 Blepharoptosis (Ptosis): Classification, Evaluation, and Surgical Management
Blepharoptosis (Ptosis): Classification, Evaluation, and Surgical Management
Introduction
Blepharoptosis, derived from the Greek term meaning “falling,” refers specifically to abnormal drooping of the upper eyelid in the primary position of gaze. This condition carries significant functional, aesthetic, and psychosocial implications despite its seemingly localized nature. The position of the upper eyelid plays a critical role in ocular surface protection, maintenance of corneal hydration through effective blinking, and preservation of an unobstructed visual axis. Even subtle deviations in eyelid height can impair superior visual fields, contribute to ocular fatigue, and alter perceived age and facial identity. Eyelid position, in conjunction with brow architecture and palpebral fissure shape, represents a fundamental component of human facial recognition, reinforcing the importance of precise diagnosis and management.
Ptosis represents a clinical sign rather than a definitive diagnosis, reflecting a broad spectrum of underlying etiologies.[1] Presentation spans all age groups and may be congenital or acquired, unilateral or bilateral, and either isolated or associated with systemic disease. A comprehensive understanding of blepharoptosis requires integration of eyelid anatomy, neuromuscular physiology, and pathologic mechanisms.
The upper eyelid consists of a complex multilayered structure, including skin, orbicularis oculi muscle, orbital septum, preaponeurotic fat, tarsal plate, levator palpebrae superioris muscle, the Müller muscle, and conjunctiva. Eyelid elevation depends primarily on the levator palpebrae superioris, innervated by the superior division of cranial nerve III, with secondary contribution from the Müller muscle under sympathetic control. Disruption at any point along this functional pathway, whether myogenic, neurogenic, aponeurotic, mechanical, or traumatic, can result in ptosis.[2]
Patients commonly report eyelid drooping, visual obstruction, a sensation of heaviness, or cosmetic concerns (see Image. Ptosis). Clinical evaluation must extend beyond surface findings to identify potentially vision- or life-threatening causes. A detailed history should address onset, variability, laterality, associated diplopia or anisocoria, prior surgical or traumatic events, and relevant systemic conditions.
Acute onset ptosis accompanied by headache, pupillary abnormalities, or extraocular motility deficits raises concern for compressive oculomotor nerve palsy, often secondary to an aneurysm, and necessitates urgent neurovascular imaging.[3] Fluctuating or fatigable ptosis with diurnal variation suggests ocular myasthenia gravis and requires targeted diagnostic testing, including bedside maneuvers and serologic evaluation.[4] Additional etiologies include iatrogenic causes such as prior botulinum toxin injection, contact lens–associated levator dehiscence, and sequelae of intraocular or eyelid surgery. Pediatric presentations warrant particular attention due to the risk of amblyopia; evaluation should focus on compensatory head posturing, visual axis occlusion, and associated syndromic features, such as Horner syndrome or congenital cranial dysinnervation disorders.
This review provides a comprehensive, clinically oriented framework for the classification, evaluation, and surgical management of blepharoptosis. Emphasis is placed on systematic diagnostic algorithms, differentiation of etiologic subtypes, and evidence-based selection of surgical techniques tailored to underlying pathophysiology. A methodical and multidisciplinary approach remains essential to optimize functional and aesthetic outcomes in patients with ptosis.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The palpebral fissure, defined as the elliptical opening between the upper and lower eyelids, serves as the functional aperture through which light enters the eye and ocular protection is maintained (see Image. Normal Eyelids in a Caucasian Female). The contour of the upper eyelid demonstrates maximal curvature slightly nasal to the midpupillary line. This critical landmark should be identified and marked preoperatively to optimize cosmetic symmetry and surgical precision. In the normal resting position, the upper eyelid typically overlies the superior limbus by approximately 1 to 2 mm, while the lower eyelid rests at or just below the inferior limbus. Subtle deviations from these relationships may indicate underlying pathology and are essential considerations in both diagnostic evaluation and surgical planning.
The eyelid structure is defined by a highly specialized, multilayered architecture that integrates protective, functional, and aesthetic roles (see Image. Eyelid Landmarks and Aesthetic Units and Anatomy of the Upper Eyelid and Brow Complex).[5] The skin is the most superficial layer and the thinnest in the human body, allowing for high mobility and fine contouring; the attachment of the levator aponeurosis to the dermis creates the upper eyelid crease, an important surgical landmark. Deep to the skin lies the orbicularis oculi muscle, a circumferential sphincter composed of pretarsal, preseptal, and orbital segments, which facilitates both involuntary blinking and forceful eyelid closure. The orbital septum, a fibrous extension of periosteum, acts as a barrier between the orbital contents and the eyelid; superiorly, the septum inserts along the orbital rim and inferiorly blends with the levator aponeurosis near the superior tarsal border.[5] Surgical entry through the septum allows access to deeper structures, although careful dissection is required to avoid disruption of levator attachments and postoperative eyelid malposition.
Posterior to the septum lies the preaponeurotic fat pad. This key intraoperative landmark helps identify the levator complex, as the levator palpebrae superioris muscle resides immediately posterior to this fat compartment. The tarsal plate, composed of dense connective tissue, provides structural integrity to the eyelid and houses the Meibomian glands, which play a critical role in tear film stability. The upper tarsus measures approximately 10 to 12 mm in vertical height, whereas the lower tarsus measures 4 to 5 mm, differences that are relevant for surgical fixation and reconstruction.
The primary elevator of the upper eyelid, the levator palpebrae superioris, originates at the orbital apex from the lesser wing of the sphenoid and courses anteriorly beneath the orbital roof. At the level of the superior orbital rim, the muscle transitions from a horizontal to vertical orientation and forms the levator aponeurosis. The Whitnall ligament, located at this transition zone approximately 10 to 12 mm above the tarsal plate, functions as a suspensory pulley that redirects levator force.[6]
The levator aponeurosis exhibits multiple insertions: anterior fibers insert into the skin to form the eyelid crease, inferior fibers attach to the anterior surface of the superior tarsus, and posterior fibers extend toward the conjunctival fornix. Medial and lateral expansions, known as the horns of the levator, anchor to the medial and lateral canthal structures, contributing to eyelid contour and stability. Innervation is supplied by the superior division of the oculomotor nerve (cranial nerve III).
The Müller muscle, a sympathetically innervated smooth muscle arising from the undersurface of the levator aponeurosis near the Whitnall ligament, inserts along the superior border of the tarsus and contributes approximately 2 mm of additional eyelid elevation. Dysfunction of this muscle accounts for the subtle ptosis observed in conditions such as Horner syndrome. The conjunctiva forms the innermost layer of the eyelid, consisting of nonkeratinized stratified squamous epithelium that reflects onto the globe. Goblet cells within the conjunctiva secrete mucin, a critical component of the tear film necessary for ocular surface lubrication and stability. A detailed understanding of this layered anatomy and the interrelationship between structural and neuromuscular components remains fundamental for accurate classification of ptosis and for selecting appropriate surgical interventions that restore both function and aesthetic harmony.
Indications
Management of blepharoptosis requires a systematic, etiology-driven approach that integrates the underlying cause, severity of eyelid malposition, levator function, patient age, ocular surface status, and associated comorbidities. The primary goals of intervention include restoration of a functional palpebral fissure with adequate clearance of the visual axis, preservation of corneal integrity, and achievement of appropriate eyelid symmetry and contour. In congenital ptosis, prevention of amblyopia is the overriding priority, whereas in adult populations, both functional improvement and aesthetic restoration frequently guide decision-making. Most patients present seeking intervention for superior visual field obstruction, impaired peripheral vision, and a subjective sense of eyelid heaviness; however, cosmetic concerns, particularly the appearance of fatigue or asymmetry, account for a substantial proportion of indications for treatment.
Appropriate management begins with accurate classification. Ptosis may be categorized as true ptosis, resulting from intrinsic dysfunction of the eyelid elevator mechanism, or pseudoptosis, in which eyelid drooping is apparent but attributable to extrinsic factors such as dermatochalasis, brow ptosis, hypotropia, or globe abnormalities.[7][8] True ptosis is further subdivided by onset into congenital and acquired forms, and by etiology into aponeurotic, neurogenic, myogenic, mechanical, and traumatic categories.[9] This classification is essential, as each subtype carries distinct natural history, prognostic implications, and management strategies.
Observation remains appropriate in selected cases. Mild, nonprogressive ptosis without visual axis involvement may be monitored, particularly in pediatric patients with adequate visual development. Neurogenic ptosis due to microvascular third cranial nerve palsy often resolves spontaneously within 3 to 6 months, supporting delayed surgical intervention until neurologic stability is confirmed. Myogenic ptosis associated with ocular myasthenia gravis frequently improves with medical therapy, including acetylcholinesterase inhibitors, corticosteroids, and immunosuppressive agents, thereby making surgical correction unnecessary or inappropriate during the active disease phase.
