Introduction
Swallowing, also known as deglutition, is a physiologic function involving coordinated muscle contractions that propel food and liquids from the oral cavity to the stomach. The process occurs in 3 distinct phases: oral, pharyngeal, and esophageal, with the oral phase being voluntary and the other 2 reflexive. The oral phase further subdivides into preparatory and propulsive stages. Each phase is defined by the location of the bolus during transit to the stomach. The oral and pharyngeal stages share anatomy with the respiratory tract, making airway protection during these stages essential. The anatomy and function of the structures involved in swallowing are discussed further in this activity.[1]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The oral preparatory stage begins when solid food or liquid enters the oral cavity. Tongue position during this phase differs depending on the consistency of the ingested substance. During liquid ingestion, the posterior tongue rises to meet the soft palate, forming a glossopalatal seal that prevents premature passage of liquid into the oropharynx. This seal does not form during mastication of solid foods, preserving communication between the oral cavity and oropharynx. Free tongue movement allows mastication and bolus formation, which would be impaired by a glossopalatal seal.
Immediately before swallow initiation, the anterior tongue rises to meet the hard palate while the posterior tongue drops, opening the oropharynx. The bolus is propelled along the palate by the tongue toward the oropharynx, marking the oral propulsive stage and the onset of the pharyngeal phase. Swallowing solid food is sequential, with the pharyngeal phase commencing after completion of the propulsive stage. In contrast, swallowing liquids involves overlap of the propulsive and pharyngeal stages. Posterior propulsion of liquid stimulates sensory receptors in the oropharynx, triggering the pharyngeal swallow almost immediately. Therefore, airway protection and pharyngeal contraction begin while the tongue continues propelling the liquid.
The pharyngeal phase is the 1st involuntary phase of swallowing, characterized by rapid muscle contractions that propel the bolus through the upper esophageal sphincter (UES) and into the esophagus. This phase is triggered when the bolus reaches the palatoglossal arch.[2] Airway protection occurs through a brief, involuntary cessation of respiration known as swallowing apnea, which typically coincides with the end of expiration.[3] Concurrently, vocal fold adduction and glottic closure form an effective barrier that prevents the entry of ingested material into the trachea. These coordinated mechanisms ensure safe bolus passage into the esophagus and minimize aspiration risk.
The esophageal phase is entirely involuntary and begins once the bolus enters the esophagus. Coordinated primary peristaltic contractions propel the bolus toward the stomach. The lower esophageal sphincter (LES) relaxes ahead of the bolus to permit passage and contracts afterward to prevent gastroesophageal reflux. Secondary peristaltic contractions may occur if residual material remains, ensuring complete luminal clearance (see Image. Swallowing Mechanism).
Embryology
The structures involved in swallowing begin developing early in fetal life, around the start of week 4 of embryogenesis. During this period, the branchial or pharyngeal arches begin forming and will give rise to the mature structures responsible for deglutition. Mature structures develop through contributions from all 3 primary germ layers and originate from 1 or more of the 6 pharyngeal arches, with the 5th arch involuting early in development. Mucosal surfaces lining the pharynx arise from endoderm. Muscles and bones originate from mesoderm, coordinated with neural crest contributions. Ectoderm forms the oral glands, tooth enamel, and nerves responsible for neural regulation of the swallowing sequence.[4][5][6][7]
Blood Supply and Lymphatics
Arterial supply to structures involved in swallowing is derived primarily from branches of the external carotid artery within the oral cavity and pharynx. The tongue receives blood from the lingual artery, a direct branch of the external carotid. The hard and soft palates obtain vascular input from branches of the maxillary and facial arteries. The hard palate is supplied by the superior alveolar and greater palatine arteries, both branches of the maxillary artery, whereas the ascending palatine artery, a branch of the facial artery, supplies the soft palate.[8][9]
Pharyngeal musculature receives arterial supply from multiple external carotid branches, with the ascending pharyngeal artery contributing significantly. In contrast, the esophagus exhibits region-specific vascularization: the cervical portion is supplied by the inferior thyroid artery, the proximal thoracic segment by bronchial branches, and the distal thoracic esophagus by direct branches from the aorta.[10][11]
Lymphatic drainage of swallowing-related structures follows a generally predictable progression from superficial oral regions to deeper cervical chains. The floor of the mouth and anterior tongue primarily drain to the submental nodes, whereas much of the oral cavity, including the palate and buccal mucosa, drains to the submandibular nodes. Lymph from these regions, together with drainage from the pharynx and larynx, is subsequently conveyed to the upper jugular nodes. The middle jugular nodes receive lymph from the base of the tongue and hypopharynx, in addition to efferent drainage from the upper jugular group, before passing to the lower jugular nodes.
