Introduction
Group A Streptococcus (GAS), or Streptococcus pyogenes, is a gram-positive bacterium that is uniquely adapted to humans and found almost exclusively in the human body. GAS is responsible for a wide range of infections, most commonly involving the upper respiratory tract and skin. In addition, GAS can cause severe invasive infections, including streptococcal toxic shock syndrome (STSS), necrotizing fasciitis, bacteremia, pneumonia, and meningitis.[1][2]
GAS infections are common. Hundreds of millions of noninvasive infections, including pharyngitis, scarlet fever, and impetigo, occur globally each year. Although invasive infections such as STSS and necrotizing fasciitis occur much less commonly than noninvasive infections, hundreds of thousands of invasive GAS (iGAS) infections occur globally every year. GAS can also lead to post-infectious immune-mediated sequelae, including acute rheumatic fever (ARF), post-streptococcal glomerulonephritis (PSGN), and complications from immune-mediated processes, such as rheumatic heart disease (RHD).[3]
GAS is the leading bacterial cause of acute pharyngitis, accounting for 5 to 15 percent of ambulatory care visits for acute pharyngitis in adults and 20 to 30 percent in children.[4][5][6] Timely diagnosis and treatment are essential to prevent ARF and other post-infectious sequelae.[5] Established criteria, diagnostic methods, and guidelines for managing GAS pharyngitis aim to ensure timely diagnosis and reduce the risk of complications, such as peritonsillar abscess, iGAS infections, immune-mediated sequelae, and GAS transmission.[5][7][8]
Despite the availability of guidelines for diagnosing GAS pharyngitis, antibiotics are often overprescribed, leading to unnecessary exposure and contributing to antibiotic resistance. Antibiotic resistance has been reported with various antibiotics, including macrolides (such as erythromycin and azithromycin) and lincosamides (including clindamycin).[9][10][11] Overprescription is driven by several factors, including poor adherence to guidelines, challenges in accurately diagnosing GAS pharyngitis, misdiagnosing GAS carriage as active infection, and pressure from patients and clinicians to prescribe antibiotics.[4][5][12] Clinicians must exercise caution and prescribe antibiotics only when necessary to minimize antibiotic pressure and reduce the risk of resistance development.[4][6][13]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
GAS is a gram-positive, nonspore-forming, catalase- and oxidase-negative bacterium that grows in pairs and chains (see Image. S pyogenes Bacterium).[14] When cultured on blood agar at 35 °C and 37 °C in a 10 percent carbon dioxide environment, GAS produces smooth, moist, grayish-white colonies with clear margins measuring over 0.5 mm. These colonies are surrounded by a zone of complete hemolysis (beta-hemolysis) (see Image. Comparisons of Hemolytic Activity of Groups A, B, G, and F Streptococci).
The Lancefield classification categorizes streptococci into serologic groups, labeled A to O, based on the reactions of antisera with carbohydrate antigens on the streptococcal cell wall.[15] At least 20 serological groups have been identified, including groups A, B, and C; GAS belongs to Lancefield group A.[16][17] Other streptococci from different Lancefield groups can cause syndromes similar to those caused by GAS. Notably, group B Streptococcus (GBS; Streptococcus agalactiae) colonizes the human gastrointestinal and genital mucosa and can lead to conditions such as puerperal sepsis, neonatal infections, pneumonia, bacteremia, and meningitis.[18]
GAS has also been subdivided based on the serotypes of the M- and T-antigens expressed on its surface.[15] Traditional serotyping methods to detect T- and M antigens have largely been replaced by sequence typing of the N-terminal part of the M-protein gene (emm), which is now primarily used for genotyping GAS, mainly for epidemiological purposes.[15][19] Whole genome sequencing (WGS) is increasingly utilized to identify epidemic strains of GAS. Over 220 emm types have been classified based on the M-protein gene sequence.[20][15] The streptococcal M-protein, a key virulence factor used for epidemiological typing, also serves as a potential vaccine antigen.[19]
Numerous virulence determinants in GAS have been identified, aiding in adhesion, colonization, evasion of the innate immune system, invasion, and dissemination within the host.[21] Key virulence factors include the M-protein, hyaluronic acid, streptokinase, and deoxyribonuclease B (DNase-B). Among its notable toxins are the pyrogenic toxins (also known as scarlatina or erythrogenic toxins), which cause the rash in scarlet fever. These toxins also stimulate mononuclear cells to produce tumor necrosis factor (TNF)-alpha and interleukins (IL-1 and IL-6), thereby contributing to fever and shock in patients with STSS.[1][22]
Certain bacterial superantigenic exotoxins, associated with syndromes such as STSS, trigger an atypical polyclonal activation of lymphocytes. This leads to rapid-onset shock and multiorgan failure, contributing to high mortality. The primary superantigenic exotoxins identified are toxic shock syndrome toxin-1 (TSST-1) and enterotoxins.[22]
GAS is uniquely adapted to humans, with mucous membranes and skin serving as its only known reservoirs. GAS commonly causes a wide spectrum of infections in the upper respiratory tract and skin, ranging from mild, superficial infections to severe iGAS.[1][2] iGAS infections generally occur in normally sterile sites, such as the bloodstream, cerebrospinal fluid, or pleura.
Epidemiology
GAS exclusively infects humans[14], spreading through respiratory secretions, fomites, and direct contact with infected skin, such as in cases of impetigo. Although GAS infections can occur at any age, children, older adults, and immunocompromised individuals are at higher risk of becoming infected.[23] Environmental factors and time spent in communal settings, such as schools, households, and nursing homes, significantly increase the risk of transmission.[24] GAS can also cause disease in young, healthy individuals, with one study reporting its occurrence in 25 percent of people without identifiable risk factors.[24]
Pharyngitis
GAS can be found in the pharynx either as an asymptomatic carrier state or as a pathogen, causing pharyngitis. Approximately 5 to 15 percent of individuals in the general population are estimated to be GAS carriers. The World Health Organization (WHO) estimates that 600 million cases of GAS pharyngitis occur globally every year, with 80 percent in children and 20 percent in adults.[25] GAS pharyngitis most commonly occurs in children aged 5 to 15 years and is the leading bacterial cause of acute pharyngitis in this age group. It accounts for 5 to 15 percent of ambulatory care visits for acute pharyngitis in adults and 20 to 30 percent in children.[4][5][6] GAS pharyngitis usually occurs most frequently in the Winter and early Spring.[5] Pharyngitis caused by GAS typically results from person-to-person transmission through oropharyngeal secretions and respiratory droplets from infected individuals.[21][26]
Impetigo
Impetigo is a skin infection caused by Staphylococcus aureus, S pyogenes, or both bacteria. According to the WHO, an estimated 100 million cases of impetigo occur globally every year.[25] In the United States (US), more than 3 million cases of impetigo are estimated to occur each year. It is highly contagious and most frequently affects children between the ages of 2 and 5 years old. Risk factors include spending time in communal settings (eg, daycare centers, schools, correctional facilities, and homeless shelters) and poor personal hygiene. While impetigo can occur year-round, it is more common in areas with hot, humid summers and mild winters.
