Introduction
Cranial nerve III palsy, also known as oculomotor nerve palsy, results from dysfunction of the third cranial nerve, which mediates most extraocular movements, elevation of the upper eyelid, and parasympathetic control of pupillary constriction and accommodation. Typical presentation includes ptosis, ophthalmoplegia, diplopia, and variable pupillary involvement, resulting in the characteristic down-and-out eye position in complete palsy.
Lesions affecting the cranial nerve III can occur along its entire course, from the oculomotor nucleus in the midbrain to terminal branches in the orbit. Clinical evaluation and management depend on patient age, pattern of oculomotor involvement, and presence of additional neurologic signs or symptoms. Etiologies range from benign microvascular ischemia to compressive intracranial lesions, including aneurysms, making prompt recognition and appropriate evaluation critical, particularly in cases presenting with pupillary dysfunction.
The third cranial nerve, also known as the oculomotor nerve, contains 2 major functional components. Parasympathetic fibers, located superficially, innervate the ciliary muscle and sphincter pupillae, mediating lens accommodation and pupillary constriction. Somatic motor fibers, located deeper, innervate the levator palpebrae superioris, which elevates the upper eyelid, and 4 extraocular muscles—the superior, medial, and inferior recti, as well as the inferior oblique. EOM innervation may be summarized using the mnemonic LR6(SO4)3, indicating that the lateral rectus muscle is supplied by cranial nerve VI (abducens), the superior oblique by cranial nerve IV (trochlear), and all remaining extraocular muscles by cranial nerve III.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
A broad range of disorders can disrupt oculomotor nerve function. Etiologies specific to lesion location are illustrated in the referenced figure (see Image. Anatomical Sites of Oculomotor Nerve Lesions).
Intracranial aneurysm is the most concerning cause of acute cranial nerve III palsy and typically results from external compression by an enlarging aneurysm. The posterior communicating artery constitutes the classic site, although aneurysms of the internal carotid and basilar arteries may also produce cranial nerve III palsy. Abrupt onset suggests aneurysmal expansion and confers an increased risk of near-term rupture, with subarachnoid hemorrhage potentially occurring within hours to days. Aneurysmal subarachnoid hemorrhage most commonly presents in the mid-50s but may occur across the age spectrum, including pediatric and older adult populations.[1][2]
Microvascular ischemia, often termed microvascular palsy or diabetic cranial nerve III palsy, is the most common etiology in adults. Small-vessel disease underlies most cases, with hypertension, advancing age, and other vascular risk factors increasing susceptibility. Although some clinically isolated presentations may reflect a small midbrain infarction, most ischemic cranial nerve III palsies arise from peripheral nerve involvement.[3]
Trauma-related cranial nerve III palsy typically follows high-impact head injury and is frequently associated with skull fracture or loss of consciousness. The occurrence of cranial nerve III palsy after minor head trauma should prompt evaluation for an alternative or additional underlying cause.
Recurrent painful ophthalmoplegic neuropathy, previously termed ophthalmoplegic migraine, occurs primarily in children and young adults and has been reclassified as a cranial neuropathy. The condition most commonly involves cranial nerve III and may result in residual neurologic deficits. In patients with typical clinical presentations, gadolinium enhancement of the affected cisternal nerve segment on magnetic resonance imaging (MRI) has been reported, supporting a recurrent demyelinating neuropathy mechanism.[4]
In children, all cases of acquired cranial nerve III palsy require thorough evaluation to exclude space-occupying intracranial lesions. Common etiologies include the following:
- Congenital causes: 43%
- Traumatic injury: 20%
- Local inflammatory processes: 13%
- Intracranial aneurysm: 7%
- Myasthenia gravis
- Migraine [5]
All pediatric patients presenting with strabismus should undergo assessment for uncorrected refractive error following administration of cycloplegic agents.[6] Congenital cranial nerve III palsy may result from developmental aplasia or hypoplasia of the oculomotor nucleus, birth-related trauma from molding forces acting on the skull during labor, intrauterine trauma, or, rarely, central nervous system infections such as meningitis.