From the lower jugular nodes, lymph drains into the medial supraclavicular nodes, which also receive input from the hypopharynx and esophagus. Additional regional drainage includes the posterior triangle nodes, which serve the nasopharynx and oropharynx, and the retropharyngeal nodes, which drain the nasopharynx and soft palate.[12][13]
Nerves
Multiple nerves participate in swallowing, with coordinated activity enabling mastication, palatal elevation, and bolus propulsion through the pharynx and esophagus. The primary cranial nerves involved include the mandibular division of the trigeminal nerve (cranial nerve V3) and the glossopharyngeal (cranial nerve IX), vagus (cranial nerve X, and hypoglossal (cranial nerve XII) nerves.
Pharyngeal sensation is mediated primarily by the glossopharyngeal nerve, whereas the vagus nerve, including its recurrent laryngeal branch, provides motor innervation critical for pharyngeal contraction and airway protection. The ansa cervicalis contributes secondarily by innervating the infrahyoid muscles, which stabilize and position the hyoid bone and larynx during swallowing.
The vagus nerve innervates the upper esophagus, while the lower esophagus receives input from the esophageal plexus, comprising parasympathetic fibers from the vagus nerve and sympathetic fibers. Sympathetic activity maintains baseline LES tone, and parasympathetic input via the vagus nerve facilitates LES relaxation during swallowing.
Muscles
Swallowing is a highly regulated and coordinated physiologic act that relies on sequential activation of multiple muscle groups across the oral cavity, pharynx, larynx, and esophagus. During the oral stage, tongue movement is critical for bolus manipulation and propulsion. Intrinsic and extrinsic tongue muscles, including the genioglossus, hyoglossus, and styloglossus, generate the complex movements required for bolus shaping and posterior transport, while the palatoglossus contributes to tongue–palate coordination. These muscles operate in concert to control bolus position and movement within the oral cavity. The mylohyoid muscle elevates the floor of the mouth and supports tongue function during this stage.
Mastication must precede bolus propulsion into the pharynx. This process is mediated by the muscles of mastication, including the medial and lateral pterygoids, masseter, and temporalis. Coordinated contraction of these muscles breaks down ingested food, forming a bolus ready for swallowing.
The pharyngeal stage of swallowing involves the greatest number of muscles and is characterized by rapid, highly coordinated movements that propel the bolus while protecting the airway. Stabilization and elevation of the soft palate prevent nasopharyngeal reflux. The tensor veli palatini tenses the soft palate, creating a stable platform that allows the levator veli palatini to elevate it effectively. Palatal elevation forms a seal between the nasopharynx and oropharynx, directing the bolus inferiorly.
Elevation of the hyoid bone and larynx is mediated by the suprahyoid muscle group, including the digastric, stylohyoid, geniohyoid, and mylohyoid muscles. These muscles act in concert to elevate and anteriorly displace the hyoid bone, contributing to airway protection and opening of the UES.[14] The infrahyoid muscles, often referred to as the "strap muscles," depress and stabilize the hyoid and larynx following elevation. This group includes the omohyoid, sternohyoid, sternothyroid, and thyrohyoid muscles.[15]
Further elevation and shortening of the pharynx are produced by the longitudinal pharyngeal muscles, including the stylopharyngeus, salpingopharyngeus, and palatopharyngeus. Contraction of these muscles expands and elevates the pharynx, creating a favorable pathway for bolus transit.[16]
Sequential constriction of the pharynx is accomplished by the pharyngeal constrictor muscles. These muscles contract in a coordinated, wave-like fashion to propel the bolus toward the UES. The cricopharyngeus muscle, forming the primary component of the UES at the pharyngoesophageal junction, regulates bolus entry into the esophagus by relaxing at the appropriate moment.[17]
Airway protection during swallowing is further maintained by the intrinsic muscles of the larynx, which adduct the vocal folds and close the laryngeal inlet. The lateral cricoarytenoid, transverse arytenoid, and oblique arytenoid muscles contribute to vocal fold closure, while the aryepiglottic muscle approximates the arytenoid cartilages and folds the epiglottis over the laryngeal inlet, reducing the risk of aspiration.[18]
The upper 1/3 of the esophagus consists of striated muscle and includes the UES. The middle 1/3 contains both striated and smooth muscle, and the lower 1/3 is composed of smooth muscle and contains the LES.
