 Anatomy, Head and Neck, Temporoparietal Fascia
Anatomy, Head and Neck, Temporoparietal Fascia
Introduction
The temporoparietal fascia (TPF), or superficial temporal fascia, is a thin connective tissue layer beneath the skin and subcutaneous tissue over the temporal fossa. This fibrous structure is continuous with the superficial musculoaponeurotic system (SMAS), connecting anteriorly to the frontalis and orbicularis oculi muscles, posteriorly to the occipitalis, and inferiorly to the platysma via the zygomatic arch (see Image. Muscles of the Head, Face, and Neck). The fascia receives a robust arterial supply from the superficial temporal artery and sensory innervation from the temporal branches of the trigeminal and facial nerves.
The TPF is clinically significant due to its reliable vascularity and pliability, making it a versatile tissue for reconstructive procedures in the head and neck. Surgically, the TPF serves as a donor flap for fascial, fasciocutaneous, and osseofascial reconstructions, enabling repair of defects in the auricle, eyelid, forehead, and nose while minimizing donor-site morbidity. Comprehensive knowledge of the fascia's anatomical relationships, neurovascular course, and biomechanical properties allows clinicians to perform safe dissections, optimize flap design, and reduce complications such as nerve injury or flap necrosis.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The TPF is continuous with the SMAS, which lies inferior to the zygomatic arch.[1] The SMAS and TPF connect with the platysma muscle in the neck, forming a unified fascial layer extending from the scalp to the clavicle. Anteriorly, the TPF integrates with the orbicularis oculi and frontalis muscles, and posteriorly with the occipitalis muscle.[2][3][4] The fascia measures approximately 2 to 3 mm in thickness and exhibits a dense vascular network.
The layers over the temporal fossa, arranged from superficial to deep, are as follows:
- Skin
- Subcutaneous tissue
- TPF
- Innominate fascia
- Deep temporal fascia
- Temporalis muscle
- Pericranium
- Cranium
The deep temporal fascia divides into superficial and deep layers before inserting into the superior aspect of the zygomatic arch. The superficial temporal fat pad separates these 2 layers (see Image. Fascial Planes of the Face).[5] Accurate knowledge of the anatomy surrounding the TPF is essential for surgical planning, as the fascia can serve as donor tissue for reconstruction. A comprehensive understanding of TPF relationships with adjacent neurovascular structures is critical for safe surgical dissection.
Deep to the TPF lies a loose, areolar, avascular plane that separates it from the deep temporal fascia. This layer, often referred to as the "innominate fascia," permits free movement of the superficial scalp over deeper muscular and fascial layers. The interaction of superficial, pliable layers with deeper, taut layers allows the scalp to preserve structural integrity while maintaining mobility. Fascia functions to enclose muscles, viscera, and neurovascular bundles into discrete organizational compartments.[6]
Embryology
The development of the head and neck structures centers on the branchial and pharyngeal apparatus. Between 4 and 7 weeks of gestation, the head and neck contain 5 or 6 pairs of branchial arches. External indentations, termed "branchial clefts," separate the arches and are lined by ectoderm. The corresponding inward grooves, or pharyngeal pouches, are lined by endoderm and represent primitive pharyngeal structures. Branchial arches consist of mesoderm, within which connective tissue, including cartilage and fascia, differentiates.
Blood Supply and Lymphatics
The scalp is rich in arterial anastomoses, with the majority of blood supply arising from the external carotid artery. Vascular supply to the TPF originates from the superficial temporal artery, the terminal branch of the external carotid artery.[7] The superficial temporal artery pierces the substance of the parotid gland anterior to the tragus. The scalp lymphatic system lacks intrinsic lymph nodes and drains primarily into parotid, anterior and posterior auricular, and occipital lymph nodes. Venous drainage patterns correspond to lymphatic drainage.[8][9]
Nerves
The superficial temporal artery courses within the TPF alongside the frontal branch of the facial nerve (see Image. Superficial Temporal Artery and Temporal Branch of the Facial Nerve).[10] Sensory innervation of the scalp arises from the trigeminal nerve medially and from the temporal, auricular, and occipital nerves laterally and posteriorly.
Surgical planning requires careful consideration of the frontotemporal branch of the facial nerve within this region (see Image. Frontal Branch of the Facial Nerve on Endoscopy). The nerve exits the parotid gland within the parotid-masseteric fascia and ascends within the innominate fascia over the zygomatic arch. At 1.5 to 3 cm above the superior border of the zygomatic arch and 0.9 to 1.4 cm posterior to the lateral orbital rim, the nerve transitions to a more superficial plane at the undersurface of the TPF, a region termed the "fascial transition zone."
