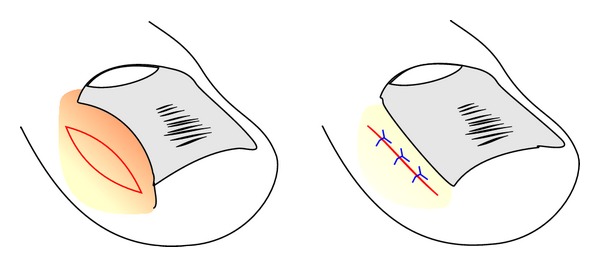
Fusiform Excision. Schematic illustration of the reduction of a hypertrophic lateral nail fold by a fusiform excision.
Haneke E. Controversies in the treatment of ingrown nails. Dermatol Res Pract. 2012;2012:783924. doi: 10.1155/2012/783924.
(Click Image to Enlarge)
Matrix Horn Resection. The schematic illustrates a selective lateral matrix horn resection.
Haneke E. Controversies in the treatment of ingrown nails. Dermatol Res Pract. 2012;2012:783924. doi: 10.1155/2012/783924.
(Click Image to Enlarge)

Lateral Matrix Horns. This image depicts the proximal lateral and medial nail portions corresponding to the lateral matrix horns. The lateral nail strips have been separated from the nail bed, and the most proximal-lateral corners of the nail are elevated to show its true shape. As they are markedly curved downwards, the matrix horns are expected to reach deep plantarly and proximally.
Haneke E. Controversies in the treatment of ingrown nails. Dermatol Res Pract. 2012;2012:783924. doi: 10.1155/2012/783924.
(Click Image to Enlarge)

Lateral Matrix Horn Phenolization. (a) The lateral nail strips are avulsed and shown. (b) Phenol is rubbed into the lateral matrix horn. (c) At the end of surgery, small antibiotic tablets are put into the wound cavity.
Haneke E. Controversies in the treatment of ingrown nails. Dermatol Res Pract. 2012;2012:783924. doi: 10.1155/2012/783924.
(Click Image to Enlarge)
Phenolization, Lateral Matrix Horn. The ingrown strip of nail plate is avulsed, and a cotton tip applicator dipped into liquefied phenol is vigorously rubbed into the matrix horn under the proximal nail fold for 2 to 3 minutes.
Haneke E. Controversies in the treatment of ingrown nails. Dermatol Res Pract. 2012;2012:783924. doi: 10.1155/2012/783924.
References
Bryant A, Knox A. Ingrown toenails: the role of the GP. Australian family physician. 2015 Mar:44(3):102-5 [PubMed PMID: 25770573]
DeLauro NM, DeLauro TM. Onychocryptosis. Clinics in podiatric medicine and surgery. 2004 Oct:21(4):617-30, vii [PubMed PMID: 15450901]
Park DH, Singh D. The management of ingrowing toenails. BMJ (Clinical research ed.). 2012 Apr 3:344():e2089. doi: 10.1136/bmj.e2089. Epub 2012 Apr 3 [PubMed PMID: 22491483]
Wollina U. Systemic Drug-induced Chronic Paronychia and Periungual Pyogenic Granuloma. Indian dermatology online journal. 2018 Sep-Oct:9(5):293-298. doi: 10.4103/idoj.IDOJ_133_18. Epub [PubMed PMID: 30258794]
Heidelbaugh JJ, Lee H. Management of the ingrown toenail. American family physician. 2009 Feb 15:79(4):303-8 [PubMed PMID: 19235497]
Langford DT, Burke C, Robertson K. Risk factors in onychocryptosis. The British journal of surgery. 1989 Jan:76(1):45-8 [PubMed PMID: 2917259]
Cho SY, Kim YC, Choi JW. Epidemiology and bone-related comorbidities of ingrown nail: A nationwide population-based study. The Journal of dermatology. 2018 Dec:45(12):1418-1424. doi: 10.1111/1346-8138.14659. Epub 2018 Sep 28 [PubMed PMID: 30264897]
Kose O, Celiktas M, Kisin B, Ozyurek S, Yigit S. Is there a relationship between forefoot alignment and ingrown toenail? A case-control study. Foot & ankle specialist. 2011 Feb:4(1):14-7. doi: 10.1177/1938640010382293. Epub 2010 Oct 4 [PubMed PMID: 20921151]
