Introduction
Calcium pyrophosphate deposition (CPPD) disease is a crystal deposition arthropathy that affects the cartilage, synovial, and periarticular tissues and is the third most common form of inflammatory arthritis. CPPD disease manifests in various clinical presentations, which often overlap with other types of arthritides. The crystals involved in CPPD disease are composed of calcium pyrophosphate dihydrate and commonly affect larger, weight-bearing joints, including the hips, knees, and shoulders. In some cases, calcium pyrophosphate (CPP) crystal deposits may be visible on imaging without any associated symptoms.[1] Due to its diverse presentation, CPPD is frequently misdiagnosed as other rheumatic conditions, including gout, rheumatoid arthritis, polymyalgia rheumatica, or even ankylosing spondylitis.[1][2]
The European Alliance of Associations for Rheumatology (EULAR) categorizes CPPD into 4 categories: (1) asymptomatic CPPD; (2) osteoarthritis with CPPD; (3) acute CPP crystal arthritis/pseudogout; (4) chronic CPP inflammatory crystal arthritis. Other rare types have been noted, including pseudo-polymyalgia rheumatica (pseudo-PMR), pseudo-neuropathic arthropathy, and tumoral CPPD.[3]
Briefly, the various types of CPPD present as follows:[3]
- Asymptomatic CPPD: This form may present as isolated hyaline or fibrocartilage calcifications (chondrocalcinosis) observed on plain x-ray or as osteoarthritis with CPP crystals without classic acute CPPD episodes.
- Osteoarthritis with CPPD: Many patients with CPPD also have degenerative arthritis, characterized by an unusual distribution similar to osteoarthritis, typically involving the knees, wrists, metacarpophalangeal joints, hips, shoulders, and ankles. This type can present with a gradual onset of pain and slow progressive joint destruction.
- Acute CPP crystal arthritis/pseudogout: Approximately 25% of patients present with the classic pseudogout presentation, characterized by acute, intermittent, and severe episodes of joint pain and swelling, accompanied by redness and tenderness similar to those of gout. Acute phase reactants may be elevated.
- Chronic CPP inflammatory crystal arthritis (previously referred to as pseudo-rheumatoid arthritis): This subtype affects approximately 25% of patients with CPPD. Presentation can involve chronic, symmetrical, deforming polyarthritis. The wrists and metacarpal joints are commonly affected, and patients may also develop carpal tunnel syndrome, synovial thickening, localised edema, and flexion contractures of the hands and wrists.
- Pseudo-polymyalgia rheumatica: Older patients with early morning stiffness and bilateral shoulder pain similar to polymyalgia rheumatica should also be considered for an atypical presentation of CPP arthritis. Involvement of proximal joints may be a feature of CPPD and has been reported in the literature.
- Pseudo-neuropathic arthropathy: Rarely, patients can present with severe destructive monoarthritis with evidence of joint destruction on radiographic imaging.
- Tumoral CPPD: This type is characterized by the accumulation of calcium foci and chondroid metaplasia, resulting in a radiographic appearance similar to a tumor.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
CPPD is believed to result from pathological formation and deposition of CPP crystals, which subsequently trigger an immune response.[1] CPP crystals are rod- or rhomboid-shaped, measure 1 to 22 μm in size, and display birefringence under polarized light.[4] The deposition of CPP crystals in hyaline or fibrocartilage is referred to as chondrocalcinosis, the precursor of CPPD.[5]
The mechanisms that lead to crystal deposition in cartilage and joints are yet to be clearly defined. Mutations of the ANKH and ENPP1 genes—both involved in cartilaginous phosphate metabolism—along with other genetic conditions, such as hypophosphatasia, or metabolic factors, including hypomagnesemia and hyperferritinemia, which lead to reduced alkaline phosphatase activity, are proposed underlying mechanisms.[1][5] CPPD is also commonly associated with age and osteoarthritis.[6] Other recognized risk factors include hemochromatosis, hyperparathyroidism, hypophosphatasia (a rare inherited bone disease), and hypomagnesemia.[2][7] Patients with Gitelman syndrome are also frequently affected, likely related to underlying hypomagnesemia.