Muscles
The main muscle occupying the temporal fossa is the temporalis muscle. This triangular muscle originates broadly on the parietal and frontal bones of the temporal fossa and on the deep surface of the deep temporal fascia. Insertion occurs at the coronoid process and anterior ramus of the mandible. The trigeminal nerve innervates the muscle via the deep temporal nerves. Contraction of the temporalis elevates the mandible to achieve jaw closure and retracts the mandible posteriorly.[11]
Surgical Considerations
The TPF flap provides extensive utility in head and neck reconstruction. First described in 1898 for reconstruction of an ear following a horse bite and for repair of the lower eyelid, the flap offers advantages in both size and flexibility. Up to 14 cm of TPF may be harvested safely, and the flap can function as a fascial, fasciocutaneous, or osseofascial flap. Clinical applications include forehead and brow, auricular, eyelid, and nasal reconstruction.[12][13][14][15][16] Plication of the TPF reduces lateral canthal rhytids, elevates the lateral brow during rhytidectomy, provides deep tissue support, and assists in preventing alopecia and visible scar formation.
Careful technique is required in this region to avoid injury to branches of the facial nerve. Dissection in the temporal region is safe above the superficial layer of the deep temporal fascia and below the innominate fascia. This plane ensures that the frontotemporal branch of the facial nerve remains superficial to the dissection.
Correct plane dissection is also necessary for safe execution of zygomatic arch fracture reduction using the Gilles approach.[17] A 2.5 cm temporal incision is made superior and anterior to the helix within the hairline. The superficial temporal artery must be preserved. Dissection proceeds to the deep layer of the deep temporal fascia.
The deep temporal fascia is incised to expose the temporalis muscle. Blunt dissection is performed between the deep temporalis fascia and the temporalis muscle using a sweeping motion. Upon reaching the level of the depressed zygomatic arch fracture, a Rowe zygomatic elevator is used to apply outward force to reduce the fracture.
The temporalis fascia is harvested routinely in tympanoplasty for reconstruction of the tympanic membrane. Ease of grafting makes this autologous donor site suitable for both medial and lateral tympanoplasty. The temporalis fascia provides reliable tissue for the subtotal and total repair of tympanic membrane perforations.[18][19][20]
Other Issues