Epidemiology
Oculomotor palsy has an annual incidence of approximately 4.0 per 100,000 individuals in population-based studies. Incidence increases markedly with age, reaching 12.5 per 100,000 in adults older than 60, compared with 1.7 per 100,000 in younger populations. In hospital-based cohorts, aneurysmal compression accounts for approximately 10% of cases, whereas population-based studies report lower rates near 6%. Vascular ischemia is the most common etiology overall, particularly among patients with diabetes mellitus and hypertension.
Pupillary involvement occurs in about 63% of oculomotor nerve palsies due to compressive lesions, compared to only 17% in microvascular cases. Among individuals with diabetes mellitus, isolated cranial nerve III palsy occurs in approximately 0.35% of hospitalized patients. Bilateral cranial nerve III palsies account for approximately 11% of cases in hospital-based populations.[7][8] In pediatric populations, trauma constitutes the predominant etiology and accounts for a substantially higher proportion of cases than in adult populations.[9]
Pathophysiology
The oculomotor nuclear complex is located in the midbrain at the level of the superior colliculus and consists of the main motor nucleus and the accessory parasympathetic nucleus, also known as the Edinger-Westphal nucleus. From the midbrain, nerve fibers traverse the interpeduncular fossa and course between the posterior cerebral artery and the superior cerebellar artery to reach the cavernous sinus. Along this segment, the oculomotor nerve lies lateral to the posterior communicating artery. The nerve subsequently divides into superior and inferior divisions before entering the orbit through the superior orbital fissure.[10]
Within the orbit, the smaller superior division innervates the superior rectus and the levator palpebrae superioris. In contrast, the larger inferior division innervates the medial and inferior recti and the inferior oblique. Before orbital entry, fibers responsible for pupillary constriction are located superficially within the nerve trunk and receive vascular supply from pial blood vessels. In contrast, deeper somatic motor fibers are supplied by the vasa vasorum.
Pathologies such as aneurysms, uncal herniation, or tumors compress the nerve externally and preferentially involve the superficial pupillomotor fibers and associated blood supply. In contrast, medical causes such as diabetes mellitus or hypertension-related microangiopathy affect the vasa vasorum and typically spare the pupillary fibers, resulting in pupil-sparing cranial nerve III palsy.[11] Aberrant regeneration of the oculomotor nerve may occur after compressive or traumatic injury but does not follow vascular etiologies such as diabetes mellitus. This pattern reflects damage to the endoneurial sheath, which occurs with compression and trauma but is not characteristic of vascular injury. Aberrant regeneration may manifest clinically as lid-gaze dyskinesis or pupil-gaze dyskinesis.
History and Physical
Ptosis occurs due to paralysis of the levator palpebrae superioris muscle.[12] Ocular deviation in cranial nerve III palsy reflects sparing of the lateral rectus and superior oblique muscles, with unopposed action producing the characteristic down-and-out eye position. In compressive cranial nerve III palsy, pupillary involvement manifests as a fixed and dilated pupil secondary to paralysis of the sphincter pupillae, with associated ciliary muscle dysfunction leading to loss of accommodation. In contrast, ischemic processes typically spare pupillary function, and accommodation remains intact. Diplopia results from the deviation of the affected eye, causing images to fall on an extrafoveal retinal point. However, ptosis frequently limits patient-reported diplopia by occluding the visual axis.
Distinct midbrain syndromes associated with cranial nerve III involvement include Benedikt syndrome, characterized by ipsilateral cranial nerve III palsy with contralateral tremor; Weber syndrome, defined by ipsilateral cranial nerve III palsy with contralateral hemiplegia; Nothnagel syndrome, which combines ipsilateral cranial nerve III palsy with cerebellar ataxia; and Claude syndrome, which presents with overlapping features of Benedikt and Nothnagel syndromes.
Evaluation
Patients presenting with acute isolated cranial nerve III palsy require neuroimaging irrespective of pupillary involvement. The choice of imaging modality depends on pupil status and overall clinical presentation.