Level 2 (mid-level) evidenceEzekian B, Englum BR, Gilmore BF, Kim J, Leraas HJ, Rice HE. Onychocryptosis in the Pediatric Patient. Clinical pediatrics. 2017 Feb:56(2):109-114. doi: 10.1177/0009922816678180. Epub 2016 Dec 8 [PubMed PMID: 27941086]
Khunger N, Kandhari R. Ingrown toenails. Indian journal of dermatology, venereology and leprology. 2012 May-Jun:78(3):279-89. doi: 10.4103/0378-6323.95442. Epub [PubMed PMID: 22565427]
Kaur L, Dayal S, Singh J, Gowda VVM. Ibrutinib-Associated Multifocal Paronychia with Periungual Pyogenic Granulomas Involving Concomitant Finger and Toe Nails. Indian dermatology online journal. 2023 Sep-Oct:14(5):700-702. doi: 10.4103/idoj.idoj_527_22. Epub 2023 May 25 [PubMed PMID: 37727563]
Gera SK, PG Zaini DKH, Wang S, Abdul Rahaman SHB, Chia RF, Lim KBL. Ingrowing toenails in children and adolescents: is nail avulsion superior to nonoperative treatment? Singapore medical journal. 2019 Feb:60(2):94-96. doi: 10.11622/smedj.2018106. Epub [PubMed PMID: 30843080]
Romero-Pérez D, Betlloch-Mas I, Encabo-Durán B. Onychocryptosis: a long-term retrospective and comparative follow-up study of surgical and phenol chemical matricectomy in 520 procedures. International journal of dermatology. 2017 Feb:56(2):221-224. doi: 10.1111/ijd.13406. Epub 2016 Oct 12 [PubMed PMID: 27734499]
Level 2 (mid-level) evidenceFrancavilla V, Secolo G, D'Armetta M, Toscano R, Campo A, Catanzaro V, Manno M, Secolo I, Messina G. Onychocryptosis: a retrospective study of clinical aspects, inflammation treatment and pain management using Ozoile as a hydrogel and cream formulation. European journal of translational myology. 2024 Jun 26:34(2):. doi: 10.4081/ejtm.2024.12487. Epub 2024 Jun 26 [PubMed PMID: 38934121]
Level 2 (mid-level) evidenceMoellhoff N, Polzer H, Baumbach SF, Kanz KG, Böcker W, Bogner-Flatz V. [Unguis incarnatus-conservative or operative treatment? A practical treatment algorithm]. Der Unfallchirurg. 2021 Apr:124(4):311-318. doi: 10.1007/s00113-020-00903-6. Epub 2020 Oct 27 [PubMed PMID: 33111185]
Daniel CR 3rd, Iorizzo M, Tosti A, Piraccini BM. Ingrown toenails. Cutis. 2006 Dec:78(6):407-8 [PubMed PMID: 17243428]
Tomczak H, Dańczak-Pazdrowska A, Polańska A, Osmola-Mańkowska A, Pazdrowski J, Błażejewska-Gąsior W, Horla A, Hasse-Cieślińska M, Adamski Z. Microbiological analysis of acute infections of the nail fold on the basis of bait thread test. Postepy dermatologii i alergologii. 2017 Apr:34(2):110-115. doi: 10.5114/ada.2017.67072. Epub 2017 Apr 13 [PubMed PMID: 28507488]
Pruangmethangkul T, Pongprutthipan M, Chottawornsak N, Kerr SJ, Rerknimitr P. Adjunctive Pulsed Dye Laser Therapy for Paronychia Induced by Anticancer Agents. Lasers in surgery and medicine. 2025 Nov:57(9):691-699. doi: 10.1002/lsm.70060. Epub 2025 Aug 30 [PubMed PMID: 40884352]
Ergün T, Korkmaz M, Ergün D, Turan K, Muratoğlu OG, Cabuk H. Treatment of Ingrown Toenail with a Minimally Invasive Nail Fixator: Comparative Study with Winograd Technique. Journal of the American Podiatric Medical Association. 2024 Jan-Feb:114(1):. pii: 22-024. doi: 10.7547/22-024. Epub [PubMed PMID: 36040860]
