Introduction
The rotator cuff is a group of shoulder muscles that facilitate a wide range of motion while maintaining glenohumeral joint stability (see Image. Rotator Cuff Muscles). The rotator cuff includes the following muscles:
- Subscapularis
- Infraspinatus
- Teres minor
- Supraspinatus
A helpful mnemonic for recalling these muscles is "SITS." The glenohumeral joint is a ball-and-socket joint composed of a large spherical humeral head and a relatively small glenoid cavity. This configuration provides substantial mobility but limited intrinsic stability. The shoulder is stabilized by the coordinated function of static and dynamic stabilizers. Static stabilizers include the joint capsule, labrum, negative intraarticular pressure, and glenohumeral ligaments, while dynamic stabilizers include the rotator cuff muscles and the long head of the biceps brachii (see Image. Muscles of the Posterior Shoulder and Upper Arm).[1][2][3]
Rotator cuff pathology is a frequent cause of shoulder pain, weakness, impaired overhead function, and glenohumeral instability. Surgical management of rotator cuff disorders requires detailed knowledge of tendon insertions, neurovascular anatomy, and the rotator cuff interval to optimize repair and avoid iatrogenic injury. Knowledge of rotator cuff anatomy and biomechanics facilitates accurate diagnosis, physical examination, imaging interpretation, and treatment planning.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The primary biomechanical role of the rotator cuff is to stabilize the glenohumeral joint through compression of the humeral head against the glenoid. The 4 rotator cuff muscles originate from the scapula and insert on the humerus. The tendons of these muscles blend with the joint capsule to form a musculotendinous cuff that surrounds the anterior, superior, and posterior aspects of the joint while leaving the inferior aspect relatively unsupported. This anatomic configuration increases the risk of inferior glenohumeral dislocation. Coordinated contraction of the rotator cuff muscles maintains humeral head centering within the glenoid during shoulder motion, permitting a broad range of motion while preserving joint stability.
In addition to their stabilizing function, the rotator cuff muscles facilitate shoulder movement. The subscapularis is the primary medial (internal) rotator of the shoulder, whereas the infraspinatus and teres minor function primarily as lateral (external) rotators. The supraspinatus initiates shoulder abduction and is particularly important during the first 0° to 15° of motion, after which the deltoid becomes the principal abductor. Each rotator cuff muscle can be assessed independently during physical examination through maneuvers that evaluate its primary function.
Embryology
The pectoral girdle and upper limb bud muscles arise from distinct embryologic origins. The scapula and muscles attached to the medial border of the scapula are derived from paraxially located somites, whereas most upper limb bud structures are derived from lateral plate mesoderm that develops opposite somites 8 to 10. Additionally, connective tissue throughout the pectoral girdle, which maintains structural continuity with the axial skeleton, is continuous with the connective tissue of the limb and superficial tissues of the thoracic region.[4]
Upper limb development generally begins several days before lower limb formation. Precursor myoblasts migrate from multiple sources to form the dorsal and ventral premuscle masses of the limb bud during Stage 12, approximately Week 5 of development. The supraspinatus arises from cells within the dorsal premuscle mass. Upper limb musculature arises from a combination of somatic cells (muscle cells and myosatellite cells) and somatopleuric cells (tendons and other connective tissue structures). As the embryo reaches approximately 11 mm in length, formation of the scapular spine and acromion occurs concurrently with development of the deltoid cellular mass. The deltoid mass undergoes horizontal division between the 11-mm and 15-mm embryonic stages, forming a myoblast mass that subsequently develops into the supraspinatus and infraspinatus. This embryologic relationship contributes to the dynamic control of the glenohumeral joint.[5]
Blood Supply and Lymphatics
The vascular supply to the rotator cuff muscles is mainly via the suprascapular, subscapular, and posterior circumflex humeral arteries. The suprascapular artery is a branch of the thyrocervical trunk—a major branch of the subclavian artery—and originates at the base of the neck. The suprascapular artery enters the posterior scapular region superior to the suprascapular foramen (the nerve passes through the foramen) and supplies the supraspinatus and infraspinatus.
The subscapular artery is the largest branch of the axillary artery. The blood vessel originates from the 3rd part of the axillary artery, follows the inferior margin of the subscapularis, and then divides into the circumflex scapular and thoracodorsal arteries. The subscapular artery provides vascular supply to the subscapularis.