Non–pupil-sparing presentations necessitate urgent computed tomography (CT) and CT angiography to rule out a posterior communicating artery aneurysm. Pupil-sparing cases in older patients with vascular risk factors may be monitored for spontaneous improvement. Patients without traditional vascular risk factors or those showing no improvement within 6 to 12 weeks should undergo contrast-enhanced MRI to identify lesions, including neoplasms, inflammatory processes, and brainstem infarction.[13][14] Evaluation for giant cell arteritis should be considered in adult patients older than 55, particularly when presenting with headache, jaw or tongue claudication, or visual loss.
Contrast-enhanced MRI of the brain and orbits is recommended for all patients presenting with acute isolated third nerve palsy, regardless of age or presence of vascular risk factors. Prospective studies indicate that 16.5% of adults with acute ocular motor mononeuropathy harbor structural lesions detectable on MRI.[15] The American College of Radiology advises high-resolution imaging with contrast-enhanced sequences to optimize visualization of intradural and foraminal cranial nerve segments.[16]
CT and CT angiography of the brain should be performed emergently to exclude compressive aneurysms in patients with pupil-involving third nerve palsies. Advanced MRI techniques, including three-dimensional gadolinium-enhanced CISS (Constructive Interference in Steady State) sequences, improve diagnostic accuracy for microvascular ischemic oculomotor palsy.[17] High-resolution CT may complement MRI when assessment of osseous integrity of the skull base and foramina is required, particularly in cases of trauma or suspected bony pathology.
Laboratory evaluation should include screening for vascular risk factors, including diabetes mellitus, hypertension, and hyperlipidemia, in all patients. Lumbar puncture with cerebrospinal fluid analysis should be considered when infectious or inflammatory etiologies remain in the differential diagnosis, initial imaging is nondiagnostic, or clinical symptoms progress despite treatment.[18][19]
Treatment / Management
Management of cranial nerve III palsy is guided by the underlying etiology. Pupil-sparing presentations typically indicate microvascular ischemia, particularly in patients with vascular risk factors such as diabetes mellitus or hypertension. Pupil-involving presentations raise concern for compressive lesions, including aneurysms, and require urgent neuroimaging and neurological consultation.
Conservative Treatment
Conservative management is appropriate for acute pupil-sparing cases, especially in patients older than 50 with vascular risk factors. Most ischemic third nerve palsies improve within a month, with complete recovery by 3 months.[20][21] Diplopia may be addressed by occluding the affected eye with an eye patch or opaque contact lens. In pediatric patients, alternate patching can prevent amblyopia secondary to ptosis or strabismus. Talebnejad et al reported the use of botulinum toxin injection into the lateral rectus during the acute phase of partial oculomotor palsy.[22] The injection induces paralysis of the lateral rectus, neutralizing outward ocular deviation in the primary gaze position.(B3)
Surgical Management
In acquired pupil-sparing third nerve palsy, surgical intervention is indicated after 6 months if spontaneous improvement does not occur. Surgical correction of oculomotor palsy is technically challenging, with the goals of aligning the eye in primary gaze and restoring binocular single vision. Eyelid surgery to correct ptosis should be performed only after ocular alignment is achieved to prevent diplopia.
