Introduction
Acute retinal necrosis (ARN) is characterized by peripheral necrotizing retinitis, usually caused by varicella-zoster virus (VZV) or herpes simplex virus (HSV-1 or HSV-2).[1] Other rare causes include cytomegalovirus (CMV) and Epstein-Barr virus (EBV).[1] Typically, ARN occurs in immunocompetent individuals; however, it can also occur in patients who are immunocompromised. Although mostly unilateral, up to 30% of patients can develop bilateral ARN, usually over the course of a few weeks to years.[2] The disease was first described in 1971 in Japan by Urayama et al.[3] They described 6 patients with panuveitis with vitritis, retinal periarteritis, peripheral confluent areas of retinal necrosis, and retinal detachment.[3] Acute retinal necrosis has also been referred to as Kirisawa uveitis in Japan.[3] Results from recent reviews emphasize that polymerase chain reaction (PCR) confirmation from aqueous or vitreous samples is now considered standard in most centers, even though ARN remains a clinical diagnosis.[4] Acute retinal necrosis, progressive outer retinal necrosis, and CMV retinitis may represent a spectrum of herpetic necrotizing retinitides modulated by host immunity and other factors.[5] Untreated patients have a high rate of bilateral involvement and disease progression with retinal detachment in the same eye.[6][7][8] Despite treatment, many patients may have vision loss due to various causes, including recurrent retinal detachment and optic atrophy.[9]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Acute retinal necrosis is usually caused by herpesviruses (VZV, HSV-1, HSV-2; rarely CMV or EBV). Results from large series and reviews report VZV as the predominant pathogen, often accounting for more than 80% to 90% of PCR-confirmed cases in adult cohorts.[8][10] Findings from recent studies have underscored that mixed infections and atypical presentations can occur, particularly in immunosuppressed patients, reinforcing the role of multiplex PCR in ocular fluids.[10][11] ARN due to VZV (VZV-ARN) may present at an older age than HSV-ARN (51 years vs 34 years).[12] A higher proportion of patients with HSV-ARN (52%) may have at least 20/60 visual acuity at presentation compared with those with VZV-ARN (35%).[12] VZV-ARN may be associated with a higher proportion of patients with poor vision (≤ 20/200) at 1 year, more severe vision loss, and a higher risk of retinal detachment (2.5-fold more common in VZV-ARN compared to HSV-ARN).[12] Findings from a case series noted that HSV-2 was the predominant cause of ARN in individuals younger than 25, while VZV and HSV-1 caused ARN in patients older than 25 years.[13] The median age of HSV-2 ARN, HSV-1 ARN, and VZV-ARN in this series was 20, 47, and 57 years, respectively.[13]
Epidemiology
Acute retinal necrosis often occurs in immunocompetent individuals, affecting men and women equally.[14] Acute retinal necrosis tends to occur in older patient populations as VZV immunity wanes. HSV-induced retinitis typically affects younger patients.[1][15] In pediatric patients and in patients younger than 21 years with ARN, HSV-2 should be considered the primary candidate virus.[16] Findings from a series of 12 eyes from 11 patients with HSV-2 ARN suggested that it may represent HSV-2 reactivation.[15] There was a history of neonatal herpes, a history of ARN, chorioretinal scars, and triggering events such as periocular trauma, neurosurgery, and high-dose corticosteroids in different patients.[15] Patients with HSV-2 ARN may have a history of meningitis, whereas those with HSV-1 ARN may have a history of encephalitis.[13][15] Acute retinal necrosis can also occur in immunocompetent patients who become immunosuppressed via corticosteroids, noncorticosteroid immunosuppressants, and chemotherapeutics. Acute retinal necrosis is also observed in patients with acquired immune deficiency syndrome and other immunocompromised patients. The antigens HLA-Aw33, HLA-B44, and HLA-DRw6 have been associated with ARN in the Japanese population. Acute retinal necrosis has also been observed in North American White populations with HLA-DQw7, HLA-Bw62, and HLA-DR4.[17] Results from a 2024 cohort (65 eyes) reported a mean age of 40 to 60 years, with VZV overwhelmingly predominant (93.8%), and a minority of patients with immunosuppression (8.5%).[8]
Pathophysiology
The virus infects retinal cells and causes necrosis. Because necrosis results from virally induced cytolysis and arteriolar and choriocapillaris occlusion, the necrotic cells slough into the vitreous chamber, exposing large areas devoid of retinal cells. During the acute phase, viral particles trigger an inflammatory response that damages retinal cells. Arteriole inflammation leads to vaso-occlusive events, thereby accelerating the rapid necrosis of retinal tissue. Contractile membranes may form in the vitreous and on the surface of the damaged retina in the late phase. Multiple breaks in the lamina cribrosa and at the margin of the normal, necrotic, and inflamed retina are caused by retinal necrosis. This process may lead to retinal detachment. Retinal detachment may occur in up to 75% of eyes with ARN within 3 months of symptom onset.[18] Vitreous traction and proliferative vitreoretinopathy often complicate retinal detachment in ARN, reducing surgical success rates.[19] The breaks may be located posteriorly as well as peripherally.[19] VZV-ARN was associated with high interleukin-10 (IL-10) levels, a higher percentage of CD8+ T cells, and a lower CD4:CD8 T-cell ratio in the aqueous humor compared to noninfectious acute anterior uveitis cases.[20] Higher proportions of serum T-helper 17 (Th17) cells and higher serum and aqueous humor levels of cytokines associated with Th17 (IL-6, IL-17, IL-17F, IL-21, IL-22) were noted in patients with ARN compared to controls.[21]
Histopathology
Acute retinal necrosis shows distinct histopathological features characterized by fulminant retinal necrosis, vasculitis, and viral cytopathic changes.[22] Histology of enucleated eyes from patients with ARN reveals widespread acute retinal necrosis, loss of normal retinal architecture, and massive retinal tissue degeneration.[22] Prominent retinal arteritis (vasculitis), with inflammatory infiltrates around arterioles and often occlusion of retinal vessels, contributing to ischemia and further necrosis, is also present.[22] In many cases, eosinophilic intranuclear inclusion bodies are observed within infected retinal cells, a hallmark of herpes-group viral infection.[22] Electron microscopy confirms the presence of herpesvirus particles in all layers of the necrotic retina, supporting a direct viral cytolytic effect.[22] In addition to retinal tissue changes, the adjacent choroid may show marked infiltration by lymphoid-like (mononuclear) agranular inflammatory cells, indicating choroiditis or choroidal involvement.[23]
History and Physical
Patients often present with rapid onset of ocular or periocular pain, eye movement pain, redness, photophobia (light sensitivity), floaters, decreased vision, blurred vision, and visual field constriction. The following should be considered: risk factors for adult immunodeficiency syndrome, immune status, any systemic disease, any previous herpetic infection, including encephalitis, and any ocular therapy or surgery. An ocular examination that evaluates the anterior chamber and vitreous cells, intraocular pressure, and dilated retinal examination with indirect ophthalmoscopy and scleral depression is required. Physical examination often reveals multifocal, confluent, well-demarcated areas of peripheral retinal whitening, suggesting retinitis or retinal necrosis (See Image. Acute Retinal Necrosis.) A physical examination can also reveal occlusive arteritis and a prominent inflammatory reaction in the vitreous and anterior chamber. The posterior pole is usually spared in the early stages of the disease. The phase of active retinitis usually lasts 4 to 6 weeks, during which an exudative retinal detachment may occur.[24]