The posterior circumflex humeral artery originates from the 3rd part of the axillary artery in the axilla. The posterior circumflex humeral artery enters the posterior scapular region through the quadrangular space (accompanied by the axillary nerve) and supplies the teres minor.
The lymphatic drainage of the rotator cuff region primarily involves the subscapular (posterior) group of axillary lymph nodes. The subscapular nodes consist of 6 to 7 lymph nodes located along the posterior axillary fold. The subscapular nodes course along the subscapular vessels.
Efferent drainage from the subscapular, pectoral, and humeral axillary lymph node groups passes to the central axillary lymph nodes. The central axillary nodes consist of 3 to 4 lymph nodes located deep to the pectoralis minor near the base of the axilla, adjacent to the 2nd part of the axillary region. Efferent drainage from the central nodes passes to the apical axillary lymph nodes.
The apical axillary nodes lie at the apex of the axilla, near the medial aspect of the axillary vein and the 1st part of the axillary artery. Efferent vessels from the apical group traverse the cervicoaxillary canal, bounded by the clavicle, the 1st rib, and the superior border of the scapula. These efferent vessels converge to form the subclavian lymphatic trunk. The subclavian lymphatic trunk either joins the jugular and bronchomediastinal trunks to form the right lymphatic duct or drains directly into the right venous angle.
Nerves
Innervation of the rotator cuff arises from the subscapular, suprascapular, and axillary nerves. The subscapular nerve (upper and lower branches) provides motor impulses to the subscapularis. Subscapular nerve branches originate from the posterior cord of the brachial plexus and contain fibers from spinal nerves C5, C6, and C7. The suprascapular nerve supplies the supraspinatus and infraspinatus. The suprascapular nerve originates from the superior trunk of the brachial plexus, contains fibers from spinal nerves C5 and C6, and passes through the suprascapular foramen under the transverse scapular ligament. The axillary nerve innervates the teres minor. This nerve originates from the posterior cord of the brachial plexus, contains fibers from spinal nerves C5 and C6, and passes through the quadrangular space into the posterior scapular region.
Muscles
The subscapularis is the largest component of the posterior wall of the axilla. This muscle prevents anterior dislocation of the humerus during abduction and produces medial rotation of the arm. A large bursa separates the subscapularis from the neck of the scapula. The muscle originates from the subscapular fossa and inserts onto the lesser tubercle of the humerus.[6]
The supraspinatus is the only rotator cuff muscle not primarily responsible for humeral rotation. This muscle originates from the supraspinous fossa. The muscle passes superior to the glenohumeral joint and inserts onto the greater tuberosity of the humerus.
The infraspinatus functions as a powerful lateral rotator of the humerus. This muscle originates from the infraspinous fossa and inserts onto the greater tuberosity of the humerus, immediately inferior to the supraspinatus insertion. The tendon of the infraspinatus is sometimes separated from the capsule of the glenohumeral joint by a bursa.
The teres minor is a narrow, elongated muscle located deep to the deltoid and is often difficult to distinguish from the infraspinatus. The teres minor originates from the lateral border of the scapula, inferior to the infraglenoid tubercle, and inserts onto the greater tuberosity of the humerus, inferior to the infraspinatus tendon.