Clinical Significance
Dysphagia is a common clinical problem, particularly among older individuals, and may result from abnormalities affecting any portion of the swallowing pathway, from the oral cavity to the LES. Prolonged or untreated impairment of swallowing can lead to significant complications, including malnutrition and aspiration. Any pathological process that disrupts structures involved in swallowing can produce clinically significant dysphagia.
Acquired structural and functional disorders frequently underlie swallowing dysfunction. Esophageal or pharyngeal strictures and webs are often associated with gastroesophageal reflux disease and can critically narrow the lumen of the esophagus or UES, impeding bolus passage. Management of these conditions commonly involves endoscopic techniques, including serial dilations. Esophageal motor disorders, such as diffuse esophageal spasm and achalasia, impair coordinated bolus transport through the esophagus and into the stomach. Heller myotomy, in which muscle fibers of the hypercontractile LES are divided, may relieve obstruction and improve swallowing in patients with achalasia.[19]
Zenker diverticulum comprises a less common but clinically significant cause of dysphagia, most frequently affecting older men. This condition is classified as a false diverticulum because it involves herniation of only the mucosa and submucosa through a defect in the cricopharyngeus muscle. Clinical presentation may include dysphagia, halitosis, regurgitation, and increased risk of aspiration. Diagnosis is typically established with a barium swallow study, and symptomatic cases may be managed surgically via open or endoscopic approaches.[20]
Malignancy should be considered in patients with progressive dysphagia, particularly when difficulty swallowing solids is accompanied by systemic features such as weight loss or bleeding. Lesions adjacent to the esophagus can cause extrinsic compression and mimic dysphagia. Relevant considerations include thyroid enlargement, mediastinal tumors, left atrial enlargement, and prior surgery or radiation therapy involving the neck or mediastinum.[21]
Congenital abnormalities can impair swallowing early in life and frequently require surgical intervention. Cleft lip or palate may disrupt oral seal formation and velopharyngeal closure, increasing the risk of nasopharyngeal regurgitation and feeding difficulties. Abnormal development of dentition or oral cavity structures can further compromise mastication and effective bolus formation. Tracheoesophageal fistulas, which may present in several anatomical variations, can severely disrupt normal swallowing mechanics at birth and generally require surgical correction. Variations in the origins and insertions of oral and pharyngeal muscles may also contribute to swallowing difficulty in affected individuals.
Neurological conditions represent an important contributor to dysphagia. Parkinson disease is frequently associated with swallowing dysfunction due to degeneration of dopaminergic neurons that control the striated muscles of the oral cavity, pharynx, and esophagus.[22] Accurate diagnosis of dysphagia depends on symptoms occurring during swallowing. Sensations of fullness or a lump in the throat unrelated to swallowing are classified as globus hystericus. Although often functional, globus hystericus may also reflect underlying abnormalities of the pharyngeal or upper esophageal musculature.