Slit lamp examination findings include conjunctival injection, scleritis, episcleritis, keratitis, or anterior uveitis (granulomatous or nongranulomatous). Increased intraocular pressure, sheathed retinal arterioles, retinal hemorrhage, optic disc edema, and retinal detachment can also be observed. The media haze and vitritis are typical of ARN and denote inflammatory activity in an immunocompetent host.[25] These findings help distinguish ARN from CMV retinitis and progressive outer retinal necrosis in patients with immunocompromised states in whom the media is typically clear, and vitritis is minimal.[26]
A typical presentation is severe anterior segment inflammation with fibrin with or without posterior synechia. The media is usually hazy due to anterior segment haze, vitritis, or cataracts. The fundus examination may reveal disc edema and peripheral yellowish areas of retinitis, which subsequently become confluent. A retinal hemorrhage is usually not very prominent if present. Kyrieleis periarteriolar plaque may be seen in ARN.[27] Extensive quadrantic involvement and poor presenting visual acuity are essential adverse prognostic indicators.[8][28] Rarely, ARN can initially present with posterior pole retinitis, which should be confirmed by PCR of aqueous or vitreous humor for HSV, VZV, CMV, or EBV).[29]
Evaluation
Acute retinal necrosis is a clinical diagnosis, and treatment should not be delayed. The classic triad of ARN consists of arteritis and phlebitis of the retinal and choroidal vasculature, a confluent, necrotizing retinitis that preferentially affects the peripheral retina, and moderate to severe vitritis.[3][30][3]The American Uveitis Society criteria for the diagnosis of ARN require the following clinical characteristics:
- Focal, well-demarcated areas of retinal necrosis located in the peripheral retina (outside of the major temporal vascular arcades)
- Rapid, circumferential progression of necrosis (if antiviral therapy has not been administered)
- Evidence of occlusive vasculopathy
- A prominent inflammatory reaction in the vitreous, and anterior chamber
- Supporting clinical criteria include optic neuropathy or optic atrophy, scleritis, and pain [10]
Three zones have been described for the description of the involved area of retinitis, (originally for CMV retinitis).[31] Retinitis at zone 1 (3000 μm around the center of the fovea and 1500 μm from the margin of the optic disc) is thought to be immediately sight-threatening. Zone 2 is the zone between zone 1 and the clinical equator, denoted by the anterior margin of the vortex ampulla. Zone 3 is anterior to zone 2 to the ora serrata. In a patient who presents with clinical findings of acute retinal necrosis, the clinician should consider a complete blood cell count with differential, baseline liver and renal function tests, human immunodeficiency virus testing, fluorescent treponemal antibody absorption, rapid plasma reagin, erythrocyte sedimentation rate, toxoplasmosis titers, purified protein derivative skin test, and chest radiograph to rule out other etiologies.
- An anterior chamber paracentesis or vitreous tap for PCR for herpesviruses (VZV, HSV, CMV, EBV) and toxoplasmosis PCR can be performed in atypical cases. Although PCR of ocular fluids can support the clinical diagnosis of ARN, treatment should not be delayed for the results. PCR for VZV or HSV in the aqueous or vitreous humor of suspected ARN is positive in 79% to 100% of cases.[4]
- In the rare cases with negative PCR results but high clinical suspicion, retinal biopsy using a pars plana approach may be appropriate.[32]
- Serum viral titers (VZV, HSV, and CMV) are also helpful.
- Intravenous fluorescein angiography can also be considered and may demonstrate the occlusive nature of retinal arteritis, capillary nonperfusion, and optic disc leakage.
- Optical coherence tomography scans of the retinitis patch may demonstrate hyperreflectivity and retinal layer disorganization, revealing the level of involvement and the presence of vitreous cells. Optical coherence tomography of the macula and optic nerve head may reveal cystoid macular edema, epiretinal membrane, or disc edema.
- Ultrawide-field fundus photography (Optos) may document disease progression and help monitor disease activity.[33][34]
- Ultrasonography (USG B-scan) may help rule out retinal detachment in hazy media.
- If intraocular lymphoma, tertiary syphilis, or encephalitis is suspected, a CT scan or MRI of the brain and lumbar puncture should be performed. Magnetic resonance imaging has shown lesions in the lateral geniculate, optic tracts, and chiasm even in immunocompetent patients with ARN who have no clinical evidence of encephalitis, suggesting viral spread through the central nervous system via axoplasmic transport from retinal ganglion cells.[35]
Multimodal imaging is crucial: wide-field fundus photography, ultra–wide-field angiography, and optical coherence tomography (including OCT-A) are recommended to document the extent of necrosis, occlusive vasculitis, cystoid macular edema, and macular or optic nerve involvement.
Treatment / Management
Immediate treatment is required and can be performed in either the inpatient or outpatient setting. The goal is to decrease the incidence of glaucoma in the fellow eye. Results from 1 study showed that 75% of patients treated with acyclovir remained disease-free in the fellow eye at 2 years, compared with 35% of patients not treated with acyclovir.[6] However, treatment does not reduce the rate of retinal detachment in the first eye.
Acyclovir has potent antiviral activity against VZV, HSV types 1 and 2, and Epstein–Barr virus; however, it has low antiviral activity against CMV. Induction therapy should be started with intravenous (IV) acyclovir at 10 to 13 mg/kg every 8 hours or 1500 mg/m2/d for 5 to 10 days.[36] Maintenance therapy follows, with oral acyclovir at 400 to 800 mg 5 times daily for 3 to 6 months, depending on the clinical response. In findings from one study, 12 patients with ARN were treated with intravenous acyclovir 1500 mg/m2/d, oral aspirin or warfarin, and oral corticosteroids (in 9 patients) after the initiation of acyclovir. The regression of retinitis lesions began at a mean of 3.9 days after the initiation of intravenous acyclovir, and lesions regressed completely in a mean of 32.5 days. Although progression was occasionally observed within 48 hours of initiation of therapy, no new retinitis lesions or progressive optic nerve involvement were observed thereafter. The study also noted that the therapy did not reduce the risk of retinal detachment (occurring in 11 of 13 eyes after an average of 59 days of therapy initiation) or vitritis.[7] Other options for induction therapy include:
- Oral valacyclovir 2000 mg 3 to 4 times daily (6000-8000 mg daily) for 7 to 10 days [4]
- Oral famciclovir 500 mg 3 times daily
- Oral valganciclovir 900 mg twice daily has been successfully used for CMV retinitis, but it also has activity against HSV and VZV. Valganciclovir can be used as empiric therapy if PCR results are not available.
