Introduction
The spleen constitutes the largest organ of the lymphatic system, located in the left hypochondriac region between the diaphragm and gastric fundus, typically spanning the ninth to 11th ribs. The organ is highly vascular, reddish-purple, and enclosed by a thin connective tissue capsule that permits limited expansion. The spleen has diaphragmatic and visceral surfaces, distinct borders, and a hilum transmitting splenic vessels, nerves, and ligamentous attachments. Visceral impressions reflect close relationships with the stomach, left kidney, colon, and pancreatic tail. Primary functions include blood filtration, immune surveillance, and sequestration of blood elements (see Image. Spleen Anatomy).
The spleen is clinically significant because traumatic injury, rupture, or splenomegaly may result in life-threatening hemorrhage. Surgical management includes splenic repair, partial splenectomy based on vascular segmentation, or complete splenectomy, often performed laparoscopically when feasible. Knowledge of splenic anatomy guides operative planning and reduces the risk of iatrogenic injury to adjacent structures. Understanding splenic physiology informs postsplenectomy management, including vaccination strategies to mitigate increased susceptibility to encapsulated bacterial infections.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Structure
The spleen is the largest organ of the lymphatic system, positioned between the fundus of the stomach and the diaphragm in the left hypochondriac region of the abdominal cavity, relatively below the left costal margin between the ninth and eleventh ribs. The organ is spongy and appears reddish-purple due to dense vascularization. The spleen is typically not palpable on routine physical examination.
The spleen is encased in a thin connective tissue capsule that protects it and allows it to expand. The internal parenchyma is subdivided into multiple smaller sections termed "lobules." The spleen comprises anterior and posterior segments and rests on the upper pole of the left kidney and the tail of the pancreas.
Three distinct borders define the spleen: superior, inferior, and intermediate. The superior border possesses a notch on its anterior end. The organ has 2 surfaces, visceral and diaphragmatic. The diaphragmatic surface is convex and smooth, whereas the visceral surface is concave and irregular, displaying multiple impressions. The most concave visceral imprint results from the fundus of the stomach. The left kidney leaves an imprint on the intermediate and inferior borders. The splenic flexure of the colon produces the colic impression. The tail of the pancreas forms an imprint between the hilum and colic impression sites.
The splenic hilum is located on the inferomedial aspect of the gastric impression. This region transmits nerves and splenic vessels and provides attachments for the splenorenal and gastrosplenic ligaments. The spleen measures approximately 10 to 12 cm (3.94–4.72 in) and weighs about 150 to 200 g (5.29–7.05 oz).[1][2][3]
The microscopic architecture of the spleen is defined by distinct white pulp and red pulp compartments separated by the marginal zone. White pulp consists of periarteriolar lymphoid sheaths (PALS) surrounding central arterioles and discrete lymphoid follicles composed of dense lymphoid tissue. The marginal zone is a transition region between the white and red pulp that contains specialized macrophage and lymphocyte populations at its interface.
Red pulp occupies the majority of the splenic parenchyma and is composed of a reticular connective tissue network supporting cords of Billroth and venous sinusoids. Cords of Billroth are irregular, anastomosing strands of reticular fibers and fibroblasts that form a densely packed meshwork, densely populated by red blood cells, white blood cells (particularly macrophages), and platelets. These cords fill the interstitial space between sinusoids and provide a scaffold through which blood elements are organized prior to entering the venous circulation. Splenic sinusoids are elongated, tubular channels lined by specialized endothelial cells with fenestrations and discontinuous basal laminae, forming open spaces that communicate with cords of Billroth. Trabecular connective tissue extends from the fibrous capsule into the parenchyma, providing structural support and a conduit for splenic vasculature. The arrangement of cords and sinusoids establishes a distinctive microscopic architecture, with cords appearing as dense, cellular networks interspersed with the paler, open lumens of the sinusoidal channels.
Function
The spleen performs multiple critical roles in hematologic and immunologic regulation. White pulp serves as a site for lymphocyte production and maturation, supporting both B and T cell populations and enabling antibody synthesis in response to antigenic stimulation. Red pulp is primarily responsible for blood filtration, facilitating the removal of senescent, damaged, or otherwise defective red blood cells. Macrophages in the red pulp identify and destroy microorganisms, including viruses, bacteria, and fungi, thereby contributing to host defense.