Scarlet Fever
It is estimated that fewer than 10 percent of persons with GAS pharyngitis will develop scarlet fever, which most commonly presents with exudative pharyngitis, fever, and the characteristic bright-red rash. Scarlet fever is caused by streptococcal pyrogenic exotoxins (SPEs) produced by GAS. A new emm1 sublineage, coined M1UK, was identified in 2008 in the United Kingdom (UK) and exhibited increased expression of the scarlet fever toxin and streptococcal pyrogenic exotoxin A (speA), leading to a rise in scarlet fever and invasive infections in the UK between 2014 and 2018. As a result, it became the dominant type in the country.[27][28][29] Following the COVID-19 pandemic, 3 emerging M1UK clades rapidly expanded across the UK, resulting in severe outcomes in children.[30] All globally sequenced M1UK isolates (speA) can be traced back to the UK, where they caused an epidemic and have since spread across Europe and internationally.[30] Although declining immunity may contribute to streptococcal outbreaks, the genetic characteristics of M1UK suggest a fitness advantage in pathogenicity and a remarkable ability to endure population bottlenecks. M1UK is now the dominant strain in England. In addition, 2 other lineages—M113SNPs and M123SNPs—were also identified.[30][31]
Cellulitis and Erysipelas
Cellulitis and erysipelas are skin infections commonly caused by S aureus and GAS. It is estimated that there were 43 million cases of cellulitis globally in 2019, resulting in over 18,000 deaths.[32] Approximately 10 percent of the cases are caused by GAS alone.[33] Risk factors for cellulitis include, among others, leg ulcers, lymphedema, congestive heart failure, venous insufficiency, diabetes mellitus, and lower socioeconomic status.[34]
iGAS
Globally, it is estimated that over 600,000 cases of iGAS occur every year, accounting for over 160,000 deaths.[25] In the US, the Centers for Disease Control and Prevention (CDC) estimates there are between 20,000 and 27,000 cases annually, accounting for around 2,000 deaths. In a population-based study covering nearly 35 million people in ten US states, there were over 21,000 cases of iGAS diagnosed from 2013 through 2022, accounting for almost 2000 deaths. Incidence rose from 3.6 infections per 100,000 persons in 2013 to 8.2 infections per 100,000 persons in 2022. Risk factors included persons experiencing homelessness, people who inject drugs, and residents of long-term care facilities.[35]
Severe illness and iGAS infections exhibit a bimodal distribution, occurring most commonly in individuals aged 2 years or younger and 50 years or older.[26][36] Risk factors associated with increased mortality include advanced age, male sex, nursing home residency, chronic underlying conditions, immunosuppression, recent surgery, septic shock, necrotizing fasciitis, concurrent viral infections, isolated bacteremia, and infection with emm type 1 or 3.[24][36]
Epidemiological surveillance is crucial for tracking epidemics, particularly given the increasing incidence and burden of GAS infections, especially iGAS, worldwide. Whole genome sequencing (WGS) plays an important role in this effort.[2][15][20][36][25] Since 2000, the dominant emm types in Europe and North America have been emm1 and emm3, with emm1 being the most prevalent among invasive infections in high-income countries.[30] The 7 emm types responsible for 50 to 70 percent of iGAS infections include emm1, emm28, emm89, emm3, emm12, emm4, and emm6 [15][37], which are collectively referred to as M1global.
RHD
It is estimated that over 15 million people are living with RHD, with an estimated 280,000 new cases of ARF occurring globally every year. The prevalence is highest in Sub-Saharan Africa, with an estimated 80 percent of RHD occurring in low and middle-income countries.[25] The single most important risk factor for RHD is failing to treat GAS pharyngitis with appropriate antibiotics, with other risk factors including living in overcrowded settings, poor personal hygiene, and limited access to healthcare.[38]
PSGN
An estimated 470,000 people develop acute PSGN globally every year, accounting for an estimated 5000 deaths.[25] As with RHD, the single most important risk factor for PSGN is failure to treat GAS pharyngitis with appropriate antibiotics. The same risk factors for GAS pharyngitis and impetigo also apply to PSGN.
Pathophysiology
GAS infections result from a complex interplay between host and bacterial factors that facilitate the establishment of infection. GAS utilizes various virulence factors, including toxins and other substances, to evade the host immune system and infect humans.[1] The hyaluronic acid capsule of GAS acts as a camouflage mechanism by resembling human hyaluronic acid, allowing the bacterium to evade immune detection. The surface-associated protein (S-protein) protects the bacterium from phagocytic destruction. Additionally, GAS produces proteases that degrade host immune signaling molecules and extracellular DNases to neutralize host immune defenses.[1]
Various surface substances, such as lipoteichoic acid and F-protein, enable GAS to adhere to host cells and facilitate colonization.[1] Cytolytic toxins, including streptolysins and hyaluronidase, contribute to tissue destruction, allowing GAS to invade the host.[1][39] Additionally, GAS has several factors, including its capsule, G protein, C5a peptidase, and M protein, that help it evade host immune defenses. Among these, M-protein is particularly significant for GAS virulence, as it inhibits the phagocytosis of host immune cells.[40]
Histopathology
Histopathological findings in GAS infections are typically characterized by acute inflammation and tissue destruction. Impetigo manifests as subcorneal pustules containing neutrophils and Gram-positive cocci. Deeper skin and soft tissue infections, such as cellulitis, will reveal diffuse edema and a neutrophil-rich infiltrate within the dermis and subcutaneous fat.
The hallmark of necrotizing fasciitis (NF) is extensive necrosis of the fascia and subcutaneous fat, often accompanied by vascular thrombosis and a lack of polymorphonuclear (PMN) leukocytes in the necrotic zones.
On light microscopy, PSGN will show diffuse endocapillary hypercellularity and exudative changes with neutrophils in the glomerular tufts. On electron microscopy, subepithelial "humps" (electron-dense deposits) can often be visualized. On immunofluorescence, a "starry sky" or "garland" pattern of C3 and IgG deposits along the capillary walls can be seen.
History and Physical
Obtaining a thorough history of the present illness and medical history is crucial for individuals presenting with GAS symptoms. GAS infections can present in diverse ways, influenced by factors such as the site of infection, toxin production, the invasiveness of the GAS strain, the patient's immune status, and whether the infection is superficial or deep. Clinicians must remain vigilant, as even mild-appearing infections can rapidly progress.
Pharyngitis
The most common symptoms of GAS pharyngitis are the sudden onset of fever and sore throat. Individuals with GAS pharyngitis, especially children, may also report headaches, nausea, vomiting, and abdominal pain.[8] When obtaining a patient history, it is common to identify exposure to a GAS infection, particularly among school-age children or individuals in communal living environments, such as nursing homes, where prevalence is higher due to close living conditions.
Physical exam findings in GAS pharyngitis commonly include generalized inflammation of the tonsils and pharynx, variable tonsillar exudates, a red, swollen uvula, and palatal petechiae. Tender cervical lymphadenopathy is frequently noted during palpation.[8] Symptoms such as conjunctivitis, cough, coryza, or diarrhea are uncommon and, when present, are more suggestive of a viral etiology.[41] Physical examination of the posterior oropharynx alone is insufficient to differentiate GAS from other causes of acute pharyngitis, such as viral pharyngitis, which is the most common cause of pharyngitis.
Impetigo
Impetigo typically occurs in school-aged children and is characterized by distinct cutaneous lesions described as discrete to confluent "honey-crusted" areas, most commonly on the face and extremities (see Image, Streptococcal impetigo). Usually, vital sign abnormalities are not associated with the clinical presentation, and the individual will have no additional physical examination findings apart from the characteristic lesions.[42]
Scarlet Fever
The diffuse erythematous rash characteristic of scarlet fever is usually associated with pharyngitis, petechiae on the soft palate, and tender cervical lymph nodes. A thorough skin examination will reveal the presence of a fine maculopapular erythematous "sandpaper" rash (see Image, scarlet fever rash on the forearm), along with a "strawberry tongue," which strongly suggests scarlet fever. The rash usually starts in the groin and axilla, expands to cover the trunk and extremities, and then desquamates. The palms and soles are usually spared. While scarlet fever is commonly associated with GAS streptococcal pharyngitis, it can also occur with iGAS infections.[43]
Cellulitis and Erysipelas
Cellulitis and erysipelas manifest as areas of redness, edema, and warmth on the skin. Fever may be present. They are typically unilateral and involve the lower extremities. While erysipelas involves the upper dermis and superficial lymphatic system, cellulitis involves the deeper dermis and subcutaneous fat. Erysipelas is well-demarcated, with sharp, raised borders, and is nonpurulent (see Image, Streptococcal erysipelas). Cellulitis tends to be less well demarcated, but when caused by GAS, it is typically nonpurulent.