These drugs have good oral bioavailability and do not require intravenous administration. Hospital admission and intravenous therapy are usually required only for patients who are unable to tolerate oral formulations, have definitive or suspected systemic involvement, are immunosuppressed, or have social factors that interfere with adherence.[37]
Findings from recent literature increasingly favor high-dose oral valacyclovir (or famciclovir or valganciclovir) as first-line therapy in many immunocompetent patients.[25] Newer oral agents with good bioavailability can achieve comparable systemic exposure and are widely used, especially when inpatient intravenous therapy is logistically challenging.[9] Systemic antivirals are the mainstay, and systemic treatment reduces contralateral eye involvement and may limit progression, although no regimen has clearly demonstrated superiority in high-quality comparative trials.[38] Monitoring renal function and dose adjustment with acyclovir, valganciclovir, and ganciclovir are essential. Initial intravenous or oral antiviral therapy is effective in the treatment of ARN, as measured by the time to the regression of retinitis and involvement of the fellow eye.[4](A1)
Intravitreal injections should be performed if sight-threatening retinitis, optic disc, or macula involvement (zone 1) is present. Ganciclovir (2–4 mg/0.1 mL) or foscarnet (1.2–2.4 mg/0.1 mL) can be administered. Injections may be repeated every 2 weeks, depending on the clinical response. Newer data provide a more substantial support for combined systemic plus intravitreal therapy. For example, findings from a 2022 cohort of combination therapy showed improved visual acuity and reduced progression when intravitreal agents were added early to systemic antivirals.[39] Intravitreal therapy should not be used as monotherapy because it does not protect the fellow eye, but is recommended as adjunctive treatment in sight-threatening or rapidly progressive cases.
The American Academy of Ophthalmology published an Ophthalmic Technology Assessment on the Diagnosis and Treatment of Acute Retinal Necrosis. The majority of patients with ARN without central nervous system involvement can be treated with oral valacyclovir (6000 mg–8000 mg daily) for 7 to 10 days. Intravitreal injection of foscarnet 2.4 mg should be considered. Diagnostic aqueous PCR testing should be performed in patients with unclear presentations, but the use of antiviral therapy should not be delayed. Long-term maintenance therapy (typically 1000 mg valacyclovir daily) for 6 months or more is common.[4]
Prednisone 0.5 to 2.0 mg/kg/d orally for up to 6 to 8 weeks should be started 24 to 48 hours after the start of antiviral therapy or once regression of necrosis is demonstrated on physical examination. Oral corticosteroids should be considered, particularly when the optic nerve is involved. A subtenon injection of triamcinolone 40 mg/1 mL can be considered after antiviral therapy is initiated. Periocular or oral corticosteroids should not be initiated in active retinitis before antiviral treatment, as they may worsen the retinitis. There is a lack of randomized data, and the potential for harm with corticosteroids if antivirals are inadequate. Topical cycloplegic agents and corticosteroids should be considered in the presence of an anterior chamber reaction.
Abnormal platelet function (platelet hyperaggregation) was noted in 6 of 7 patients with bilateral ARN.[40] Antiplatelet therapy, such as aspirin or warfarin, may be considered to prevent ischemic damage to the optic nerve and retina. However, the exact role in ARN is unknown. Many authors now consider routine antiplatelet or anticoagulant use as optional rather than the standard of care in the absence of other systemic indications. Aspirin may not prevent retinal detachment.[40]
Prophylactic barrier laser photocoagulation posterior to active retinitis may be considered to wall off the area and prevent subsequent retinal detachment. If applied, the laser should be placed behind the area of active retinitis in the apparently normal retina because a laser directly over the area of retinitis may cause an iatrogenic break. Prophylactic laser therapy may be difficult due to an inflamed, painful eye, poor pupillary dilation, and media haze. The use of prophylactic laser is controversial and is not always practiced because it might not prevent the development of retinal detachment in up to 58% of lasered eyes.[4]
Early prophylactic pars plana vitrectomy (before retinal detachment) has been attempted in patients with ARN. The retina was attached in 28 of 48 eyes (58.3%) in the (early) vitrectomy group and 42 of 56 eyes (75.0%) in the observation group at the final visit in a large series of 104 patients. The role of early pars plana vitrectomy before retinal detachment needs further evaluation, and there is no substantial evidence that it helps prevent retinal detachment.[41](B2)
Early vitreoretinal surgery for retinal detachment should be planned. The surgical procedure is difficult due to media haze, aggressive anterior segment inflammation, cataract, posterior synechia causing a poorly dilating pupil, and extensive vitreous membrane. Breaks are multiple and may be posterior. Proliferative vitreoretinopathy may be severe. Aggressive postoperative inflammation, including fibrinous reaction, may be noted. Despite retinal reattachment, optical atrophy and epiretinal membrane may limit visual gain. Proliferative vitreoretinopathy may lead to retinal redetachment after vitreoretinal surgery. In results from a series of 12 eyes from 10 patients with ARN and retinal detachment who underwent vitrectomy, all eyes had successful retinal reattachment at a mean final follow-up of 4.4 years.[42] A final visual acuity of better than 20/100 was achieved in only 3 eyes, and a lack of optic nerve involvement was associated with good visual outcomes.[42] Results from another study showed that specific surgical procedures (pars plana vitrectomy) were not independently associated with better final visual acuity when adjusted for baseline factors. In contrast, initial vision and retinal detachment were crucial prognostic factors for final vision.[28]
Differential Diagnosis
The differential diagnosis includes:
- CMV retinitis:
- Immunocompromised patients
- Clear media (minimal or no vitritis)
- Prominence of hemorrhage
- Early involvement of the posterior pole/arcades, and early involvement of the periphery in granular CMV retinitis
- Progressive outer retinal necrosis:
- Immunocompromised patient
- No vitritis
- Outer retinal involvement
- Posterior pole involved early
- Minimal retinal hemorrhage
- Paravascular clear area
- Syphilis:
- Granulomatous inflammation
- Posterior placoid chorioretinitis
- Retinal arterial involvement
- Round vitreous opacities
- Systemic features of syphilis, including palm and foot skin changes
- Toxoplasmosis:
- Intense vitritis
- Area of focal retinitis visible through vitritis as headlight in the fog
- Pigmented scar of old retinochoroiditis near the active area of retinitis; may not be present in some cases
- The features may be atypical with multiple lesions, less vitritis, and cerebral involvement in immunocompromised patients or those with AIDS.