The teres minor, supraspinatus, infraspinatus, and subscapularis collectively form the rotator cuff. The supraspinatus, infraspinatus, and teres minor insert on the greater tubercle of the humerus, while the subscapularis inserts on the lesser tubercle. Collectively, these muscles stabilize the glenohumeral joint and contribute to rotation and abduction mechanics.[7]
Physiologic Variants
Few variants of the infraspinatus are described in current literature, although fusion with the teres minor has been reported in some individuals. Subchondral cysts may be identified at the insertion sites of the supraspinatus and infraspinatus on the humeral head. Subchondral cysts may be misinterpreted as rotator cuff pathology or degenerative change. Cysts located at dorsal insertion sites are typically asymptomatic. Cystic changes identified at the anterior aspect of the humerus warrant assessment for potential subscapularis pathology.[8]
Several physiologic variants of the subscapularis have been described, including accessory subscapularis slips and aberrant muscle tissue overlying the subscapularis. Additional muscle bellies or tendinous slips may arise from the anterior scapula and insert near the lesser tubercle, joint capsule, or proximal humerus. These variants may occasionally contribute to impingement or altered shoulder biomechanics. Aberrant muscle covering the subscapularis is a rare variant described in the literature, characterized by an additional muscular layer overlying the subscapularis.[9]
Magnetic resonance imaging (MRI) studies have demonstrated an aponeurotic expansion of the supraspinatus tendon adjacent to the bicipital groove in approximately 50% of evaluated images. The tendon-like structure arises from the anterior portion of the supraspinatus tendon and courses distally in a parallel orientation anterolateral to the long head of the biceps brachii tendon. Distal insertion occurs on the superior aspect of the pectoralis major tendon. The proposed function of this aponeurotic expansion includes reinforcement of the anterior supraspinatus tendon, which has a relatively small footprint on the greater tuberosity. A biomechanical role analogous to the rotator cable of the rotator cuff interval has been suggested.[10]
Clinical Significance
Rotator Cuff Syndrome
Rotator cuff syndrome (RCS) comprises a spectrum of clinical pathology, ranging from minor injuries such as acute rotator cuff tendinitis to advanced or chronic rotator cuff tendinopathy and degenerative conditions.[11] Rotator cuff injuries are a common cause of shoulder pain. Rotator cuff tendons, particularly the supraspinatus tendon, are uniquely susceptible to compressive forces from subacromial impingement. Improper athletic technique, poor posture, poor conditioning, and failure of the subacromial bursa to protect supporting tendons contribute to a progressive injury sequence from acute inflammation to calcification, degenerative thinning, and eventual tendon tear (see Image. Rotator Cuff Tear).[12][13][14]
Rotator cuff muscles may be evaluated independently in patients presenting with RCS. The supraspinatus is evaluated using the Jobe test, commonly referred to as the "empty can test." The arm is placed in abduction with internal rotation, with the thumb pointing downward, followed by application of downward resistance. A positive result occurs when pain or weakness is elicited during the maneuver. The infraspinatus may be assessed through resisted external rotation with the elbow flexed and the arm maintained in a neutral position of abduction and adduction. Teres minor evaluation is performed using the hornblower's test, with the arm abducted to 90° and the elbow flexed to 90° while external rotation is resisted. A positive test is indicated by pain or weakness during the maneuver.[15]
Subscapularis evaluation involves several specialized tests. The Gerber lift-off test is performed with the shoulder internally rotated and the dorsum of the hand placed against the lower back, followed by attempted active separation of the hand from the back. A positive result occurs when the patient is unable to lift the hand or experiences pain. The abdominal compression or belly-press test is used when the hand cannot be placed behind the back. This test requires internal rotation of the arm with the elbow flexed to 90° and the hand, wrist, and elbow aligned in a straight line, followed by pressing the hand against the abdomen. A positive result occurs when the elbow drifts posteriorly or when pain, weakness, or compensatory wrist flexion is observed. The bear hug test is performed with the patient placing the ipsilateral palm on the contralateral shoulder while resisting anterior force applied by the examiner, with failure to maintain position indicating a positive test finding.[16]
The American Academy of Orthopedic Surgeons suggests that patients with rotator cuff problems without tears can be treated conservatively with exercise and nonsteroidal anti-inflammatory drug (NSAID) therapy. The patient must learn to limit overhead activities and use ice packs or heating pads. Proper physical therapy effectively treats most patients without subacromial decompression. No significant difference in outcome has been reported for surgery over physical therapy in several trials. Subacromial injection with steroids showed a short-term benefit in some studies and may improve a patient's compliance with physical therapy. Surgical consultation is indicated if symptoms persist after 3 months of conservative management. Arthroscopic acromioplasty may be a topic to discuss with the patient.[17]
Rotator cuff tendonitis and tendinosis
Rotator cuff tendinitis and tendinosis represent a focal spectrum within RCS, reflecting acute inflammatory change and chronic degenerative tendon remodeling, respectively. Rotator cuff tendinitis typically corresponds to early overuse injury with reversible inflammatory features, whereas tendinosis reflects collagen disorganization, mucoid degeneration, and reduced tendon tensile capacity. Clinical evaluation aligns with RCS assessment, including pain provocation testing and strength assessment, with imaging via ultrasound or MRI used to characterize tendon integrity and chronicity. Management is primarily conservative, including load modification, NSAID administration, structured physical therapy, and selective use of subacromial corticosteroid injection, with escalation based on symptom persistence and functional limitation.