Definitive indications for intervention include visual axis obstruction, development or risk of amblyopia, persistent superior visual field limitation, and compensatory mechanisms such as chin elevation or frontalis overactivity. Additional indications include stable ptosis following resolution of reversible causes, typically beyond 3 to 6 months in neurogenic and traumatic cases, as well as significant cosmetic deformity affecting quality of life. In traumatic ptosis, early surgical exploration is indicated in penetrating injuries with suspected levator disruption, whereas blunt trauma is initially managed conservatively due to the potential for spontaneous recovery; persistent dysfunction beyond 6 months generally warrants operative correction.[10]
Etiology-specific considerations play a central role in determining management. Aponeurotic ptosis, the most common form in adults, typically presents in the fifth to sixth decade and results from dehiscence, disinsertion, or attenuation of the levator aponeurosis.[11][12][13] Characteristic findings include preserved levator function, a high eyelid crease, and thinning of the upper eyelid with redundant skin, making these patients ideal candidates for levator advancement or aponeurotic repair.
Neurogenic ptosis arises from disruption of innervation to the levator palpebrae superioris or the Müller muscle and most commonly involves third cranial nerve palsy and Horner syndrome.[14] Third nerve palsy presents with ptosis and ophthalmoplegia, with pupillary involvement suggesting compressive etiologies such as a posterior communicating artery aneurysm, necessitating urgent evaluation.[15] Surgical correction in such cases must account for poor Bell phenomenon and risk of exposure keratopathy, often favoring staged management with initial strabismus correction followed by ptosis repair using frontalis suspension with planned undercorrection. Horner syndrome produces mild ptosis due to sympathetic denervation of the Müller muscle and is associated with miosis, anhidrosis, and, in congenital cases, iris heterochromia.[16][17][16]
Myogenic ptosis encompasses a heterogeneous group of disorders characterized by intrinsic muscle dysfunction and reduced levator function. Common etiologies include myasthenia gravis, myotonic dystrophy, chronic progressive external ophthalmoplegia (CPEO), and oculopharyngeal muscular dystrophy.[18][19][20][21][20] Myasthenia gravis presents with variable, fatigable ptosis, often accompanied by diplopia, with clinical features including worsening ptosis on sustained upward gaze and a Cogan lid twitch.[22]
Diagnosis is supported by bedside testing (eg, ice test), serologic assays, and electrophysiologic studies, with primary management focused on immunomodulatory therapy. Surgical correction may be considered in refractory cases, typically with undercorrection to mitigate the risk of exposure. Myotonic dystrophy presents with progressive ptosis, external ophthalmoplegia, and systemic features including facial muscle involvement, cataracts, and endocrine abnormalities.[19]
CPEO, a mitochondrial myopathy, produces bilateral symmetric ptosis and ophthalmoplegia with minimal diplopia due to symmetric involvement; associated syndromes such as Kearns-Sayre may include cardiac conduction abnormalities and multisystem disease.[20][23][24] Oculopharyngeal muscular dystrophy presents later in life with ptosis, dysphagia, and proximal muscle weakness.[21] Surgical intervention in myogenic ptosis must be approached cautiously due to poor levator function and high risk of postoperative exposure keratopathy.
Mechanical ptosis results from increased eyelid weight or from structural restriction that prevents normal elevation. Causes include eyelid or orbital tumors, dermatochalasis, cicatricial changes from trauma or inflammation, and edema due to allergic or infectious processes.[25] Pediatric etiologies may include capillary hemangiomas or neurofibromas, whereas adult causes include sebaceous gland carcinoma and thyroid-associated orbitopathy.[26][27] Management requires treatment of the underlying pathology before or in conjunction with eyelid surgery.
Traumatic ptosis arises from direct injury to the levator muscle, its aponeurosis, or neural supply.[10] Penetrating injuries often necessitate early surgical repair to restore anatomy and prevent fibrosis, whereas blunt trauma is typically managed conservatively with serial reassessment due to the potential for spontaneous recovery. Chronic, stable ptosis following trauma represents an indication for surgical correction tailored to residual levator function.
Pseudoptosis must be carefully distinguished from true ptosis, as management differs fundamentally. Apparent eyelid drooping may result from dermatochalasis, brow ptosis, ocular misalignment, enophthalmos, anophthalmos, or contralateral eyelid retraction.[28] Failure to recognize pseudoptosis can lead to inappropriate surgical intervention and suboptimal outcomes. Comprehensive evaluation, including assessment of brow position, extraocular motility, globe position, and margin reflex distance, is essential to ensure that treatment targets the underlying cause rather than its manifestation.
Clinical presentation further refines indications for evaluation and urgency of management. Patients commonly report eyelid drooping, visual obscuration, heaviness, and cosmetic concerns. Acute onset ptosis associated with headache, diplopia, anisocoria, or pain raises concern for compressive oculomotor nerve pathology and requires urgent neurovascular imaging.[3] Fluctuating ptosis with diurnal variation suggests ocular myasthenia gravis and necessitates targeted diagnostic evaluation, including bedside and serologic testing.[4] Additional history should include prior periocular procedures, botulinum toxin exposure, contact lens use, and systemic conditions such as thyroid or mitochondrial disease, as these factors may influence both diagnosis and management. A comprehensive, structured approach to indications ensures that management is appropriately timed, etiology-specific, and aligned with both functional and aesthetic goals, thereby optimizing patient outcomes while minimizing complications.
Contraindications
Contraindications to ptosis surgery center on identifying reversible, unstable, or misdiagnosed conditions in which operative intervention would be ineffective or harmful. Surgical decision-making must account for etiology, disease stability, ocular surface integrity, and patient-specific risk factors. Many cases of ptosis represent a symptom of an underlying disorder rather than an isolated structural problem, and failure to address the primary cause can lead to poor outcomes.
Active or untreated underlying disease is a key contraindication. Myogenic ptosis due to ocular myasthenia gravis should not be managed surgically during the active phase, as symptoms are variable and often improve with medical therapy, including pyridostigmine, corticosteroids, or other immunosuppressants.[29] Neurogenic ptosis from microvascular third nerve palsy frequently resolves within 3 to 6 months, warranting observation before surgery. Acute ptosis with pupillary involvement raises concern for compressive aneurysm and requires urgent neurovascular evaluation rather than surgical correction.[15] Similarly, mechanical ptosis due to inflammation, infection, edema, or thyroid-associated orbitopathy should be treated medically before surgery is considered.[27][25]
Ocular surface compromise represents a major relative contraindication. A poor Bell phenomenon, reduced corneal sensation, or significant dry eye increases the risk of postoperative exposure keratopathy, particularly in neurogenic and myogenic ptosis such as third nerve palsy or chronic progressive external ophthalmoplegia. In these patients, surgery, if performed, must be conservative, often with intentional undercorrection.
Unstable or evolving ptosis also precludes immediate intervention. Traumatic ptosis following blunt injury is typically observed initially, as edema, hematoma, or neuropraxia may resolve; surgery is reserved for stable deficits after several months. Early repair is limited to penetrating injuries with clear levator disruption. Progressive neuromuscular disorders, including myotonic dystrophy and oculopharyngeal muscular dystrophy, present additional challenges due to recurrence risk and limited durability of surgical outcomes.[19][21][20]
Misdiagnosis is a critical and preventable contraindication. Pseudoptosis due to dermatochalasis, brow ptosis, hypotropia, or globe abnormalities must be distinguished from true ptosis, as levator-based surgery alone will not address the underlying issue and may worsen outcomes.[28] Comprehensive evaluation, including brow position, ocular alignment, and margin reflex distance, is essential. Additional relative contraindications include uncontrolled systemic disease, poor surgical candidacy, and inability to comply with postoperative care. Overall, appropriate patient selection, grounded in etiology, stability, and ocular surface assessment, is essential to avoid complications and ensure that surgical intervention provides meaningful functional and aesthetic benefit.
Equipment
A basic oculoplastic surgery instrument set, local anesthetic containing epinephrine, a skin marking pen, and a measuring scale are all that is needed to perform a successful ptosis surgery.
Preparation
A thorough preoperative evaluation, including a detailed history and meticulous clinical investigation, helps improve the success of ptosis surgery.
Preoperative Evaluation and Clinical Assessment
A thorough preoperative evaluation is fundamental to optimizing surgical outcomes in ptosis repair and begins with the initial patient assessment. Subtle findings such as facial asymmetry, frontalis overaction, chin elevation, or abnormal head posture may indicate compensatory mechanisms and provide insight into severity and chronicity. Standardized eyelid measurements are essential and should be performed with the patient in primary gaze, the brow immobilized, and the examiner at eye level to avoid parallax error. Key parameters include marginal reflex distance 1 (MRD1), marginal reflex distance 2 (MRD2), palpebral fissure height (PFH), levator function, and margin crease distance (MCD).
PFH represents the vertical distance between the upper and lower eyelid margins measured in the pupillary plane with the eyes in primary gaze, with a normal value of approximately 10 mm. MRD1 is defined as the distance from the corneal light reflex to the upper eyelid margin and normally measures 4 to 5 mm; comparison between eyes is particularly important in unilateral ptosis, as a difference of 2 mm indicates mild ptosis, 3 mm moderate ptosis, and 4 mm severe ptosis. MRD2, measured from the corneal light reflex to the lower eyelid margin, complements MRD1, with the sum of MRD1 and MRD2 equaling the PFH under normal conditions.