The TPF is a highly reliable flap with an abundant vascular supply. Injury to the arterial network perfusing the TPF can result in flap necrosis. Vascular compromise may occur in patients with burns, head trauma, or prior scalp or skull surgery, making TPF use as a flap inadvisable. Assessment of vascular integrity may be performed using Doppler ultrasonography.[21]
Media
(Click Image to Enlarge)
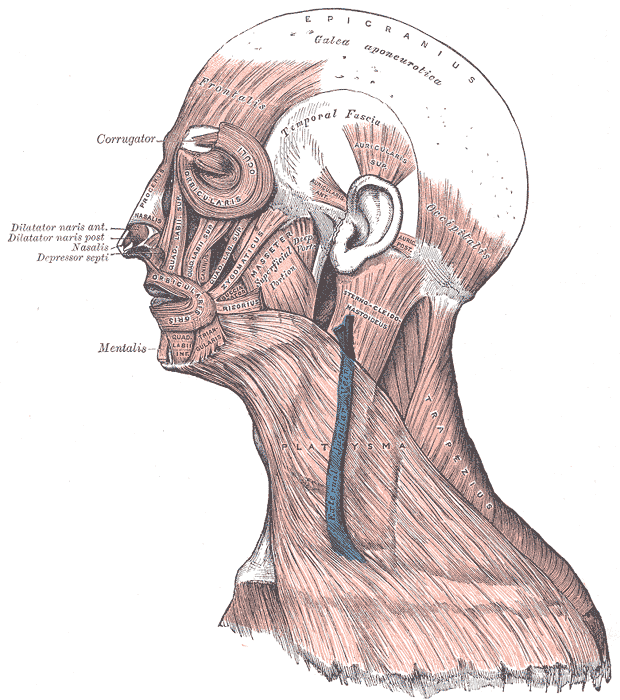
Muscles of the Head, Face, and Neck. The epicranius, galea aponeurotica, frontalis, temporal fascia, auricularis superior, auricularis anterior, auricularis posterior, occipitalis, sternocleidomastoid, platysma, trapezius, orbicularis oculi, corrugator, procerus, nasalis, dilator naris anterior, dilator naris posterior, depressor septi, mentalis, orbicularis oris, masseter, zygomaticus, and risorius muscles are shown in the image.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
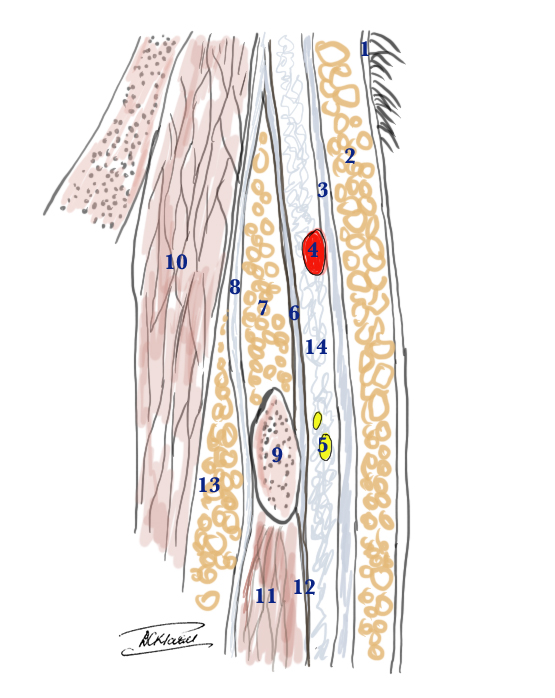
Superficial Temporal Artery and Temporal Branch of the Facial Nerve. This illustration shows an anatomical cross-section above the zygomatic arch with the relative layers. The numbered structures are: 1) skin; 2) subcutaneous fat; 3) superficial temporal fascia (also called the "temporoparietal fascia"); 4) temporal artery within the superficial temporal fascia; 5) temporal branch of the facial nerve just deep to the artery below the superficial temporal fascia; 6) superficial layer of deep temporal fascia; 7) superficial temporal fat pad; 8) deep layer of deep temporal fascia; 9) zygomatic arch; 10) temporalis muscle; 11) masseter muscle; and 12) masseteric fascia.
Contributed by Prof. Bhupendra C. K. Patel MD, FRCS
(Click Image to Enlarge)
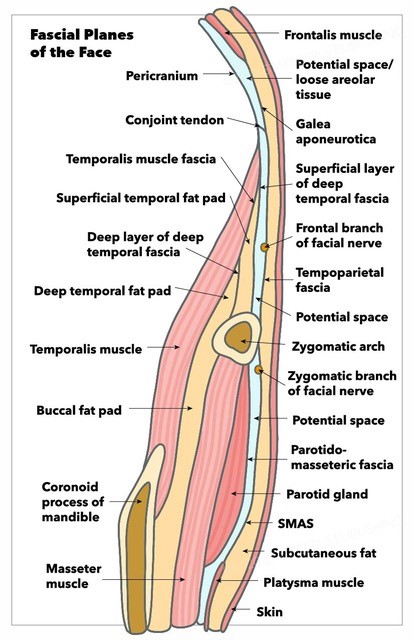
Fascial Planes of the Face. This illustration depicts the facial fascial planes, highlighting the continuity of the frontalis muscle, galea aponeurotica, temporoparietal fascia, superficial musculoaponeurotic system, platysma, and the location of the facial nerve.
Contributed by K Humphreys and MH Hohman, MD, FACS
(Click Image to Enlarge)
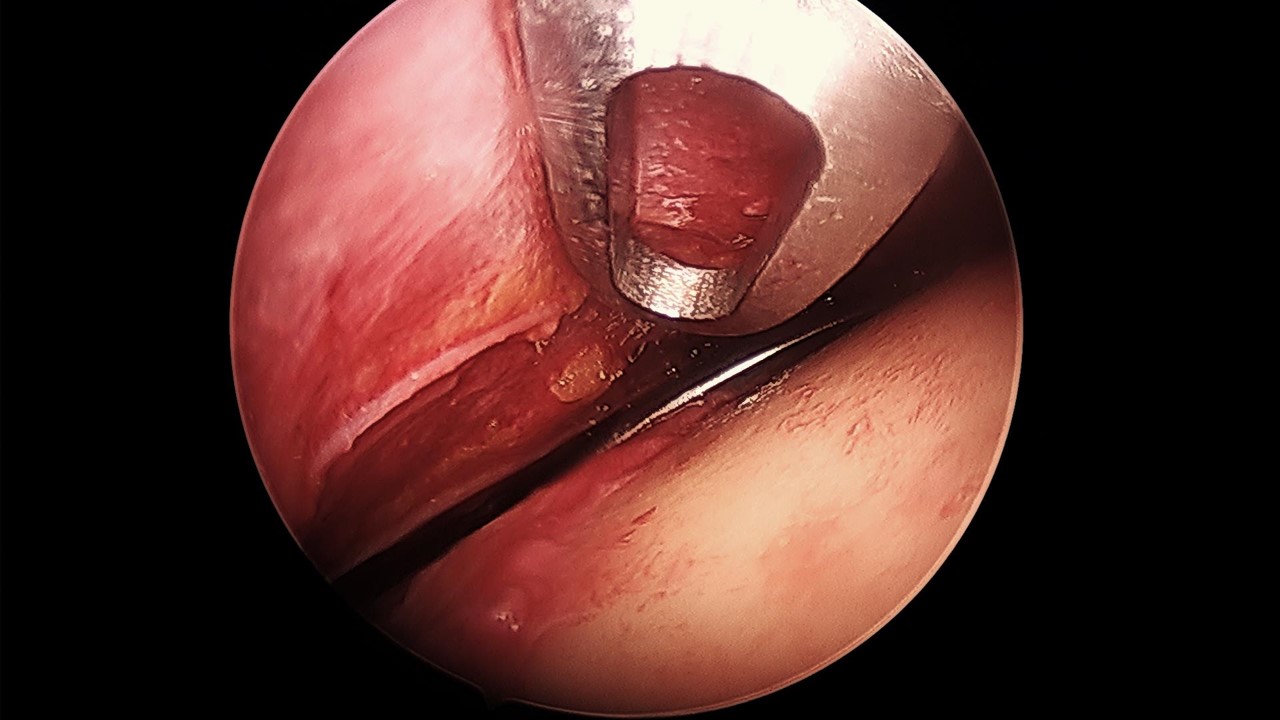
Frontal Branch of the Facial Nerve on Endoscopy. This image shows the nerve coursing along the underside of the temporoparietal fascia, appearing as a pale linear structure just to the left of the tip of the optical dissector.
Contributed by Marc H Hohman, MD, FACS
References
Minelli L, van der Lei B, Mendelson BC. The Superficial Musculoaponeurotic System: Does It Really Exist as an Anatomical Entity? Plastic and reconstructive surgery. 2024 May 1:153(5):1023-1034. doi: 10.1097/PRS.0000000000010557. Epub 2023 Apr 11 [PubMed PMID: 37039509]