iGAS
iGAS infections include NF and TSST-1 and are severe infections requiring prompt diagnosis and management, as affected individuals can deteriorate rapidly. NF is a critical, life-threatening soft tissue infection that involves the skin, subcutaneous tissue, and fascia. This can resemble cellulitis, making it easy to misdiagnose. One key finding in NF is that the pain is disproportionate to physical exam findings.[44] Clinicians must maintain a high level of suspicion, as misdiagnosis or treatment delays can lead to poor outcomes. Prompt intervention with aggressive surgical debridement and antibiotic therapy is critical.[45]
STSS is a severe and life-threatening condition caused by GAS. This condition results from an iGAS infection where bacterial enterotoxins are released, leading to severe systemic symptoms. STSS often develops following a primary GAS infection, particularly in deep wound infections. Clinically, individuals typically present with symptoms of severe sepsis, including tachycardia, hypotension, poor tissue perfusion, and signs of end-organ dysfunction.[46]
RHD
ARF typically presents 2 to 3 weeks after pharyngitis and characteristically causes rheumatic carditis, inflammation of the cardiac valves, most commonly the mitral and aortic valves. Valvular regurgitation results, which typically do not cause symptoms until they become severe, include symptomatic dyspnea and exercise intolerance. On exam, regurgitant murmurs can be detected on auscultation of the chest. Classically, mitral regurgitation presents with a holosystolic murmur.
PSGN
Acute PSGN may be asymptomatic, characterized only by microscopic hematuria and reduced serum complement, or may be symptomatic with acute nephritic syndrome, characterized by hematuria, edema, oliguria, and hypertension. In one prospective study, asymptomatic PSGN occurred four times as frequently as symptomatic PSGN.[47]
Evaluation
Pharyngitis
In an individual with symptoms of GAS pharyngitis and no symptoms of a viral infection, such as rhinorrhea, cough, hoarseness, oral ulcers, or conjunctivitis, it is prudent to proceed with GAS testing. GAS pharyngitis testing is recommended in:
- Symptomatic children less than 3 years of age who have risk factors for GAS infection, such as an older sibling with GAS infection
- Children 3 years and older and adolescents with symptoms of GAS infection
- Adults with symptoms compatible with GAS pharyngitis who lack symptoms of viral pharyngitis
Testing can include a rapid antigen detection test for GAS, molecular assays, or throat culture. In a systematic review, the rapid antigen test had a sensitivity of 86% and a specificity of 95%, although performance varied substantially across studies.[48] One major advantage of the rapid antigen test is that results are made available more quickly than with molecular testing and culture. Molecular assays such as polymerase chain reaction (PCR) and nucleic acid amplification tests (NAATs) are highly sensitive and specific for diagnosing GAS as well, but have a longer turnaround time than point-of-care tests. For both rapid antigen and NAAT tests, it is reasonable to forego a throat culture if the results are positive. If the results are negative, a throat culture should be performed. Throat culture has long been the gold standard for diagnosing GAS pharyngitis, although the turnaround time limits its usefulness.
The Centor criteria are used to estimate the probability of GAS pharyngitis using a clinical scoring system. A 2011 meta-analysis found that the Centor criteria had a sensitivity of 49 percent, meaning that around half of persons with GAS pharyngitis were missed. The specificity was higher at 82 percent, making it more helpful for ruling in people with likely GAS pharyngitis[49]
Impetigo
A diagnosis of impetigo is typically made clinically based on consistent physical exam findings. A Gram stain and culture can be performed to confirm the diagnosis, but they are typically not needed.
Scarlet Fever
As with impetigo, a diagnosis is made clinically in an individual with GAS pharyngitis and a characteristic erythematous rash and a strawberry tongue.
Cellulitis and Erysipelas
Cellulitis and erysipelas are typically made clinically. Imaging is not needed unless there are concerns for an underlying abscess, in which ultrasound can be helpful.
iGAS
If there is a clinical concern for an iGAS infection, such as NF, this is a surgical emergency, and a diagnosis is made in the operating room during exploration of the infected tissue. Although radiographic imaging, such as a computed tomography (CT) scan, can support the diagnosis, surgery should not be delayed while waiting for additional diagnostic studies. A diagnosis of STSS is made based on compatible clinical findings and isolation of GAS from a normally sterile site.
RHD
A diagnosis of RHD can be made when there is a history of acute rheumatic fever and a valvular abnormality on a transthoracic echocardiogram, as defined by the World Heart Federation criteria for RHD.[50] If there is no history of acute rheumatic fever, a diagnosis of RHD can be made if there are morphologic features of RHD of either the aortic valve or mitral valve.
PSGN
PSGN is typically diagnosed when there is a history of recent GAS infection and clinical findings of acute nephritis, such as hematuria, proteinuria, oliguria, edema, and hypertension.
Treatment / Management
Pharyngitis
GAS is among the few causes of pharyngitis for which antibiotics are recommended. Symptoms may resolve without treatment, but antibiotic therapy is important for reducing the risk of post-infectious complications. Antibiotics are not recommended for asymptomatic GAS carriers. Penicillin remains the treatment of choice for GAS pharyngitis. Oral penicillin V can be used in children, although amoxicillin is often preferred as the taste of amoxicillin in suspension is more palatable than that of penicillin, and oral penicillin V requires more frequent dosing. In adults, oral penicillin V is the preferred treatment, although oral amoxicillin can be used instead. A single intramuscular dose of penicillin G benzathine can also be used, particularly for individuals who are unlikely to complete the full course of oral antibiotics. For individuals with a penicillin allergy or who cannot take it, cephalosporins (such as cephalexin), clindamycin, and macrolides (such as azithromycin) can be used. A test of cure is typically not indicated for individuals whose symptoms resolve after completing antibiotics.
Impetigo
For individuals with limited impetigo, topical mupirocin or fusidic acid (if available) is usually effective. Both agents have activity against both S aureus and GAS. For individuals with systemic symptoms, such as fever, or who are at risk for complications (eg, immunosuppression), oral agents should be considered. An agent with a spectrum of activity against both S aureus and GAS, such as dicloxacillin or cephalexin, should be used. If impetigo is known to be caused by GAS only, oral penicillin V or amoxicillin should be used, with amoxicillin preferred, given the unpleasant taste of oral penicillin V and the more frequent dosing. Macrolides or clindamycin can alternatively be used to treat GAS-only impetigo.
Scarlet Fever
The treatment of scarlet fever is the same as for GAS pharyngitis. Either oral penicillin V or amoxicillin is preferred; cephalosporins, macrolides, or clindamycin can be used alternatively.
Cellulitis and Erysipelas
It is not always easy to differentiate between erysipelas and cellulitis, so typically infections are treated as cellulitis unless the diagnosis is clearly erysipelas. Treatment should always cover GAS as well as methicillin-sensitive S aureus (MSSA), and coverage should include methicillin-resistant S aureus (MRSA) if there are risk factors for MRSA (eg, known MRSA colonization or injection drug use), systemic symptoms, or purulence.
GAS causes most cases of erysipelas and can be managed as an outpatient with oral antibiotics, including penicillin V, amoxicillin, or cephalexin.
