Introduction
Chronic rhinosinusitis (CRS) is characterized by persistent sinonasal symptoms with mucosal inflammation lasting 12 weeks or more. Diagnosing CRS can be more difficult than diagnosing acute sinusitis because common symptoms like fever and facial pain may be absent or mild. CRS can develop after an episode of acute sinusitis or a viral upper respiratory tract infection, but not all acute cases progress to CRS. CRS may develop gradually over months or years. Diagnostic uncertainty is common because symptom severity may not correlate with patient history, endoscopic findings, and radiographic imaging. The etiology of CRS may involve systemic factors:
- Genetic conditions
- Immunodeficiency
- Autoimmune diseases
- Idiopathic conditions
Local factors also influence the etiology:
- Sinonasal anatomical abnormalities
- Obstruction
- Neoplasms
Routine laboratory tests are often low-yield unless other comorbidities are present. Key diagnostic methods include contrast-enhanced computed tomography scans with thin-cut coronal slices, nasal endoscopy (possibly with culture or biopsy), and MRI (typically reserved for complex cases involving intracranial, ocular, or fungal complications). Treatment begins by managing predisposing factors such as viral upper respiratory tract infections, environmental or allergic triggers, asthma, immunodeficiency, gastroesophageal reflux disease, or, rarely, cystic fibrosis. Pharmacologic treatment may include symptomatic therapy, corticosteroids, antimicrobials, or other targeted agents. In those with severe or refractory disease, the recently approved humanized monoclonal antibody dupilumab may be considered.[1]
Surgical treatment options include open approach sinus surgery, functional endoscopic sinus surgery, and balloon sinuplasty for certain cases. Potential complications include superimposed infections, orbital involvement such as preseptal cellulitis or an orbital abscess, osteomyelitis, mucoceles, and, rarely, intracranial complications.[2] Most patients require long-term care and treatment of comorbidities, such as allergies or asthma, to prevent recurrent disease.[3][4][5][6]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
CRS is a complex disease with multiple risk factors. Common predisposing factors for CRS include anatomic abnormalities, allergic and nonallergic rhinitis, asthma, nasal polyps, impaired mucociliary clearance, immunologic disorders, recurrent viral upper respiratory tract infections, dental disease, systemic inflammatory diseases, or tumor obstruction. Etiologies can be categorized as follows:
Systemic
- Genetic diseases: cystic fibrosis
- Immunodeficiency: eg, human immunodeficiency virus
- Autoimmune diseases
- Gastroesophageal reflux
- Aspirin-exacerbated respiratory disease: Samter triad
- Granulomatosis with polyangiitis (formerly Wegener granulomatosis)
- Eosinophilic granulomatosis with polyangiitis (formerly Churg-Strauss vasculitis)
- Sarcoidosis [7][8]
Local Host Factors
- Sinonasal anatomic variations
- Trauma
- Foreign bodies
- Neoplasm
- Benign: nasal polyps
- Malignant
- Iatrogenic causes: postoperative complications or scarring
Environmental and Microbial
Epidemiology
Chronic rhinosinusitis affects all age groups, and 12% of the adult United States (US) population has experienced CRS in the past 12 months.[13] CRS has a high impact on the quality of life. Antibiotics are often used for rhinosinusitis, but widespread use is associated with high costs, adverse effects, and antimicrobial resistance.[14] According to the CDC National Center for Health Statistics, the epidemiology for adults 18 and older in the US, 2018, has the following characteristics:
- Sex: Radiologic sinus inflammation, symptoms of CRS, and sinus opacification are more common in women.[15] The highest incidence of CRS is found among White women (15.4%).
- Race/ethnicity: The prevalence of sinusitis was 10.5% for Native American or Alaskan Natives, 6.6% for Asian, 10.8% for Black, 8% for Hispanic or Latino, 11.7% for White, and 12.5% for patients of mixed race or ethnicity.
- Education: Patients without a high school diploma had a lower prevalence (8.6%). Conversely, those with higher education levels had prevalence rates ranging from 11.0% to 13.4% (higher education may be associated with better access to healthcare and diagnosis).
- Employment: Patients who had never been employed had a sinusitis prevalence of 8.7%, whereas those who were currently unemployed but had been employed previously had a prevalence of 13.4%. The prevalence among employed individuals was 10.2%. These higher figures among the currently unemployed may reflect the impact of chronic sinusitis on quality of life and productivity.
- Region: Geographic differences within the US are consistent across studies, with the Southern US showing the highest rates of sinusitis diagnosis (13.4%). In comparison, rates were 9.9% in the Northeast, 9.4% in the West, and 10.5% in the Midwest in 2018.[16][17][18][19]
Pathophysiology
Chronic rhinosinusitis is likely a chronic inflammatory disease influenced by several factors. Many people associate CRS with sinus infections, as it often occurs after an episode of acute sinusitis that is either untreated or does not respond to medical treatment. However, CRS is frequently triggered by a disruption of the intrinsic mucociliary transport system within the paranasal sinuses, leading to the stagnation of secretions. The causes of obstruction are either mechanical obstruction at the osteomeatal complex or mucosal edema, often due to rhinitis. The stagnation of mucus provides a rich environment for the growth of pathogens, typically aerobic bacteria, but may include mixed flora and fungi.[20] CRS in children may represent a distinct spectrum of pathophysiology from that in adults.[21] Additional factors that may contribute to the inflammatory process in CRS include:
- Allergy [22]
- Immune deficiency [23]
- Biofilms [9]
- Osteitis [24]
- Anatomical and physiologic variations
- Superantigens that trigger excessive stimulation of T lymphocytes [25]
- Fungi [26]
- Aspirin sensitivity (Samter triad) [27][28]
Lastly, whether CRS is associated with polyps or not, it is characterized by inflammation, vasodilation, growth, and changes in glandular activity. Activation of nerve endings triggers neurogenic inflammation and morphologically identifiable mucosal remodeling.[29]
Histopathology
The allergic polyp is the most common type of nasal polyp, accounting for 86% of cases. The cause of nasal polyps is unknown, but they are characterized histologically by significant goblet cell hyperplasia, thickening of the basal membrane with hyalinization, the presence of eosinophils and mast cells in the stroma, and edema.[30] The surface epithelium of allergic-type nasal polyps can be intact, completely denuded, or partially denuded respiratory mucosa. The epithelium may also show various changes, including basal-layer hyperplasia, squamous metaplasia, goblet-cell hyperplasia, and infiltration by inflammatory cells, especially eosinophils.[31]
History and Physical
Clinicians should obtain a thorough patient history because CRS signs and symptoms overlap substantially with those of other conditions, most commonly viral upper respiratory tract illness, chronic rhinitis, allergic rhinitis, acute sinusitis, or recurrent acute sinusitis. The poor correlation among symptoms, endoscopic findings, and radiographic images further complicates the diagnosis of CRS. CRS may develop over months to years, and is often misdiagnosed because patients typically present without pain or fever.