Ferrari M, Vural A, Schreiber A, Mattavelli D, Gualtieri T, Taboni S, Bertazzoni G, Rampinelli V, Tomasoni M, Buffoli B, Doglietto F, Rodella LF, Deganello A, Nicolai P. Side-Door Temporoparietal Fascia Flap: A Novel Strategy for Anterior Skull Base Reconstruction. World neurosurgery. 2019 Jun:126():e360-e370. doi: 10.1016/j.wneu.2019.02.056. Epub 2019 Feb 27 [PubMed PMID: 30822581]
Zuo KJ, Wilkes GH. Clinical Outcomes of Osseointegrated Prosthetic Auricular Reconstruction in Patients With a Compromised Ipsilateral Temporoparietal Fascial Flap. The Journal of craniofacial surgery. 2016 Jan:27(1):44-50. doi: 10.1097/SCS.0000000000002181. Epub [PubMed PMID: 26703031]
Level 2 (mid-level) evidenceMavropoulos JC, Bordeaux JS. The temporoparietal fascia flap: a versatile tool for the dermatologic surgeon. Dermatologic surgery : official publication for American Society for Dermatologic Surgery [et al.]. 2014 Sep:40 Suppl 9():S113-9. doi: 10.1097/dss.0000000000000114. Epub [PubMed PMID: 25158871]
Level 3 (low-level) evidenceLee HJ, Kim HM, Ahn HS, Lee JH, Kim HJ. Novel Clinical Anatomical Consideration of the Superficial and Deep Layers of the Deep Temporal Fascia. Plastic and reconstructive surgery. 2024 Mar 1:153(3):591-599. doi: 10.1097/PRS.0000000000010507. Epub 2023 Apr 4 [PubMed PMID: 37010473]
Lam D, Carlson ER. The temporalis muscle flap and temporoparietal fascial flap. Oral and maxillofacial surgery clinics of North America. 2014 Aug:26(3):359-69. doi: 10.1016/j.coms.2014.05.004. Epub [PubMed PMID: 25086696]
Park H. Vascular Anatomy of the Temporoparietal Fascia in Microtia: A Computed Tomographic Angiographic Analysis of 172 Patients. Plastic and reconstructive surgery. 2025 Nov 17:():. doi: 10.1097/PRS.0000000000012621. Epub 2025 Nov 17 [PubMed PMID: 41264376]
Lopez R, Benouaich V, Chaput B, Dubois G, Jalbert F. Description and variability of temporal venous vascularization: clinical relevance in temporoparietal free flap technique. Surgical and radiologic anatomy : SRA. 2013 Nov:35(9):831-6. doi: 10.1007/s00276-013-1087-3. Epub 2013 Feb 26 [PubMed PMID: 23440495]
Demirdover C, Sahin B, Vayvada H, Oztan HY. The versatile use of temporoparietal fascial flap. International journal of medical sciences. 2011:8(5):362-8 [PubMed PMID: 21698054]
Yang SH, Park H, Yoo DS, Joo W, Rhoton A. Microsurgical anatomy of the facial nerve. Clinical anatomy (New York, N.Y.). 2021 Jan:34(1):90-102. doi: 10.1002/ca.23652. Epub 2020 Aug 21 [PubMed PMID: 32683749]
Zhang Y, Steinbacher J, Weninger WJ, Heber UM, Reissig L, Yildiz E, Tzou CJ. Surgical Anatomy of Temporalis Muscle Transfer with Fascia Lata Augmentation for the Reanimation of the Paralyzed Face: A Cadaveric Study. Archives of plastic surgery. 2023 Jan:50(1):42-48. doi: 10.1055/s-0042-1758469. Epub 2023 Feb 6 [PubMed PMID: 36755657]
