Introduction
The Scarpa fascia is a membranous layer of the anterior abdominal wall. The following distinct layers are identified traversing the abdominal wall from superficial to deep: skin, subcutaneous tissue, superficial fascia, external oblique muscle, internal oblique muscle, transversus abdominis muscle, transversalis fascia, preperitoneal adipose tissue, and peritoneum. The superficial fascia consists of 2 components: a membranous layer, the Scarpa fascia, and an outer fatty layer known as the Camper fascia (see Image. Fascial Layers).
The Scarpa fascia lies deep to the Camper fascia and superficial to the external oblique muscle. Lateral attachment occurs at the aponeurosis of the external oblique muscle. Medial continuity is present with the linea alba and pubic symphysis. In the upper thigh, fusion occurs with the fascia lata approximately 1 fingerbreadth inferior to the inguinal ligament. The term “Scarpa fascia” is based on the anatomic region of distribution.
The Scarpa fascia extends over the spermatic cord and into the scrotum, where the layer is termed "dartos fascia." From the scrotum, the fascia may be traced posteriorly as it continues as Colles fascia while blending with the deeper layers of the perineum. In female individuals, extension occurs into the labia majora. The Scarpa fascia is a clinically important structure due to its role in abdominal incision repair and in the formation of fascial planes that limit the extravasation of bodily fluids.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The Scarpa fascia is a dense collagenous connective tissue layer of the anterior abdominal wall. The layer is considerably thinner than the Camper fascia and contains elastic fibers and loose connective tissue. Recent anatomical and histologic studies have demonstrated that the Scarpa fascia is part of a continuous fascial network that contributes to mechanical support and force transmission throughout the abdominal wall.
The Scarpa fascia serves an essential role in separating the overlying Camper fascia (fatty layer) from the underlying muscles. The layer also permits the Camper fascia to glide freely over the underlying abdominal wall structures (external oblique fascia or rectus sheath), thereby reducing friction generated by muscular contraction and facilitating abdominal flexion, extension, and rotation.
Due to the parallel orientation of collagen fibers along the direction of mechanical stress, the Scarpa fascia can withstand unidirectional tensile forces while maintaining flexibility. This structural arrangement enables the fascia to provide a supportive yet pliable conduit for nerves and blood vessels traversing the abdominal wall muscles. As a component of the abdominal wall, the Scarpa fascia also contributes to the protection of intra-abdominal organs.[1]
Embryology
The mesoderm, also known as the middle germ layer, gives rise to nearly all connective tissues in the human body. During embryogenesis, the paraxial mesoderm located on either side of the notochord differentiates into the sclerotome and dermomyotome. The sclerotome forms the vertebral bodies, whereas the dermomyotome further divides into the dermatome and myotome, which give rise to the dermis and skeletal muscle.
In humans, the dermatome becomes identifiable around the 3rd week of embryogenesis. As a component of the superficial connective tissue associated with the skin, the Scarpa fascia develops from the dermatome lineage.[2]
Blood Supply and Lymphatics
The anterior abdominal wall receives blood supply from the intercostal, subcostal, lumbar, and epigastric arteries. The lateral abdominal wall is supplied by the inferior posterior intercostal arteries and lumbar arteries branching from the descending aorta.
The Scarpa fascia receives a substantial portion of its blood supply from the epigastric vessels. The superior epigastric artery, a branch of the internal thoracic artery, travels within the rectus sheath and ultimately anastomoses with the inferior epigastric artery near the umbilicus. The inferior epigastric artery originates from the external iliac artery. Recent anatomical studies have further characterized the vascular supply of the superficial fascia, highlighting its importance in surgical procedures involving the abdominal wall.[3]
Lymphatic drainage of the abdominal wall inferior to the umbilicus occurs primarily through the superficial inguinal lymph nodes. Detailed anatomical investigations have demonstrated lymphatic vessels within the superficial fascial system of the abdomen.[4] The lateral abdominal wall drains to the upper lateral quadrant of the superficial inguinal nodes, whereas the medial abdominal wall drains to the upper medial quadrant.
Nerves
The abdominal wall receives segmental sensory innervation in a dermatomal distribution. The skin surrounding the umbilicus corresponds to the T10 dermatome. The intercostal (T7–T11) and subcostal (T12) nerves become anterior cutaneous nerves as they traverse the rectus sheath toward the skin. The iliohypogastric and ilioinguinal (L1) nerves also contribute sensory innervation. The iliohypogastric nerve carries sensory information from the skin superior to the suprapubic region, wher eas the ilioinguinal nerve provides sensation to portions of the labia majora or scrotum and the medial thigh. These nerves traverse the Scarpa fascia as they course toward the skin.