Shoulder impingement
"Shoulder impingement" is a clinical term often used nonspecifically to describe pain and symptoms associated with overhead activity. Shoulder impingement is best subdivided into internal and external forms.
Internal impingement is commonly observed in overhead-throwing athletes, such as baseball pitchers and javelin throwers. The condition affects the posterior lateral articular surface of the rotator cuff, where contact occurs between the cuff and the posterior superior glenoid rim and labrum during maximal abduction and external rotation of the shoulder, particularly during the late cocking phase of throwing. The term “thrower’s shoulder” describes a constellation of adaptive anatomic changes that develop over time in this population. These adaptive changes include increased humeral retroversion and posterior capsular tightness. Glenohumeral internal rotation deficit results from these adaptations and is recognized as a predisposing factor for internal impingement.[18]
External impingement is commonly used synonymously with shoulder impingement syndrome. External impingement involves compression of the rotator cuff by extrinsic structures, including the acromion, resulting in subacromial bursitis and bursal-sided rotator cuff injury.[19]
On clinical examination, the primary complaint is lateral shoulder pain that typically worsens with overhead activities. Patients often describe a painful arc during flexion and abduction from 60° to 120°, along with nocturnal pain when lying on the affected side. The presentation may be acute or chronic. Acute presentation is more common in younger patients following a recent traumatic event or significant overexertion (eg, lifting a heavy box). Functional impairment is often significant in acute cases. Chronic presentation is more common in older patients or individuals with repetitive overhead activity, with gradual loss of strength and function.
The range of motion is typically preserved, although provocative testing is positive. The Hawkins-Kennedy test elicits pain with passive forced internal rotation of the shoulder.
Evaluation of shoulder impingement may include subscapularis testing with the Gerber lift-off, belly-press, and bear hug maneuvers. The lift-off test result is positive when hand lift from the back is not possible, or pain is present. The belly-press test finding is positive when the elbow drifts posteriorly, or wrist flexion compensates. The bear hug test is positive when the patient cannot resist external rotation.
Partial- and full-thickness rotator cuff tears
The potential etiologies and underlying causes of rotator cuff tears are multifaceted. Degeneration, impingement, and tensile overload secondary to trauma may all contribute to the development of rotator cuff tears. Supraspinatus tendon tears most often begin as partial-thickness injuries. Progression to full-thickness tears may occur over time, with potential involvement of all 4 rotator cuff muscles. Rotator cuff tears most commonly present in middle-aged to older patients. Repetitive overhead activity is a frequent etiology in younger athletic populations. Rotator cuff tears involving the teres minor do not demonstrate spontaneous healing.
Pain and weakness are the primary presenting symptoms on examination. Pain is typically localized over the lateral deltoid, worsens with overhead activity, and is exacerbated by lying on the affected side at night. Absence of pain does not exclude the diagnosis, as a significant proportion of patients may be asymptomatic. In fact, partial-thickness tears are associated with greater pain and disability than full-thickness tears.
The drop arm test provides confirmatory evidence. When performing this test, the patient elevates the arm to shoulder level in abduction, followed by slow, controlled descent. A positive result occurs when the arm drops suddenly or cannot be lowered smoothly, consistent with a rotator cuff tear.
The Napoleon test is performed in a manner similar to the abdominal compression test. A positive result occurs when effective abdominal compression is achieved only with compensatory wrist flexion to 90°. An intermediate result, indicating partial subscapularis function, is observed when wrist flexion occurs between 30° and 60°.[20]
Shoulder radiography is typically the 1st-line imaging modality for undifferentiated shoulder pain. The results are usually unremarkable, though x-rays may assist in the identification of large rotator cuff tears when humeral migration over the glenoid is present in a symptomatic shoulder. Radiographs are likely to be normal in subscapularis injury. However, an avulsion may demonstrate a bony abnormality.