Wang J, Xie L, Zhang N, Hu L, Wang J, Zhang S, Liu J, Wang X, Yan X. Clinical Application of the High Superficial Musculoaponeurotic System for Facial Rejuvenation in Chinese Patients. Plastic and reconstructive surgery. Global open. 2025 May:13(5):e6775. doi: 10.1097/GOX.0000000000006775. Epub 2025 May 12 [PubMed PMID: 40356621]
Nguyen HH, Tran HTT, Vu D, Ngo LM. Endoscopic-Assisted Harvest of Temporoparietal Fascia Flap Through a Single Incision for Single-Stage Auricular Reconstruction With Porous Polyethylene Framework: How I Do It. The Journal of craniofacial surgery. 2025 Sep 23:():. doi: 10.1097/SCS.0000000000011980. Epub 2025 Sep 23 [PubMed PMID: 40986841]
Yotsuyanagi T, Yamashita K, Takada A, Miura T. Our Evolved Technique for Microtia Reconstruction: An Advanced Form of the Yotsuyanagi Method. The Journal of craniofacial surgery. 2025 Sep 23:():. doi: 10.1097/SCS.0000000000011842. Epub 2025 Sep 23 [PubMed PMID: 40986838]
Kuo CI, Xiao P, Chang SC. Immediate Reconstruction With Autologous Temporoparietal Fascia After Enucleation of Infected or Extruded Alloplastic Nasal Implants. The Journal of craniofacial surgery. 2025 Mar-Apr 01:36(2):427-431. doi: 10.1097/SCS.0000000000010909. Epub 2024 Nov 27 [PubMed PMID: 39601559]
Cavadas PC, Sanz Giménez-Rico JR, Lan Cavadas AR. Total Eyelid Reconstruction in the Anophthalmic Orbit Simplified: The Trilamellar Temporoparietal Fascia Flap. Plastic and reconstructive surgery. Global open. 2025 Oct:13(10):e7212. doi: 10.1097/GOX.0000000000007212. Epub 2025 Oct 6 [PubMed PMID: 41059169]
Bergeron JM, Hohman MH, Raggio BS. Zygomatic Arch Fracture. StatPearls. 2026 Jan:(): [PubMed PMID: 31751088]
Parhiscar A, Har-El G, Turk JB, Abramson DL. Temporoparietal osteofascial flap for head and neck reconstruction. Journal of oral and maxillofacial surgery : official journal of the American Association of Oral and Maxillofacial Surgeons. 2002 Jun:60(6):619-22 [PubMed PMID: 12022094]
Level 2 (mid-level) evidenceClymer MA, Burkey BB. Other flaps for head and neck use: temporoparietal fascial free flap, lateral arm free flap, omental free flap. Facial plastic surgery : FPS. 1996 Jan:12(1):81-9 [PubMed PMID: 9244013]
Movassaghi K, Lewis M, Shahzad F, May JW Jr. Optimizing the Aesthetic Result of Parotidectomy with a Facelift Incision and Temporoparietal Fascia Flap. Plastic and reconstructive surgery. Global open. 2019 Feb:7(2):e2067. doi: 10.1097/GOX.0000000000002067. Epub 2019 Feb 8 [PubMed PMID: 30881826]
Jawad BA, Hohman MH, Raggio BS. Temporoparietal Fascia Flaps. StatPearls. 2026 Jan:(): [PubMed PMID: 32310365]