- Behcet disease:
- Most patients have oral aphthous ulcers
- Skin and genital lesions
- Panuveitis
- Hypopyon
- Severe media haze or vitritis
- Vasculitis with few retinal hemorrhages
- Patches of retinitis
- HLA-B51 gene may be present
- Pathergy test results may be positive
- Fungal or bacterial endophthalmitis
- Pain, redness, eylid edema, and photophobia may be severe
- Hypopyon, corneal edema, corneal infection
- History of previous ocular surgery, intravenous drug infusion, or sepsis
- Discharge from the eye
- Severe visual decline, media haze, with echoes in the vitreous with or without choroidal thickening on ultrasonography
- Vitreous tap results positive for bacteria or fungus in stain or culture
- Panuveitis due to other causes
- Large cell lymphoma or intraocular lymphoma
- Older adults
- Vitreous opacity without cystoid macular edema
- Sheet-like vitreous on slit-lamp examination
- Ill-defined subretinal orange lesions
- History of behavioral change
- The vitreous biopsy may show lymphoma cells; the yield is typically low, and excellent collaboration with the pathologist is required
- An MRI of the brain may reveal central nervous system lymphoma
In ambiguous cases, PCR of ocular fluids and serology for Treponema pallidum and Toxoplasma gondii are critical to differentiate ARN from mimicking conditions.
Prognosis
The visual prognosis of ARN is poor, and 64% of affected eyes achieve a final acuity of worse than 20/200 due to multiple complications, including retinal detachment, optic neuropathy, macular abnormality, and retinal ischemia.[43] Visual outcomes may improve (up to 92% of eyes achieve at least 20/400, and 46% achieve a final vision of at least 20/40), and involvement of the fellow eye may be reduced with prompt diagnosis and early treatment.[44] Results from a large series reported that zone 1 disease and optic disc involvement were associated with a final vision of 20/200 or worse.[41] Visual outcomes in acute retinal necrosis (ARN) remain guarded, with findings from a recent multicenter series and registry data showing that a substantial proportion of affected eyes still have severe visual loss despite contemporary management.[28][45][46] Nevertheless, timely diagnosis and intensive systemic and local antiviral therapy can enable approximately half of treated eyes to achieve a final acuity of 20/200 or better, with a meaningful subset recovering to 20/40 or better, particularly when the disease is detected before macular or optic nerve involvement.[28][45][46][47][46] Findings from recent prognostic studies have clarified that baseline clinical status, rather than the specific treatment combination, largely determines visual outcome in ARN.[8][48] Worse initial visual acuity, retinal detachment at presentation or developing during follow-up, more extensive retinal necrosis (often defined as involvement of 3 or more quadrants or > 50% to 75% of retina), intraocular viral load, and macular or optic disc involvement are consistently linked to poor final vision in multivariable models.[8][48][8][49] In contrast, after adjustment for these baseline factors, individual therapeutic choices—such as the specific systemic antiviral regimen, use of prophylactic barrier laser, or performance of early vitrectomy—have not shown strong, independent associations with long-term visual acuity in several recent cohorts and large database studies.[45][50] Both a 2022 outcome series and more recent 2023–2025 analyses emphasize that prophylactic barrier laser has not demonstrated a clear, independent protective effect against retinal detachment or poor visual acuity when confounders such as extent of retinitis and vitreous clarity are taken into account.[28][46][48][46][50] Similarly, large registry data suggest that differing systemic antiviral regimens and adjunctive procedures result in broadly comparable median visual outcomes at 6 to 12 months, underscoring that baseline visual acuity and the occurrence of retinal detachment remain the dominant determinants of prognosis and should be central to risk stratification and patient counseling.[9][45][47][9][48][50]
Complications