Epidemiology
Approximately 30% to 50% of patients with CPPD are older than 85.[8] Men and women appear to be equally affected.[2][7][6]
Chondrocalcinosis has been frequently used as a surrogate for CPPD. The prevalence of chondrocalcinosis varies depending on the location of the joint, the imaging modality used, and the individual's ethnicity.[6][9][10] On plain radiographs, chondrocalcinosis is observed in 7.0% to 8.1% of knees, and in 10.0% to 10.4% of cases when the knees plus either the hand/wrist or the hip/symphysis pubis are involved.[11] An ultrasound study of patients with knee pain found that CPPD was present in 22% and 10% of patients in fibrocartilage and hyaline cartilage, respectively.[6]
A study found that the presence of cartilage calcification—another possible marker for CCPD—is 4% to 7% in the United States and Europe.[12] The low sensitivity of conventional radiography likely leads to an underestimation of CPPD prevalence.[1]
Pathophysiology
The pathophysiology of CPP disease is linked to an imbalance of inorganic pyrophosphate in the cartilage's extracellular matrix, which promotes its interaction with calcium and leads to the formation of calcium pyrophosphate crystals.[13] CPP crystals are commonly deposited in cartilaginous structures but can also be found in the fibrocartilaginous layers at the insertion sites of tendons and ligaments. The deposition of CPP crystals triggers an inflammatory cascade, activating the immune system and leading to synovitis and progressive joint damage. Tissue nonspecific alkaline phosphatase may contribute to the increased risk of osteoporotic fractures and cardiovascular events observed after acute episodes of CPP arthritis.[14] In severe cases associated with Gitelman disease, involvement of the axial skeleton may also occur.[15]
Histopathology
Histologically, the presence of weakly birefringent, double-refracting crystals on polarized light microscopy is diagnostic of CPPD disease. These crystals are rhomboid or parallelepipedal, as opposed to the strongly negatively birefringent, needle-shaped urate crystals of gout.[12][16]
History and Physical
Acute CPPD crystal arthritis typically presents as either acute monoarticular or oligoarticular arthritis. This condition is often characterized by the sudden onset of pain, warmth, swelling, and, in some cases, periarticular erythema. When a large joint is involved, systemic symptoms such as fever, chills, and malaise may also occur.[17] Although the knees are the most commonly affected joints, studies have shown that radiographic chondrocalcinosis is common in the wrists and hips, even in the absence of knee involvement.[18]
CPPD of the atlanto-occipital joint, also known as crowned dens syndrome, can cause periodic acute cervico-occipital pain accompanied by fever, neck stiffness, and laboratory evidence of inflammation.[19] Chronic CPPD crystal arthritis can present as persistent inflammatory polyarthritis or recurrent acute flares. The persistent inflammatory polyarthritis subtype often resembles rheumatoid arthritis or polymyalgia rheumatica. Some subtypes of CPPD, particularly the pseudo-neuropathic type, can lead to structural damage, particularly in the wrist and metacarpophalangeal joints, with clinical presentation often characterized by mechanical pain in the affected joint.[1] Clinical manifestations of CPPD disease may be atypical in the older population due to cognitive impairment and inflammation-induced delirium, which can make diagnosis more challenging.[1]
Compared to CPPD, primary osteoarthritis is more likely to affect the medial knee compartment, resulting in a varus deformity.[3] CPPD can also have overlapping symptoms with gout, which also affects the large joints; however, gout is much more likely to affect the first metatarsal joint (podagra) and other small joints of the metatarsals.
The first validated classification criteria for symptomatic CPPD were recently developed by the American College of Rheumatology and the EULAR in 2023 (see Table. Calcium Pyrophosphate Deposition Disease, Classification Criteria).[20] EULAR 2023 CPPD Guidelines. A patient is classified as having CPPD under the following conditions:
- They meet the entry criterion of having a history of at least 1 episode of joint pain, swelling, or tenderness.
- They do not meet any exclusion criteria (ie, symptoms are better explained by another diagnosis)
- They fulfill at least 1 sufficient criterion, such as clinical and radiographic evidence of crowned dens syndrome or the presence of CPP crystals in a patient with inflammatory arthritis
If these criteria are not met, CPPD can be defined based on a cumulative point system, with a total score greater than 56 indicating the diagnosis (see Table. CPPD Cumulative Point-Based Criteria).