CRS is characterized by at least 12 weeks of symptoms, including 2 or more of the following:
- Thick or discolored drainage (either anterior, posterior, or both)
- Nasal congestion
- Facial pain, pressure, fullness
- Decreased sense of smell
More subtle symptoms may include postnasal drip, headache, chronic unproductive cough (especially in children), sore throat, halitosis, malaise, anorexia, visual changes, sneezing, decreased hearing, ear fullness, dizziness, unexplained taste changes, or fevers. The patient's past medical, surgical, trauma, and family histories may also provide important diagnostic clues. Additionally, a history of allergic, immunologic, or metabolic diseases should be assessed (see Image. Lund-Mackay Scoring System for Staging Sinusitis).
The next step in the evaluation is a physical examination to document inflammation and obstruction as part of a complete head and neck examination. Key points to consider include:
- Sinus palpation for tenderness or swelling (subjective)
- Transillumination of the maxillary or frontal sinuses (may be of limited value)
- Anterior rhinoscopy
- Limited view of the anterior portion of the nose, depending on the level of obstruction
- May be improved with a topical decongestant
- Nasal endoscopy with or without video
- Provides anterior, middle, and posterior views of the nasal mucosa, nasal septum, and turbinates
- Access to the osteomeatal complex
- Enables a culture of purulent secretions
- Assessment for obstructions or nasal polyps
- Ocular examination
- Extraocular movements or cranial nerve palsies
- Gross visual disturbances
- Conjunctival examination
- Lacrimation
- Enopthalmus or exopthalmus
- Otologic examination
- Assess for serous otitis media, which may indicate nasopharyngeal mass or obstruction
- Oral and oropharyngeal examination
- Postnasal drainage
- Palate integrity or masses in the nasopharynx
- Dental disease
- Laryngeal examination (fiberoptic laryngoscopy)
- Assess for laryngeal-pharyngeal reflux
- Pulmonary examination
- Assess for upper and lower airway disease
- Neurologic examination
- Assess cranial nerves
Evaluation
The evaluation of CRS depends on the suspected underlying pathology and may include laboratory studies, radiographic imaging, cultures, or biopsy.
Laboratory Studies
Routine laboratory testing has limited value unless the history suggests there is an underlying disease process or comorbidity. Allergy and immune function testing results may vary with individual patient characteristics; however, they should be used to support the diagnosis of CRS rather than to establish it.[32] Common tests include:
- Allergy testing: Radioallergosorbent assay test or skin testing [33]
- Immunological testing: Serum immunoglobulin (Ig) and IgG subclasses [34]
- Total immunoglobulin E levels in allergic fungal sinusitis [35][36]
- HIV testing [37]
Radiographic Imaging
- Plain radiography: Limited value [38]
- May show mucosal thickening or sinus opacification
- Neither sensitive nor specific for CRS
- Air-fluid levels are rarely seen in CRS
- CT scan: Multiplanar contrast-enhanced
- Criterion standard [39]
- Evaluates opacification of sinuses or thickened mucosal membranes (See Image. Acute Sinusitis).
- Detects inflammatory disease, nasal polyps, and mucoceles
- Assesses sinus ostial obstruction, such as the osteomeatal complex
- Detects tumors or bony defects, including sclerosis, septations, erosions, and bowing
- Assesses the orbits, cribiform plates, and optic canal
- Evaluates dental and palatal pathologies
- Used for planning and is valuable for image-guided procedures
- MRI scan
- Best for soft-tissue contrast
- Complementary to a CT scan [40]
- Useful to assess tumors, orbital and intracranial complications, and fungal sinusitis
Cultures
- Nasal swab cultures: Little to no diagnostic value
- Blood cultures: Severe cases of recurrent acute exacerbations of CRS [41]
- Endoscopically directed middle meatus cultures: Sensitivity of 80.9% and a specificity of 90.5% [42]
- Maxillary sinus tap culture (inferior meatal puncture): Used less often since it may be less accurate than a middle meatus culture. Helpful when a middle meatus culture is not feasible, such as in an intubated patient
Biopsy
- Evaluates presumed ciliary dysfunction, along with the sweat test for cystic fibrosis [43]
- Excludes inverting papilloma or malignant tumor
- Nasal cytology
- This may provide diagnostic value for the inflammatory response, but it is more useful in noninfectious rhinitis than in CRS.[44]
Newer Methods
Treatment / Management
Accurate diagnosis remains the most challenging aspect of CRS.[47] While supportive care can treat various nasal and sinus problems, CRS treatment must be precise and personalized for each patient. Unfortunately, some patients are underdiagnosed, overdiagnosed, or misdiagnosed with CRS. Not every patient shows the same signs and symptoms, has the same risk factors, responds similarly to treatments, or achieves long-term relief and improved quality of life. Therefore, all patients with CRS need both immediate and ongoing care tailored to their individual needs. Clinicians should provide a clear rationale for any treatment intervention, whether medical or surgical. Treatment should be directed to improving sinus drainage and outflow, enhancing mucociliary clearance, eradicating inflammation and infection, and improving access of topical therapies to the inflamed mucosa.[48](A1)
Supportive Care
- Humidification and hot compresses
- Over-the-counter analgesics, such as nonsteroidal anti-inflammatory drugs or acetaminophen
- Topical intranasal corticosteroids
- Nasal saline irrigation
- Topical or systemic decongestants (sympathomimetics)
- Antihistamines generally have no role unless there is an allergic component
- Guaifenesin (expectorant)
- Mucolytics
Control of Contributing Factors
- Upper respiratory tract illnesses
- Allergy and asthma
- Environmental triggers such as dust, dust mites, pet dander, cigarette smoke, toxins, or pollutants
- Gastroesophageal and laryngopharyngeal reflux
- Immunodeficiency
- Cystic fibrosis
Corticosteroids
- Oral corticosteroid therapy followed by topical corticosteroid therapy may be effective in reducing nasal polyp size and improving olfaction.[49]
- These confer synergistic benefits when combined with antibiotics.[50]
- Topical intranasal corticosteroid delivery systems are effective and well-tolerated.[51][52] (A1)
Antibiotics, Antifungals, and Biofilms
- The role of antibiotics in the treatment of CRS is debatable; their benefit may be transient and attributable to anti-inflammatory effects.[53]
- A biofilm is a community of bacteria or fungi that surrounds itself with a protective extracellular matrix. Biofilms are present in both healthy individuals and CRS patients, so their clinical significance remains uncertain. Biofilms may influence CRS treatment strategies.[9]
- Nasal irrigation with aminoglycosides should be avoided due to the risk of systemic absorption and toxicity; topical antifungals are not beneficial.[48][54]
- Treatment with topical antibiotics provides little if any benefit.[55]
- The initial choice of antibiotics is empiric, and cultures may be helpful in recalcitrant cases:
- An exacerbation of acute sinusitis could be treated with coverage for β-lactamase–producing organisms. Methicillin-resistant Staphylococcus aureus coverage is necessary in some cases due to ongoing antibiotic exposure.