For individuals with cellulitis who are not severely ill, do not require parenteral antibiotics, and do not require MRSA coverage, empiric coverage for GAS and MSSA is indicated. Oral dicloxacillin or cephalexin is a good choice. If there is a severe beta-lactam allergy, trimethoprim-sulfamethoxazole, linezolid, or clindamycin can be used instead. If empiric coverage for MRSA is indicated, trimethoprim-sulfamethoxazole, amoxicillin plus doxycycline, linezolid, or clindamycin can be used. For individuals who require parenteral antibiotics, if MRSA coverage is not indicated, empiric coverage of GAS and MSSA with intravenous cefazolin, nafcillin, or oxacillin can be used. For GAS and MRSA coverage, intravenous vancomycin or daptomycin can be used. For severely ill individuals, broad-spectrum coverage is indicated with vancomycin or daptomycin plus cefepime or meropenem.
iGAS
The cornerstone of management for NF is prompt surgical exploration and debridement of necrotic tissue plus empiric broad-spectrum antibiotics. Empiric antibiotics should cover gram-positive, gram-negative, and anaerobic organisms and should be initiated immediately after blood cultures are obtained. Options include a carbapenem (eg, imipenem, meropenem, or ertapenem) or piperacillin-tazobactam plus vancomycin or daptomycin (to cover for MRSA) plus clindamycin. If NF is determined to be caused by GAS only, antibiotics can be narrowed to penicillin G plus clindamycin. The management of STSS includes treatment of septic shock and its associated complications, surgical debridement of infected tissue (if needed), and administration of intravenous immune globulin. Antibiotic therapy should empirically cover both GAS and MRSA, and both empiric and targeted antimicrobial therapy are the same as that for NF.
RHD
The management of RHD includes periodic echocardiographic evaluation of valvular abnormalities, prophylaxis against endocarditis for individuals undergoing invasive dental procedures, and valve repair or replacement if cardiac function deteriorates or symptoms of congestive heart failure become severe.
PSGN
If a GAS infection is present at the time of diagnosis, treatment of the underlying infection with penicillin or amoxicillin is indicated. Otherwise, management should focus on treating the clinical manifestations of PSGN, such as volume overload and hypertension. For individuals with severe PSGN, a kidney biopsy may be indicated if there is significant deterioration in renal function and/pr progression towards hemodialysis.
Antimicrobial Resistance
Although GAS remains susceptible to beta-lactams (eg, penicillin and amoxicillin), there is increasing resistance to alternative antibiotics such as macrolides and clindamycin. Reports from China indicate macrolide resistance rates as high as 90%, with resistance in some European countries ranging from 20% to 40% and lincosamide (eg, clindamycin) resistance reaching up to 19%. In other parts of Europe, these rates can be as low as 2%.[51][52] This resistance is attributed to multiple factors, including macrolide resistance mechanisms involving the MLSb phenotype.[51][52][53] There are rare reports of reduced susceptibility of GAS to beta-lactams[10][54][55], although no fully resistant GAS strains have been confirmed, and GAS remains uniformly susceptible to beta-lactams.(A1)
Differential Diagnosis
Pharyngitis
- Viral pharyngitis (eg, adenovirus, rhinovirus, Sars-CoV-2 and other coronaviruses, enteroviruses, influenza, parainfluenza, herpes simplex virus, Epstein-Barr virus, cytomegalovirus, respiratory syncytial virus)
- Acute HIV infection
- Groups C and G Streptococcus
- Neisseria gonorrhoeae
- Fusobacterium necrophorum
- Arcanobacterium haemolyticum
- Corynebcterium diptheriae
- Mycoplasma pneumoniae
- Tularemia
- Treponema pallidum
- Peritonsillar abscess, retropharyngeal abscess, Lemierre syndrome
- Non-infectious causes (eg, allergic rhinitis, gastroesophageal reflux disease, irritants such as smoke, trauma)
- Systemic diseases (eg, Kawasaki disease, Behcet syndrome)
Impetigo
- Herpes simplex virus
- Contact dermatitis
- Tinea infection
- Eczema
- Scabies
- Ecthyma
- Drug eruption
- Burns
- Arthropod bites
- Varicella
- Pyoderma gangrenosum
- Pemphigus vulgaris or bullous pemphigoid
- Erythema multiforme
Scarlet Fever
- Viral exanthems (eg, rubeola/measles, rubella, Fifth disease)
- Other bacterial infections (eg, non-GAS Streptococcal species, A haemolyticum
- Drug eruption
- Staphylococcal scaled skin syndrome
- Toxic shock syndrome
- Kawasaki disease
Cellulitis and Erysipelas
- Necrotizing fasciitis
- Toxic shock syndrome
- Clostridial myonecrosis/gas gangrene
- Erythema migrans
- Herpes zoster
- Septic bursitis
- Non-infectious causes (eg, contact dermatitis, gout, drug reaction, arthropod bite, deep vein thrombosis, panniculitis, vaccine site reaction, statis dermatitis [although this is usually bilateral], lymphadema)
iGAS
- Cellulitis or erysipelas
- Abscess
- Toxic shock syndrome
- Pyoderma gangrenosum
- Clostridial myonecrosis/gas gangrene
- Pyomyositis
- Deep vein thrombosis
- Acute compartment syndrome
- Vasculitis
RHD
- Mitral valve prolapse
- Infective endocarditis
- Congenital heart disease
- Viral myocarditis/carditis
- Degenerative valve disease
PSGN
- Non-PSGN causes of acute nephritis (eg, membranoproliferative glomerulonephritis, IgA nephropathy, lupus nephritis)
- C3 glomerulopathy
- Anti-GBM disease
- Hemolytic-uremic syndrome (HUS)
- Alport syndrome
- Thin basement membrane disease
Pertinent Studies and Ongoing Trials
As of March 2026, the following clinical trials of GAS were ongoing:
Prevention
- NCT07085702 is a multicenter, phase I, randomized, blinded study evaluating the safety and immunogenicity of three doses of two new formulations of a low-dose, medium-dose, and high-dose GAS vaccine.
- NCT07078357 is a single-center, phase I/IIa, randomized, double-blind, placebo-controlled, dose-escalation study evaluating the safety and immunogenicity of a GAS vaccine candidate (StreptInCor).
- NCT06370208 is a single-center, randomized, double-blind trial evaluating whether prophylactic use of S. salivarius eK12 can reduce the frequency and severity of GAS pharyngitis episodes in children.
Prognosis
The prognosis for most GAS infections is generally excellent, with the caveat that GAS can cause long-term sequelae, as previously discussed (eg, RHD and PSGN).
For GAS pharyngitis, symptoms typically resolve within a few days of starting antibiotics and will often resolve on their own, even without antibiotic treatment (although antibiotics are important for preventing long-term complications). Similarly, scarlet fever symptoms typically resolve within a couple of days of antibiotic treatment. Impetigo has an excellent prognosis, with most infections becoming noncontagious within 24 to 48 hours after treatment initiation. Symptoms usually start improving within 3 days of treatment initiation, with complete healing after a week or so.
Individuals with cellulitis or erysipelas typically experience symptom improvement within 24 to 48 hours after antibiotic initiation. If symptoms are not improving or are worsening, the differential diagnosis should be reevaluated.
NF carries a high mortality rate, even with appropriate management, with mortality rates ranging from 12 to 20 percent.[56][57][58][59] STSS carries an even poorer prognosis. In a systematic review and meta-analysis, STSS was associated with a mortality rate as high as 50 percent.[60][57]
The prognosis for RHD varies with the timeliness of detection, access to penicillin prophylaxis, and timely surgical intervention. In a prospective observational study from 24 low- and middle-income countries, nearly 15 percent of individuals with RHD died within 3 years, most commonly due to heart failure or sudden death.[61]
PSGN generally has a favorable prognosis. Over 90 percent of children recover completely within weeks to months, with only a small minority progressing to acute renal failure or persistent proteinuria and hematuria.[62] Adults who develop PSGN are more likely to have a worse outcome due to underlying renal dysfunction.