MRI is generally considered the most accurate modality for the evaluation of rotator cuff injuries. MRI provides critical information regarding the degree of tendon tear, tendon retraction, and muscle atrophy, which is essential for preoperative planning of rotator cuff repair. Findings in subscapularis tendon tears may range from mild degenerative changes to full-thickness tendon disruption. MRI also allows assessment of the muscle belly.
Diagnostic ultrasound is a cost-effective and accessible modality for evaluation of the subscapularis tendon when performed by an experienced sonographer. Ultrasound provides less anatomical detail compared with MRI but is useful for diagnosis and management.[21]
Conservative treatment with NSAIDs and, most importantly, physical therapy, is the 1st-line approach to management. Many patients regain functional capacity with conservative management. However, surgical intervention is indicated when pain, weakness, or functional impairment persists.[22][23][24]
Partial-thickness tears may be managed with debridement. Full-thickness tears may warrant side-to-side repair. Complete avulsions require reattachment to bone.
Surgical repair may be performed via open or arthroscopic approaches. Arthroscopic treatment is indicated for both acute and chronic full-thickness tears, as delays may result in significant muscle atrophy, tendon retraction, and poorer surgical outcomes.
Other Issues
The rotator cuff interval is a region located between the supraspinatus and subscapularis tendons. The structure and function of this space were evaluated in a study by Jost et al. The rotator cuff interval was found to comprise the supraspinatus tendon, the subscapularis tendon, the coracohumeral ligament, the superior glenohumeral ligament, and the glenohumeral joint capsule.[25]
The rotator cuff interval is divisible into a 2-layer medial portion and a 4-layer lateral portion. The medial portion limits inferior translation. The lateral portion is subdivided into a 3-layer fibrous plate and a 1-layer lateral component, and it has a primary role in limiting external rotation when the arm is adducted.
The coracohumeral ligament component of the rotator cuff interval is identified as a key stabilizing structure. The coracohumeral ligament contributes to restriction of external rotation, limitation of inferior translation, and overall stability of the glenohumeral joint.
Rotator cuff interval function is an important surgical consideration. Closure of the lateral portion of the rotator cuff interval restricts external rotation of the adducted shoulder. Therefore, closure should be performed with the shoulder positioned in external rotation to preserve postoperative range of motion.