Surgical strategies depend on the severity of the palsy. Complete cranial nerve III palsy may be managed with resection of the medial rectus and recession of the lateral rectus to correct horizontal deviation.[23] This procedure may be combined with superior oblique tendon transposition to generate tonic adducting force, maintaining the globe in the primary position. In partial third nerve palsy, the surgical approach is tailored to the extent of EOM involvement. Correction of paralytic strabismus should precede ptosis repair. Pupil-involving oculomotor palsy requires thorough evaluation and urgent referral to a neurologist.[24](B2)
Contralateral recession–resection surgery is an alternative approach for patients with third nerve palsy and aberrant regeneration. This technique can simultaneously correct strabismus and ptosis. In a series of 11 patients, alignment within 10 prism diopters was achieved, with mean ptosis improving from 3.9 to 0.9 mm.[25]
Differential Diagnosis
Differential diagnoses for oculomotor palsy include ophthalmoplegic migraine, internuclear ophthalmoplegia, adult-acquired or congenital ptosis, and anisocoria due to a tonic pupil, iris sphincter injury, or pharmacologic mydriasis. Other considerations include myasthenia gravis and thyroid ophthalmopathy.[26]
Prognosis
In most cases of cranial nerve III palsy, the prognosis is favorable, with spontaneous resolution of symptoms typically occurring within a few months. The extent of recovery depends on the underlying etiology and the interventions applied.[27]
Enhancing Healthcare Team Outcomes
Oculomotor palsy is a neurologic condition resulting from dysfunction of the third cranial nerve, which controls most EOM movements, eyelid elevation, and parasympathetic functions of the pupil and lens. Typical presentation includes ptosis, ophthalmoplegia, diplopia, and variable pupillary involvement, resulting in the characteristic down-and-out eye position in complete palsy. Etiologies range from microvascular ischemia and trauma to compressive lesions such as aneurysms, neoplasms, or hemorrhage, affecting both adult and pediatric populations. Accurate recognition and timely evaluation, including neuroimaging and laboratory studies, are essential to differentiate urgent from nonurgent causes and guide appropriate intervention and follow-up.
Both cosmetic and functional outcomes should inform treatment planning. Surgical intervention is frequently indicated for complete oculomotor palsy and often achieves cosmetically acceptable ocular alignment.[28] Patients with incomplete third nerve paralysis may also attain favorable functional and cosmetic results through strabismus surgery, optimizing both eye position and visual performance.