Levator function, assessed as the excursion of the upper eyelid from maximal downgaze to maximal upgaze with the frontalis muscle immobilized, is the most critical measurement in ptosis evaluation because it directly determines the surgical approach. Normal levator excursion exceeds 15 mm, and function is graded as poor (<4 mm), fair (5–9 mm), good (9–11 mm), and excellent (>12 mm); patients with poor levator function typically require frontalis sling procedures rather than levator-based repair.[30] MCD, measured from the eyelid margin to the skin crease in downgaze, normally ranges from 7 to 8 mm in men and 8 to 10 mm in women. In congenital ptosis, the crease is often absent or poorly defined, whereas in aponeurotic ptosis, the crease is typically elevated. Precise recreation of the eyelid crease, matched to the contralateral side, is essential during surgical correction to achieve optimal symmetry and aesthetic outcomes.
A comprehensive ocular examination is required to exclude alternative diagnoses and identify coexisting pathology. Evaluation includes visual acuity, refraction, pupillary assessment, ocular motility, and cover testing to rule out hypotropia or pseudoptosis. Corneal sensation, tear film status, and the presence of lagophthalmos must be assessed because they affect the risk of postoperative exposure. Funduscopic examination may reveal findings such as retinal pigmentary degeneration in myopathic conditions. External examination should also document brow ptosis, dermatochalasis, or cicatricial changes, as these may necessitate concurrent procedures such as blepharoplasty.
Specialized Functional Testing
Targeted functional testing further refines diagnosis and surgical planning. Assessment of the Bell phenomenon is critical, as poor upward globe rotation increases the risk of postoperative exposure keratopathy and may necessitate undercorrection or avoidance of surgery. A Hering test should be performed in unilateral ptosis to evaluate for contralateral eyelid droop upon manual elevation, which has important implications for bilateral surgical planning. The phenylephrine test is particularly useful in cases of mild ptosis or Horner syndrome, helping to identify candidates for posterior approach procedures such as conjunctival Müllerectomy.
Evaluation for myasthenia gravis includes fatigue testing (sustained upgaze) and the ice test, in which improvement in eyelid position supports a neuromuscular etiology. Hertel exophthalmometry is used to identify proptosis or enophthalmos, aiding in differentiation from pseudoptosis. These targeted assessments ensure accurate classification and appropriate procedural selection.
Laboratory and Imaging Workup
Laboratory testing should be directed by suspected etiology rather than performed routinely. In suspected ocular myasthenia gravis, evaluation includes acetylcholine receptor, muscle-specific kinase, acetylcholine receptor (antibody, and low-density lipoprotein receptor-related protein 4. Thyroid function testing and thyroid-stimulating hormone receptor antibodies are indicated in suspected thyroid-associated orbitopathy.
Imaging is reserved for cases with concerning neurologic or orbital features. Acute or subacute third nerve palsy, particularly with pupillary involvement, requires urgent computed tomography angiography or magnetic resonance angiography (to exclude an aneurysm. At the same time, magnetic resonance imaging of the brain and orbits is indicated for suspected demyelinating, inflammatory, or neoplastic processes. In pediatric Horner syndrome, imaging of the sympathetic chain from the brainstem to the chest may be necessary to identify underlying pathology.
Surgical Planning Considerations
Preoperative planning integrates clinical measurements with etiology to determine the optimal surgical approach. Levator function guides procedure selection, while eyelid crease height and symmetry must be carefully considered to achieve acceptable cosmetic outcomes. Identification of coexisting brow ptosis or dermatochalasis is essential, as combined procedures are often required in involutional cases. Recognition of risk factors, such as a poor Bell phenomenon or ocular surface disease, informs decisions regarding the degree of correction and the need for conservative surgical strategies.
Patient Counseling and Informed Consent
Comprehensive patient counseling is a critical component of preparation. Patients should receive a preoperative review of the surgical plan, including technique, incision location, and expected scar characteristics. Use of pre- and postoperative photographs enhances understanding of realistic outcomes.
Demonstration of expected eyelid elevation in the clinic is particularly valuable in conservative or Müller muscle–based procedures. Discussion must include potential complications such as overcorrection, undercorrection, contour asymmetry, lagophthalmos, dry eye, exposure keratopathy, infection, and recurrence. Patients should also be counseled regarding the possibility of contralateral surgery, particularly in the presence of the Hering law effects, and informed consent must be obtained.
Postoperative Photography and Documentation
Standardized preoperative photography is essential for documentation, surgical planning, and postoperative comparison. Images should be obtained in multiple positions, including primary gaze, upgaze, downgaze, eyelid closure, and oblique views. Postoperative photographs, typically obtained at approximately 2 months, allow objective assessment of surgical outcomes and symmetry. Consistent photographic technique is critical for accurate comparison and quality assessment. A structured and meticulous approach to patient preparation ensures accurate diagnosis, appropriate procedure selection, risk mitigation, and alignment of surgical outcomes with patient expectations.
Technique or Treatment
Historical Evolution and Contemporary Surgical Approaches in Blepharoptosis
Early surgical management of ptosis was rudimentary and focused primarily on excision of excess upper eyelid skin, without direct correction of the underlying elevator mechanism. The evolution of modern ptosis surgery began in the late 19th century with efforts to recruit the frontalis muscle as a compensatory elevator. Dransart (1880) first described suspension of the eyelid to the brow using absorbable catgut sutures, a concept later modified by Pagenstecher, who utilized silk sutures for improved durability.
Subsequent innovations by Wright (1922) and Crawford (1956) introduced the use of autologous fascia lata as a sling material, anchored to the tarsal plate and frontalis muscle, establishing a durable and physiologic method of frontalis suspension.[31] Additional autologous materials, including palmaris tendon and temporalis fascia, were also explored, followed by the development of nonabsorbable synthetic materials. Tillet and Tillet (1966) further advanced the technique by introducing silicone rod slings, which emphasized improved elasticity and dynamic eyelid movement and reduced postoperative lagophthalmos.[32]
Parallel advancements occurred in levator-based procedures. Bowman (1857) first described levator resection via a conjunctival approach, which was subsequently refined by Blaskovics (1909). Further technical improvements by Berke and Illif established levator resection as a cornerstone of ptosis surgery, with Berke (1959) notably introducing the concept of intraoperative adjustment based on levator function to guide eyelid height and optimize outcomes.[33] The anterior (transcutaneous) approach, popularized by Everbush (1883) and Wolf (1896), provided improved exposure of the levator aponeurosis, facilitating more precise identification, advancement, or resection. This approach remains widely utilized due to its anatomic clarity and reproducibility, particularly for surgeons early in their experience.
Less invasive posterior approaches were later developed to address mild ptosis. Fasanella and Servat (1961) described a vertical lid-shortening procedure involving resection of the tarsus, conjunctiva, and Müller’s muscle, offering a simplified technique for select cases.[34] Putterman (1972) refined this concept by isolating resection to the Müller muscle and conjunctiva while preserving the tarsal plate, thereby reducing structural disruption and improving predictability.[35]
Contemporary management of ptosis remains predominantly surgical, with technique selection guided by etiology, severity, and levator function (see Video. Upper Blepharoplasty and Ptosis Repair). In adults, the most commonly employed procedures include levator aponeurosis advancement or resection via an anterior approach and Müller muscle-conjunctival resection via a posterior approach. Frontalis suspension is less frequently used in adults. Still, it remains the procedure of choice in cases of poor levator function, particularly in myogenic and neurogenic ptosis, where the risk of exposure keratopathy is elevated. The reversibility of sling procedures provides an additional safety advantage in these high-risk populations.
Levator Aponeurosis Advancement Procedure
This is the procedure of choice for aponeurotic and involutional ptosis, which is caused by dehiscence, disinsertion, or thinning of the levator aponeurosis.[36][37] The method can be combined with an upper eyelid blepharoplasty in patients with associated dermatochalasis. The following steps comprise this procedure:
- Preoperative skin marking
- Precise preoperative marking is essential for achieving symmetry and optimal cosmetic outcomes. Markings are performed with the patient in the sitting position, eyes in primary gaze, to replicate the physiologic eyelid position. The upper eyelid crease is outlined prior to infiltration of local anesthetic to avoid distortion of landmarks. In patients with a well-defined preexisting crease, that crease is used as the reference. In unilateral ptosis with an elevated or absent crease, markings are based on the contralateral normal eyelid. In bilateral ptosis, the crease is typically marked at 8 to 10 mm centrally along the pupillary axis and tapered to approximately 5 to 6 mm medially and laterally to maintain a natural contour.
- Anesthesia and intraoperative considerations
- Local anesthesia is administered using 2% lidocaine with 1:100,000 epinephrine, providing both analgesia and vasoconstriction to enhance hemostasis. Approximately 1 to 1.5 mL is infiltrated along the marked incision line. Careful limitation of anesthetic volume is critical, as excessive infiltration can transiently impair levator function and compromise intraoperative assessment of eyelid height. Monitored anesthesia care with light intravenous sedation may be used for patient comfort; however, over-sedation should be avoided to permit patient cooperation during intraoperative eyelid position assessment.