Evaluation
Basic bloodwork should include a basic metabolic panel (including calcium, magnesium, and phosphate), parathyroid hormone level, iron studies, thyroid-stimulating hormone level, and uric acid level.[1]
Crystal identification in synovial fluid aspirates by compensated polarized light microscopy remains the gold standard for diagnosing CPP arthritis.[21] Given the invasive nature of synovial fluid analysis, the role of imaging continues to evolve in clinical practice. Commonly used imaging modalities for diagnosing CPPD include plain x-ray, computed tomography (CT), dual-energy computed tomography (DECT), and ultrasound.[22]
CCP deposits are found more commonly in fibrocartilage, such as in weight-supporting structures like the spine, pubic symphysis, and menisci, than in hyaline cartilage, such as in articular joints. Conventional radiography is the first-line imaging modality for identifying CPP calcification.[23] The classic findings on x-ray are linear and punctate densities in the hyaline/fibrous cartilage, synovial membranes, or tendons.[23] However, some studies have found that conventional radiography has a sensitivity of only about 40% for detecting clinically significant CPPD.[24]
Over the last decade, the ultrasound has been extensively used as a diagnostic modality for crystal arthropathies. This modality is more sensitive but less specific than conventional radiography.[22] Ultrasound findings are hyperechoic deposits of variable shape and size, localized within the fibrous/hyaline cartilage, that remain fixed or move along with the fibrous/hyaline cartilage during dynamic assessment and do not create posterior shadowing.[23]
Conventional computed tomography generally shows well-defined punctate or linear calcifications, less dense than cortical bone, within the fibrous/hyaline cartilage, synovial membranes, or tendons.[23]
DECT is considered the most sensitive imaging modality for detecting crystals based on their characteristic attenuation, described by its material-specific dual-energy gradient.[25] DECT has the potential to differentiate between different crystal deposits.[21] Findings indicating CPPD are punctate or linear calcifications less dense than cortical bone in the fibrous/hyaline cartilage, synovial membranes, or tendons with a dual-energy index between 0.016 and 0.036.[23]
Treatment / Management
Despite ongoing progress in clinical research on CPPD, no disease-modifying therapies have been approved to reduce the deposition of CPP crystals. The goal of treatment is largely based on decreasing inflammation, reducing the frequency and severity of symptoms, and stabilizing any underlying metabolic disease that may predispose patients to CPP deposition.[22]
The treatment of acute CPP arthritis has mostly been guided by the treatment of acute gout flares. In 2011, the EULAR recommended the use of nonsteroidal anti-inflammatory drugs, colchicine, and systemic or intra-articular corticosteroids depending on the patient's age and other comorbidities.[26] In 2023, the COLCHICORT trial recommended initiating treatment of acute CPP crystal arthritis with a daily dose of 30 mg prednisone as first-line therapy.[27] When colchicine is used, early administration (within 12 hours of arthritis onset) is crucial. For chronic CPP crystal inflammatory arthritis, daily colchicine is the preferred first-line treatment, whereas methotrexate and tocilizumab are considered second-line options.[28](A1)
Differential Diagnosis
The manifestations of CPPD can mimic several other rheumatological conditions and have different phenotypes. About one-fourth of patients experience acute CPP arthritis, often called pseudogout, whereas chronic CPP arthritis, previously referred to as pseudo-rheumatoid arthritis, affects approximately another 25% of patients. Asymptomatic CPPD may present as chondrocalcinosis on plain radiographs without apparent clinical consequences. A significant portion of patients with CPPD have associated degenerative arthritis, most commonly osteoarthritis. A key distinguishing feature in knee involvement is that primary osteoarthritis predominantly affects the medial compartment, whereas the lateral compartment is more frequently involved in CPPD-related osteoarthritis. Pseudo-polymyalgia rheumatica is a term used for the atypical presentation of CPPD in older adults with early morning stiffness and bilateral shoulder pain. Pseudo-neuropathic arthropathy and tumoral CPPD are some other rare presentations of CPPD.[3]