- S aureus colonization is possible in patients with CRS with nasal polyps, and doxycycline therapy has been effective.[56]
- In patients without nasal polyps, a macrolide antibiotic may be effective when used for 3 months.[57]
- Antibiotic resistance is a risk in patients with CRS due to extended antibiotic use.[58] (A1)
Dupilumab and Other Biologic Agents
- The Food and Drug Administration (FDA) approved dupilumab in June 2019 for the treatment of inadequately controlled severe chronic rhinosinusitis with nasal polyps (CRSwNP) in adults.[59] Dupilumab is a humanized monoclonal antibody that inhibits interleukin-4 (IL-4) and IL-13 signaling by specifically binding to the IL-4Rα subunit.[60]
- Dupilumab and other biologic agents are effective in treating refractory CRSwNP, but are one component of a broader management strategy.[61]
- Endoscopic sinus surgery may be comparable to biologic agents in controlling CRS symptoms.
- Traditional medical and surgical treatments may cost substantially less than biologic agents. (A1)
Surgery
- External open approach (traditional)
- May be combined with several approaches, including functional endoscopic sinus surgery
- Caldwell-Luc
- External ethmoidectomy
- Frontal sinus osteoplastic flap
- Frontal sinus trephine
- Weber-Ferguson incision for large tumors
- Functional endoscopic sinus surgery
- Involves the immediate removal of polyps, mucosal thickening, allergic mucin, or fungal debris to halt disease progression and enlarge the sinus ostium
- Removes the physical obstruction in the sinuses and facilitates drainage.
- Improves sinonasal outflow tract dimensions and facilitates mucociliary clearance and topical medication application.
- Eliminates the source of the pressure atrophy and prevents the progression of bone erosion.
- Removes the osteitic bone that contributes to sinonasal obstruction.
- Early surgical intervention is necessary because medical interventions cannot correct sinus obstruction or allow the egress of stimulating antigens [62][63]
- Technical options
- Procedural components
- Endoscopic uncinectomy
- Ethmoidectomy (anterior or posterior)
- Maxillary antrostomy
- Sphenoidotomy
- Frontal sinus opening
- Involves the immediate removal of polyps, mucosal thickening, allergic mucin, or fungal debris to halt disease progression and enlarge the sinus ostium
- Balloon sinuplasty [66][67]
- Minimally invasive treatment
- Approved by the FDA in 2005
- Patients with frontal or sphenoid disease are more likely to undergo balloon sinuplasty or a hybrid procedure
Differential Diagnosis
The differential diagnosis of CRS includes:
- Recurrent acute sinusitis
- Acute bacterial sinusitis
- Viral upper respiratory tract illness
- Allergic and nonallergic rhinitis
- Facial neuralgia
- Migraine or other primary headache disorders
- Dental infection
- Periodontal abscess
- Nasal and sinus tumors
- Inverting papilloma
- Aspirin and nonsteroidal anti-inflammatory drug sensitivity
- Foreign body
- Fungal sinusitis
- Juvenile nasopharyngeal angiofibroma
- Cystic fibrosis
Prognosis
Despite the complexity of host factors and their significant impact on health-related quality of life, the prognosis for CRS is favorable for most patients. Treatment of CRS improves health-state utility values and significantly reduces symptom burden.[68] Long-term results of sinus surgery for CRS show significant improvement in quality of life at 6 months postoperatively, with benefits persisting for nearly 11 years.[69] Long-term medical therapy appears to improve outcomes and reduce the need for additional surgery. Results from many long-term studies show improvements in sinusitis symptoms, sleep quality, fatigue, and fibromyalgia symptoms.[70][71]
Complications
Prompt investigation of complex sinusitis is essential to prevent debilitating and fatal sequelae.[72] Complications might include:
Noninfectious:
- Fatigue and reduced concentration
- Absenteeism and reduced productivity
- Nasal obstruction
- Sleep disturbance
- Asthma exacerbations
- Anosmia and dysgeusia
Infectious:
- Chronic infection with multiple pathogens resistant to medical therapy
- Osteomyelitis
- Fungal sinusitis
- Mucocele
- Localized spread
- Laryngitis
- Pharyngitis
- Bronchitis
- Pneumonia
Ocular:
- Periorbital cellulitis
- Orbital cellulitis
- Orbital abscess
- Dacryocystitis
- Surgical complications
- Loss of vision
- Ophthalmopegia
Intracranial:
- Cerebrospinal fluid leak
- Meningitis
- Mastoiditis
- Subdural empyema
- Brain abscess
- Cavernous sinus thrombosis
Postoperative and Rehabilitation Care
Postoperative care instructions should be based on the patient’s comorbidities, the extent of the surgery, and factors such as bleeding risk, infection, and pathology. Active patient participation during the postoperative phase is emphasized because it can significantly improve healing and outcomes. During the first week after surgery, patients should follow these instructions:
- Use nasal saline mist or irrigation
- Avoid strenuous activities
- Avoid airplane travel, altitude changes, scuba diving, or swimming
Most patients find that nonsteroidal anti-inflammatory medications or acetaminophen are sufficient for pain management, though some may require a short course of opioid analgesics. Antibiotics or corticosteroids are not routinely prescribed, but may be used depending on the specific circumstances. Patients should discontinue aspirin or other anticoagulants, as well as topical nasal corticosteroids or antihistamine sprays, until approved by the surgeon. Patients should also avoid using continuous positive airway pressure or bilevel positive airway pressure devices until their use is deemed appropriate.