Evaluation of dysphagia commonly includes barium swallow studies, esophageal manometry, and esophagogastroduodenoscopy. These modalities together assess structural, functional, and mucosal abnormalities contributing to impaired swallowing.[23]
Media
(Click Image to Enlarge)
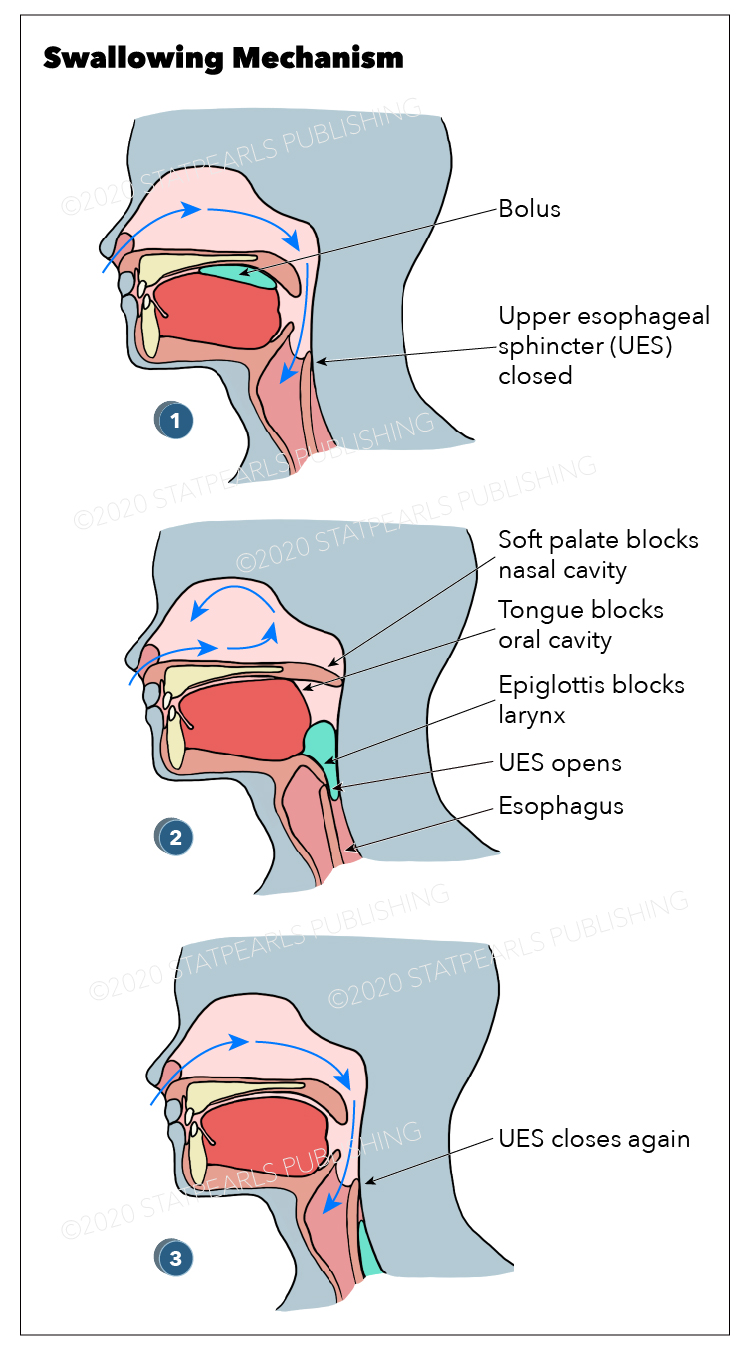
Swallowing Mechanism. This diagram illustrates the oral, pharyngeal, and esophageal stages of deglutition, highlighting bolus movement, soft palate elevation, epiglottis closure, and upper esophageal sphincter (UES) dynamics.
Graphic by Emma Gregory
References
Matsuo K, Palmer JB. Anatomy and physiology of feeding and swallowing: normal and abnormal. Physical medicine and rehabilitation clinics of North America. 2008 Nov:19(4):691-707, vii. doi: 10.1016/j.pmr.2008.06.001. Epub [PubMed PMID: 18940636]
Panara K, Ramezanpour Ahangar E, Padalia D. Physiology, Swallowing. StatPearls. 2025 Jan:(): [PubMed PMID: 31082115]
Costa MM, Lemme EM. Coordination of respiration and swallowing: functional pattern and relevance of vocal folds closure. Arquivos de gastroenterologia. 2010 Jan-Mar:47(1):42-8 [PubMed PMID: 20520974]
Casale J, Giwa AO. Embryology, Branchial Arches. StatPearls. 2025 Jan:(): [PubMed PMID: 30860722]
Frisdal A, Trainor PA. Development and evolution of the pharyngeal apparatus. Wiley interdisciplinary reviews. Developmental biology. 2014 Nov-Dec:3(6):403-18. doi: 10.1002/wdev.147. Epub 2014 Aug 29 [PubMed PMID: 25176500]
Level 3 (low-level) evidenceRosero Salazar DH, Carvajal Monroy PL, Wagener FADTG, Von den Hoff JW. Orofacial Muscles: Embryonic Development and Regeneration after Injury. Journal of dental research. 2020 Feb:99(2):125-132. doi: 10.1177/0022034519883673. Epub 2019 Nov 1 [PubMed PMID: 31675262]
Lacruz RS, Habelitz S, Wright JT, Paine ML. DENTAL ENAMEL FORMATION AND IMPLICATIONS FOR ORAL HEALTH AND DISEASE. Physiological reviews. 2017 Jul 1:97(3):939-993. doi: 10.1152/physrev.00030.2016. Epub [PubMed PMID: 28468833]
Cho JH, Kim JW, Park HW, Suh JD, Kim JK, Yoon JH. Arterial supply of the human soft palate. Surgical and radiologic anatomy : SRA. 2017 Jul:39(7):731-734. doi: 10.1007/s00276-016-1798-3. Epub 2017 Jan 30 [PubMed PMID: 28138793]
Kamrani P, Sadiq NM. Anatomy, Head and Neck, Oral Cavity (Mouth). StatPearls. 2025 Jan:(): [PubMed PMID: 31424855]
Burger D, Piehslinger E. [The blood supply of the cervical esophagus]. Acta anatomica. 1991:142(3):204-7 [PubMed PMID: 1796734]