- Surgical Steps
- Surgical exposure and dissection
- Following standard sterile preparation and draping, both eyes are left exposed to allow continuous comparison of eyelid position. A lid crease incision is created using a No. 15 blade, with adjunctive use of unipolar cautery or CO2 laser as needed for hemostasis. Dissection proceeds through the orbicularis oculi muscle along the full length of the incision to expose the orbital septum. Hypertrophied orbicularis fibers may be conservatively excised. Inferior dissection in the suborbicularis plane exposes the superior border of the tarsal plate; excessive dissection toward the lash line is avoided to prevent postoperative lash ptosis.
- The orbital septum is identified and opened, often facilitated by gentle globe pressure to prolapse the preaponeurotic fat pad. The septum is incised carefully, preferably slightly superiorly, to avoid inadvertent injury to the levator aponeurosis. Blunt dissection separates the preaponeurotic fat from the underlying levator complex, and all fibrous septal attachments to the levator are released to prevent postoperative lid retraction. A Desmarres retractor aids in maintaining exposure.
- Identification and advancement of the levator aponeurosis
- The disinserted or attenuated levator aponeurosis is identified as a thin, pale structure at the junction where the septum fuses with the aponeurosis. In cases of dehiscence, the Müller muscle and its vascular arcade may be visible just superior to the tarsal plate. The aponeurosis is mobilized and advanced inferiorly for reattachment to the tarsus.
- A double-armed 5-0 Vicryl or polyester suture is placed through the central tarsus approximately 2 mm below the superior border using a partial-thickness bite to avoid full-thickness penetration and corneal injury. The suture is then passed through the aponeurosis in a horizontal mattress configuration, and a temporary (slip) knot is tied. The patient is asked to open the eyes, and eyelid height and contour are assessed in both supine and sitting positions. Adjustments in suture placement are made as needed to achieve optimal symmetry. Once satisfactory positioning is confirmed, the suture is secured, and additional medial and lateral sutures are placed to refine the contour.
- Eyelid crease formation and wound closure
- If necessary, eyelid crease–forming sutures are placed using interrupted 6-0 nonabsorbable sutures. These sutures engage the lower skin edge, pass partially through the levator aponeurosis, and exit through the upper skin edge to recreate a well-defined crease. Skin closure is performed with interrupted 6-0 plain gut or equivalent sutures. Topical antibiotic ointment is applied, and a light dressing or temporary eye patch may be placed.
- Postoperative care
- Postoperative management focuses on edema control, infection prevention, and ocular surface protection. Patients are instructed to apply cold compresses for the first 48 hours to reduce swelling. Topical antibiotic ointment is applied to the incision site, and frequent use of lubricating eye drops is recommended to prevent exposure-related complications. Sutures are typically removed 7 to 10 days postoperatively. Close follow-up is essential to monitor eyelid position and wound healing, and to identify early complications such as overcorrection, undercorrection, or lagophthalmos.
- Surgical exposure and dissection
Modified Müller Muscle–Conjunctival Resection
Modified Müller muscle–conjunctival resection (MMCR) is a posterior approach technique indicated for patients with mild ptosis and excellent levator function, as well as select cases of ptosis secondary to Horner syndrome or in anophthalmic sockets. The procedure is a modification of the Fasanella–Servat technique, with resection limited to the conjunctiva and the Müller muscle rather than including the tarsus. Preoperative confirmation of candidacy is essential and includes a positive response to a 2.5% topical phenylephrine test, which predicts postoperative eyelid elevation. A commonly cited guideline suggests approximately 4 mm of resection for every 1 mm of desired ptosis correction. However, this relationship is variable and often individualized based on the surgeon's experience and intraoperative judgment.[38] Adequate healthy conjunctiva within the superior fornix is also a prerequisite for safe and effective resection.
- Preoperative preparation and marking
- Following routine sterile preparation and draping, both eyes are kept exposed to allow intraoperative comparison of eyelid height. Traction sutures using 5-0 silk are placed in the upper eyelid to facilitate eversion. A Desmarres retractor is used to evert and stabilize the eyelid, with traction sutures secured to the forehead drapes. The conjunctival surface is gently dried, and markings are made just superior to the tarsal border. A second marking is placed superior to the first at a distance corresponding to half the intended resection length. For example, a planned 8-mm resection to correct 2-mm ptosis requires a second marking at 4 mm above the superior tarsal border.
- Anesthesia
- Local anesthesia is administered with 1 to 2 mL of 2% lidocaine containing 1:100,000 epinephrine injected into the superior conjunctival fornix, producing ballooning of the conjunctiva to facilitate dissection. Additional infiltration at the lid crease and light intravenous sedation under monitored anesthesia care may be provided. As with anterior approaches, oversedation should be avoided to preserve the ability to perform intraoperative eyelid assessment when needed.
- Surgical technique
- Three 6-0 silk sutures are placed through the superior conjunctival markings, incorporating conjunctiva and the Müller muscle while avoiding the levator aponeurosis. Gentle traction on these sutures separates the Müller muscle and conjunctiva from the underlying levator complex. The Desmarres retractor is then removed, and a Putterman clamp is applied across the base of the elevated tissue, ensuring that the tarsal plate is excluded.
- A double-armed 6-0 absorbable suture (plain gut or Vicryl) is passed in a running horizontal mattress fashion beneath the clamp from one end to the other. The clamped tissue, comprising conjunctiva and the Müller muscle, is then excised using a #15 blade, with the clamp serving as a cutting guide. The suture is then run in reverse in a similar horizontal mattress fashion and tied securely to complete the closure. An alternative technique involves externalizing the suture through the full thickness of the eyelid to the skin surface, where it is tied and later removed approximately 1 week postoperatively.
- Postoperative care
- Postoperative management emphasizes edema control and ocular surface protection. Patients are instructed to apply cold compresses for the first 48 hours. Topical antibiotic ointment is applied, typically at bedtime for one week, and frequent use of lubricating eye drops is recommended to prevent exposure-related symptoms. Follow-up evaluation ensures appropriate eyelid position, assesses healing, and identifies complications such as overcorrection, undercorrection, or ocular surface irritation.
Frontalis Sling Surgery
Frontalis sling surgery is indicated for patients with severe ptosis and poor levator function (less than 4 mm), particularly in conditions such as severe congenital ptosis, myogenic ptosis (eg, myasthenia gravis, chronic progressive external ophthalmoplegia), neurogenic ptosis (eg, third cranial nerve palsy), blepharophimosis syndrome, and Marcus Gunn jaw-winking syndrome. The procedure utilizes the frontalis muscle, which contributes approximately 2 to 3 mm of eyelid elevation, by suspending the eyelid to the brow, thereby allowing brow elevation to elevate the eyelid. Various materials may be used for suspension, including autogenous (fascia lata, palmaris longus tendon, temporalis fascia), allogenic (banked fascia lata), and synthetic materials (polypropylene, Supramid nylon, Mersilene mesh, silicone), with fascia lata considered the gold standard and silicone rod commonly used due to its elasticity and adjustability.[39]
- Preoperative marking (Fox pentagon technique)
- The Fox pentagon technique is most commonly used due to its relative simplicity and fewer incisions compared to the Crawford method, particularly when synthetic materials are employed. Skin markings consist of 5 small incisions: 2 eyelid incisions placed approximately 2 mm above the lid margin at the medial and lateral limbus (adjusted as needed to optimize contour), 2 brow incisions located just above the medial and lateral canthi, and a central forehead incision positioned in the pupillary plane slightly superior to the brow markings.
- Anesthesia
- General anesthesia is preferred in children, whereas local anesthesia with monitored intravenous sedation is typically used in adults. Local infiltration is performed with 2% lidocaine containing 1:100,000 epinephrine at the marked incision sites, followed by applying pressure to promote vasoconstriction and improve hemostasis.
- Surgical technique
- After routine sterile preparation and draping, both eyes and the forehead are kept exposed to allow continuous intraoperative assessment of eyelid position and sling passage. Stab incisions are created at the marked sites, and the central forehead incision is enlarged to approximately 3 to 5 mm. The sling material, mounted on a needle, is passed from the central forehead incision to the medial eyebrow incision, engaging the frontalis muscle. The sling is then directed from the medial brow incision to the medial eyelid incision, passing deep to the orbicularis oculi but anterior to the orbital septum and tarsal plate. The sling is then passed from the medial to the lateral eyelid incision, where it lies superficial to the tarsus, with careful attention to avoid globe injury, often aided by use of a lid guard. Then the sling is passed in reverse from the lateral eyelid incision to the lateral brow incision, then back to the central forehead incision, completing the pentagonal configuration.
- Adjustment and fixation
- Eyelid height and contour are adjusted intraoperatively, with assessment in both supine and, when feasible, seated positions to ensure symmetry. Once the desired lid height is achieved, the sling is secured, commonly using a silicone sleeve, and excess material is trimmed. The knot and sleeve are buried within a subcutaneous pocket to reduce the risk of extrusion.