Pertinent Studies and Ongoing Trials
To date, there are no specific outcomes agreed on for the assessment of CPPD disease.[1] A scoping review by the OMERACT CPPD working group identified imaging manifestations, joint pain, and response to treatment domains as the most commonly reported outcomes.[29]
The field of CPPD disease is rapidly evolving. Future research should focus on the genetics and metabolomics of sporadic CPPD disease, as well as the incidence and prevalence of CPPD disease and its various phenotypes. The imaging field is evolving, underscoring the need for continued efforts to standardize imaging protocols. Therapeutic studies are needed to explore the efficacy of existing IL-1 and IL-6 inhibitors, as well as novel agents, including inflammasome inhibitors and other new targets, in reducing CPP crystal-induced inflammation.[1]
Prognosis
Acute attacks of CPP crystal arthritis are generally self-limiting, typically lasting 7 to 10 days. Patients with chronic CPP inflammatory arthritis experience recurrent flare-ups, with symptoms that frequently overlap those of rheumatoid arthritis.[17] Some patients may develop tenosynovitis leading to carpal or cubital tunnel syndrome.[12][17]
Acute CPP crystal arthritis causes severe joint pain that temporarily restricts movements and can lead to significant disability, often requiring bed rest or limiting daily activities. This condition may also negatively affect mental health. Chronic CPPD disease leads to reduced mobility, frequently necessitating walking aids and increasing care needs. Pain often disrupts sleep and limits exercise, social interactions, leisure activities, and work.[1]
Complications
The presence of CPP crystals triggers an inflammatory response, which can lead to atypical presentations and complications. In a rare scenario, biopsy of tophi-like nodules, typically found only in urate-related gout, revealed CPPD.[30] Tumoral CPPD, a rare clinical phenotype of CPPD, may present as CPP crystals in the spine, leading to ossification of the ligamentum flavum.[31]
Deterrence and Patient Education
Patients with CPPD should be educated about potential triggers of arthritic flares, including surgical procedures and trauma.[8] Patients who develop CPPD at a younger age should be screened for underlying metabolic abnormalities, such as hemochromatosis.[11] Providing education on early diagnosis and strategies to prevent joint damage is essential.
Enhancing Healthcare Team Outcomes
Patients with calcium phosphate deposition disease are at risk for serious disability. Although disease-modifying therapy is not available, early treatment with currently available treatment may help reduce morbidity and mortality. The care of patients with this disease necessitates a collaborative approach among healthcare professionals to ensure patient-centered care and improve overall outcomes. Rheumatologists, primary care providers, advanced practitioners, nurses, pharmacists, and other healthcare professionals involved in the care of these patients should possess the essential clinical skills and knowledge to diagnose and manage this disease accurately. This expertise includes expertise in recognizing the varied clinical presentations, and rheumatologists capable of performing arthrocentesis are essential.
A strategic approach is equally crucial, involving evidence-based strategies to optimize treatment plans and minimize adverse effects. Ethical considerations should guide decision-making, ensuring informed consent and respecting patient autonomy in treatment choices. Each healthcare professional should be aware of their responsibilities and contribute their unique expertise to the patient's care plan, fostering a multidisciplinary approach. Effective interprofessional communication is paramount, allowing seamless information exchange and collaborative decision-making among the team members. Care coordination plays a pivotal role in ensuring that the patient's journey from diagnosis to treatment and follow-up is well-managed, minimizing errors and enhancing patient safety. By embracing these principles of skill, strategy, ethics, responsibilities, interprofessional communication, and care coordination, healthcare professionals can deliver patient-centered care, ultimately improving patient outcomes and enhancing team performance in the management of calcium pyrophosphate deposition disease.