The marginal zone mediates interactions between circulating blood elements and lymphoid tissue, directing pathogens into the white pulp for immune processing.[4] The red pulp also serves as a reservoir for leukocytes and platelets, which can be rapidly mobilized to sites of injury, participate in regulating inflammation, and support hemostatic compensation during blood loss. Although not a vital organ, the spleen’s integrated functions in blood surveillance, immune defense, and cellular storage are essential for optimal hematologic and immunologic homeostasis.
Embryology
The spleen originates from mesenchymal cells of the mesoderm situated between the tiers of the dorsal mesogastrium as early as the fifth and sixth weeks of fetal development. The characteristic shape of the spleen is established early in the fetal period. Rotation of the stomach during embryonic development causes the left mesogastrium surface to fuse with the peritoneum above the left kidney, resulting in the dorsal attachment of the lienorenal ligament. The yolk sac wall and the area near the dorsal aorta provide cells required for the hemopoietic function of the spleen. By the second trimester, the spleen is capable of generating both red and white blood cells.
Blood Supply and Lymphatics
As mentioned, the spleen is highly vascularized. The splenic artery provides the primary arterial supply, entering the splenic hilum near the middle of the visceral surface.[5] This blood vessel originates from the celiac trunk and courses within the splenorenal ligament, laterally and across the superior aspect of the pancreas. Upon approaching the spleen, the splenic artery divides into 5 branches, each supplying distinct regions of the organ. This arrangement results in vascular segmentation of the spleen, as the 5 subbranches do not anastomose. Venous drainage occurs via the splenic vein, which emerges from the hilum, passes posterior to the pancreas, and joins the superior mesenteric vein to form the portal vein.
As a major lymphatic organ, the spleen contains lymphatic vessels, some of which arise from the capsule rather than from the proper splenic tissue. Only efferent lymphatic vessels are present. Consequently, the spleen functions analogously to a large lymph node. These vessels supply lymph to neighboring nodes, including the pancreaticosplenic lymph nodes.
Nerves
Sympathetic fibers supplying the spleen originate from the celiac plexus. Parasympathetic fibers derive from the vagus nerve (cranial nerve X).
Physiologic Variants
The spleen exhibits several natural physiological variations, most commonly relating to organ size, with differences generally minimal. Congenital abnormalities of the spleen also occur and may affect organ morphology or position. Variations in shape include lobulations, notches, and clefts. Accessory spleens represent additional splenic tissue separate from the main organ. A wandering or displaced spleen may result from laxity of the supporting ligaments. Polysplenia, also known as "Chaudhry disease," is characterized by multiple splenic nodules or lobules.
Surgical Considerations
Surgery of the spleen is not uncommon and is typically indicated for traumatic events that cause bleeding. Splenic rupture or laceration may result in life-threatening internal hemorrhage, warranting splenectomy. Partial splenectomy may be considered, depending on vascular segmentation, as the arterial subbranches of the spleen do not anastomose. Splenectomy may be performed via laparoscopy or laparotomy. Laparoscopy is preferred whenever feasible, as it generally results in less scarring and a faster recovery than laparotomy. Other conditions that may require splenectomy include, but are not limited to, hypersplenism (overactive spleen), hematologic disorders such as idiopathic thrombocytopenic purpura, thalassemia, hemolytic anemia, sickle cell disease, and malignancies, including lymphoma, Hodgkin disease, and leukemia.[6][7][8]
Clinical Significance
Knowledge of the spleen and its disorders is critical to clinical practice. Although the organ is not vital, splenic dysfunction can be life-threatening. Understanding splenic functions and the ability of red bone marrow, the liver, and lymph nodes to compensate for these functions permits classification of the spleen as a nonvital organ, thereby guiding treatment strategies. Management may include repair, partial splenectomy, or complete splenectomy, as previously described.
The spleen is among the abdominal organs with the highest incidence of injury, with rupture comprising a major concern. Splenectomy may be indicated to prevent excessive hemorrhage into the peritoneal cavity. Rupture is defined by the disruption of the splenic capsule and underlying parenchyma. Blunt force or penetrating trauma can precipitate such injury. Splenic rupture should be carefully considered in cases of left rib fractures, as displacement of a rib fragment can puncture the spleen.
The spleen may become enlarged (splenomegaly) due to multiple factors, including viral or bacterial infections, venous obstruction with associated increased venous pressure, malignancy, and circulatory disturbances related to abnormal cellular activity. Splenic enlargement increases the risk of rupture, which may necessitate surgical removal. Enlarged spleens can be palpable on physical examination and evaluated further using radiographic imaging.