- Closure
- All incisions are closed with interrupted 6-0 plain gut sutures. A Frost suture may be placed through the lower eyelid to provide temporary corneal protection in the immediate postoperative period.
- Postoperative care
- Postoperative management includes applying cold compresses for the first 48 hours to minimize edema, applying topical antibiotic ointment at bedtime for approximately 1 week, and frequent administration of lubricating eye drops to maintain ocular surface protection. Frost sutures, if placed, are typically removed after 48 hours. Close follow-up is essential to monitor eyelid position and symmetry, and to detect potential complications such as lagophthalmos, exposure keratopathy, or recurrence.
Frontalis Muscle Advancement
Frontalis muscle advancement is a surgical option for severe ptosis in patients with poor levator function, in which a flap of the frontalis muscle is mobilized and advanced inferiorly to attach to the tarsal plate, thereby allowing brow elevation to elevate the eyelid. This technique provides a dynamic and more physiologic alternative to sling procedures by directly recruiting frontalis muscle action while preserving a more natural eyelid contour and movement.
- Preoperative marking
- The upper eyelid crease is marked before incision, using standard lid crease landmarks and symmetry with the contralateral side when applicable. Accurate marking is essential, as intraoperative adjustments are limited under general anesthesia conditions.
- Anesthesia
- Most frontalis muscle flap advancements are performed under general anesthesia. General anesthesia poses challenges to achieving precise eyelid symmetry, as induction often results in globe deviation toward exotropia and hypertropia, obscuring the true primary gaze position. Accurate preoperative marking and careful intraoperative estimation of eyelid height are therefore critical to achieving optimal outcomes, with adjustments based on anticipated postoperative positioning rather than intraoperative globe alignment.[40]
- Surgical technique
- An incision is made along the marked lid crease, and dissection proceeds through the orbicularis oculi muscle to expose the anterior surface of the tarsal plate. Dissection is then carried superiorly in the suborbicularis preseptal plane up to the supraorbital margin, where the arcus marginalis is identified. From this point, biplanar dissection is continued above the arcus marginalis into both subcutaneous and subgaleal planes, extending approximately 2 cm above the eyebrow to mobilize a frontalis muscle flap. The width of the flap is designed to be slightly less than the horizontal palpebral fissure, and the distal edge is shaped in an arch configuration to mimic the natural curvature of the levator aponeurosis insertion.
- The mobilized frontalis flap is advanced inferiorly and secured to the upper one-third of the anterior surface of the tarsal plate using 5-0 polypropylene sutures. Intraoperative adjustments are performed to position the eyelid margin at the level of the superior limbus, taking into account expected postoperative changes. Hemostasis is achieved, and the skin incision is closed with 6-0 Ethilon sutures.
- Variations of technique
- Multiple modifications of frontalis flap advancement have been described to optimize functional and aesthetic outcomes:
- The tripartite frontalis muscle flap divides the distal flap into 3 segments, redistributing tension and reducing lid tenting.
- The orbicularis oculi muscle and orbital septum flap transmit frontalis action indirectly by advancing these structures to the tarsus.
- The orbicularis oculi–frontalis muscle composite flap allows downward advancement while minimizing risk to the temporal branch of the facial nerve.
- The forked frontalis aponeurosis suspension technique creates a bifurcated flap that preserves frontalis function and reduces the risk of neurovascular injury.
- The frontalis transfer via a suborbicularis tunnel technique improves functional outcomes by preserving tissue planes.
- Overlap techniques that combine the frontalis muscle with an inferiorly based orbital septum flap enable synergistic action between the frontalis and levator systems.
- The frontal orbicularis oculi muscle flap incorporates orbicularis, septum, and distal frontalis fibers into a composite flap advanced to the tarsus, with improved contour and reduced recurrence rates.
- The double-breasted technique divides the orbicularis flap into superior and inferior components, with layered fixation that has been associated with minimal postoperative lagophthalmos.[40]
- Multiple modifications of frontalis flap advancement have been described to optimize functional and aesthetic outcomes:
- Closure
- Following flap fixation and confirmation of eyelid position, meticulous hemostasis is achieved. The skin is closed using fine interrupted sutures, typically 6-0 Ethilon, to optimize cosmetic outcome.
- Postoperative care
- Postoperative management includes routine wound care, application of cold compresses to reduce edema, and lubrication to protect the ocular surface. Close follow-up is required to monitor eyelid height and symmetry, as well as complications such as undercorrection, recurrence, or exposure-related issues.
The Pelin Easy and Needle Up to Stretch, PEANUTS, Technique for MMCR
The PEANUTS technique is a modification of the conventional MMCR designed to simplify posterior approach ptosis correction. Traditional MMCR utilizes a Putterman clamp to secure and stretch the conjunctiva and Müller’s muscle before resection. The PEANUTS technique replaces this specialized instrument with a standard disposable 21-gauge needle, which is used to engage, stabilize, and uniformly stretch the posterior lamella, thereby enabling controlled, precise excision, improving visualization, and reducing instrument burden.[41]
- Indications and patient selection
- Ideal candidates include patients with mild-to-moderate aponeurotic ptosis, preserved levator function of at least 10 mm, and a positive response to preoperative phenylephrine testing. Contraindications include prior significant eyelid or corneal trauma, previous ocular surgery involving the posterior lamella, irregular eyelid margins, and preexisting ocular surface disease, as these conditions may compromise surgical accuracy or increase the risk of complications.
- Anesthesia
- The procedure is performed under local anesthesia. Approximately 0.1 mL of 2% lidocaine with 1:100,000 epinephrine is injected medially and temporally beneath the upper eyelid skin to provide adequate analgesia and vasoconstriction.
- Surgical technique
- The upper eyelid is everted over a Desmarres retractor to expose the superior border of the tarsal plate. A caliper is used to mark a resection length of approximately 4 to 5 mm on the conjunctiva and the Müller muscle. A 21-gauge needle is then introduced temporally and passed horizontally through the marked tissue to exit nasally, providing even traction and stabilization of the posterior lamella.
- A 6-0 Prolene suture is passed full-thickness through the eyelid, and a running horizontal mattress suture is placed just superior to the tarsal border. The suture ends are externalized and secured over 1-mm silicone bolsters to maintain tension and approximation. The elevated conjunctiva and the Müller muscle are then excised using Stevens scissors, with the blades oriented parallel to the suture line to ensure controlled and precise resection.
- Rationale and advantages
- Replacing the Putterman clamp with a disposable needle eliminates the bulk of the traditional instrument, improving visualization of the superior tarsal border and facilitating more accurate resection placement. Reduced instrument size reduces crowding in the operative field and lowers procedural costs. The needle provides stable tissue traction while maintaining a streamlined surgical setup, enhancing efficiency without compromising precision.[41]
- Outcomes and technical considerations
- Reported case series demonstrate favorable functional and cosmetic outcomes with the PEANUTS technique, including reliable eyelid elevation and preservation of posterior lamellar integrity without significant intraoperative or postoperative complications. The absence of a clamp's inherent rigidity and weight requires greater surgeon control and steady technique to maintain tissue stability during resection. Careful handling is essential to prevent tissue slippage and ensure consistent results throughout the procedure.
Sutureless Conjunctival-Sparing Müllerectomy
This is a posterior approach for correcting mild-to-moderate blepharoptosis in patients with good levator function. Unlike traditional MMCR, which involves excision of the conjunctiva, this technique preserves the conjunctiva by creating a flap and selectively targeting the Müller muscle. The “sutureless” component refers to the use of bipolar cautery to plicate and contract the Müller muscle, eliminating the need for sutures while achieving eyelid elevation by shortening the tissue.[42]
- Indications and patient selection
- Appropriate candidates include patients with mild-to-moderate ptosis, good levator function, and a favorable response to phenylephrine testing. Conjunctival preservation makes this technique particularly advantageous in patients in whom ocular surface integrity is critical or in whom future ocular procedures (eg, glaucoma surgery or anophthalmic socket reconstruction) may be anticipated.
- Anesthesia
- Local anesthesia is administered using 1% lidocaine with 1:100,000 epinephrine injected subconjunctivally. This facilitates hydrodissection, delineates the surgical plane between the conjunctiva and the Müller muscle, and provides hemostasis.
- Surgical technique
- The upper eyelid is everted to expose the superior border of the tarsal plate. A #15 Bard-Parker blade is used to create a conjunctival incision along the superior edge of the tarsus. Sharp dissection with Westcott scissors separates the conjunctiva from the underlying Müller muscle, creating a conjunctival flap that is reflected inferiorly toward the lower eyelid. The desired portion of the Müller muscle is then grasped with forceps.
- Hemostat forceps are applied to the muscle to create a controlled “crush zone” that defines the treatment area. Bipolar cautery is subsequently applied to the crushed segment, inducing contraction and shortening of the Müller muscle down to the level of the superior tarsal border. After adequate contraction is achieved, the conjunctival flap is repositioned over the treated muscle without sutures, relying on natural tissue adherence for stabilization.