Effective management of cranial nerve III palsy requires collaboration across multiple disciplines. Clinicians and general practitioners are responsible for initial assessment, recognition of clinical patterns, and coordination of the diagnostic workup. Advanced practitioners and nurses support monitoring, patient education, and symptom management, whereas pharmacists review medications that may influence vascular risk or interact with planned interventions. Interprofessional communication ensures that findings are clearly shared among neurologists, ophthalmologists, radiologists, and surgical teams, facilitating coordinated care plans. This collaborative approach enhances patient-centered outcomes, promotes safety, and optimizes team performance by integrating diverse expertise to address both acute presentations and long-term functional recovery.
Media
(Click Image to Enlarge)
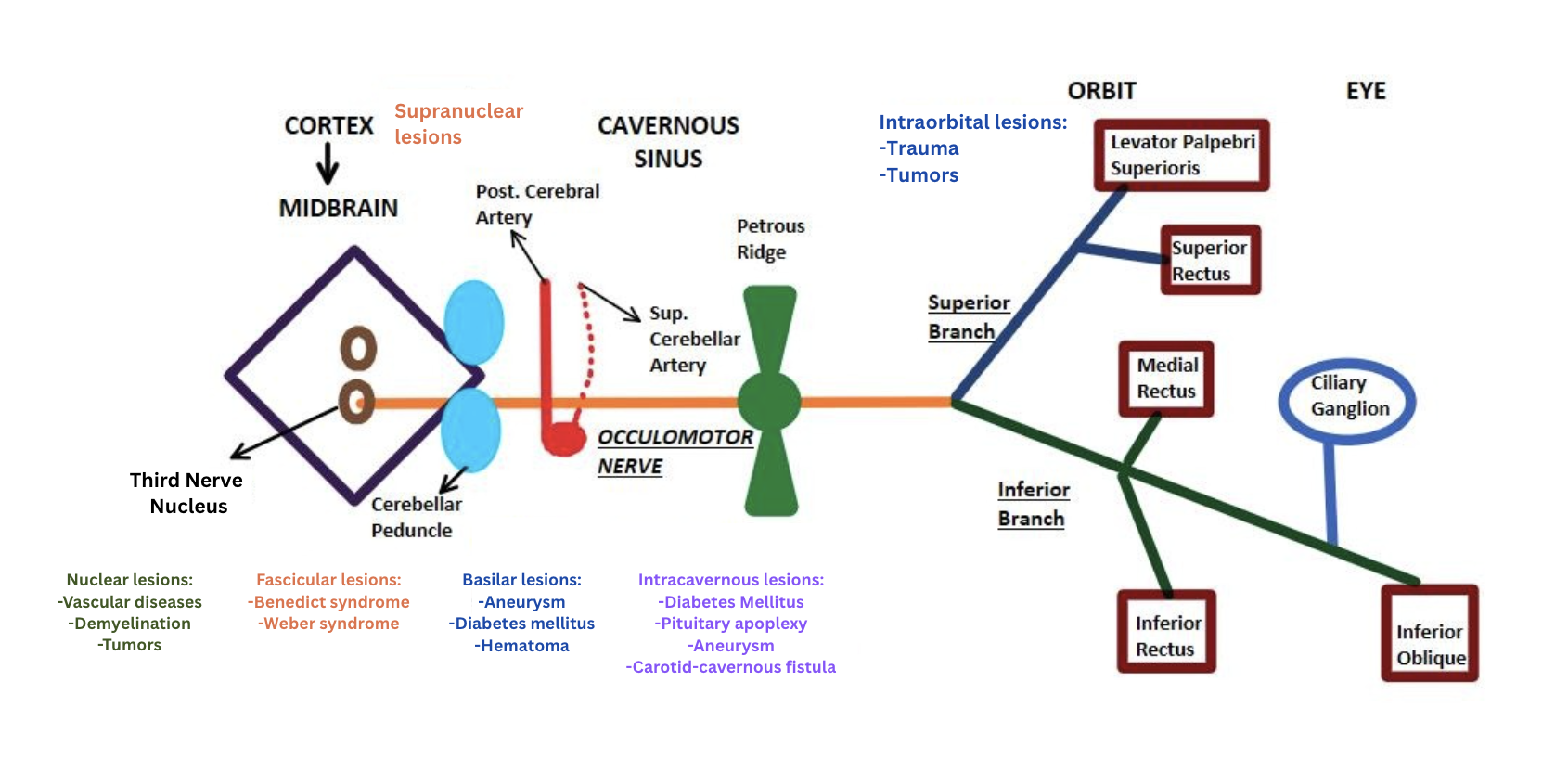
Anatomical Sites of Oculomotor Nerve Lesions. The diagram illustrates key anatomical sites along the oculomotor nerve pathway susceptible to lesions.
Contributed by P Modi, MBBS
References
Fang C, Leavitt JA, Hodge DO, Holmes JM, Mohney BG, Chen JJ. Incidence and Etiologies of Acquired Third Nerve Palsy Using a Population-Based Method. JAMA ophthalmology. 2017 Jan 1:135(1):23-28. doi: 10.1001/jamaophthalmol.2016.4456. Epub [PubMed PMID: 27893002]
Ding Y, Ding X, Huang B. Intracranial aneurysm risk stratification in acute ocular motor nerve palsy based on clinical features. Scientific reports. 2025 Oct 22:15(1):36871. doi: 10.1038/s41598-025-20898-7. Epub 2025 Oct 22 [PubMed PMID: 41125709]
Zhao B, Bhatti MT, Fang C, Hodge DO, Holmes JM, Mohney BG, Chen JJ. Vascular Risk Factors in Isolated Microvascular Ischemic Third Nerve Palsy: A Population-Based Study. Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society. 2023 Jun 1:43(2):248-253. doi: 10.1097/WNO.0000000000001755. Epub 2022 Nov 25 [PubMed PMID: 36730253]
Ansari SM, Dua SG, Mafraji M. Recurrent Painful Ophthalmoplegic Neuropathy in an Adult Patient: A Case Report With Literature Review. Cureus. 2022 May:14(5):e25297. doi: 10.7759/cureus.25297. Epub 2022 May 24 [PubMed PMID: 35755526]
Level 3 (low-level) evidenceSingh A, Bahuguna C, Nagpal R, Kumar B. Surgical management of third nerve palsy. Oman journal of ophthalmology. 2016 May-Aug:9(2):80-6. doi: 10.4103/0974-620X.184509. Epub [PubMed PMID: 27433033]
Alswaina N, Elkhamary SM, Shammari MA, Khan AO. Ophthalmic Features of Outpatient Children Diagnosed with Intracranial Space-Occupying Lesions by Ophthalmologists. Middle East African journal of ophthalmology. 2015 Jul-Sep:22(3):327-30. doi: 10.4103/0974-9233.159739. Epub [PubMed PMID: 26180471]
Greco D, Gambina F, Pisciotta M, Abrignani M, Maggio F. Clinical characteristics and associated comorbidities in diabetic patients with cranial nerve palsies. Journal of endocrinological investigation. 2012 Feb:35(2):146-9. doi: 10.3275/7574. Epub 2011 Mar 7 [PubMed PMID: 21399393]