Patients are advised to contact their clinician if they experience any of the following symptoms:
- Excessive bleeding
- Fever greater than 38.6 °C (101.5 °F) that lasts more than 24 hours
- Clear, watery nasal discharge
- Orbital swelling or bruising
- Changes in vision
- Severe headache
- Neck stiffness
- Severe nausea, vomiting, or diarrhea
Most patients should anticipate several days to 1 week off from work, school, or other activities, particularly if they involve strenuous tasks. The timing of postoperative visits may vary depending on whether absorbable or removable packing was used during surgery. Most surgeons recommend endoscopic debridement in the clinic at 1, 3, and 6 weeks postoperatively, although some patients may need additional care. Endoscopic debridement is a crucial part of postoperative care because it helps restore sinus drainage and identify infection or other complications.
Long-term follow-up can be tailored to patient needs, depending on the extent of nasal polyposis, recurrent signs and symptoms, and ongoing infections. Most patients will benefit from consistent use of nasal saline and nasal corticosteroids, and, if necessary, allergy management. Lifestyle adjustments include humidification, hydration, and avoiding known triggers or allergens. Some patients may also benefit from antibiotics, corticosteroids, or biologic therapy (such as dupilumab) if they have persistent anosmia, nasal obstruction, or recurrent infections. Others will require further endoscopic evaluation and repeat CT scans if their sinus disease returns or they require revision surgery.
Consultations
Possible consultations include pulmonary, gastroenterology, neurology, neurosurgery, ophthalmology, allergy/immunology, infectious disease, neuroradiology, pediatrics, oncology, and audiology specialists.
Deterrence and Patient Education
Long-term management of CRS is a shared responsibility among patients, families, and clinicians. While not all upper respiratory illnesses present as acute exacerbations of CRS, many patients experience chronic inflammation, nasal and sinus outflow blockage, and ongoing symptoms. Treatment often involves a combination of medical therapy, revision surgery, allergy treatment if needed, and biologics such as dupilumab or omalizumab if necessary. Patients with CRS, especially those who have previously undergone functional endoscopic sinus surgery, are advised to seek care if symptoms recur or persist, as they may benefit from a comprehensive endoscopic evaluation and possible repeat imaging. Other patients require reevaluation while being treated for underlying comorbidities.
Pearls and Other Issues
CRS is associated with several complications and underlying etiologies that require ongoing evaluation and long-term care:
- Although CRS affects more than 10% of US adults, accurate diagnosis can be challenging.
- Despite advancements in surgical techniques and new medical therapies, treating CRS should include a patient-centered approach, as individual treatment needs vary.
- Patients, families, and clinicians should understand that managing CRS might require lifelong attention and support.
Enhancing Healthcare Team Outcomes
Providing patient-centered care for individuals with CRS requires a collaborative effort among healthcare professionals, including clinicians, nurses, pharmacists, and other specialists. Healthcare professionals must have a strong understanding of nasal and sinus anatomy and physiology, along with the clinical skills needed to make accurate diagnoses. This knowledge includes proficiency in sinonasal endoscopy, interpretation of radiological and pathological findings, investigation of underlying systemic illnesses, and management of complex sinonasal issues. A strategic approach balances clinical expertise and evidence-based guidelines with patient expectations to create personalized care plans.
Ethical communication among team members is paramount. An otolaryngologist must be available for patients experiencing a relapse and maintain vigilance in partnership with patients and other healthcare professionals, especially if the patient needs immediate follow-up care. Open and transparent communication facilitates rapid diagnosis, prevents complications, and hastens patient care. Patient preferences are central to shared decision-making, as there may be multiple approaches to both short- and long-term sinonasal disease.
Education and training keep the healthcare team up to date on best practices. Ongoing professional development ensures that healthcare professionals are equipped to respond to individual patient needs. Clinicians should be discouraged from antibiotic overuse, repeated surgery, and systemic corticosteroid use in patients who may have alternative options such as biologic therapy. A patient-centered approach prioritizes the patient's well-being and preferences in all decisions. In managing CRS, an interprofessional team ensures a comprehensive response, minimizes complications, and prioritizes patient safety and quality care.
Media
(Click Image to Enlarge)
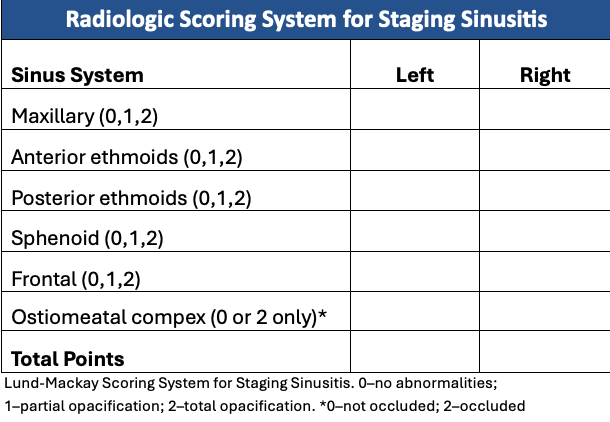
Lund-Mackay Scoring System for Staging Sinusitis. This scoring system for staging sinusitis is based on a noncontrast CT scan of the sinuses.
Contributed by CB Shermetaro, DO
(Click Image to Enlarge)

Acute Sinusitis. An axial CT scan of the paranasal sinuses shows opacification of the left maxillary sinus, consistent with a diagnosis of acute sinusitis.