Complications
GAS is associated with significant morbidity and mortality if infections are not properly and promptly treated. In addition to causing infections, GAS can trigger immune-mediated sequelae, such as ARF and PSGN, as well as long-term sequelae such as RHD.[3] The valvular damage caused by ARF can be permanent and, in severe cases, may necessitate surgical intervention, including valve repair or replacement.[63]
Deterrence and Patient Education
Isolation and prevention of exposure are crucial in limiting the spread of viral and bacterial infections, including GAS. This is particularly important for conditions such as impetigo and GAS pharyngitis, which are highly contagious through saliva, droplets, and skin contact. These infections are common among school-age children who have frequent close contact with peers. Therefore, isolating individuals with GAS infections is crucial, as they should stay home from school, daycare, or work until they are no longer considered infectious. After 24 hours of antibiotic treatment, approximately 80% of patients are considered noninfectious.
Pearls and Other Issues
Key thoughts to consider when evaluating and treatint GAS infections are as follows:
- Children over 3 years of age with a negative rapid antigen detection test for GAS should have it confirmed by a throat culture for GAS. Individuals with clear viral symptoms (eg, runny nose, cough, hoarseness) do not need testing for GAS.
- Look for "sandpaper" rashes, petechiae on the soft palate, tender cervical lymphadenopathy, and a strawberry tongue.
- GAS is a leading cause of cellulitis and erysipelas, often presenting with rapid progression. In cases of recurrent lower-extremity cellulitis, check for underlying tinea pedis.
- Severe muscle aches, high persistent fever, rapid skin breakdown, hypotension, and mental status changes are signs of invasive GAS infection, such as NF or STSS.
- Rheumatic fever and glomerulonephritis are non-suppurative complications that can follow untreated or improperly treated infections.
Enhancing Healthcare Team Outcomes
Diagnosing and managing GAS infections, particularly iGAS such as NF and STSS, requires an interprofessional healthcare team, including infectious disease specialists, microbiologists, nursing staff, critical care specialists, and infectious disease pharmacists. One of the most important ways the healthcare team can improve patient outcomes is by promptly recognizing the signs of iGAS infections so they can be optimally managed. Early detection and appropriate management are essential in improving patient outcomes.
Healthcare professionals must be able to recognize signs of sepsis and shock, carefully evaluating physical examination findings, systemic signs of infection, and potential pathological foci. Timely recognition and intervention can significantly improve clinical outcomes, as severe iGAS infections require prompt antibiotic administration and additional treatments, such as surgery for NF or drainage of pleural effusion in GAS pneumonia. Effective management requires coordination among infectious disease specialists, clinicians, nursing staff, and pharmacists to ensure optimal care for these infections.
Media
(Click Image to Enlarge)
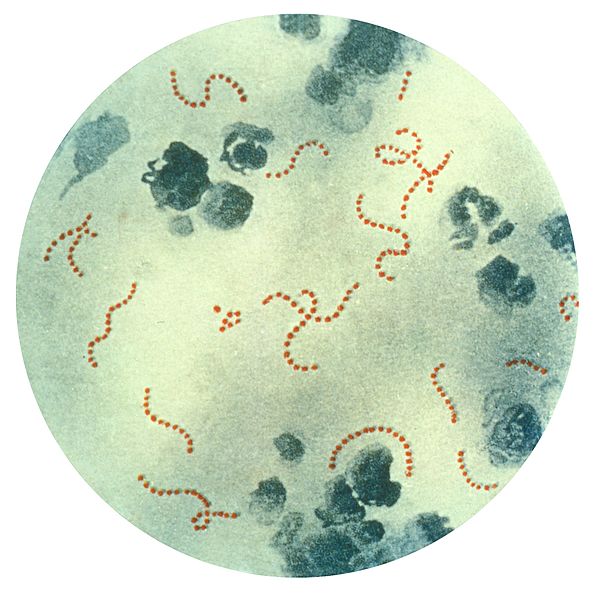
Streptococcus pyogenes Bacteria. This illustration depicts a photomicrograph of a specimen highlighting chain-linked S pyogenes bacteria.
Public Health Image Library, Public Domain, Centers for Disease Control and Prevention
(Click Image to Enlarge)
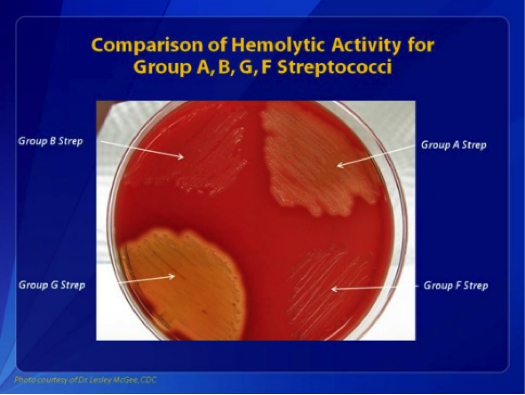
Comparisons of Hemolytic Activity of Groups A, B, G, and F Streptococci. Group B Streptococcus appears as small, colorless colonies and causes beta hemolysis in the shown culture.
Centers for Disease Control and Prevention
References
Brouwer S, Rivera-Hernandez T, Curren BF, Harbison-Price N, De Oliveira DMP, Jespersen MG, Davies MR, Walker MJ. Pathogenesis, epidemiology and control of Group A Streptococcus infection. Nature reviews. Microbiology. 2023 Jul:21(7):431-447. doi: 10.1038/s41579-023-00865-7. Epub 2023 Mar 9 [PubMed PMID: 36894668]
Dunne EM, Hutton S, Peterson E, Blackstock AJ, Hahn CG, Turner K, Carter KK. Increasing Incidence of Invasive Group A Streptococcus Disease, Idaho, USA, 2008-2019. Emerging infectious diseases. 2022 Sep:28(9):1785-1795. doi: 10.3201/eid2809.212129. Epub [PubMed PMID: 35997313]
Martin JM, Green M. Group A streptococcus. Seminars in pediatric infectious diseases. 2006 Jul:17(3):140-8 [PubMed PMID: 16934708]
Oliver J, Malliya Wadu E, Pierse N, Moreland NJ, Williamson DA, Baker MG. Group A Streptococcus pharyngitis and pharyngeal carriage: A meta-analysis. PLoS neglected tropical diseases. 2018 Mar:12(3):e0006335. doi: 10.1371/journal.pntd.0006335. Epub 2018 Mar 19 [PubMed PMID: 29554121]
Level 1 (high-level) evidenceShulman ST, Bisno AL, Clegg HW, Gerber MA, Kaplan EL, Lee G, Martin JM, Van Beneden C, Infectious Diseases Society of America. Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2012 Nov 15:55(10):e86-102. doi: 10.1093/cid/cis629. Epub 2012 Sep 9 [PubMed PMID: 22965026]
Level 1 (high-level) evidenceCarville KS, Meagher N, Abo YN, Manski-Nankervis JA, Fielding J, Steer A, McVernon J, Price DJ. Burden of antimicrobial prescribing in primary care attributable to sore throat: a retrospective cohort study of patient record data. BMC primary care. 2024 Apr 17:25(1):117. doi: 10.1186/s12875-024-02371-y. Epub 2024 Apr 17 [PubMed PMID: 38632513]
Level 2 (mid-level) evidenceWorrall G, Hutchinson J, Sherman G, Griffiths J. Diagnosing streptococcal sore throat in adults: randomized controlled trial of in-office aids. Canadian family physician Medecin de famille canadien. 2007 Apr:53(4):666-71 [PubMed PMID: 17872717]
Level 1 (high-level) evidenceShulman ST, Bisno AL, Clegg HW, Gerber MA, Kaplan EL, Lee G, Martin JM, Van Beneden C. Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2012 Nov 15:55(10):1279-82. doi: 10.1093/cid/cis847. Epub [PubMed PMID: 23091044]