- Outcomes
- Clinical outcomes demonstrate a mean improvement in MRD1 of approximately 2.85 mm at 6 months, with sustained functional and cosmetic results reported through 2.5 years of follow-up. The procedure provides predictable elevation while maintaining the structural integrity of the posterior lamella.
- Advantages and considerations
- Preservation of conjunctiva and goblet cells supports tear film stability and ocular surface health, representing a key advantage over traditional MMCR. Elimination of sutures reduces the risk of corneal abrasion and foreign-body sensation, thereby improving postoperative comfort. Operative time is significantly reduced, averaging approximately 4.4 minutes compared to 8.5 minutes for standard MMCR. Conjunctival preservation also maintains tissue availability for potential future procedures. Successful execution depends on precise dissection and controlled cautery application to achieve consistent muscle contraction without overcorrection.
Oxymetazoline for Ptosis Correction
Surgical correction remains the standard treatment for blepharoptosis; however, operative intervention carries risks including infection, scarring, eyelid asymmetry, and patient reluctance toward invasive procedures. These limitations have prompted the development of nonsurgical alternatives. Oxymetazoline 0.1% ophthalmic solution was approved by the Food and Drug Administration in July 2020 as the first pharmacologic therapy for acquired blepharoptosis, providing a minimally invasive option for selected patients.[43][44]
- Mechanism of action
- Oxymetazoline is an α-adrenergic receptor agonist that stimulates the Müller muscle, a sympathetically innervated smooth muscle contributing to upper eyelid elevation. Activation of these receptors induces contraction of the Müller muscle, resulting in elevation of the upper eyelid margin and improvement in eyelid position.
- Dosage and administration
- The medication is administered topically as a 0.1% ophthalmic solution, typically as 1 drop instilled into the affected eye once daily.
- Clinical outcomes
- Clinical studies demonstrate meaningful improvement in eyelid position following treatment, with a mean increase in MRD1 of approximately 1.4 mm from baseline. Improvement in superior visual field parameters and reduction in functional visual field deficits have also been observed.
- Duration of effect
- Onset of action occurs rapidly, generally within 10 minutes of instillation, with therapeutic effect lasting up to 8 hours following a single dose.
- Indications
- Primary indication includes mild to moderate acquired involutional (age-related) ptosis, particularly in patients seeking nonsurgical management or those who are not optimal surgical candidates.
- Advantages
- Noninvasive administration provides both functional and cosmetic improvement without the risks associated with surgery. Ease of use and rapid onset make this therapy an attractive option for patients who prefer conservative management or require temporary correction.
- Limitations
- Therapeutic effects are transient, necessitating repeated daily use. Limited evidence exists regarding efficacy in other etiologies of ptosis, including neuromuscular, traumatic, iatrogenic, or synkinetic causes.
- Adverse effects
- Adverse effects are generally mild and self-limited, with approximately 12.2% of patients reporting symptoms such as ocular dryness, irritation, or headache.
Complications
The following complications may occur with any ptosis repair:
- UndercorrectionThis phenomenon may occur with any technique. In the immediate postoperative period, the lid appears undercorrected due to the lid edema. Patients may be reassured. However, if the undercorrection persists, then revision surgery may be required. The wound can be reopened, and the aponeurosis re-advanced.
- OvercorrectionOvercorrection is more often encountered following advancement for aponeurotic/involutional ptosis. Mild overcorrection in the immediate postoperative period may be tackled with eyelid traction. The patient may be asked to look downward and pull on the eyelashes with the thumb and forefinger; this may be done for a few minutes, 3 to 4 times a day. Severe overcorrection will require immediate revision. The wound can be reopened and the sutures cut. The levator is then placed at a more recessed position or secured to the tarsal plate using hang-back sutures.
- Lagophthalmos and exposure keratopathyAll patients are counseled preoperatively about postoperative lagophthalmos and decreased blink rate. Management of lagophthalmos in the immediate postoperative period is with copious lubricants. A temporary frost suture may be applied. In cases where severe exposure keratopathy develops, a revision surgery is done to lower the lid height.
- Eyelid contour defects and height asymmetryContour defects result from improper suture placement on the tarsus. Patients presenting with small contour defects usually settle down with time. Lid massage and eyelid traction exercises are advised. Persistent or severe contour abnormalities require revision surgery and proper suture placement on the tarsus.
- Conjunctival prolapseExtensive dissection between the conjunctiva and levator can disrupt the suspensory ligaments of the superior fornix and produce conjunctival prolapse. Mild prolapse can be treated conservatively with lubricants. Severe prolapse requires repositioning of the conjunctiva with Pang sutures. The suture is passed through the prolapsed conjunctiva and secured at the skin crease.
- Eyelash ptosisExcessive dissection of the orbicularis from the tarsus results in lash ptosis, which anterior lamella repositioning sutures can correct.
- Suture granulomaSmall granulomas can form at the suture site. They can be excised with Wescott scissors and the base cauterized. The suture causing the granuloma also requires removal.
These complications can occur with frontalis muscle advancement:
- Risk of transient hypoesthesiaThere is a possibility of temporary, mild sensory loss due to inadvertent injury to the supraorbital nerve while making the vertical incision on the frontalis muscle. Elevating the transposed flap more laterally reduces the risk, as increased lateral elevation produces more visible tenting of the eyelid margin.
- Reduction in forehead wrinklingBecause the frontalis muscle is partially detached and repositioned, postoperative forehead wrinkling may be diminished. This makes the technique relatively unsuitable for patients with unilateral ptosis who naturally have deep forehead creases.
- Lower eyebrow position in upgaze (unilateral cases)In unilateral procedures, the operated side may show a slightly lower brow height on superior gaze due to altered frontalis mechanics.
- Limited symmetry and synchrony of eyelid movementPerfectly symmetrical and synchronous eyelid elevation cannot be expected in unilateral cases. As frontalis is not a true eyelid elevator, its action resembles a vertical “window-blind” pull, in contrast to the natural upward-and-posterior vector of the levator muscle.[40]
Clinical Significance
Correction of ptosis is clinically significant, as it directly resolves both functional and aesthetic deficiencies associated with eyelid misalignment. Upper eyelid ptosis can impair the superior visual field, prompting patients to adopt compensatory strategies such as elevating the brows, turning the head, or engaging the frontalis muscle to maintain adequate vision. These changes may result in secondary symptoms such as headaches, ocular strain, and muscular discomfort in the cervical region and forehead.
Surgical correction restores the native palpebral aperture, enhancing visual function and alleviating the physical strain associated with chronic compensatory mechanisms. Patients typically describe an immediate alleviation of eyelid heaviness, a symptom that is difficult to measure but is often regarded as one of the most distressing effects of ptosis. Ptosis surgery improves daily activities, including reading, driving, and work requiring sustained visual focus, by restoring normal vision field and eyelid posture. The cosmetic and psychosocial advantages of ptosis correction, in addition to functional recovery, are significant. Ptosis is frequently linked to exhaustion, senescence, or apathy, resulting in adverse self-image and possible social censure. Surgical correction yields a revitalized, symmetrical, and more vigilant appearance, enhancing self-confidence and overall quality of life.
There tend to be improvements in patient-reported outcome measures, including health-related quality of life and psychological well-being scores, following ptosis correction. These enhancements span multiple age groups, underscoring that the advantages extend beyond aesthetic improvement to encompass a more comprehensive restoration of social functioning and psychological well-being. Consequently, ptosis correction serves as both a reconstructive procedure for functional rehabilitation and an intervention with significant effects on patient identity, mental health, and social participation.
Enhancing Healthcare Team Outcomes
Improving patient-centered care in ptosis correction requires a collaborative, interprofessional strategy that incorporates the expertise of ophthalmologists, oculoplastic surgeons, plastic surgeons, ophthalmic nurses, optometrists, and other healthcare professionals. Initial patient interactions typically involve ophthalmic nurses or optometrists, who are crucial in documenting symptoms, conducting vision and visual field exams, and ensuring precise baseline evaluations. Prompt recognition of functional impairment, ocular surface illness, or concomitant diseases enables appropriate referrals and rapid professional assessment.
Surgeons, whether oculoplastic or plastic, need to determine the most appropriate surgical approach based on anatomical considerations, levator function, and individual patient characteristics, while also identifying instances in which surgery is contraindicated. Pharmacists ensure the safe use of medications during the preoperative period, especially for patients undergoing immunosuppressive therapy for autoimmune-related ptosis or those with intricate comorbidities on anticoagulation. Efficient communication among these disciplines guarantees that every member of the care team is synchronized on the treatment plan, reducing errors and enhancing patient safety.
Surgeons must consider functional requirements with aesthetic factors, securing informed consent that encompasses both medical indications and patient objectives. Nurses and advanced practitioners can assist in delivering essential perioperative education, highlighting postoperative care directives, indicators of problems such as infection or lagophthalmos, and the significance of follow-up appointments. This collaborative educational initiative enables patients and families to actively engage in care, thereby reducing complications and improving adherence to treatment protocols. Effortless care coordination, from the initial consultation to surgical intervention and long-term follow-up, diminishes fragmentation and improves both outcomes and patient satisfaction. By fostering a culture of interprofessional communication and collective accountability, healthcare teams addressing ptosis correction can provide safer, more effective, and patient-centered care, while simultaneously enhancing overall team performance.