Contributed by S Bhimji, MD
References
Kim DH, Stybayeva G, Hwang SH. Comparative Effectiveness of Dupilumab Versus Sinus Surgery for Chronic Rhinosinusitis With Polyps: Systematic Review and a Meta-Analysis. American journal of rhinology & allergy. 2024 Nov:38(6):428-436. doi: 10.1177/19458924241272978. Epub 2024 Aug 16 [PubMed PMID: 39149992]
Level 1 (high-level) evidenceMaran AG. Endoscopic sinus surgery. European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS) : affiliated with the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery. 1994:251(6):309-18 [PubMed PMID: 7848639]
Klimek L, Koennecke M, Hagemann J, Wollenberg B, Becker S. [Immunology of chronic rhinosinusitis with nasal polyps as a basis for treatment with biologicals]. HNO. 2019 Jan:67(1):15-26. doi: 10.1007/s00106-018-0557-7. Epub [PubMed PMID: 30167718]
Pipolo C, Saibene AM, Felisati G. Prevalence of pain due to rhinosinusitis: a review. Neurological sciences : official journal of the Italian Neurological Society and of the Italian Society of Clinical Neurophysiology. 2018 Jun:39(Suppl 1):21-24. doi: 10.1007/s10072-018-3336-z. Epub [PubMed PMID: 29904833]
Brook I. Acute and chronic bacterial sinusitis. Infectious disease clinics of North America. 2007 Jun:21(2):427-48, vii [PubMed PMID: 17561077]
Brook I. Microbiology and antimicrobial management of sinusitis. Otolaryngologic clinics of North America. 2004 Apr:37(2):253-66, v-vi [PubMed PMID: 15064061]
Stryjewska-Makuch G, Janik MA, Lisowska G, Kolebacz B. Bacteriological analysis of isolated chronic sinusitis without polyps. Postepy dermatologii i alergologii. 2018 Aug:35(4):375-380. doi: 10.5114/ada.2018.77667. Epub 2018 Aug 21 [PubMed PMID: 30206450]
Cho HJ, Kim CH. Oxygen matters: hypoxia as a pathogenic mechanism in rhinosinusitis. BMB reports. 2018 Feb:51(2):59-64 [PubMed PMID: 29366441]
Fastenberg JH, Hsueh WD, Mustafa A, Akbar NA, Abuzeid WM. Biofilms in chronic rhinosinusitis: Pathophysiology and therapeutic strategies. World journal of otorhinolaryngology - head and neck surgery. 2016 Dec:2(4):219-229. doi: 10.1016/j.wjorl.2016.03.002. Epub 2016 May 5 [PubMed PMID: 29204570]
Brook I. Microbiology of sinusitis. Proceedings of the American Thoracic Society. 2011 Mar:8(1):90-100. doi: 10.1513/pats.201006-038RN. Epub [PubMed PMID: 21364226]
Brook I. Microbiology of chronic rhinosinusitis. European journal of clinical microbiology & infectious diseases : official publication of the European Society of Clinical Microbiology. 2016 Jul:35(7):1059-68. doi: 10.1007/s10096-016-2640-x. Epub 2016 Apr 16 [PubMed PMID: 27086363]
Ferguson BJ. Definitions of fungal rhinosinusitis. Otolaryngologic clinics of North America. 2000 Apr:33(2):227-35 [PubMed PMID: 10736401]
Payne SC, McKenna M, Buckley J, Colandrea M, Chow A, Detwiller K, Donaldson A, Dubin M, Finestone S, Filip P, Khalid A, Peters AT, Rosenfeld R, Akrami Z, Dhepyasuwan N. Clinical Practice Guideline: Adult Sinusitis Update. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2025 Aug:173 Suppl 1():S1-S56. doi: 10.1002/ohn.1344. Epub [PubMed PMID: 40742114]
Level 1 (high-level) evidenceSmith SS, Evans CT, Tan BK, Chandra RK, Smith SB, Kern RC. National burden of antibiotic use for adult rhinosinusitis. The Journal of allergy and clinical immunology. 2013 Nov:132(5):1230-2. doi: 10.1016/j.jaci.2013.07.009. Epub 2013 Aug 26 [PubMed PMID: 23987794]
Hirsch AG, Nordberg C, Bandeen-Roche K, Tan BK, Schleimer RP, Kern RC, Sundaresan A, Pinto JM, Kennedy TL, Greene JS, Kuiper JR, Schwartz BS. Radiologic sinus inflammation and symptoms of chronic rhinosinusitis in a population-based sample. Allergy. 2020 Apr:75(4):911-920. doi: 10.1111/all.14106. Epub 2019 Dec 2 [PubMed PMID: 31713250]
Zhou AS, Prince AA, Maxfield AZ, Corrales CE, Shin JJ. The Impact of Sinonasal Symptoms in Relation to Potentially Life-Threatening Comorbidities. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2023 Dec:169(6):1462-1471. doi: 10.1002/ohn.395. Epub 2023 Jun 14 [PubMed PMID: 37313804]
Park JJH, Seidel DU, Bachert C, Dazert S, Kostev K. Medication use in patients with chronic rhinosinusitis in Germany - a large retrospective patient-based study. Rhinology. 2019 Apr 1:57(2):94-100. doi: 10.4193/Rhin18.055. Epub [PubMed PMID: 30076702]
Level 2 (mid-level) evidencePhilpott CM, Erskine S, Hopkins C, Kumar N, Anari S, Kara N, Sunkaraneni S, Ray J, Clark A, Wilson A, CRES group, Erskine S, Philpott C, Clark A, Hopkins C, Robertson A, Ahmed S, Kara N, Carrie S, Sunkaraneni V, Ray J, Anari S, Jervis P, Panesaar J, Farboud A, Kumar N, Cathcart R, Almeyda R, Khalil H, Prinsley P, Mansell N, Salam M, Hobson J, Woods J, Coombes E. Prevalence of asthma, aspirin sensitivity and allergy in chronic rhinosinusitis: data from the UK National Chronic Rhinosinusitis Epidemiology Study. Respiratory research. 2018 Jun 27:19(1):129. doi: 10.1186/s12931-018-0823-y. Epub 2018 Jun 27 [PubMed PMID: 29945606]
Barac A, Ong DSY, Jovancevic L, Peric A, Surda P, Tomic Spiric V, Rubino S. Fungi-Induced Upper and Lower Respiratory Tract Allergic Diseases: One Entity. Frontiers in microbiology. 2018:9():583. doi: 10.3389/fmicb.2018.00583. Epub 2018 Apr 3 [PubMed PMID: 29666610]