Superior migration of the humeral head secondary to rotator cuff tear or insufficiency may require release of the medial coracohumeral ligament to maintain central positioning of the humeral head within the glenoid fossa.
Contracture of the rotator cuff interval with restricted external rotation may be managed by lateral interval release while maintaining integrity of the coracohumeral ligament. Lim et al identified the presence of the pectoralis minor tendon inserting into the rotator cuff interval in 11 of 99 subjects studied. The pectoralis minor tendon tethered the retracted supraspinatus tendon in 7 of the 11 subjects. This tethering increased the tension across the tendon repair. Complete resection of the pectoralis minor tendon was required in these cases to achieve optimal repair.[26]
Media
(Click Image to Enlarge)
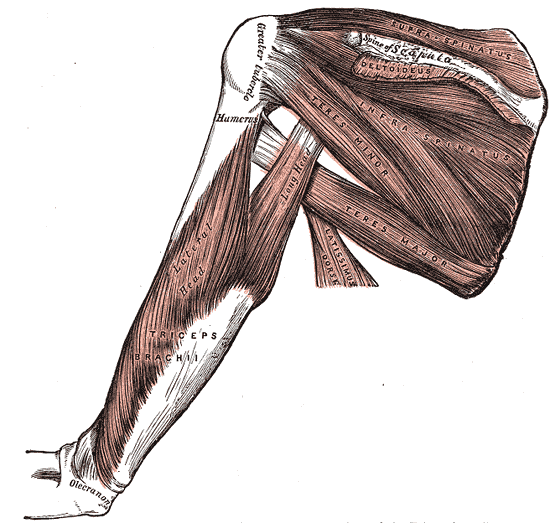
Muscles of the Posterior Shoulder and Upper Arm. This posterior view of the right upper limb highlights the deep musculature of the scapular and brachial regions. The rotator cuff and surrounding muscles are visible, including the supraspinatus, infraspinatus, teres minor, teres major, and a reflected portion of the deltoideus arising near the spine of the scapula. The triceps brachii is detailed with its long head and lateral head visible along the humerus, extending down toward the olecranon. A section of the latissimus dorsi is also shown inferior to the scapular muscles. The greater tubercle of the humerus serves as a prominent lateral landmark.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
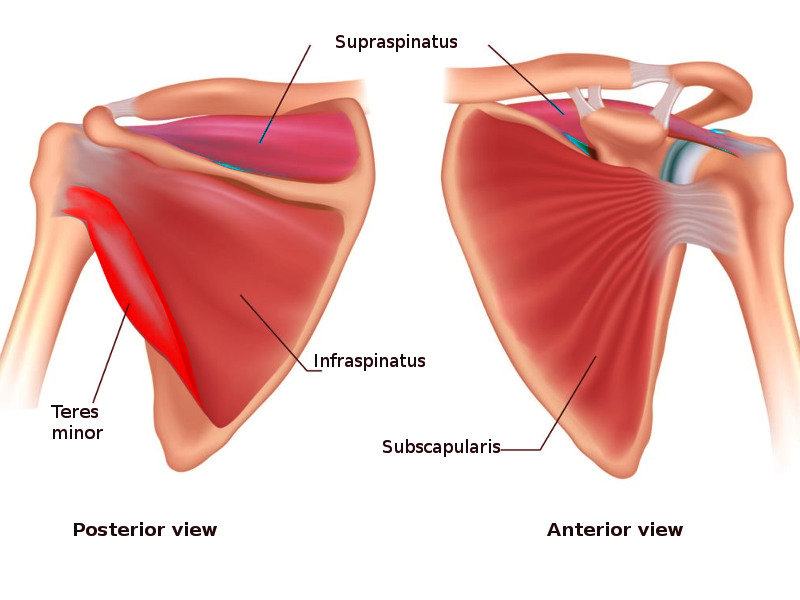
Rotator Cuff Muscles. This dual-panel illustration displays the rotator cuff muscles, which are prominent shoulder girdle muscles, from 2 distinct anatomical perspectives. The posterior view on the left demonstrates the supraspinatus, infraspinatus, and teres minor situated along the posterior aspect of the scapula. The anterior view on the right isolates the broad subscapularis covering the subscapular fossa, while also showing the anterior projection of the supraspinatus deep to the clavicle and acromion.
Contributed by O Chaigasame, MD
(Click Image to Enlarge)
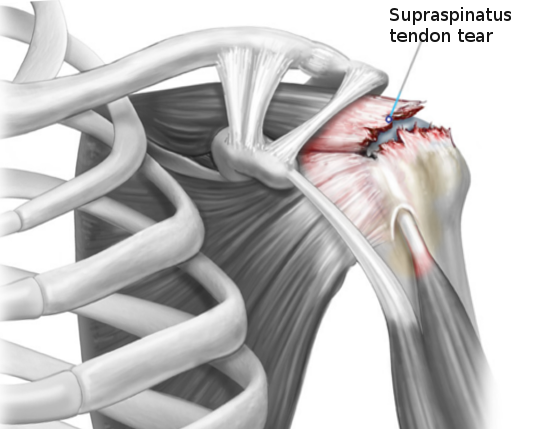
Rotator Cuff Tear. This anterior view of the left shoulder shows a severe rotator cuff injury with a prominent tear of the supraspinatus tendon near its insertion on the greater tubercle of the humerus. The clavicle, acromion, coracoid process, ribs, and long head of the biceps brachii tendon provide anatomical context for the lesion.