Media
(Click Image to Enlarge)
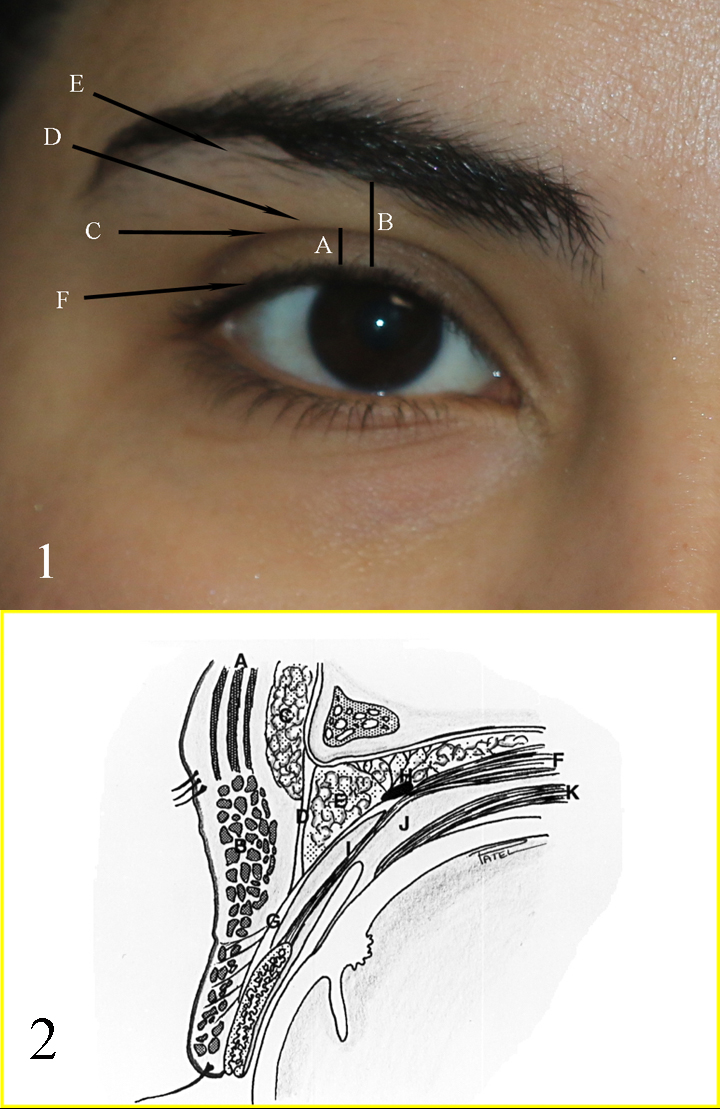
Eyelid Landmarks and Aesthetic Units and Anatomy of the Upper Eyelid and Brow Complex. Fig 1: A: Upper eyelid platform; B: Brow to lid margin distance; C: Upper eyelid crease; D: Upper eyelid fold; E: Brow fat pad; F: Eyelid margin and eyelash curve Fig 2: A: Frontalis muscle; B: Orbicularis muscle; C: Brow fat pad; D: Orbital septum; E: Preaponeurotic fat pads; F: Levator muscle; G: Levator aponeurosis; H: Whitnall ligament; I: Müller muscle; J: Common sheath; K: Superior rectus muscle.
Contributed by BCK Patel, MD, FRCS
(Click Image to Enlarge)

Normal Eyelids in a Caucasian Female. Skin creases are naturally asymmetrical. The highest point of the upper eyelid is slightly medial to the pupil's center, though it may appear more lateral when the patient converges. Fullness above the crease creates a fold, and fullness below the brows contributes to a youthful look.
Contributed by BCK Patel, MD, FRCS
(Click Video to Play)
Upper Blepharoplasty and Ptosis Repair. This video shows the basic steps of the procedure and examples of results.
Contributed by BCK Patel, MD, FRCS
(Click Image to Enlarge)

Ptosis. This photograph shows a young individual with unilateral left eye ptosis.
Contributed by B Shahzad, MBBS
References
Finsterer J. Ptosis: causes, presentation, and management. Aesthetic plastic surgery. 2003 May-Jun:27(3):193-204 [PubMed PMID: 12925861]
Yim KHC, Ma A, Yuen HKL. Does Müller Muscle Conjunctival Resection Ptosis Correction Work if Müller Muscle Was Previously Resected? Ophthalmic plastic and reconstructive surgery. 2025 Aug 11:():. doi: 10.1097/IOP.0000000000003043. Epub 2025 Aug 11 [PubMed PMID: 40788669]
Chodvadiya SA Jr, Manade V, Kotecha M, Ta J. Radiologic Imaging in Third Nerve Palsy: A Case Series Investigating Etiology, Patterns, and Clinical Implications. Cureus. 2023 Aug:15(8):e43986. doi: 10.7759/cureus.43986. Epub 2023 Aug 23 [PubMed PMID: 37746364]
Level 2 (mid-level) evidenceShuey NH. Ocular myasthenia gravis: a review and practical guide for clinicians. Clinical & experimental optometry. 2022 Mar:105(2):205-213. doi: 10.1080/08164622.2022.2029683. Epub 2022 Feb 14 [PubMed PMID: 35157811]
Kakizaki H, Malhotra R, Selva D. Upper eyelid anatomy: an update. Annals of plastic surgery. 2009 Sep:63(3):336-43. doi: 10.1097/SAP.0b013e31818b42f7. Epub [PubMed PMID: 19602949]
Ng SK, Chan W, Marcet MM, Kakizaki H, Selva D. Levator palpebrae superioris: an anatomical update. Orbit (Amsterdam, Netherlands). 2013 Feb:32(1):76-84. doi: 10.3109/01676830.2012.736602. Epub [PubMed PMID: 23387464]
Zeppieri M, Cazzato V, Surico PL, Caputo GG, Parodi PC, D'Esposito F, Musa M, Gagliano C, Scarabosio A. Comparative Analysis of Anterior vs Posterior Approaches in Eyelid Ptosis Repair. Discovery medicine. 2025 Apr:37(195):598-607. doi: 10.24976/Discov.Med.202537195.52. Epub [PubMed PMID: 40287797]
Level 2 (mid-level) evidenceAzad AD, Reshef ER, Lee NG. Hyperglobus and Pseudoptosis in Type 1 Lipogenic Thyroid Eye Disease. American journal of ophthalmology case reports. 2023 Dec:32():101890. doi: 10.1016/j.ajoc.2023.101890. Epub 2023 Jul 13 [PubMed PMID: 37496819]
Level 3 (low-level) evidenceLatting MW, Huggins AB, Marx DP, Giacometti JN. Clinical Evaluation of Blepharoptosis: Distinguishing Age-Related Ptosis from Masquerade Conditions. Seminars in plastic surgery. 2017 Feb:31(1):5-16. doi: 10.1055/s-0037-1598188. Epub [PubMed PMID: 28255284]
McCoskey M, Yoon MK. Traumatic Ptosis. International ophthalmology clinics. 2024 Apr 1:64(2):1-9. doi: 10.1097/IIO.0000000000000489. Epub 2024 Mar 25 [PubMed PMID: 38525978]
Hou D, Tian B, Wang X, Wang Q, Zhu Y. Cause Analysis and Surgical Treatment of Aponeurotic Ptosis With Upper Eyelid Depression. The Journal of craniofacial surgery. 2024 Oct 1:35(7):1947-1951. doi: 10.1097/SCS.0000000000010155. Epub 2024 May 29 [PubMed PMID: 38810237]
Zloto O, Shah P, Paiusco V, Singh B, Kang S, Verity D, Fabiola M. The Outcomes of Involutional Ptosis Surgeries in a Single Tertiary Center. Current eye research. 2024 Mar:49(3):325-329. doi: 10.1080/02713683.2023.2277137. Epub 2023 Nov 3 [PubMed PMID: 37921352]
Dortzbach RK, Sutula FC. Involutional blepharoptosis. A histopathological study. Archives of ophthalmology (Chicago, Ill. : 1960). 1980 Nov:98(11):2045-9 [PubMed PMID: 7436841]
Son Y, Lee EJ, Kim NH, Lee SJ. Imaging Findings in Neurogenic Ptosis. Journal of the Korean Society of Radiology. 2025 Jul:86(4):483-500. doi: 10.3348/jksr.2024.0107. Epub 2025 Jul 25 [PubMed PMID: 40787295]
Rosso M, Ramaswamy S, Sucharew H, Vagal A, Anziska Y, Levine SR. Isolated Third Cranial Nerve Palsy in Pituitary Apoplexy: Case Report and Systematic Review. Journal of stroke and cerebrovascular diseases : the official journal of National Stroke Association. 2021 Sep:30(9):105969. doi: 10.1016/j.jstrokecerebrovasdis.2021.105969. Epub 2021 Jul 22 [PubMed PMID: 34303962]
Level 1 (high-level) evidenceKhan Z, Bollu PC. Horner Syndrome. StatPearls. 2026 Jan:(): [PubMed PMID: 29763176]
Maamouri R, Ferchichi M, Houmane Y, Gharbi Z, Cheour M. Neuro-Ophthalmological Manifestations of Horner's Syndrome: Current Perspectives. Eye and brain. 2023:15():91-100. doi: 10.2147/EB.S389630. Epub 2023 Jul 13 [PubMed PMID: 37465361]
Level 3 (low-level) evidenceElrod RD, Weinberg DA. Ocular myasthenia gravis. Ophthalmology clinics of North America. 2004 Sep:17(3):275-309; v [PubMed PMID: 15337189]
Hamel JI. Myotonic Dystrophy. Continuum (Minneapolis, Minn.). 2022 Dec 1:28(6):1715-1734. doi: 10.1212/CON.0000000000001184. Epub [PubMed PMID: 36537977]
Ali A, Esmaeil A, Behbehani R. Mitochondrial Chronic Progressive External Ophthalmoplegia. Brain sciences. 2024 Jan 27:14(2):. doi: 10.3390/brainsci14020135. Epub 2024 Jan 27 [PubMed PMID: 38391710]