Biel MA, Brown CA, Levinson RM, Garvis GE, Paisner HM, Sigel ME, Tedford TM. Evaluation of the microbiology of chronic maxillary sinusitis. The Annals of otology, rhinology, and laryngology. 1998 Nov:107(11 Pt 1):942-5 [PubMed PMID: 9823843]
Heath J, Hartzell L, Putt C, Kennedy JL. Chronic Rhinosinusitis in Children: Pathophysiology, Evaluation, and Medical Management. Current allergy and asthma reports. 2018 May 29:18(7):37. doi: 10.1007/s11882-018-0792-8. Epub 2018 May 29 [PubMed PMID: 29845321]
Helman SN, Barrow E, Edwards T, DelGaudio JM, Levy JM, Wise SK. The Role of Allergic Rhinitis in Chronic Rhinosinusitis. Immunology and allergy clinics of North America. 2020 May:40(2):201-214. doi: 10.1016/j.iac.2019.12.010. Epub 2020 Jan 14 [PubMed PMID: 32278445]
Chiarella SE, Grammer LC. Immune deficiency in chronic rhinosinusitis: screening and treatment. Expert review of clinical immunology. 2017 Feb:13(2):117-123. doi: 10.1080/1744666X.2016.1216790. Epub 2016 Aug 18 [PubMed PMID: 27500811]
Bhandarkar ND, Sautter NB, Kennedy DW, Smith TL. Osteitis in chronic rhinosinusitis: a review of the literature. International forum of allergy & rhinology. 2013 May:3(5):355-63. doi: 10.1002/alr.21118. Epub 2012 Dec 19 [PubMed PMID: 23258589]
Fraser JD, Proft T. The bacterial superantigen and superantigen-like proteins. Immunological reviews. 2008 Oct:225():226-43. doi: 10.1111/j.1600-065X.2008.00681.x. Epub [PubMed PMID: 18837785]
Tyler MA, Lam K, Marino MJ, Yao WC, Schmale I, Citardi MJ, Luong AU. Revisiting the controversy: The role of fungi in chronic rhinosinusitis. International forum of allergy & rhinology. 2021 Nov:11(11):1577-1587. doi: 10.1002/alr.22826. Epub 2021 Jun 2 [PubMed PMID: 34076362]
Level 3 (low-level) evidenceKim SD, Cho KS. Samter's Triad: State of the Art. Clinical and experimental otorhinolaryngology. 2018 Jun:11(2):71-80. doi: 10.21053/ceo.2017.01606. Epub 2018 Apr 13 [PubMed PMID: 29642688]
Dominas C, Gadkaree S, Maxfield AZ, Gray ST, Bergmark RW. Aspirin-exacerbated respiratory disease: A review. Laryngoscope investigative otolaryngology. 2020 Jun:5(3):360-367. doi: 10.1002/lio2.387. Epub 2020 May 1 [PubMed PMID: 32596477]
Klimek L, Böttcher I. [What are the changes in the nasal mucosa caused by allergic rhinitis?]. Deutsche medizinische Wochenschrift (1946). 2008 Jul:133 Suppl 3():S88-94. doi: 10.1055/s-2008-1067327. Epub [PubMed PMID: 18642237]
Couto LG, Fernades AM, Brandão DF, Santi Neto Dd, Valera FC, Anselmo-Lima WT. Histological aspects of rhinosinusal polyps. Brazilian journal of otorhinolaryngology. 2008 Mar-Apr:74(2):207-12 [PubMed PMID: 18568198]
Pawliczak R, Lewandowska-Polak A, Kowalski ML. Pathogenesis of nasal polyps: an update. Current allergy and asthma reports. 2005 Nov:5(6):463-71 [PubMed PMID: 16216171]
Shin JJ, Wilson M, McKenna M, Rosenfeld R, Ammon K, Crosby D, Fuchs JM, Hensler JB, Illing EA, Lam K, Levine C, Kmucha ST, McCoul ED, Miller J, Rodriguez K, Rowan NR, Sedaghat AR, Tan BK, Roy E, Dhepyasuwan N. Clinical Practice Guideline: Surgical Management of Chronic Rhinosinusitis. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2025 Jun:172 Suppl 2():S1-S47. doi: 10.1002/ohn.1287. Epub [PubMed PMID: 40424072]
Level 1 (high-level) evidenceChinoy B, Yee E, Bahna SL. Skin testing versus radioallergosorbent testing for indoor allergens. Clinical and molecular allergy : CMA. 2005 Apr 15:3(1):4 [PubMed PMID: 15833110]
Mazza JM, Lin SY. Primary immunodeficiency and recalcitrant chronic sinusitis: a systematic review. International forum of allergy & rhinology. 2016 Oct:6(10):1029-1033. doi: 10.1002/alr.21789. Epub 2016 May 17 [PubMed PMID: 27187624]
Level 1 (high-level) evidenceWise SK, Ahn CN, Lathers DM, Mulligan RM, Schlosser RJ. Antigen-specific IgE in sinus mucosa of allergic fungal rhinosinusitis patients. American journal of rhinology. 2008 Sep-Oct:22(5):451-6. doi: 10.2500/ajr.2008.22.3227. Epub [PubMed PMID: 18954501]
Ahn CN, Wise SK, Lathers DM, Mulligan RM, Harvey RJ, Schlosser RJ. Local production of antigen-specific IgE in different anatomic subsites of allergic fungal rhinosinusitis patients. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2009 Jul:141(1):97-103. doi: 10.1016/j.otohns.2009.03.002. Epub [PubMed PMID: 19559966]
Godofsky EW, Zinreich J, Armstrong M, Leslie JM, Weikel CS. Sinusitis in HIV-infected patients: a clinical and radiographic review. The American journal of medicine. 1992 Aug:93(2):163-70 [PubMed PMID: 1497012]
Kolo ES. The role of plain radiographs in the diagnosis of chronic maxillary rhinosinusitis in adults. African health sciences. 2012 Dec:12(4):459-63 [PubMed PMID: 23515592]
Expert Panel on Neurologic Imaging:, Kirsch CFE, Bykowski J, Aulino JM, Berger KL, Choudhri AF, Conley DB, Luttrull MD, Nunez D Jr, Shah LM, Sharma A, Shetty VS, Subramaniam RM, Symko SC, Cornelius RS. ACR Appropriateness Criteria(®) Sinonasal Disease. Journal of the American College of Radiology : JACR. 2017 Nov:14(11S):S550-S559. doi: 10.1016/j.jacr.2017.08.041. Epub [PubMed PMID: 29101992]