Splenectomy carries significant clinical implications in the context of splenic injury. Absence of the spleen reduces immunological capacity, impairing the ability to respond to infectious agents. Individuals without a spleen are particularly susceptible to infections caused by Streptococcus pneumoniae, Neisseria meningitidis, and Haemophilus influenzae. Vaccination is recommended to mitigate this risk. In conditions such as sickle cell disease, immunizations may be necessary to support immune function that is otherwise compromised by abnormal cellular interactions within the spleen, ensuring optimal defense against pathogens.
Media
(Click Image to Enlarge)
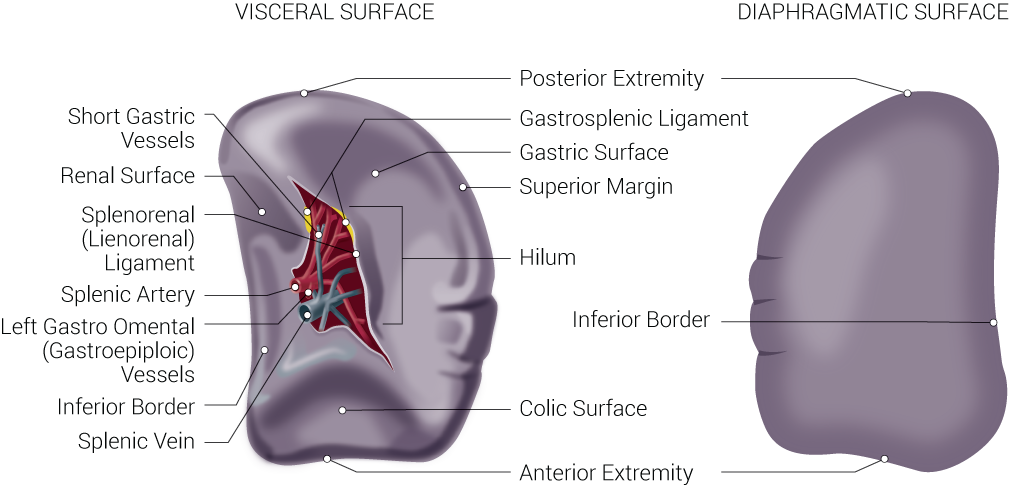
Spleen Anatomy. Spleen anatomy includes visceral surface, diaphragmatic surface, short gastric vessels, renal surface, splenorenal (lienorenal) ligament, splenic artery, left gastro omental (gastroepiploic) vessels, inferior border, splenic vein, posterior extremity, gastrosplenic ligament, gastric surface, superior margin, hilum, colic surface, and anterior extremity.
Illustrated by B Palmer
References
Steiniger BS, Wilhelmi V, Berthold M, Guthe M, Lobachev O. Locating human splenic capillary sheaths in virtual reality. Scientific reports. 2018 Oct 24:8(1):15720. doi: 10.1038/s41598-018-34105-3. Epub 2018 Oct 24 [PubMed PMID: 30356180]
Lung K, Lui F. Anatomy, Abdomen and Pelvis: Arteries. StatPearls. 2025 Jan:(): [PubMed PMID: 30247834]
Pabst R. Clinical relevance of the compartments and lymphocyte subsets in the human spleen. Cell and tissue research. 2025 Oct:402(1):109-119. doi: 10.1007/s00441-025-04001-0. Epub 2025 Aug 29 [PubMed PMID: 40877610]
Bajwa SA, Kasi A. Anatomy, Abdomen and Pelvis: Accessory Spleen. StatPearls. 2025 Jan:(): [PubMed PMID: 30085582]
Moraes DMV, Gutierres A, Colleoni Neto R, Lindemann IL, Rottenfusser R, Carlotto JRM. Anatomy of the splenic artery: what does the surgeon need to know? Revista do Colegio Brasileiro de Cirurgioes. 2022:49():e20223294. doi: 10.1590/0100-6991e-20223294-en. Epub 2022 Sep 30 [PubMed PMID: 36197345]
Wang CF, Launico MV. Splenic Rupture. StatPearls. 2025 Jan:(): [PubMed PMID: 30247826]
Roy P, Mukherjee R, Parik M. Splenic trauma in the twenty-first century: changing trends in management. Annals of the Royal College of Surgeons of England. 2018 Aug 16:100(8):1-7. doi: 10.1308/rcsann.2018.0139. Epub 2018 Aug 16 [PubMed PMID: 30112955]
Bohn JP, Steurer M. Current and evolving treatment strategies in adult immune thrombocytopenia. Memo. 2018:11(3):241-246. doi: 10.1007/s12254-018-0428-7. Epub 2018 Aug 15 [PubMed PMID: 30220932]