Level 1 (high-level) evidenceFleming-Dutra KE, Hersh AL, Shapiro DJ, Bartoces M, Enns EA, File TM Jr, Finkelstein JA, Gerber JS, Hyun DY, Linder JA, Lynfield R, Margolis DJ, May LS, Merenstein D, Metlay JP, Newland JG, Piccirillo JF, Roberts RM, Sanchez GV, Suda KJ, Thomas A, Woo TM, Zetts RM, Hicks LA. Prevalence of Inappropriate Antibiotic Prescriptions Among US Ambulatory Care Visits, 2010-2011. JAMA. 2016 May 3:315(17):1864-73. doi: 10.1001/jama.2016.4151. Epub [PubMed PMID: 27139059]
Vannice KS, Ricaldi J, Nanduri S, Fang FC, Lynch JB, Bryson-Cahn C, Wright T, Duchin J, Kay M, Chochua S, Van Beneden CA, Beall B. Streptococcus pyogenes pbp2x Mutation Confers Reduced Susceptibility to β-Lactam Antibiotics. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2020 Jun 24:71(1):201-204. doi: 10.1093/cid/ciz1000. Epub [PubMed PMID: 31630171]
DeMuri GP, Sterkel AK, Kubica PA, Duster MN, Reed KD, Wald ER. Macrolide and Clindamycin Resistance in Group a Streptococci Isolated From Children With Pharyngitis. The Pediatric infectious disease journal. 2017 Mar:36(3):342-344. doi: 10.1097/INF.0000000000001442. Epub [PubMed PMID: 27902646]
Shaikh N, Swaminathan N, Hooper EG. Accuracy and precision of the signs and symptoms of streptococcal pharyngitis in children: a systematic review. The Journal of pediatrics. 2012 Mar:160(3):487-493.e3. doi: 10.1016/j.jpeds.2011.09.011. Epub 2011 Nov 1 [PubMed PMID: 22048053]
Level 1 (high-level) evidenceMarston HD, Dixon DM, Knisely JM, Palmore TN, Fauci AS. Antimicrobial Resistance. JAMA. 2016 Sep 20:316(11):1193-1204. doi: 10.1001/jama.2016.11764. Epub [PubMed PMID: 27654605]
Gera K, McIver KS. Laboratory growth and maintenance of Streptococcus pyogenes (the Group A Streptococcus, GAS). Current protocols in microbiology. 2013 Oct 2:30():9D.2.1-9D.2.13. doi: 10.1002/9780471729259.mc09d02s30. Epub 2013 Oct 2 [PubMed PMID: 24510893]
Gherardi G, Vitali LA, Creti R. Prevalent emm Types among Invasive GAS in Europe and North America since Year 2000. Frontiers in public health. 2018:6():59. doi: 10.3389/fpubh.2018.00059. Epub 2018 Mar 9 [PubMed PMID: 29662874]
van Sorge NM, Cole JN, Kuipers K, Henningham A, Aziz RK, Kasirer-Friede A, Lin L, Berends ETM, Davies MR, Dougan G, Zhang F, Dahesh S, Shaw L, Gin J, Cunningham M, Merriman JA, Hütter J, Lepenies B, Rooijakkers SHM, Malley R, Walker MJ, Shattil SJ, Schlievert PM, Choudhury B, Nizet V. The classical lancefield antigen of group a Streptococcus is a virulence determinant with implications for vaccine design. Cell host & microbe. 2014 Jun 11:15(6):729-740. doi: 10.1016/j.chom.2014.05.009. Epub [PubMed PMID: 24922575]
Lancefield RC. THE ANTIGENIC COMPLEX OF STREPTOCOCCUS HAEMOLYTICUS : I. DEMONSTRATION OF A TYPE-SPECIFIC SUBSTANCE IN EXTRACTS OF STREPTOCOCCUS HAEMOLYTICUS. The Journal of experimental medicine. 1928 Jan 1:47(1):91-103 [PubMed PMID: 19869404]
Raabe VN, Shane AL. Group B Streptococcus (Streptococcus agalactiae). Microbiology spectrum. 2019 Mar:7(2):. doi: 10.1128/microbiolspec.GPP3-0007-2018doi: 10.1128/microbiolspec.gpp3-0007-2018. Epub [PubMed PMID: 30900541]
Sanderson-Smith M, De Oliveira DM, Guglielmini J, McMillan DJ, Vu T, Holien JK, Henningham A, Steer AC, Bessen DE, Dale JB, Curtis N, Beall BW, Walker MJ, Parker MW, Carapetis JR, Van Melderen L, Sriprakash KS, Smeesters PR, M Protein Study Group. A systematic and functional classification of Streptococcus pyogenes that serves as a new tool for molecular typing and vaccine development. The Journal of infectious diseases. 2014 Oct 15:210(8):1325-38. doi: 10.1093/infdis/jiu260. Epub 2014 May 5 [PubMed PMID: 24799598]
Level 1 (high-level) evidenceTagini F, Aubert B, Troillet N, Pillonel T, Praz G, Crisinel PA, Prod'hom G, Asner S, Greub G. Importance of whole genome sequencing for the assessment of outbreaks in diagnostic laboratories: analysis of a case series of invasive Streptococcus pyogenes infections. European journal of clinical microbiology & infectious diseases : official publication of the European Society of Clinical Microbiology. 2017 Jul:36(7):1173-1180. doi: 10.1007/s10096-017-2905-z. Epub 2017 Jan 26 [PubMed PMID: 28124734]
Level 2 (mid-level) evidenceWalker MJ, Barnett TC, McArthur JD, Cole JN, Gillen CM, Henningham A, Sriprakash KS, Sanderson-Smith ML, Nizet V. Disease manifestations and pathogenic mechanisms of Group A Streptococcus. Clinical microbiology reviews. 2014 Apr:27(2):264-301. doi: 10.1128/CMR.00101-13. Epub [PubMed PMID: 24696436]
Level 3 (low-level) evidenceAtchade E, De Tymowski C, Grall N, Tanaka S, Montravers P. Toxic Shock Syndrome: A Literature Review. Antibiotics (Basel, Switzerland). 2024 Jan 18:13(1):. doi: 10.3390/antibiotics13010096. Epub 2024 Jan 18 [PubMed PMID: 38247655]
Avire NJ, Whiley H, Ross K. A Review of Streptococcus pyogenes: Public Health Risk Factors, Prevention and Control. Pathogens (Basel, Switzerland). 2021 Feb 22:10(2):. doi: 10.3390/pathogens10020248. Epub 2021 Feb 22 [PubMed PMID: 33671684]
Lamagni TL, Darenberg J, Luca-Harari B, Siljander T, Efstratiou A, Henriques-Normark B, Vuopio-Varkila J, Bouvet A, Creti R, Ekelund K, Koliou M, Reinert RR, Stathi A, Strakova L, Ungureanu V, Schalén C, Strep-EURO Study Group, Jasir A. Epidemiology of severe Streptococcus pyogenes disease in Europe. Journal of clinical microbiology. 2008 Jul:46(7):2359-67. doi: 10.1128/JCM.00422-08. Epub 2008 May 7 [PubMed PMID: 18463210]
Level 3 (low-level) evidenceCarapetis JR, Steer AC, Mulholland EK, Weber M. The global burden of group A streptococcal diseases. The Lancet. Infectious diseases. 2005 Nov:5(11):685-94 [PubMed PMID: 16253886]
Thompson KM, Sterkel AK, McBride JA, Corliss RF. The Shock of Strep: Rapid Deaths Due to Group a Streptococcus. Academic forensic pathology. 2018 Mar:8(1):136-149. doi: 10.23907/2018.010. Epub 2018 Mar 7 [PubMed PMID: 31240031]
Zhi X, Li HK, Li H, Loboda Z, Charles S, Vieira A, Huse K, Jauneikaite E, Reeves L, Mok KY, Coelho J, Lamagni T, Sriskandan S. Emerging Invasive Group A Streptococcus M1(UK) Lineage Detected by Allele-Specific PCR, England, 2020(1). Emerging infectious diseases. 2023 May:29(5):1007-1010. doi: 10.3201/eid2905.221887. Epub 2023 Apr 5 [PubMed PMID: 37019153]