Contributed by S Bhimji, MD
References
Varacallo MA, El Bitar Y, Sina RE, Mair SD. Rotator Cuff Syndrome. StatPearls. 2026 Jan:(): [PubMed PMID: 30285401]
Varacallo MA, El Bitar Y, Mair SD. Rotator Cuff Tendonitis. StatPearls. 2026 Jan:(): [PubMed PMID: 30335303]
Cowan PT, Mudreac A, Varacallo MA. Anatomy, Back, Scapula. StatPearls. 2026 Jan:(): [PubMed PMID: 30285370]
Valasek P, Theis S, DeLaurier A, Hinits Y, Luke GN, Otto AM, Minchin J, He L, Christ B, Brooks G, Sang H, Evans DJ, Logan M, Huang R, Patel K. Cellular and molecular investigations into the development of the pectoral girdle. Developmental biology. 2011 Sep 1:357(1):108-16. doi: 10.1016/j.ydbio.2011.06.031. Epub 2011 Jun 29 [PubMed PMID: 21741963]
Level 3 (low-level) evidenceWarmbrunn MV, de Bakker BS, Hagoort J, Alefs-de Bakker PB, Oostra RJ. Hitherto unknown detailed muscle anatomy in an 8-week-old embryo. Journal of anatomy. 2018 Aug:233(2):243-254. doi: 10.1111/joa.12819. Epub 2018 May 3 [PubMed PMID: 29726018]
Vosloo M, Keough N, De Beer MA. The clinical anatomy of the insertion of the rotator cuff tendons. European journal of orthopaedic surgery & traumatology : orthopedie traumatologie. 2017 Apr:27(3):359-366. doi: 10.1007/s00590-017-1922-z. Epub 2017 Feb 16 [PubMed PMID: 28204962]
Medina G, Bartolozzi AR 3rd, Spencer JA, Morgan C. The Thrower's Shoulder. JBJS reviews. 2022 Mar 18:10(3):. doi: 10.2106/JBJS.RVW.21.00194. Epub 2022 Mar 18 [PubMed PMID: 35302966]
Kadi R, Milants A, Shahabpour M. Shoulder Anatomy and Normal Variants. Journal of the Belgian Society of Radiology. 2017 Dec 16:101(Suppl 2):3. doi: 10.5334/jbr-btr.1467. Epub 2017 Dec 16 [PubMed PMID: 30498801]
Zielinska N, Tubbs RS, Konschake M, Olewnik Ł. Unknown variant of the accessory subscapularis muscle? Anatomical science international. 2022 Jan:97(1):138-142. doi: 10.1007/s12565-021-00633-8. Epub 2021 Sep 30 [PubMed PMID: 34591277]
Moser TP, Cardinal É, Bureau NJ, Guillin R, Lanneville P, Grabs D. The aponeurotic expansion of the supraspinatus tendon: anatomy and prevalence in a series of 150 shoulder MRIs. Skeletal radiology. 2015 Feb:44(2):223-31. doi: 10.1007/s00256-014-1993-4. Epub 2014 Sep 2 [PubMed PMID: 25179795]
D'Ambrosi R, Ragone V, Comaschi G, Usuelli FG, Ursino N. Retears and complication rates after arthroscopic rotator cuff repair with scaffolds: a systematic review. Cell and tissue banking. 2019 Mar:20(1):1-10. doi: 10.1007/s10561-019-09750-1. Epub 2019 Jan 23 [PubMed PMID: 30673902]
Level 1 (high-level) evidenceWolff AB, Sethi P, Sutton KM, Covey AS, Magit DP, Medvecky M. Partial-thickness rotator cuff tears. The Journal of the American Academy of Orthopaedic Surgeons. 2006 Dec:14(13):715-25 [PubMed PMID: 17148619]
Inderhaug E, Kalsvik M, Kollevold KH, Hegna J, Solheim E. Long-term results after surgical treatment of subacromial pain syndrome with or without rotator cuff tear. Journal of orthopaedics. 2018 Sep:15(3):757-760. doi: 10.1016/j.jor.2018.03.004. Epub 2018 Mar 17 [PubMed PMID: 29946199]
Harrison AK, Flatow EL. Subacromial impingement syndrome. The Journal of the American Academy of Orthopaedic Surgeons. 2011 Nov:19(11):701-8 [PubMed PMID: 22052646]
Dupuis F, Barrett E, Dubé MO, McCreesh KM, Lewis JS, Roy JS. Cryotherapy or gradual reloading exercises in acute presentations of rotator cuff tendinopathy: a randomised controlled trial. BMJ open sport & exercise medicine. 2018:4(1):e000477. doi: 10.1136/bmjsem-2018-000477. Epub 2018 Dec 26 [PubMed PMID: 30622733]