Acute retinal necrosis is associated with a broad spectrum of sight-threatening complications involving both the posterior and anterior segments.[1] Rhegmatogenous retinal detachment is the most frequent and visually devastating complication, which develops in roughly 25% to 75% of affected eyes and often arises from atrophic or tractional retinal breaks at the junction between necrotic and uninvolved retina, frequently accompanied by early, aggressive proliferative vitreoretinopathy and vitreous traction.[51] Eyes with ARN may also develop exudative or mixed-mechanism retinal detachment due to severe occlusive vasculitis, breakdown of the blood–retinal barrier, and intense choroidal and retinal inflammation.[24] Optic neuropathy and optic atrophy are common late sequelae, reflecting ischemic or inflammatory damage to the nerve head and often contribute to poor final visual acuity despite successful retinal reattachment.[52] Retinal ischemia from necrotizing retinitis and occlusive vasculitis can be extensive and may drive downstream complications such as neovascularization and vitreous hemorrhage.[53][54] Ischemia-driven retinal and optic disc neovascularization in chronic retinal necrosis (usually due to CMV) can lead to vitreous hemorrhage and, in severe cases, neovascular glaucoma, often requiring panretinal photocoagulation and anti–vascular endothelial growth factor therapy in addition to a surgical procedure.[55][56] Fibrocellular proliferation on the macular and peripheral retinal surfaces can lead to epiretinal membrane formation, further distorting the macula and limiting visual recovery even after the acute phase resolves. Cystoid macular edema is a recognized, though relatively uncommon, late complication of ARN, often associated with persistent low-grade inflammation and diffuse capillary leakage on fluorescein angiography after complex retinal detachment repair.[57] Dexamethasone implants have been successfully used in cases of cystoid macular edema.[58] However, dexamethasone implants should be administered under antiviral therapy, because the infection can reactivate after an intravitreal dexamethasone implant.[59] A case report noted activation of ARN in a patient with a history of herpetic encephalitis who received 2 dexamethasone implants for macular edema due to retinal venous occlusion.[60] Many eyes with ARN show a mottled or pigmentary retinopathy in previously necrotic areas after healing, reflecting damage to the retinal pigment epithelium and outer retina.[61] Chronic intraocular inflammation and surgical intervention predispose to cataract formation—often with posterior synechiae—and to secondary angle-closure, making cataract surgical procedures in these eyes technically challenging. Inflammatory and corticosteroid-related mechanisms also contribute to secondary glaucoma, which may be further intensified by pupillary block, peripheral anterior synechiae, or silicone oil tamponade after retinal detachment surgery. Persistent vitreous haze is common in the active phase and may persist despite antiviral therapy, reflecting ongoing inflammatory activity and contributing to visual blur and diagnostic difficulty. Long-term outcome studies of vitrectomy for ARN-related rhegmatogenous retinal detachment consistently show high rates of anatomic reattachment with contemporary techniques. However, the final vision is frequently limited by optic atrophy, macular scarring, and recurrent detachments driven by aggressive proliferative vitreoretinopathy.[42][62]
Enhancing Healthcare Team Outcomes
The diagnosis and management of ARN are complex, and a prompt diagnosis is essential to preserve vision. Clinicians should immediately refer patients with herpes simplex infection of the eye to an ophthalmologist. Immediate treatment is required and can be performed in either the inpatient or outpatient setting. The goal is to reduce the incidence of fellow-eye involvement. The involvement of emergency clinicians, primary care clinicians, infectious disease specialists, and retina and uveitis subspecialists in structured care pathways is encouraged, particularly in patients with systemic immunosuppression or central nervous system involvement. There is also an increased focus on long-term follow-up and maintenance of oral antivirals to reduce fellow-eye involvement and recurrences, which can be emphasized when discussing care coordination and patient counseling.[1]
Media
(Click Image to Enlarge)
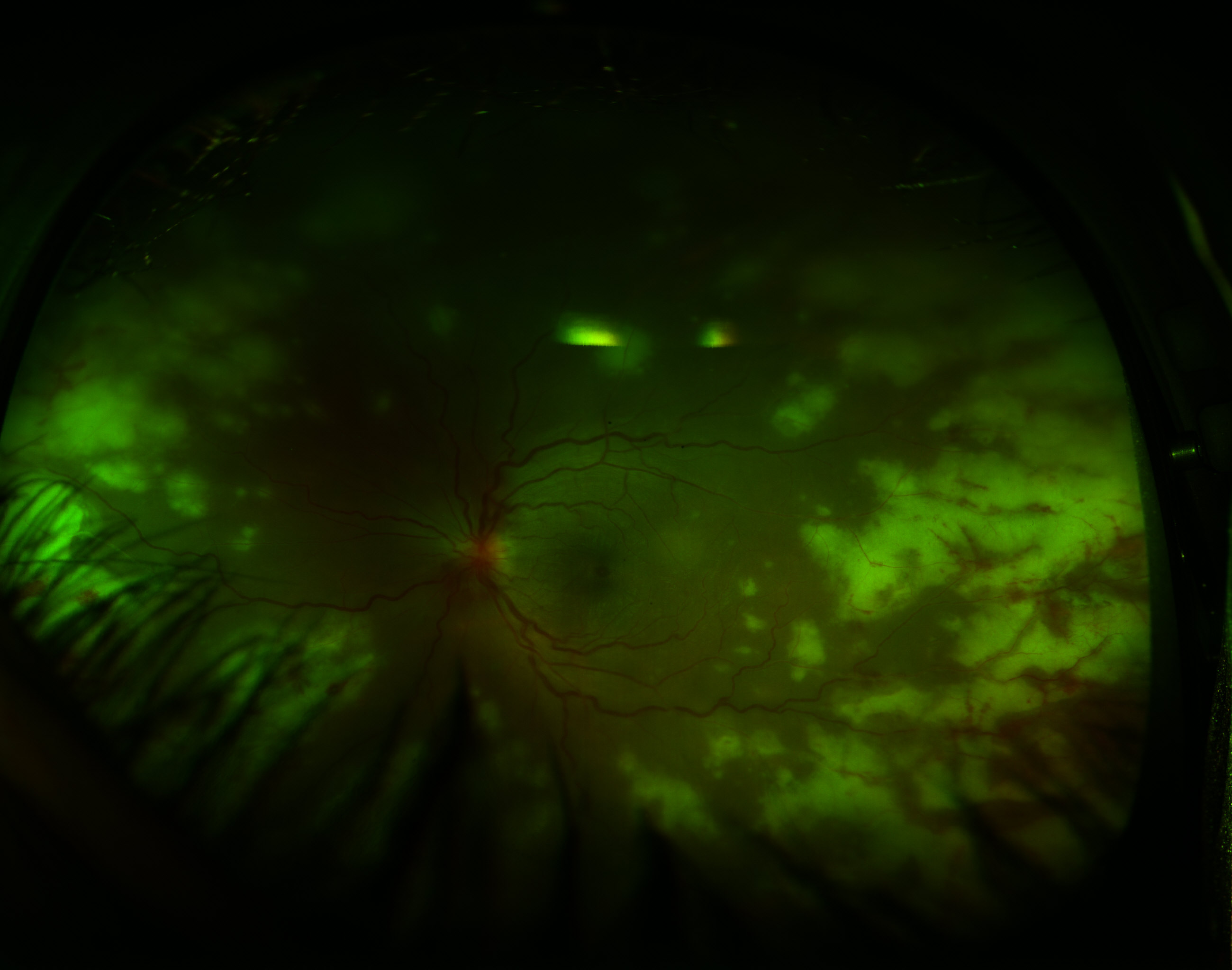
Acute Retinal Necrosis. Retinitis is demonstrated by the peripheral whitish retinal lesions. Typical additional findings include vitreous involvement and a paucity of hemorrhages, as opposed to cytomegalovirus retinitis, which presents with no vitreous involvement and a prominence of hemorrhages.