Lamagni T, Guy R, Chand M, Henderson KL, Chalker V, Lewis J, Saliba V, Elliot AJ, Smith GE, Rushton S, Sheridan EA, Ramsay M, Johnson AP. Resurgence of scarlet fever in England, 2014-16: a population-based surveillance study. The Lancet. Infectious diseases. 2018 Feb:18(2):180-187. doi: 10.1016/S1473-3099(17)30693-X. Epub 2017 Nov 27 [PubMed PMID: 29191628]
Lynskey NN, Jauneikaite E, Li HK, Zhi X, Turner CE, Mosavie M, Pearson M, Asai M, Lobkowicz L, Chow JY, Parkhill J, Lamagni T, Chalker VJ, Sriskandan S. Emergence of dominant toxigenic M1T1 Streptococcus pyogenes clone during increased scarlet fever activity in England: a population-based molecular epidemiological study. The Lancet. Infectious diseases. 2019 Nov:19(11):1209-1218. doi: 10.1016/S1473-3099(19)30446-3. Epub 2019 Sep 10 [PubMed PMID: 31519541]
Level 2 (mid-level) evidenceVieira A, Wan Y, Ryan Y, Li HK, Guy RL, Papangeli M, Huse KK, Reeves LC, Soo VWC, Daniel R, Harley A, Broughton K, Dhami C, Ganner M, Ganner MA, Mumin Z, Razaei M, Rundberg E, Mammadov R, Mills EA, Sgro V, Mok KY, Didelot X, Croucher NJ, Jauneikaite E, Lamagni T, Brown CS, Coelho J, Sriskandan S. Rapid expansion and international spread of M1(UK) in the post-pandemic UK upsurge of Streptococcus pyogenes. Nature communications. 2024 May 10:15(1):3916. doi: 10.1038/s41467-024-47929-7. Epub 2024 May 10 [PubMed PMID: 38729927]
Li HK, Zhi X, Vieira A, Whitwell HJ, Schricker A, Jauneikaite E, Li H, Yosef A, Andrew I, Game L, Turner CE, Lamagni T, Coelho J, Sriskandan S. Characterization of emergent toxigenic M1(UK) Streptococcus pyogenes and associated sublineages. Microbial genomics. 2023 Apr:9(4):. doi: 10.1099/mgen.0.000994. Epub [PubMed PMID: 37093716]
Miller KM, Lamagni T, Hay R, Cannon JW, Marks M, Bowen AC, Kaslow DC, Cherian T, Seale AC, Pickering J, Daw JN, Moore HC, Van Beneden C, Carapetis JR, Manning L. Standardization of Epidemiological Surveillance of Group A Streptococcal Cellulitis(). Open forum infectious diseases. 2022 Sep:9(Suppl 1):S25-S30. doi: 10.1093/ofid/ofac267. Epub 2022 Sep 15 [PubMed PMID: 36128406]
Level 2 (mid-level) evidenceBruun T, Oppegaard O, Kittang BR, Mylvaganam H, Langeland N, Skrede S. Etiology of Cellulitis and Clinical Prediction of Streptococcal Disease: A Prospective Study. Open forum infectious diseases. 2016 Jan:3(1):ofv181. doi: 10.1093/ofid/ofv181. Epub 2015 Nov 25 [PubMed PMID: 26734653]
Curman P, Dräger S, Olbrich H, Hernandez G, Bieber K, Gaffal E, Kahle B, Kridin K, Szymczak S, Ludwig RJ. Identifying common risk factors for primary cellulitis in a large-scale retrospective cohort study. International journal of infectious diseases : IJID : official publication of the International Society for Infectious Diseases. 2026 May:166():108494. doi: 10.1016/j.ijid.2026.108494. Epub 2026 Feb 19 [PubMed PMID: 41722760]
Level 2 (mid-level) evidenceGregory CJ, Okaro JO, Reingold A, Chai S, Herlihy R, Petit S, Farley MM, Harrison LH, Como-Sabetti K, Lynfield R, Snippes Vagnone P, Sosin D, Anderson BJ, Burzlaff K, Martin T, Thomas A, Schaffner W, Talbot HK, Beall B, Chochua S, Chung Y, Park S, Van Beneden C, Li Y, Schrag SJ. Invasive Group A Streptococcal Infections in 10 US States. JAMA. 2025 May 6:333(17):1498-1507. doi: 10.1001/jama.2025.0910. Epub [PubMed PMID: 40193120]
Nelson GE, Pondo T, Toews KA, Farley MM, Lindegren ML, Lynfield R, Aragon D, Zansky SM, Watt JP, Cieslak PR, Angeles K, Harrison LH, Petit S, Beall B, Van Beneden CA. Epidemiology of Invasive Group A Streptococcal Infections in the United States, 2005-2012. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2016 Aug 15:63(4):478-86. doi: 10.1093/cid/ciw248. Epub 2016 Apr 22 [PubMed PMID: 27105747]
Luca-Harari B, Darenberg J, Neal S, Siljander T, Strakova L, Tanna A, Creti R, Ekelund K, Koliou M, Tassios PT, van der Linden M, Straut M, Vuopio-Varkila J, Bouvet A, Efstratiou A, Schalén C, Henriques-Normark B, Strep-EURO Study Group, Jasir A. Clinical and microbiological characteristics of severe Streptococcus pyogenes disease in Europe. Journal of clinical microbiology. 2009 Apr:47(4):1155-65. doi: 10.1128/JCM.02155-08. Epub 2009 Jan 21 [PubMed PMID: 19158266]
Mendoza RF, Mutarelli A, Mendoza BF, Barbosa JAA, Oliveira RL, Nascimento BR, Pantaleão AN, Fonseca IMG, Oliveira MAR, Pinto AS, Beaton A, Nunes MCP. Risk Factors for Acute Rheumatic Disease: Exploring Factors at Individual and Collective Levels. Revista da Sociedade Brasileira de Medicina Tropical. 2024:57():. pii: S0037-86822024000100302. doi: 10.1590/0037-8682-0139-2024. Epub 2024 Nov 15 [PubMed PMID: 39570153]
Starr CR, Engleberg NC. Role of hyaluronidase in subcutaneous spread and growth of group A streptococcus. Infection and immunity. 2006 Jan:74(1):40-8 [PubMed PMID: 16368955]
Heath A, DiRita VJ, Barg NL, Engleberg NC. A two-component regulatory system, CsrR-CsrS, represses expression of three Streptococcus pyogenes virulence factors, hyaluronic acid capsule, streptolysin S, and pyrogenic exotoxin B. Infection and immunity. 1999 Oct:67(10):5298-305 [PubMed PMID: 10496909]
Level 3 (low-level) evidenceSchroeder BM. Diagnosis and management of group A streptococcal pharyngitis. American family physician. 2003 Feb 15:67(4):880, 883-4 [PubMed PMID: 12613739]
Pereira LB. Impetigo - review. Anais brasileiros de dermatologia. 2014 Mar-Apr:89(2):293-9 [PubMed PMID: 24770507]
Hurst JR, Brouwer S, Walker MJ, McCormick JK. Streptococcal superantigens and the return of scarlet fever. PLoS pathogens. 2021 Dec:17(12):e1010097. doi: 10.1371/journal.ppat.1010097. Epub 2021 Dec 30 [PubMed PMID: 34969060]
Kanagasabai A, Evans C, Jones HE, Hay AD, Dawson S, Savović J, Elwenspoek MMC. Systematic review and meta-analysis of the accuracy of McIsaac and Centor score in patients presenting to secondary care with pharyngitis. Clinical microbiology and infection : the official publication of the European Society of Clinical Microbiology and Infectious Diseases. 2024 Apr:30(4):445-452. doi: 10.1016/j.cmi.2023.12.025. Epub 2024 Jan 3 [PubMed PMID: 38182052]