Berlit P. Isolated and combined pareses of cranial nerves III, IV and VI. A retrospective study of 412 patients. Journal of the neurological sciences. 1991 May:103(1):10-5 [PubMed PMID: 1865222]
Level 2 (mid-level) evidenceKodsi SR, Younge BR. Acquired oculomotor, trochlear, and abducent cranial nerve palsies in pediatric patients. American journal of ophthalmology. 1992 Nov 15:114(5):568-74 [PubMed PMID: 1443017]
Flanders M, Hasan J, Al-Mujaini A. Partial third cranial nerve palsy: clinical characteristics and surgical management. Canadian journal of ophthalmology. Journal canadien d'ophtalmologie. 2012 Jun:47(3):321-5. doi: 10.1016/j.jcjo.2012.03.030. Epub [PubMed PMID: 22687316]
Level 3 (low-level) evidenceMotoyama Y, Nonaka J, Hironaka Y, Park YS, Nakase H. Pupil-sparing oculomotor nerve palsy caused by upward compression of a large posterior communicating artery aneurysm. Case report. Neurologia medico-chirurgica. 2012:52(4):202-5 [PubMed PMID: 22522330]
Level 3 (low-level) evidenceKomurcu HF, Ayberk G, Ozveren MF, Anlar O. Pituitary adenoma apoplexy presenting with bilateral third nerve palsy and bilateral proptosis: a case report. Medical principles and practice : international journal of the Kuwait University, Health Science Centre. 2012:21(3):285-7. doi: 10.1159/000334783. Epub 2011 Dec 8 [PubMed PMID: 22156441]
Level 3 (low-level) evidenceGarg A, Micieli JA. Importance of the "Rule of the Pupil" in the Modern Neuroimaging Era. Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society. 2021 Sep 1:41(3):293-297. doi: 10.1097/WNO.0000000000001175. Epub [PubMed PMID: 33470742]
Margolin E, Lam CTY. Approach to a Patient with Diplopia in the Emergency Department. The Journal of emergency medicine. 2018 Jun:54(6):799-806. doi: 10.1016/j.jemermed.2017.12.045. Epub 2018 Feb 14 [PubMed PMID: 29426788]
Tamhankar MA, Volpe NJ. Management of acute cranial nerve 3, 4 and 6 palsies: role of neuroimaging. Current opinion in ophthalmology. 2015 Nov:26(6):464-8. doi: 10.1097/ICU.0000000000000200. Epub [PubMed PMID: 26367093]
Level 3 (low-level) evidenceExpert Panel on Neurological Imaging, Rath TJ, Policeni B, Juliano AF, Agarwal M, Block AM, Burns J, Conley DB, Crowley RW, Dubey P, Friedman ER, Gule-Monroe MK, Hagiwara M, Hunt CH, Jain V, Powers WJ, Rosenow JM, Taheri MR, DuChene Thoma K, Zander D, Corey AS. ACR Appropriateness Criteria® Cranial Neuropathy: 2022 Update. Journal of the American College of Radiology : JACR. 2022 Nov:19(11S):S266-S303. doi: 10.1016/j.jacr.2022.09.021. Epub [PubMed PMID: 36436957]
Roques M, Serani M, Lecler A, Biotti D, Drissi C, Bonneville F. 3D Gadolinium-Enhanced CISS for the Diagnosis of Ischemic Third Nerve Palsy. AJNR. American journal of neuroradiology. 2025 Nov 3:46(11):2348-2354. doi: 10.3174/ajnr.A8865. Epub 2025 Nov 3 [PubMed PMID: 41130904]