Yan Y, Chen C, Chen Y, Wu Y, Shi Z. Arterial patterns in the thoracic and abdominal segments of the esophagus: anatomy and clinical significance. Surgical and radiologic anatomy : SRA. 1998:20(6):399-402 [PubMed PMID: 9932323]
Koroulakis A, Jamal Z, Agarwal M. Anatomy, Head and Neck, Lymph Nodes. StatPearls. 2025 Jan:(): [PubMed PMID: 30020689]
Lengelé B, Hamoir M, Scalliet P, Grégoire V. Anatomical bases for the radiological delineation of lymph node areas. Major collecting trunks, head and neck. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology. 2007 Oct:85(1):146-55 [PubMed PMID: 17383038]
Level 3 (low-level) evidenceKhan YS, Fakoya AO, Bordoni B. Anatomy, Head and Neck: Suprahyoid Muscle. StatPearls. 2025 Jan:(): [PubMed PMID: 31536316]
Fischer C, Ransmayer G. [The attachment and function of the infrahyoid muscles]. Anatomischer Anzeiger. 1989:168(3):237-43 [PubMed PMID: 2764279]
Choi DY, Bae JH, Youn KH, Kim HJ, Hu KS. Anatomical considerations of the longitudinal pharyngeal muscles in relation to their function on the internal surface of pharynx. Dysphagia. 2014 Dec:29(6):722-30. doi: 10.1007/s00455-014-9568-z. Epub 2014 Aug 21 [PubMed PMID: 25142243]
Heyd C, Yellon R. Anatomy, Head and Neck, Pharynx Muscles. StatPearls. 2025 Jan:(): [PubMed PMID: 30969574]
Andaloro C, Sharma P, La Mantia I. Anatomy, Head and Neck: Larynx Arytenoid Cartilage. StatPearls. 2025 Jan:(): [PubMed PMID: 30020624]
Nau P, Rattner D. Laparoscopic Heller myotomy as the gold standard for treatment of achalasia. Journal of gastrointestinal surgery : official journal of the Society for Surgery of the Alimentary Tract. 2014 Dec:18(12):2201-7. doi: 10.1007/s11605-014-2655-5. Epub 2014 Sep 10 [PubMed PMID: 25205539]
Level 2 (mid-level) evidenceNesheiwat Z, Antunes C. Zenker Diverticulum. StatPearls. 2025 Jan:(): [PubMed PMID: 29763172]
Walker HK, Hall WD, Hurst JW, Wolf DC. Dysphagia. Clinical Methods: The History, Physical, and Laboratory Examinations. 1990:(): [PubMed PMID: 21250248]
Suttrup I, Warnecke T. Dysphagia in Parkinson's Disease. Dysphagia. 2016 Feb:31(1):24-32. doi: 10.1007/s00455-015-9671-9. Epub 2015 Nov 21 [PubMed PMID: 26590572]
Yadlapati R. High-resolution esophageal manometry: interpretation in clinical practice. Current opinion in gastroenterology. 2017 Jul:33(4):301-309. doi: 10.1097/MOG.0000000000000369. Epub [PubMed PMID: 28426462]
Level 3 (low-level) evidence