Level 1 (high-level) evidenceHippensteel KJ, Brophy R, Smith MV, Wright RW. A Comprehensive Review of Physical Examination Tests of the Cervical Spine, Scapula, and Rotator Cuff. The Journal of the American Academy of Orthopaedic Surgeons. 2019 Jun 1:27(11):385-394. doi: 10.5435/JAAOS-D-17-00090. Epub [PubMed PMID: 30383577]
Tashjian RZ. AAOS clinical practice guideline: optimizing the management of rotator cuff problems. The Journal of the American Academy of Orthopaedic Surgeons. 2011 Jun:19(6):380-3 [PubMed PMID: 21628649]
Level 3 (low-level) evidenceKibler WB, Sciascia AD, Grantham WJ. The shoulder joint complex in the throwing motion. Journal of shoulder and elbow surgery. 2024 Feb:33(2):443-449. doi: 10.1016/j.jse.2023.06.031. Epub 2023 Jul 26 [PubMed PMID: 37499784]
Farfaras S, Sernert N, Rostgard Christensen L, Hallström EK, Kartus JT. Subacromial Decompression Yields a Better Clinical Outcome Than Therapy Alone: A Prospective Randomized Study of Patients With a Minimum 10-Year Follow-up. The American journal of sports medicine. 2018 May:46(6):1397-1407. doi: 10.1177/0363546518755759. Epub 2018 Mar 15 [PubMed PMID: 29543510]
Level 2 (mid-level) evidenceHanchard NC, Lenza M, Handoll HH, Takwoingi Y. Physical tests for shoulder impingements and local lesions of bursa, tendon or labrum that may accompany impingement. The Cochrane database of systematic reviews. 2013 Apr 30:2013(4):CD007427. doi: 10.1002/14651858.CD007427.pub2. Epub 2013 Apr 30 [PubMed PMID: 23633343]
Level 1 (high-level) evidenceZheng F, Wang H, Gong H, Fan H, Zhang K, Du L. Role of Ultrasound in the Detection of Rotator-Cuff Syndrome: An Observational Study. Medical science monitor : international medical journal of experimental and clinical research. 2019 Aug 6:25():5856-5863. doi: 10.12659/MSM.915547. Epub 2019 Aug 6 [PubMed PMID: 31386649]
Level 2 (mid-level) evidenceDi Benedetto P, Beltrame A, Cicuto C, Battistella C, Gisonni R, Cainero V, Causero A. Rotator cuff tears reparability index based on pre-operative MRI: our experience. Acta bio-medica : Atenei Parmensis. 2019 Jan 10:90(1-S):36-46. doi: 10.23750/abm.v90i1-S.8074. Epub 2019 Jan 10 [PubMed PMID: 30714997]
Karjalainen TV, Jain NB, Page CM, Lähdeoja TA, Johnston RV, Salamh P, Kavaja L, Ardern CL, Agarwal A, Vandvik PO, Buchbinder R. Subacromial decompression surgery for rotator cuff disease. The Cochrane database of systematic reviews. 2019 Jan 17:1(1):CD005619. doi: 10.1002/14651858.CD005619.pub3. Epub 2019 Jan 17 [PubMed PMID: 30707445]
Level 1 (high-level) evidenceWitney-Lagen C, Mazis G, Bruguera J, Atoun E, Sforza G, Levy O. Do elderly patients gain as much benefit from arthroscopic rotator cuff repair as their younger peers? Journal of shoulder and elbow surgery. 2019 Jun:28(6):1056-1065. doi: 10.1016/j.jse.2018.10.010. Epub 2019 Jan 28 [PubMed PMID: 30704915]
Ahmad ZY, Diaz LE, Roemer FW, Goud A, Guermazi A. Imaging Review of Subscapularis Tendon and Rotator Interval Pathology. Radiology research and practice. 2022:2022():4009829. doi: 10.1155/2022/4009829. Epub 2022 Jan 11 [PubMed PMID: 35070451]
Servasier L, Jeudy J, Raimbeau G, Bigorre N. Arthroscopic release of the pectoralis minor tendon as an adjunct to acromioplasty in the treatment of subacromial syndrome associated with scapular dyskinesia. Orthopaedics & traumatology, surgery & research : OTSR. 2022 Apr:108(2):103211. doi: 10.1016/j.otsr.2022.103211. Epub 2022 Jan 22 [PubMed PMID: 35077896]