Muscles
The muscles of the abdominal wall include the external oblique, internal oblique, transversus abdominis, rectus abdominis, and pyramidalis. The external oblique is the outermost muscle of the anterior abdominal wall and arises from the lower ribs before attaching to the iliac crest and linea alba. The Scarpa fascia lies directly superficial to the external oblique and serves as an important structure separating the underlying abdominal wall muscles from the skin and subcutaneous tissue. The internal oblique originates from the thoracolumbar fascia, iliac crest, and the lateral half of the inguinal ligament and courses cranially and anteriorly to attach to the lower ribs, the linea alba, and the pubic crest via the conjoint tendon.
The transversus abdominis lies on the lateral aspect of the abdomen and originates from the lower costal cartilages, thoracolumbar fascia, iliac crest, and inguinal ligament before attaching to the linea alba and pubic crest via the conjoint tendon. The rectus abdominis runs vertically along the anterior abdominal wall from the pubic bone to the xiphoid process and the 5th, 6th, and 7th costal cartilages.
The pyramidalis is a small triangular muscle that lies anterior to the rectus abdominis within the rectus sheath. This muscle originates from the pubic symphysis and pubic crest and inserts onto the linea alba. The pyramidalis is present in approximately 80% of the population.[5]
Physiologic Variants
The Scarpa fascia is most prominent in the lower abdomen, with well-developed fibers along the lateral abdominal wall superficial to the rectus sheath. Compared with the lateral abdominal wall, the fascia is less developed along the midline.
Historically, the Scarpa fascia was believed to be limited to the lower abdomen and perineum. Modern imaging and anatomical studies have demonstrated that the superficial fascial system may extend across the torso, with regional variations in thickness and organization.[6] Variations in the arrangement and thickness of the Scarpa fascia may depend on body region and sex.[7]
Surgical Considerations
The Scarpa fascia plays an important role in the healing of abdominal incisions and in facilitating abdominal contouring procedures. Contemporary studies suggest that preservation of the fascia during abdominoplasty reduces postoperative seroma formation.[8] Seroma, defined as a collection of serous or serosanguinous fluid, is the most common complication associated with abdominoplasty. Preservation of the adipofascial layer helps maintain lymphatic drainage and reduces fluid accumulation.
Careful sparing of the adipose–fascial tissue may decrease the volume and duration of postoperative drainage and shorten hospital stay.[9] Preservation of the Scarpa fascia has also been associated with improved aesthetic outcomes.
Another surgical application under investigation involves the use of Scarpa adipofascial flaps in reconstructive procedures. Such flaps have been utilized in the repair of large scalp defects and in other reconstructive surgeries.
Clinical Significance
Early theories suggested that the Scarpa fascia prevented hernia formation, though this concept is no longer supported.[10] The fascia does not provide sufficient structural strength to prevent hernias. Instead, the superficial fascia functions primarily as a scaffolding layer that anchors the abdominal wall skin to deeper tissues.
Fluid may accumulate within fascial planes in conditions such as acute hemorrhagic pancreatitis. Retroperitoneal hemorrhage may produce characteristic bruising patterns, such as the Grey Turner or Cullen sign. Imaging studies have shown that the distribution of these findings corresponds to boundaries defined by fascial attachments. Similarly, retroperitoneal hemorrhage may produce the Fox sign, which presents as ecchymosis along the inguinal ligament in the inguinal region, corresponding to the inferior attachment of the Scarpa fascia to the fascia lata of the thigh.
Trauma or surgery may lead to scar tissue formation and adhesions within fascial planes. Such changes can alter the biomechanical properties of the fascia and reduce the ability of fascial layers to glide between adjacent structures, potentially contributing to altered tissue mechanics. Extravasation of urine following damage to the penile urethra and the Buck fascia allows urine to escape into the superficial fascial plane and collect under the dartos fascia in the penis, scrotum, and perineum, as well as under the Scarpa fascia in the lower anterior abdominal wall, but not into the thigh.[11]
Media
(Click Image to Enlarge)
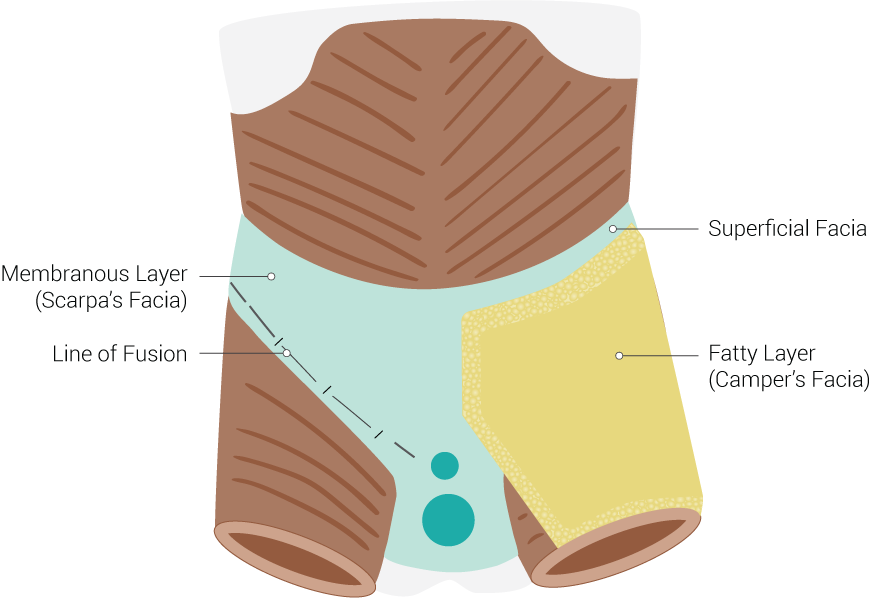
Fascial Layers. This illustration of fascial layers includes the superficial fascia, the fatty layer (Camper fascia), the line of fusion, and the membranous layer (Scarpa fascia).