Jordan DR, Klapper SR, Farmer J. Oculopharyngeal Muscular Dystrophy Ptosis, Mueller's Muscle Involvement, and a Review of Management Over 34 Years. Ophthalmic plastic and reconstructive surgery. 2022 Nov-Dec 01:38(6):535-542. doi: 10.1097/IOP.0000000000002118. Epub 2022 Jan 13 [PubMed PMID: 35030153]
Pietris J, Madike R, Lam A, Al Sharifi A, Bacchi S, Gupta AK, Kovoor JG, Chan W. Cogan's Lid Twitch for Myasthenia Gravis: A Systematic Review. Seminars in ophthalmology. 2023 Nov:38(8):727-736. doi: 10.1080/08820538.2023.2211134. Epub 2023 May 11 [PubMed PMID: 37166275]
Level 1 (high-level) evidenceKim JY, Yang HK, Kim N, Kim MJ, Cho SI, Seong MW, Park SS, Hwang JM. Strabismus in chronic progressive external ophthalmoplegia. Acta ophthalmologica. 2021 Mar:99(2):e274-e280. doi: 10.1111/aos.14558. Epub 2020 Nov 15 [PubMed PMID: 33191655]
Koka K, Patel BC. Ptosis Correction. StatPearls. 2026 Jan:(): [PubMed PMID: 30969650]
Schoelles KJ, Auw-Haedrich C. Updates on eyelid cancers. Asia-Pacific journal of ophthalmology (Philadelphia, Pa.). 2024 Mar-Apr:13(2):100057. doi: 10.1016/j.apjo.2024.100057. Epub 2024 Apr 12 [PubMed PMID: 38615904]
Lai KKH, Li CK, Tsang A, Wong SYS, Ko CKL. Ocular adnexal intramuscular hemangioma arising from the eyelid: case report and literature review. Orbit (Amsterdam, Netherlands). 2023 Jun:42(3):290-294. doi: 10.1080/01676830.2021.1990352. Epub 2021 Oct 22 [PubMed PMID: 34686104]
Level 3 (low-level) evidenceKumar N, Meel R, Bakhshi S, Pushpam D, Pushker N, Bajaj MS, Kashyap S, Sen S, Pathy S, Sharma S. Neoadjuvant Chemotherapy in Non-Metastatic Eyelid Sebaceous Gland Carcinoma: A Report in 10 Cases. Ocular oncology and pathology. 2024 Sep:10(3):123-130. doi: 10.1159/000538295. Epub 2024 Mar 21 [PubMed PMID: 39224524]
Level 3 (low-level) evidenceSert S, Arici C, Mergen B, Ekmekci OB. Effect of Ptosis Surgery on Tear Oxidative Stress Levels in Patients with Blepharoptosis and Pseudoptosis. Beyoglu eye journal. 2023:8(4):266-272. doi: 10.14744/bej.2023.33255. Epub 2023 Dec 1 [PubMed PMID: 38089078]
Jienmaneechotchai T, Apinyawasisuk S, Jariyakosol S, Hirunwiwatkul P. Interobserver and Intra-Observer Reliability of Eyelid Tests for Ocular Myasthenia Gravis. Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society. 2022 Jun 1:42(2):230-233. doi: 10.1097/WNO.0000000000001425. Epub 2021 Oct 22 [PubMed PMID: 34860746]
Anderson RL, Dixon RS. Aponeurotic ptosis surgery. Archives of ophthalmology (Chicago, Ill. : 1960). 1979 Jun:97(6):1123-8 [PubMed PMID: 375893]
Level 3 (low-level) evidenceCRAWFORD JS. Repair of ptosis using frontalis muscle and fascia lata. Transactions - American Academy of Ophthalmology and Otolaryngology. American Academy of Ophthalmology and Otolaryngology. 1956 Sep-Oct:60(5):672-8 [PubMed PMID: 13380883]
Tillett CW, Tillett GM. Silicone sling in the correction of ptosis. American journal of ophthalmology. 1966 Sep:62(3):521-3 [PubMed PMID: 5331721]
BERKE RN. Results of resection of the levator muscle through a skin incision in congenital ptosis. A.M.A. archives of ophthalmology. 1959 Feb:61(2):177-201 [PubMed PMID: 13616781]
FASANELLA RM, SERVAT J. Levator resection for minimal ptosis: another simplified operation. Archives of ophthalmology (Chicago, Ill. : 1960). 1961 Apr:65():493-6 [PubMed PMID: 13698293]
Putterman AM, Urist MJ. Müller muscle-conjunctiva resection. Technique for treatment of blepharoptosis. Archives of ophthalmology (Chicago, Ill. : 1960). 1975 Aug:93(8):619-23 [PubMed PMID: 1156223]
Kim YK, Chang LS, Kim EH. The anterior layer of the levator aponeurosis in blepharoptosis correction. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2021 Jun:74(6):1309-1315. doi: 10.1016/j.bjps.2020.10.040. Epub 2020 Nov 14 [PubMed PMID: 33358565]
Ambat JM, Morishige N, Takahashi Y, Kakizaki H. Changes in Eyelid Height Based on Intra-Operative Quantification of Levator Aponeurosis Advancement in Patients with Unilateral Ptosis. Seminars in ophthalmology. 2025 Apr:40(3):182-187. doi: 10.1080/08820538.2024.2388625. Epub 2024 Aug 8 [PubMed PMID: 39115176]
Dresner SC. Further modifications of the Müller's muscle-conjunctival resection procedure for blepharoptosis. Ophthalmic plastic and reconstructive surgery. 1991:7(2):114-22 [PubMed PMID: 1863563]
Takahashi Y, Leibovitch I, Kakizaki H. Frontalis suspension surgery in upper eyelid blepharoptosis. The open ophthalmology journal. 2010 Dec 14:4():91-7. doi: 10.2174/1874364101004010091. Epub 2010 Dec 14 [PubMed PMID: 21331314]
Bhattacharjee K, Sawarkar K, Soni D, Wavikar G. Journey of frontalis muscle advancement in severe blepharoptosis: Review of the techniques, modifications, and outcomes. Indian journal of ophthalmology. 2024 Nov 1:72(11):1569-1579. doi: 10.4103/IJO.IJO_357_24. Epub 2024 Aug 14 [PubMed PMID: 39141490]
Kaynak P, Şengün GD, Öztürker C, Akgöz E. Ptosis Repair by "PEANUTS" MMCR: "Pelin's Easy and Needle Up To Stretch" Müller's Muscle Conjunctival Resection Without the Putterman Clamp. Turkish journal of ophthalmology. 2025 Jun 25:55(3):174-176. doi: 10.4274/tjo.galenos.2025.61697. Epub [PubMed PMID: 40560178]
Mancini R, Forouzan P, Keenum ZG, Tenzel PA, Petroll WM. Sutureless Conjunctiva-Sparing Posterior Ptosis Repair Surgery: A Novel Technique. American journal of ophthalmology. 2023 Jul:251():77-89. doi: 10.1016/j.ajo.2023.03.001. Epub 2023 Mar 8 [PubMed PMID: 36898493]
Brito EM, Ferri F, Odulanmi T, Vera Silva MA, Cordero JP, Foran L, Newman MI, Sarraga AG. Oxymetazoline and Blepharoptosis: A Case Series and Proposed Treatment Algorithm. Cureus. 2025 Jul:17(7):e88649. doi: 10.7759/cureus.88649. Epub 2025 Jul 24 [PubMed PMID: 40861715]
Level 2 (mid-level) evidenceNewland M, Eberly H, Ma C, Lighthall JG. The Use of Oxymetazoline 0.1% Ophthalmic Solution for Acquired Blepharoptosis: A Systematic Review. The Laryngoscope. 2025 Jan:135(1):8-14. doi: 10.1002/lary.31723. Epub 2024 Aug 22 [PubMed PMID: 39172003]
Level 1 (high-level) evidence