Contributed by K Tripathy, MD
References
Hoogewoud F, Rossi DC, Stappler T, Guex-Crosier Y. Acute retinal necrosis: A mini review. Frontiers in ophthalmology. 2022:2():916113. doi: 10.3389/fopht.2022.916113. Epub 2022 Aug 22 [PubMed PMID: 38983554]
Butler NJ, Moradi A, Salek SS, Burkholder BM, Leung TG, Dunn JP, Thorne JE. Acute Retinal Necrosis: Presenting Characteristics and Clinical Outcomes in a Cohort of Polymerase Chain Reaction-Positive Patients. American journal of ophthalmology. 2017 Jul:179():179-189. doi: 10.1016/j.ajo.2017.05.006. Epub 2017 May 10 [PubMed PMID: 28501392]
Level 2 (mid-level) evidenceDuker JS, Blumenkranz MS. Diagnosis and management of the acute retinal necrosis (ARN) syndrome. Survey of ophthalmology. 1991 Mar-Apr:35(5):327-43 [PubMed PMID: 2038718]
Level 3 (low-level) evidenceSchoenberger SD, Kim SJ, Thorne JE, Mruthyunjaya P, Yeh S, Bakri SJ, Ehlers JP. Diagnosis and Treatment of Acute Retinal Necrosis: A Report by the American Academy of Ophthalmology. Ophthalmology. 2017 Mar:124(3):382-392. doi: 10.1016/j.ophtha.2016.11.007. Epub 2017 Jan 13 [PubMed PMID: 28094044]
Guex-Crosier Y, Rochat C, Herbort CP. Necrotizing herpetic retinopathies. A spectrum of herpes virus-induced diseases determined by the immune state of the host. Ocular immunology and inflammation. 1997 Dec:5(4):259-65 [PubMed PMID: 9455742]
Level 3 (low-level) evidencePalay DA, Sternberg P Jr, Davis J, Lewis H, Holland GN, Mieler WF, Jabs DA, Drews C. Decrease in the risk of bilateral acute retinal necrosis by acyclovir therapy. American journal of ophthalmology. 1991 Sep 15:112(3):250-5 [PubMed PMID: 1882936]
Blumenkranz MS, Culbertson WW, Clarkson JG, Dix R. Treatment of the acute retinal necrosis syndrome with intravenous acyclovir. Ophthalmology. 1986 Mar:93(3):296-300 [PubMed PMID: 3703498]
Li Y, Chen L, Li P, Kang H, Tao Y. Risk factors and prognostic factors associated with retinal detachment and visual outcomes in acute retinal necrosis. BMC ophthalmology. 2024 Sep 15:24(1):296. doi: 10.1186/s12886-024-03533-3. Epub 2024 Sep 15 [PubMed PMID: 39277752]
Anthony CL, Bavinger JC, Yeh S. Advances in the Diagnosis and Management of Acute Retinal Necrosis. Annals of eye science. 2020 Sep:5():. pii: 28. doi: 10.21037/aes-2019-dmu-09. Epub 2020 Sep 15 [PubMed PMID: 33381683]
Level 3 (low-level) evidenceHolland GN. Standard diagnostic criteria for the acute retinal necrosis syndrome. Executive Committee of the American Uveitis Society. American journal of ophthalmology. 1994 May 15:117(5):663-7 [PubMed PMID: 8172275]
Level 1 (high-level) evidenceSugita S, Takase H, Nakano S. Role of Recent PCR Tests for Infectious Ocular Diseases: From Laboratory-Based Studies to the Clinic. International journal of molecular sciences. 2023 May 2:24(9):. doi: 10.3390/ijms24098146. Epub 2023 May 2 [PubMed PMID: 37175854]
Wong R, Pavesio CE, Laidlaw DA, Williamson TH, Graham EM, Stanford MR. Acute retinal necrosis: the effects of intravitreal foscarnet and virus type on outcome. Ophthalmology. 2010 Mar:117(3):556-60. doi: 10.1016/j.ophtha.2009.08.003. Epub 2009 Dec 23 [PubMed PMID: 20031221]
Ganatra JB, Chandler D, Santos C, Kuppermann B, Margolis TP. Viral causes of the acute retinal necrosis syndrome. American journal of ophthalmology. 2000 Feb:129(2):166-72 [PubMed PMID: 10682968]
Cochrane TF, Silvestri G, McDowell C, Foot B, McAvoy CE. Acute retinal necrosis in the United Kingdom: results of a prospective surveillance study. Eye (London, England). 2012 Mar:26(3):370-7; quiz 378. doi: 10.1038/eye.2011.338. Epub 2012 Jan 27 [PubMed PMID: 22281865]
Tran TH, Stanescu D, Caspers-Velu L, Rozenberg F, Liesnard C, Gaudric A, Lehoang P, Bodaghi B. Clinical characteristics of acute HSV-2 retinal necrosis. American journal of ophthalmology. 2004 May:137(5):872-9 [PubMed PMID: 15126152]
Silva RA, Berrocal AM, Moshfeghi DM, Blumenkranz MS, Sanislo S, Davis JL. Herpes simplex virus type 2 mediated acute retinal necrosis in a pediatric population: case series and review. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2013 Feb:251(2):559-66. doi: 10.1007/s00417-012-2164-8. Epub 2012 Oct 5 [PubMed PMID: 23052715]
Level 2 (mid-level) evidenceHolland GN, Cornell PJ, Park MS, Barbetti A, Yuge J, Kreiger AE, Kaplan HJ, Pepose JS, Heckenlively JR, Culbertson WW. An association between acute retinal necrosis syndrome and HLA-DQw7 and phenotype Bw62, DR4. American journal of ophthalmology. 1989 Oct 15:108(4):370-4 [PubMed PMID: 2801857]
Gartry DS, Spalton DJ, Tilzey A, Hykin PG. Acute retinal necrosis syndrome. The British journal of ophthalmology. 1991 May:75(5):292-7 [PubMed PMID: 1645179]
Level 3 (low-level) evidenceClarkson JG, Blumenkranz MS, Culbertson WW, Flynn HW Jr, Lewis ML. Retinal detachment following the acute retinal necrosis syndrome. Ophthalmology. 1984 Dec:91(12):1665-8 [PubMed PMID: 6151638]
Kang H, Wei Y, Liu M, Yu D, Tao Y. Flow cytometric analysis of T lymphocytes and cytokines in aqueous humor of patients with varicella zoster virus-mediated acute retinal necrosis. BMC ophthalmology. 2021 May 1:21(1):193. doi: 10.1186/s12886-021-01951-1. Epub 2021 May 1 [PubMed PMID: 33933004]
Zhang P, Liu S, Wang Z, Zhou M, Jiang R, Xu G, Chang Q. Immune Cell Status and Cytokines Profiles in Patients with Acute Retinal Necrosis. Ocular immunology and inflammation. 2021 Nov 17:29(7-8):1452-1458. doi: 10.1080/09273948.2020.1734214. Epub 2020 Mar 11 [PubMed PMID: 32160075]
Culbertson WW, Blumenkranz MS, Haines H, Gass DM, Mitchell KB, Norton EW. The acute retinal necrosis syndrome. Part 2: Histopathology and etiology. Ophthalmology. 1982 Dec:89(12):1317-25 [PubMed PMID: 6298683]