Poto R, Pelaia C, di Salvatore A, Saleh H, Scadding GW, Varricchi G. Imaging of chronic rhinosinusitis with nasal polyps in the era of biological therapies. Current opinion in allergy and clinical immunology. 2024 Aug 1:24(4):243-250. doi: 10.1097/ACI.0000000000000964. Epub 2024 Feb 12 [PubMed PMID: 38205820]
Level 3 (low-level) evidenceYaniv D, Stern D, Vainer I, Ben Zvi H, Yahav D, Soudry E. The bacteriology of recurrent acute exacerbations of chronic rhinosinusitis: a longitudinal analysis. European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS) : affiliated with the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery. 2020 Nov:277(11):3051-3057. doi: 10.1007/s00405-020-06157-7. Epub 2020 Jul 4 [PubMed PMID: 32623506]
Benninger MS, Payne SC, Ferguson BJ, Hadley JA, Ahmad N. Endoscopically directed middle meatal cultures versus maxillary sinus taps in acute bacterial maxillary rhinosinusitis: a meta-analysis. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2006 Jan:134(1):3-9 [PubMed PMID: 16399172]
Level 1 (high-level) evidenceIovănescu G, Pop LL, Vintilă DR, Marin KC, Mogoantă CA, Lăzureanu DC, Borugă VM, Ciucă IM. Nasal polyposis from cystic fibrosis in children - the experience of a single center. Romanian journal of morphology and embryology = Revue roumaine de morphologie et embryologie. 2023 Apr-Jun:64(2):235-240. doi: 10.47162/RJME.64.2.14. Epub [PubMed PMID: 37518881]
She W, Yang J, Wang C, Zhang L. Diagnostic Value of Nasal Cytology in Chronic Rhinosinusitis Assessed by a Liquid-based Cytological Technique. American journal of rhinology & allergy. 2018 May:32(3):181-187. doi: 10.1177/1945892418768581. Epub 2018 Apr 17 [PubMed PMID: 29660995]
Kalaiarasi R, Vijayakumar C, Archana R, Venkataramanan R, Chidambaram R, Shrinuvasan S, Prabhu R. Role of Thermography in the Diagnosis of Chronic Sinusitis. Cureus. 2018 Mar 10:10(3):e2298. doi: 10.7759/cureus.2298. Epub 2018 Mar 10 [PubMed PMID: 29755895]
Ishimaru T, Ishimaru H. Thermography for the Diagnosis of Acute Inflammation in the Paranasal Sinus. International archives of otorhinolaryngology. 2020 Apr:24(2):e215-e220. doi: 10.1055/s-0039-1698778. Epub 2020 Jan 28 [PubMed PMID: 32256844]
Novis SJ, Akkina SR, Lynn S, Kern HE, Keshavarzi NR, Pynnonen MA. A diagnostic dilemma: chronic sinusitis diagnosed by non-otolaryngologists. International forum of allergy & rhinology. 2016 May:6(5):486-90. doi: 10.1002/alr.21691. Epub 2016 Jan 11 [PubMed PMID: 26750399]
Rosenfeld RM, Piccirillo JF, Chandrasekhar SS, Brook I, Ashok Kumar K, Kramper M, Orlandi RR, Palmer JN, Patel ZM, Peters A, Walsh SA, Corrigan MD. Clinical practice guideline (update): adult sinusitis. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2015 Apr:152(2 Suppl):S1-S39. doi: 10.1177/0194599815572097. Epub [PubMed PMID: 25832968]
Level 1 (high-level) evidenceVaidyanathan S, Barnes M, Williamson P, Hopkinson P, Donnan PT, Lipworth B. Treatment of chronic rhinosinusitis with nasal polyposis with oral steroids followed by topical steroids: a randomized trial. Annals of internal medicine. 2011 Mar 1:154(5):293-302. doi: 10.7326/0003-4819-154-5-201103010-00003. Epub [PubMed PMID: 21357906]
Level 1 (high-level) evidenceVenekamp RP, Thompson MJ, Hayward G, Heneghan CJ, Del Mar CB, Perera R, Glasziou PP, Rovers MM. Systemic corticosteroids for acute sinusitis. The Cochrane database of systematic reviews. 2014 Mar 25:(3):CD008115. doi: 10.1002/14651858.CD008115.pub3. Epub 2014 Mar 25 [PubMed PMID: 24664368]
Level 1 (high-level) evidenceSnidvongs K, Kalish L, Sacks R, Sivasubramaniam R, Cope D, Harvey RJ. Sinus surgery and delivery method influence the effectiveness of topical corticosteroids for chronic rhinosinusitis: systematic review and meta-analysis. American journal of rhinology & allergy. 2013 May-Jun:27(3):221-33. doi: 10.2500/ajra.2013.27.3880. Epub [PubMed PMID: 23710959]
Level 1 (high-level) evidenceDouglas RG, Psaltis AJ, Rimmer J, Kuruvilla T, Cervin A, Kuang Y. Phase 1 clinical study to assess the safety of a novel drug delivery system providing long-term topical steroid therapy for chronic rhinosinusitis. International forum of allergy & rhinology. 2019 Apr:9(4):378-387. doi: 10.1002/alr.22288. Epub 2019 Jan 15 [PubMed PMID: 30645028]
Barshak MB, Durand ML. The role of infection and antibiotics in chronic rhinosinusitis. Laryngoscope investigative otolaryngology. 2017 Feb:2(1):36-42. doi: 10.1002/lio2.61. Epub 2017 Jan 23 [PubMed PMID: 28894821]
Orlandi RR, Kingdom TT, Hwang PH, Smith TL, Alt JA, Baroody FM, Batra PS, Bernal-Sprekelsen M, Bhattacharyya N, Chandra RK, Chiu A, Citardi MJ, Cohen NA, DelGaudio J, Desrosiers M, Dhong HJ, Douglas R, Ferguson B, Fokkens WJ, Georgalas C, Goldberg A, Gosepath J, Hamilos DL, Han JK, Harvey R, Hellings P, Hopkins C, Jankowski R, Javer AR, Kern R, Kountakis S, Kowalski ML, Lane A, Lanza DC, Lebowitz R, Lee HM, Lin SY, Lund V, Luong A, Mann W, Marple BF, McMains KC, Metson R, Naclerio R, Nayak JV, Otori N, Palmer JN, Parikh SR, Passali D, Peters A, Piccirillo J, Poetker DM, Psaltis AJ, Ramadan HH, Ramakrishnan VR, Riechelmann H, Roh HJ, Rudmik L, Sacks R, Schlosser RJ, Senior BA, Sindwani R, Stankiewicz JA, Stewart M, Tan BK, Toskala E, Voegels R, Wang de Y, Weitzel EK, Wise S, Woodworth BA, Wormald PJ, Wright ED, Zhou B, Kennedy DW. International Consensus Statement on Allergy and Rhinology: Rhinosinusitis. International forum of allergy & rhinology. 2016 Feb:6 Suppl 1():S22-209. doi: 10.1002/alr.21695. Epub [PubMed PMID: 26889651]