Level 2 (mid-level) evidenceVinay K, Narayan Ravivarma V, Thakur V, Choudhary R, Narang T, Dogra S, Varthya SB. Efficacy and safety of phenol-based partial matricectomy in treatment of onychocryptosis: A systematic review and meta-analysis. Journal of the European Academy of Dermatology and Venereology : JEADV. 2022 Apr:36(4):526-535. doi: 10.1111/jdv.17871. Epub 2022 Jan 7 [PubMed PMID: 34913204]
Level 1 (high-level) evidenceDeBrule MB. Operative treatment of ingrown toenail by nail fold resection without matricectomy. Journal of the American Podiatric Medical Association. 2015 Jul:105(4):295-301. doi: 10.7547/13-121.1. Epub [PubMed PMID: 26218152]
Livingston MH, Coriolano K, Jones SA. Nonrandomized assessment of ingrown toenails treated with excision of skinfold rather than toenail (NAILTEST): An observational study of the Vandenbos procedure. Journal of pediatric surgery. 2017 May:52(5):832-836. doi: 10.1016/j.jpedsurg.2017.01.029. Epub 2017 Jan 29 [PubMed PMID: 28190555]
Level 2 (mid-level) evidenceHaneke E. Controversies in the treatment of ingrown nails. Dermatology research and practice. 2012:2012():783924. doi: 10.1155/2012/783924. Epub 2012 May 20 [PubMed PMID: 22675345]
Oh SJ, Lee J, Park S, Park JH, Lee D. Hutchinson Sign: Biopsy May Assist in Diagnosis of Subungual Melanoma in Situ. Dermatologic surgery : official publication for American Society for Dermatologic Surgery [et al.]. 2022 Jan 1:48(1):28-31. doi: 10.1097/DSS.0000000000003233. Epub [PubMed PMID: 34608084]
Grover C, Gupta P, Arora R, Jain P. Giant Cell Tumor of Flexor Tendon Sheath: An Interesting Clinical Presentation as Subungual Growth. Skin appendage disorders. 2025 Feb:11(1):87-92. doi: 10.1159/000540487. Epub 2024 Aug 13 [PubMed PMID: 39911971]
Dany M. Nail unit squamous cell carcinoma: updates on diagnosis, surgical approach, and the use of mohs micrographic surgery. Cutis. 2020 Nov:106(5):E11-E14. doi: 10.12788/cutis.0122. Epub [PubMed PMID: 33465201]
Haynes D, Haneke E, Rubin AI. Clinical, onychoscopic, nail clipping, and histopathological findings of malignant onychopapilloma. Journal of cutaneous pathology. 2024 Jul:51(7):500-505. doi: 10.1111/cup.14620. Epub 2024 Apr 2 [PubMed PMID: 38563529]
Quinto-González KL, Espinosa-Gutiérrez A, Hernández-Méndez-Villamil E, Borjón-Cisneros AE. [Glomus tumor of subungual presentation in the thumb and use of ultrasound in its diagnosis. Case report and literature review]. Acta ortopedica mexicana. 2023 Nov-Dec:37(6):368-371 [PubMed PMID: 38467459]
Level 3 (low-level) evidenceYoo H, Kim H, Kwon ST, Jo SJ, Mun JH, Lee C, Kwak Y, Kim BJ. Tumor invasion in the hyponychium is associated with distant metastasis and poor prognosis in subungual melanoma: A histologic landscape of 44 cases. Journal of the American Academy of Dermatology. 2022 May:86(5):1027-1034. doi: 10.1016/j.jaad.2021.06.847. Epub 2021 Jun 18 [PubMed PMID: 34153394]
Level 3 (low-level) evidenceWaterton K, Magro CM, Lipner SR. Nail Unit Squamous Cell Carcinoma with Onycholemmal Features: Case Report and Review of the Literature. Skin appendage disorders. 2023 Aug:9(4):284-290. doi: 10.1159/000529906. Epub 2023 Apr 14 [PubMed PMID: 37564691]
Level 3 (low-level) evidence