Level 3 (low-level) evidenceRungger-Brändle E, Roux L, Leuenberger PM. Bilateral acute retinal necrosis (BARN). Identification of the presumed infectious agent. Ophthalmology. 1984 Dec:91(12):1648-58 [PubMed PMID: 6097853]
Perhiar BA, Siddiqui MR, Ibrahim S. Acute retinal necrosis with exudative retinal detachment in a child. BMJ case reports. 2021 Dec 15:14(12):. doi: 10.1136/bcr-2021-245984. Epub 2021 Dec 15 [PubMed PMID: 34911728]
Level 3 (low-level) evidenceKalogeropoulos D, Afshar F, Kalogeropoulos C, Vartholomatos G, Lotery AJ. Diagnostic and therapeutic challenges in acute retinal necrosis; an update. Eye (London, England). 2024 Jul:38(10):1816-1826. doi: 10.1038/s41433-024-03028-x. Epub 2024 Mar 22 [PubMed PMID: 38519714]
Lewis ML, Culbertson WW, Post JD, Miller D, Kokame GT, Dix RD. Herpes simplex virus type 1. A cause of the acute retinal necrosis syndrome. Ophthalmology. 1989 Jun:96(6):875-8 [PubMed PMID: 2544841]
Chawla R, Tripathy K, Sharma YR, Venkatesh P, Vohra R. Periarterial Plaques (Kyrieleis' Arteriolitis) in a Case of Bilateral Acute Retinal Necrosis. Seminars in ophthalmology. 2017:32(2):251-252. doi: 10.3109/08820538.2015.1045153. Epub 2015 Jul 10 [PubMed PMID: 26161821]
Level 3 (low-level) evidenceShiezadeh E, Hosseini SM, Bakhtiari E, Mojarrad A, Motamed Shariati M. Clinical characteristics and management outcomes of acute retinal necrosis. Scientific reports. 2023 Oct 7:13(1):16927. doi: 10.1038/s41598-023-44310-4. Epub 2023 Oct 7 [PubMed PMID: 37805622]
Ben-Avi R, Amer R. Posterior pole involvement as the presenting feature of varicella zoster virus- associated acute retinal necrosis in a young healthy man. Journal of ophthalmic inflammation and infection. 2025 Nov 21:15(1):88. doi: 10.1186/s12348-025-00540-3. Epub 2025 Nov 21 [PubMed PMID: 41269439]
Tripathy K, Sharma YR, Chawla R, Basu K, Vohra R, Venkatesh P. Triads in Ophthalmology: A Comprehensive Review. Seminars in ophthalmology. 2017:32(2):237-250. doi: 10.3109/08820538.2015.1045150. Epub 2015 Jul 6 [PubMed PMID: 26148300]
Holland GN, Buhles WC Jr, Mastre B, Kaplan HJ. A controlled retrospective study of ganciclovir treatment for cytomegalovirus retinopathy. Use of a standardized system for the assessment of disease outcome. UCLA CMV Retinopathy. Study Group. Archives of ophthalmology (Chicago, Ill. : 1960). 1989 Dec:107(12):1759-66 [PubMed PMID: 2556989]
Level 2 (mid-level) evidenceFreeman WR, Wiley CA, Gross JG, Thomas EL, Rao NA, Liggett PE. Endoretinal biopsy in immunosuppressed and healthy patients with retinitis. Indications, utility, and techniques. Ophthalmology. 1989 Oct:96(10):1559-65 [PubMed PMID: 2587052]
Tripathy K, Sharma YR, Gogia V, Venkatesh P, Singh SK, Vohra R. Serial ultra wide field imaging for following up acute retinal necrosis cases. Oman journal of ophthalmology. 2015 Jan-Apr:8(1):71-2. doi: 10.4103/0974-620X.149896. Epub [PubMed PMID: 25709284]
Level 3 (low-level) evidenceTripathy K, Chawla R, Venkatesh P, Sharma YR, Vohra R. Ultrawide Field Imaging in Uveitic Non-dilating Pupils. Journal of ophthalmic & vision research. 2017 Apr-Jun:12(2):232-233. doi: 10.4103/2008-322X.205360. Epub [PubMed PMID: 28540019]
Farrell TA, Wolf MD, Folk JC, Pulido JS, Yuh WT. Magnetic resonance imaging in a patient with herpes zoster keratouveitis and contralateral acute retinal necrosis. American journal of ophthalmology. 1991 Dec 15:112(6):735-6 [PubMed PMID: 1957917]
Tam PM, Hooper CY, Lightman S. Antiviral selection in the management of acute retinal necrosis. Clinical ophthalmology (Auckland, N.Z.). 2010 Feb 2:4():11-20 [PubMed PMID: 20169044]
Lains I, Eliott D. Challenges and Updates on the Management of Acute Retinal Necrosis. International ophthalmology clinics. 2022 Apr 1:62(2):173-196. doi: 10.1097/IIO.0000000000000415. Epub [PubMed PMID: 35325918]
Putera I, Ridwan AS, Dewi M, Cifuentes-González C, Rojas-Carabali W, Sitompul R, Edwar L, Susiyanti M, Aziza Y, Pavesio C, Chee SP, Mahendradas P, Biswas J, Kempen JH, Gupta V, de-la-Torre A, La Distia Nora R, Agrawal R. Antiviral treatment for acute retinal necrosis: A systematic review and meta-analysis. Survey of ophthalmology. 2024 Jan-Feb:69(1):67-84. doi: 10.1016/j.survophthal.2023.09.004. Epub 2023 Sep 27 [PubMed PMID: 37774799]
Level 1 (high-level) evidenceDebiec MR, Lindeke-Myers AT, Shantha JG, Bergstrom CS, Hubbard GB 3rd, Yeh S. Outcomes of Combination Systemic and Intravitreal Antiviral Therapy for Acute Retinal Necrosis. Ophthalmology. Retina. 2021 Mar:5(3):292-300. doi: 10.1016/j.oret.2020.07.012. Epub 2020 Jul 16 [PubMed PMID: 32683108]
Ando F, Kato M, Goto S, Kobayashi K, Ichikawa H, Kamiya T. Platelet function in bilateral acute retinal necrosis. American journal of ophthalmology. 1983 Jul:96(1):27-32 [PubMed PMID: 6869477]
Iwahashi-Shima C, Azumi A, Ohguro N, Okada AA, Kaburaki T, Goto H, Sonoda KH, Namba K, Mizuki N, Mochizuki M. Acute retinal necrosis: factors associated with anatomic and visual outcomes. Japanese journal of ophthalmology. 2013 Jan:57(1):98-103. doi: 10.1007/s10384-012-0211-y. Epub 2012 Nov 2 [PubMed PMID: 23117419]
Level 2 (mid-level) evidenceAlmeida DR, Chin EK, Tarantola RM, Tegins EO, Lopez CA, Boldt HC, Gehrs KM, Sohn EH, Russell SR, Folk JC, Mahajan VB. Long-term outcomes in patients undergoing vitrectomy for retinal detachment due to viral retinitis. Clinical ophthalmology (Auckland, N.Z.). 2015:9():1307-14. doi: 10.2147/OPTH.S87644. Epub 2015 Jul 16 [PubMed PMID: 26229423]
Fisher JP, Lewis ML, Blumenkranz M, Culbertson WW, Flynn HW Jr, Clarkson JG, Gass JD, Norton EW. The acute retinal necrosis syndrome. Part 1: Clinical manifestations. Ophthalmology. 1982 Dec:89(12):1309-16 [PubMed PMID: 7162777]