Level 1 (high-level) evidenceBellapianta JM, Ljungquist K, Tobin E, Uhl R. Necrotizing fasciitis. The Journal of the American Academy of Orthopaedic Surgeons. 2009 Mar:17(3):174-82 [PubMed PMID: 19264710]
Schmitz M, Roux X, Huttner B, Pugin J. Streptococcal toxic shock syndrome in the intensive care unit. Annals of intensive care. 2018 Sep 17:8(1):88. doi: 10.1186/s13613-018-0438-y. Epub 2018 Sep 17 [PubMed PMID: 30225523]
Rodríguez-Iturbe B, Rubio L, García R. Attack rate of poststreptococcal nephritis in families. A prospective study. Lancet (London, England). 1981 Feb 21:1(8217):401-3 [PubMed PMID: 6110037]
Cohen JF, Bertille N, Cohen R, Chalumeau M. Rapid antigen detection test for group A streptococcus in children with pharyngitis. The Cochrane database of systematic reviews. 2016 Jul 4:7(7):CD010502. doi: 10.1002/14651858.CD010502.pub2. Epub 2016 Jul 4 [PubMed PMID: 27374000]
Level 1 (high-level) evidenceAalbers J, O'Brien KK, Chan WS, Falk GA, Teljeur C, Dimitrov BD, Fahey T. Predicting streptococcal pharyngitis in adults in primary care: a systematic review of the diagnostic accuracy of symptoms and signs and validation of the Centor score. BMC medicine. 2011 Jun 1:9():67. doi: 10.1186/1741-7015-9-67. Epub 2011 Jun 1 [PubMed PMID: 21631919]
Level 1 (high-level) evidenceRwebembera J, Marangou J, Mwita JC, Mocumbi AO, Mota C, Okello E, Nascimento B, Thorup L, Beaton A, Kado J, Kaethner A, Kumar RK, Lawrenson J, Marijon E, Mirabel M, Nunes MCP, Piñeiro D, Pinto F, Ralston K, Sable C, Sanyahumbi A, Saxena A, Sliwa K, Steer A, Viali S, Wheaton G, Wilson N, Zühlke L, Reményi B. 2023 World Heart Federation guidelines for the echocardiographic diagnosis of rheumatic heart disease. Nature reviews. Cardiology. 2024 Apr:21(4):250-263. doi: 10.1038/s41569-023-00940-9. Epub 2023 Nov 2 [PubMed PMID: 37914787]
Rafei R, Al Iaali R, Osman M, Dabboussi F, Hamze M. A global snapshot on the prevalent macrolide-resistant emm types of Group A Streptococcus worldwide, their phenotypes and their resistance marker genotypes during the last two decades: A systematic review. Infection, genetics and evolution : journal of molecular epidemiology and evolutionary genetics in infectious diseases. 2022 Apr:99():105258. doi: 10.1016/j.meegid.2022.105258. Epub 2022 Feb 24 [PubMed PMID: 35219865]
Level 1 (high-level) evidenceGergova R, Boyanov V, Muhtarova A, Alexandrova A. A Review of the Impact of Streptococcal Infections and Antimicrobial Resistance on Human Health. Antibiotics (Basel, Switzerland). 2024 Apr 15:13(4):. doi: 10.3390/antibiotics13040360. Epub 2024 Apr 15 [PubMed PMID: 38667036]
Sun L, Xiao Y, Huang W, Lai J, Lyu J, Ye B, Chen H, Gu B. Prevalence and identification of antibiotic-resistant scarlet fever group A Streptococcus strains in some paediatric cases at Shenzhen, China. Journal of global antimicrobial resistance. 2022 Sep:30():199-204. doi: 10.1016/j.jgar.2022.05.012. Epub 2022 May 23 [PubMed PMID: 35618209]
Level 3 (low-level) evidenceBeres SB, Zhu L, Pruitt L, Olsen RJ, Faili A, Kayal S, Musser JM. Integrative Reverse Genetic Analysis Identifies Polymorphisms Contributing to Decreased Antimicrobial Agent Susceptibility in Streptococcus pyogenes. mBio. 2022 Feb 22:13(1):e0361821. doi: 10.1128/mbio.03618-21. Epub 2022 Jan 18 [PubMed PMID: 35038921]
Capoor MR, Nair D, Deb M, Batra K, Aggarwal P. Resistance to erythromycin and rising penicillin MIC in Streptococcus pyogenes in India. Japanese journal of infectious diseases. 2006 Oct:59(5):334-6 [PubMed PMID: 17060703]
Chen Y, Huang Y, Shou J, Song R, Tan J, Deng J. Epidemiology and prognostic factors of necrotizing fasciitis in resource-limited regions based on 119 cases. Scientific reports. 2025 Jul 28:15(1):27458. doi: 10.1038/s41598-025-13278-8. Epub 2025 Jul 28 [PubMed PMID: 40721651]
Level 3 (low-level) evidenceMegas IF, Delavari S, Marti Edo A, Habild G, Billner M, Reichert B, Breidung D. Prognostic Factors in Necrotizing Fasciitis: Insights from a Two-Decade, Two-Center Study Involving 209 Cases. Infectious disease reports. 2024 May 16:16(3):472-480. doi: 10.3390/idr16030035. Epub 2024 May 16 [PubMed PMID: 38804445]
Level 3 (low-level) evidenceKhamnuan P, Chongruksut W, Jearwattanakanok K, Patumanond J, Yodluangfun S, Tantraworasin A. Necrotizing fasciitis: risk factors of mortality. Risk management and healthcare policy. 2015:8():1-7. doi: 10.2147/RMHP.S77691. Epub 2015 Feb 16 [PubMed PMID: 25733938]
Bodansky DMS, Begaj I, Evison F, Webber M, Woodman CB, Tucker ON. A 16-year Longitudinal Cohort Study of Incidence and Bacteriology of Necrotising Fasciitis in England. World journal of surgery. 2020 Aug:44(8):2580-2591. doi: 10.1007/s00268-020-05559-2. Epub [PubMed PMID: 32383053]
Auger N, Carrier FM, Waechter J, Brousseau É, Maniraho A, Ayoub A, Bégin P. Long-term outcomes of patients with toxic shock syndrome: A matched cohort study. The Journal of infection. 2024 Aug:89(2):106213. doi: 10.1016/j.jinf.2024.106213. Epub 2024 Jun 27 [PubMed PMID: 38944286]
Karthikeyan G, Ntsekhe M, Islam S, Rangarajan S, Avezum A, Benz A, Cabral TTJ, Changsheng M, Chillo P, Gonzalez-Hermosillo JA, Gitura B, Damasceno A, Dans AML, Davletov K, Elghamrawy A, ElSayed A, Fana GT, Gondwe L, Haileamlak A, Kayani AM, Lwabi P, Maklady F, Molefe-Baikai OJ, Musuku J, Ogah OS, Paniagua M, Rusingiza E, Sharma SK, Zuhlke L, Connolly S, Yusuf S, INVICTUS Investigators. Mortality and Morbidity in Adults With Rheumatic Heart Disease. JAMA. 2024 Jul 9:332(2):133-140. doi: 10.1001/jama.2024.8258. Epub [PubMed PMID: 38837131]
Ong LT. Management and outcomes of acute post-streptococcal glomerulonephritis in children. World journal of nephrology. 2022 Sep 25:11(5):139-145. doi: 10.5527/wjn.v11.i5.139. Epub [PubMed PMID: 36187464]
Carapetis JR, Beaton A, Cunningham MW, Guilherme L, Karthikeyan G, Mayosi BM, Sable C, Steer A, Wilson N, Wyber R, Zühlke L. Acute rheumatic fever and rheumatic heart disease. Nature reviews. Disease primers. 2016 Jan 14:2():15084. doi: 10.1038/nrdp.2015.84. Epub 2016 Jan 14 [PubMed PMID: 27188830]