Riegel DC, Jauregui R, Dugue A. Clinical Reasoning: An 83-Year-Old Female Patient With a Pupil-Involving Oculomotor Nerve Palsy. Neurology. 2025 Dec 23:105(12):e214383. doi: 10.1212/WNL.0000000000214383. Epub 2025 Nov 17 [PubMed PMID: 41248458]
Hörner R, Kassubek J, Dreyhaupt J, Ludolph AC. The spectrum and differential diagnosis of acquired ocular motor nerve palsies: a clinical study of 502 patients. Journal of neurology. 2022 Apr:269(4):2140-2148. doi: 10.1007/s00415-021-10761-w. Epub 2021 Sep 19 [PubMed PMID: 34537871]
Chou PY, Wu KH, Huang P. Ptosis as the only manifestation of diabetic superior division oculomotor nerve palsy: A case report. Medicine. 2017 Nov:96(46):e8739. doi: 10.1097/MD.0000000000008739. Epub [PubMed PMID: 29145322]
Level 3 (low-level) evidenceTiffin PA, MacEwen CJ, Craig EA, Clayton G. Acquired palsy of the oculomotor, trochlear and abducens nerves. Eye (London, England). 1996:10 ( Pt 3)():377-84 [PubMed PMID: 8796166]
Talebnejad MR, Sharifi M, Nowroozzadeh MH. The role of Botulinum toxin in management of acute traumatic third-nerve palsy. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2008 Oct:12(5):510-3. doi: 10.1016/j.jaapos.2008.03.009. Epub 2008 Jun 16 [PubMed PMID: 18558505]
Kattleman B, Flanders M, Wise J. Supramaximal horizontal rectus surgery in the management of third and sixth nerve palsy. Canadian journal of ophthalmology. Journal canadien d'ophtalmologie. 1986 Oct:21(6):227-30 [PubMed PMID: 3779510]
Level 3 (low-level) evidenceWang WX, Xu BN, Wang FY, Wu C, Sun ZH. Microsurgical management of posterior cerebral artery aneurysms: A report of thirty cases in modern era. British journal of neurosurgery. 2015 Jun:29(3):406-12. doi: 10.3109/02688697.2015.1004301. Epub 2015 Feb 20 [PubMed PMID: 25697238]
Level 2 (mid-level) evidenceFouad HM, Kamal AM, Awadein A, Del Monte MA. Contralateral Surgery for the Treatment of Third Nerve Palsy with Aberrant Regeneration. American journal of ophthalmology. 2021 Feb:222():166-173. doi: 10.1016/j.ajo.2020.07.044. Epub 2020 Aug 7 [PubMed PMID: 32777375]
De Silva DA, Siow HC. A case report of ophthalmoplegic migraine: a differential diagnosis of third nerve palsy. Cephalalgia : an international journal of headache. 2005 Oct:25(10):827-30 [PubMed PMID: 16162261]
Level 3 (low-level) evidenceKim K, Noh SR, Kang MS, Jin KH. Clinical Course and Prognostic Factors of Acquired Third, Fourth, and Sixth Cranial Nerve Palsy in Korean Patients. Korean journal of ophthalmology : KJO. 2018 Jun:32(3):221-227. doi: 10.3341/kjo.2017.0051. Epub 2018 Mar 20 [PubMed PMID: 29770635]
Schumacher-Feero LA, Yoo KW, Solari FM, Biglan AW. Third cranial nerve palsy in children. American journal of ophthalmology. 1999 Aug:128(2):216-21 [PubMed PMID: 10458179]
Level 2 (mid-level) evidence