Level 3 (low-level) evidenceCain RB, Lal D. Update on the management of chronic rhinosinusitis. Infection and drug resistance. 2013:6():1-14. doi: 10.2147/IDR.S26134. Epub 2013 Jan 23 [PubMed PMID: 23378777]
Van Zele T, Gevaert P, Holtappels G, Beule A, Wormald PJ, Mayr S, Hens G, Hellings P, Ebbens FA, Fokkens W, Van Cauwenberge P, Bachert C. Oral steroids and doxycycline: two different approaches to treat nasal polyps. The Journal of allergy and clinical immunology. 2010 May:125(5):1069-1076.e4. doi: 10.1016/j.jaci.2010.02.020. Epub [PubMed PMID: 20451040]
Rudmik L, Soler ZM. Medical Therapies for Adult Chronic Sinusitis: A Systematic Review. JAMA. 2015 Sep 1:314(9):926-39. doi: 10.1001/jama.2015.7544. Epub [PubMed PMID: 26325561]
Level 1 (high-level) evidenceRamakrishnan VR, Mace JC, Soler ZM, Smith TL. Examination of high-antibiotic users in a multi-institutional cohort of chronic rhinosinusitis patients. International forum of allergy & rhinology. 2017 Apr:7(4):343-351. doi: 10.1002/alr.21903. Epub 2017 Jan 13 [PubMed PMID: 28084683]
Lipworth B, Chan R, Kuo CR. Dupilumab for nasal polyposis. Lancet (London, England). 2020 Jul 25:396(10246):233. doi: 10.1016/S0140-6736(20)30562-6. Epub [PubMed PMID: 32711789]
Bachert C, Han JK, Desrosiers M, Hellings PW, Amin N, Lee SE, Mullol J, Greos LS, Bosso JV, Laidlaw TM, Cervin AU, Maspero JF, Hopkins C, Olze H, Canonica GW, Paggiaro P, Cho SH, Fokkens WJ, Fujieda S, Zhang M, Lu X, Fan C, Draikiwicz S, Kamat SA, Khan A, Pirozzi G, Patel N, Graham NMH, Ruddy M, Staudinger H, Weinreich D, Stahl N, Yancopoulos GD, Mannent LP. Efficacy and safety of dupilumab in patients with severe chronic rhinosinusitis with nasal polyps (LIBERTY NP SINUS-24 and LIBERTY NP SINUS-52): results from two multicentre, randomised, double-blind, placebo-controlled, parallel-group phase 3 trials. Lancet (London, England). 2019 Nov 2:394(10209):1638-1650. doi: 10.1016/S0140-6736(19)31881-1. Epub 2019 Sep 19 [PubMed PMID: 31543428]
Level 1 (high-level) evidenceHardison SA, Senior BA. The argument against the use of dupilumab in patients with limited polyp burden in chronic rhinosinusitis with nasal polyposis (CRSwNP). Journal of otolaryngology - head & neck surgery = Le Journal d'oto-rhino-laryngologie et de chirurgie cervico-faciale. 2023 Sep 28:52(1):64. doi: 10.1186/s40463-023-00668-z. Epub 2023 Sep 28 [PubMed PMID: 37759322]
Stammberger H. Endoscopic endonasal surgery--concepts in treatment of recurring rhinosinusitis. Part II. Surgical technique. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 1986 Feb:94(2):147-56 [PubMed PMID: 3083327]
Hafner B, Davris S, Riechelmann H, Mann WJ, Amedee RG. Endonasal sinus surgery improves mucociliary transport in severe chronic sinusitis. American journal of rhinology. 1997 Jul-Aug:11(4):271-4 [PubMed PMID: 9292177]
Olson G, Citardi MJ. Image-guided functional endoscopic sinus surgery. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2000 Sep:123(3):188-94 [PubMed PMID: 10964289]
Tschopp KP, Thomaser EG. Outcome of functional endonasal sinus surgery with and without CT-navigation. Rhinology. 2008 Jun:46(2):116-20 [PubMed PMID: 18575012]
Chaaban MR, Rana N, Baillargeon J, Baillargeon G, Resto V, Kuo YF. Outcomes and Complications of Balloon and Conventional Functional Endoscopic Sinus Surgery. American journal of rhinology & allergy. 2018 Sep:32(5):388-396. doi: 10.1177/1945892418782248. Epub 2018 Jun 27 [PubMed PMID: 29947260]
Chaaban MR, Baillargeon JG, Baillargeon G, Resto V, Kuo YF. Use of balloon sinuplasty in patients with chronic rhinosinusitis in the United States. International forum of allergy & rhinology. 2017 Jun:7(6):600-608. doi: 10.1002/alr.21939. Epub 2017 May 8 [PubMed PMID: 28481017]
Rudmik L, Mace J, Soler ZM, Smith TL. Long-term utility outcomes in patients undergoing endoscopic sinus surgery. The Laryngoscope. 2014 Jan:124(1):19-23. doi: 10.1002/lary.24135. Epub 2013 May 13 [PubMed PMID: 23670699]
Smith TL,Schlosser RJ,Mace JC,Alt JA,Beswick DM,DeConde AS,Detwiller KY,Mattos JL,Soler ZM, Long-term outcomes of endoscopic sinus surgery in the management of adult chronic rhinosinusitis. International forum of allergy [PubMed PMID: 31207172]
Sautter NB, Mace J, Chester AC, Smith TL. The effects of endoscopic sinus surgery on level of fatigue in patients with chronic rhinosinusitis. American journal of rhinology. 2008 Jul-Aug:22(4):420-6. doi: 10.2500/ajr.2008.22.3196. Epub [PubMed PMID: 18702910]
Soler ZM, Mace J, Smith TL. Fibromyalgia and chronic rhinosinusitis: outcomes after endoscopic sinus surgery. American journal of rhinology. 2008 Jul-Aug:22(4):427-32. doi: 10.2500/ajr.2008.22.3198. Epub [PubMed PMID: 18702911]
Hong P, Pereyra CA, Guo U, Breslin A, Melville L. Evaluating Complications of Chronic Sinusitis. Case reports in emergency medicine. 2017:2017():8743828. doi: 10.1155/2017/8743828. Epub 2017 Jan 9 [PubMed PMID: 28163938]
Level 3 (low-level) evidence