Level 3 (low-level) evidenceCrapotta JA, Freeman WR, Feldman RM, Lowder CY, Ambler JS, Parker CE, Meisler DM. Visual outcome in acute retinal necrosis. Retina (Philadelphia, Pa.). 1993:13(3):208-13 [PubMed PMID: 8235101]
Lains I, Ivanov A, Ross C, Hall N, Elze T, Lorch A, Miller JW, Sobrin L, Gong D, IRIS® Registry Data Analytic Center Consortium. Treatment Regimen and Outcomes in Acute Retinal Necrosis: An IRIS® Registry Study. Ophthalmology. 2024 Dec:131(12):1468-1470. doi: 10.1016/j.ophtha.2024.07.020. Epub 2024 Jul 20 [PubMed PMID: 39033858]
Mojarrad A, Omidtabrizi A, Ansari Astaneh M, Bakhtiari E, Shiezadeh E, Hassani M, Hosseini SM. Acute retinal necrosis. Management and visual outcomes: a case series. International journal of retina and vitreous. 2022 Sep 15:8(1):66. doi: 10.1186/s40942-022-00417-w. Epub 2022 Sep 15 [PubMed PMID: 36109794]
Level 2 (mid-level) evidenceMooss VS, Murthy KR, Babu K, Tirumalai AA. Clinical profile and treatment outcomes in acute retinal necrosis in a South Indian patient population. Indian journal of ophthalmology. 2025 Jun 1:73(6):858-863. doi: 10.4103/IJO.IJO_1585_24. Epub 2025 Apr 17 [PubMed PMID: 40244572]
Chambonnet M, Labalette P. [Prognostic factors for acute retinal necrosis: Retrospective analysis of a series of 37 immunocompetent patients]. Journal francais d'ophtalmologie. 2025 Dec:48(10):104261. doi: 10.1016/j.jfo.2024.104261. Epub 2025 Dec 2 [PubMed PMID: 41337953]
Level 2 (mid-level) evidenceAksu-Ceylan N, Güner ME, Cebeci Z, Altınkurt E, Kır N, Oray M, Tugal-Tutkun İ. Association Between Prognosis of Acute Retinal Necrosis and Retinal Involvement. Turkish journal of ophthalmology. 2022 Dec 28:52(6):405-411. doi: 10.4274/tjo.galenos.2021.58609. Epub [PubMed PMID: 36578219]
Bavinger JC, Anthony CL, Lindeke-Myers AT, Lynch S, Xu LT, Barnett J, Levine D, Patel P, Shah R, Jain N, Rao P, Hendrick A, Cribbs BE, Yan J, Hubbard GB 3rd, Shantha JG, O'Keefe GD, Yeh S. Risk Factors for Retinal Detachment in Acute Retinal Necrosis. Ophthalmology. Retina. 2022 Jun:6(6):478-483. doi: 10.1016/j.oret.2022.01.016. Epub 2022 Feb 1 [PubMed PMID: 35114414]
Nasir S, Mehfooz S, Basu S, Pappuru RR, Tyagi M. Clinical features and outcomes of Rhegmatogenous Retinal Detachments in Acute Retinal Necrosis. Taiwan journal of ophthalmology. 2025 Apr-Jun:15(2):277-282. doi: 10.4103/tjo.TJO-D-25-00012. Epub 2025 Jun 3 [PubMed PMID: 40584203]
Witmer MT, Pavan PR, Fouraker BD, Levy-Clarke GA. Acute retinal necrosis associated optic neuropathy. Acta ophthalmologica. 2011 Nov:89(7):599-607. doi: 10.1111/j.1755-3768.2010.01911.x. Epub 2010 Jul 20 [PubMed PMID: 20645925]
Mayer CS, Blobner K, Storr J, Baur ID, Khoramnia R. Acute Retinal Necrosis: Signs, Treatment, Complications and Outcome. Diagnostics (Basel, Switzerland). 2022 Feb 2:12(2):. doi: 10.3390/diagnostics12020386. Epub 2022 Feb 2 [PubMed PMID: 35204477]
Wang CL, Kaplan HJ, Waldrep JC, Pulliam M. Retinal neovascularization associated with acute retinal necrosis. Retina (Philadelphia, Pa.). 1983 Fall-Winter:3(4):249-52 [PubMed PMID: 6201970]
Matsuoka T, Asao K, Hashida N, Nishida K. Chronic Retinal Necrosis Severely Complicated by Neovascular Glaucoma: A Case Report. Case reports in ophthalmology. 2017 Sep-Dec:8(3):489-495. doi: 10.1159/000480724. Epub 2017 Oct 26 [PubMed PMID: 29282399]
Level 3 (low-level) evidenceSchneider EW, Elner SG, van Kuijk FJ, Goldberg N, Lieberman RM, Eliott D, Johnson MW. Chronic retinal necrosis: cytomegalovirus necrotizing retinitis associated with panretinal vasculopathy in non-HIV patients. Retina (Philadelphia, Pa.). 2013 Oct:33(9):1791-9. doi: 10.1097/IAE.0b013e318285f486. Epub [PubMed PMID: 23584702]
Rana V, Markan A, Arora A, Tripathi M, Mahendradas P, Sharma V, Roodkee U, Kumar S, Goenka R. Cystoid Macular Edema Secondary to Acute Retinal Necrosis: The Role of Fundus Fluorescein Angiography in Guiding Treatment. Cureus. 2025 Nov:17(11):e96108. doi: 10.7759/cureus.96108. Epub 2025 Nov 4 [PubMed PMID: 41221412]
Sørland RØ, Erichsen AK, Jonsdottir TE, Bromnes MN, Lauritzen PM, Eidet JR. Successful treatment with repeated dexamethasone implant injections for recurrent macular edema after acute retinal necrosis. Journal of ophthalmic inflammation and infection. 2022 Oct 21:12(1):33. doi: 10.1186/s12348-022-00310-5. Epub 2022 Oct 21 [PubMed PMID: 36269441]
Majumder PD, Biswas J, Ambreen A, Amin R, Pannu ZR, Bedda AM. Intravitreal dexamethasone implant for the treatment of cystoid macular oedema associated with acute retinal necrosis. Journal of ophthalmic inflammation and infection. 2016 Dec:6(1):49. doi: 10.1186/s12348-016-0116-x. Epub 2016 Dec 23 [PubMed PMID: 28012104]
Zhang ZY, Liu XY, Jiang T. Acute retinal necrosis following dexamethasone intravitreal implant (Ozurdex®) administration in an immunocompetent adult with a history of HSV encephalitis: a case report. BMC ophthalmology. 2020 Jun 22:20(1):247. doi: 10.1186/s12886-020-01514-w. Epub 2020 Jun 22 [PubMed PMID: 32571253]
Level 3 (low-level) evidenceKeorochana N, Suleesathira B, Vongkulsiri S. Pigmentary retinopathy and nodular granuloma associated with acute retinal necrosis from varicella zoster virus and human herpes virus type 6: Case report. Medicine. 2023 Jun 30:102(26):e33958. doi: 10.1097/MD.0000000000033958. Epub [PubMed PMID: 37390266]
Level 3 (low-level) evidenceIannetti L, Visioli G, Alisi L, Armentano M, Pirraglia MP, Accorinti M, Di Martino V, Gharbiya M. Long-Term Functional Outcomes of Retinal Detachment Due to Acute Retinal Necrosis: A Case Series. Biomedicines. 2024 Oct 11:12(10):. doi: 10.3390/biomedicines12102320. Epub 2024 Oct 11 [PubMed PMID: 39457631]
Level 2 (mid-level) evidence