Illustrated by B Palmer
References
Fede C, Clair C, Pirri C, Petrelli L, Zhao X, Sun Y, Macchi V, Stecco C. The Human Superficial Fascia: A Narrative Review. International journal of molecular sciences. 2025 Feb 3:26(3):. doi: 10.3390/ijms26031289. Epub 2025 Feb 3 [PubMed PMID: 39941057]
Level 3 (low-level) evidenceFormstone C, Aldeiri B, Davenport M, Francis-West P. Ventral body wall closure: Mechanistic insights from mouse models and translation to human pathology. Developmental dynamics : an official publication of the American Association of Anatomists. 2025 Feb:254(2):102-141. doi: 10.1002/dvdy.735. Epub 2024 Sep 25 [PubMed PMID: 39319771]
Pirri C, Petrelli L, Fede C, Guidolin D, Tiengo C, De Caro R, Stecco C. Blood supply to the superficial fascia of the abdomen: An anatomical study. Clinical anatomy (New York, N.Y.). 2023 May:36(4):570-580. doi: 10.1002/ca.23993. Epub 2023 Jan 10 [PubMed PMID: 36576229]
Albertin G, Astolfi L, Fede C, Simoni E, Contran M, Petrelli L, Tiengo C, Guidolin D, De Caro R, Stecco C. Detection of Lymphatic Vessels in the Superficial Fascia of the Abdomen. Life (Basel, Switzerland). 2023 Mar 20:13(3):. doi: 10.3390/life13030836. Epub 2023 Mar 20 [PubMed PMID: 36983991]
Hutzley S, Ruden E, Bosch KV, Schubert B, Markand S. Morphometric Analysis of Pyramidalis Muscle in Midwestern Americans: A Cadaveric Approach. Missouri medicine. 2023 Mar-Apr:120(2):139-142 [PubMed PMID: 37091943]
Chen DZ, Ganapathy A, Nayak Y, Mejias C, Bishop GL, Mellnick VM, Ballard DH. Analysis of Superficial Subcutaneous Fat Camper's and Scarpa's Fascia in a United States Cohort. Journal of cardiovascular development and disease. 2023 Aug 14:10(8):. doi: 10.3390/jcdd10080347. Epub 2023 Aug 14 [PubMed PMID: 37623360]
Valença-Filipe R, Mendes J, Pereira F, Vardasca R, Amarante J, Costa-Ferreira A. Physical properties of Scarpa's fascia. Clinical anatomy (New York, N.Y.). 2024 May:37(4):397-404. doi: 10.1002/ca.24087. Epub 2023 Jun 28 [PubMed PMID: 37377018]
Wijaya WA, Liu Y, He Y, Qing Y, Li Z. Abdominoplasty with Scarpa Fascia Preservation: A Systematic Review and Meta-analysis. Aesthetic plastic surgery. 2022 Dec:46(6):2841-2852. doi: 10.1007/s00266-022-02835-5. Epub 2022 Mar 17 [PubMed PMID: 35301571]
Level 1 (high-level) evidencevan der Sluis N, van Dongen JA, Caris FLS, Wehrens KME, Carrara M, van der Lei B. Does Scarpa's Fascia Preservation in Abdominoplasty Reduce Seroma? A Systematic Review. Aesthetic surgery journal. 2023 Jun 14:43(7):NP502-NP512. doi: 10.1093/asj/sjad024. Epub [PubMed PMID: 36747469]
Ullah SM, Grant RC, Johnson M, McAlister VC. Scarpa's fascia and clinical signs: the role of the membranous superficial fascia in the eponymous clinical signs of retroperitoneal catastrophe. Annals of the Royal College of Surgeons of England. 2013 Oct:95(7):519-22. doi: 10.1308/003588413X13629960048514. Epub [PubMed PMID: 24112501]
Patel AB, Osterberg EC, Satarasinghe PN, Wenzel JL, Akbani ST, Sahi SL, Emigh BJ, Wolf JS Jr, Brown CVR. Urethral Injuries: Diagnostic and Management Strategies for Critical Care and Trauma Clinicians. Journal of clinical medicine. 2023 Feb 13:12(4):. doi: 10.3390/jcm12041495. Epub 2023 Feb 13 [PubMed PMID: 36836030]