Media
(Click Image to Enlarge)
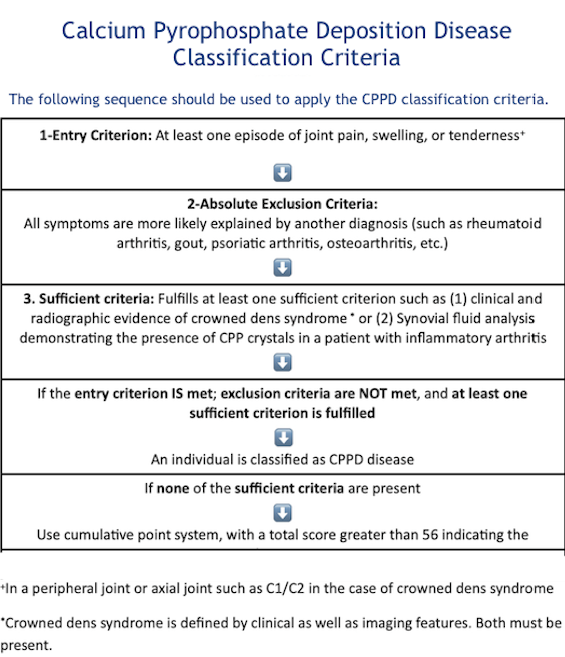
Calcium Pyrophosphate Deposition Disease, Classification Criteria. This table outlines the classification criteria for calcium pyrophosphate deposition (CPPD) disease, which requires a history of joint pain, swelling, or tenderness, along with imaging or crystal evidence of CPPD to confirm diagnosis.
Abbreviations: CPP: calcium pyrophosphate; CPPD: calcium pyrophosphate deposition.
Adapted from: Abhishek A, Tedeschi SK, Pascart T, et al. The 2023 ACR/EULAR classification criteria for calcium pyrophosphate deposition disease. Ann Rheum Dis. 2023;82(10):1248-1257. doi: 10.1136/ard-2023-224575.
(Click Image to Enlarge)
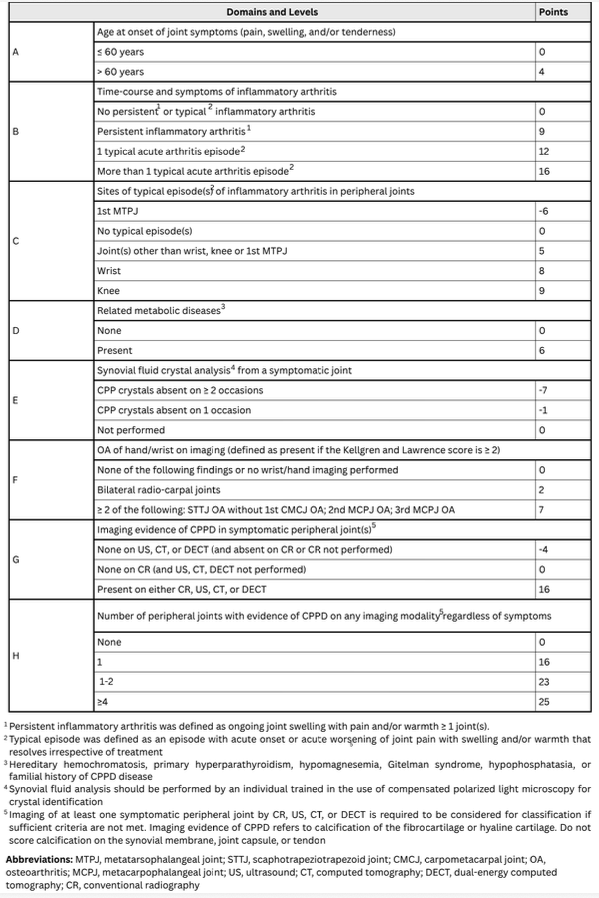
CPPD Cumulative Point-Based Criteria. Items may be scored if they have been present at any point during the patient’s lifetime. If multiple items in one domain apply, use the one with the highest score. Imaging of at least one symptomatic joint using CR, US, CT, or DECT is required.
Adapted from: Abhishek A, Tedeschi SK, Pascart T, et al. The 2023 ACR/EULAR classification criteria for calcium pyrophosphate deposition disease. Ann Rheum Dis. 2023;82(10):1248-1257. doi: 10.1136/ard-2023-224575.
References
Pascart T, Filippou G, Lioté F, Sirotti S, Jauffret C, Abhishek A. Calcium pyrophosphate deposition disease. The Lancet. Rheumatology. 2024 Nov:6(11):e791-e804. doi: 10.1016/S2665-9913(24)00122-X. Epub 2024 Jul 29 [PubMed PMID: 39089298]
Krekeler M, Baraliakos X, Tsiami S, Braun J. High prevalence of chondrocalcinosis and frequent comorbidity with calcium pyrophosphate deposition disease in patients with seronegative rheumatoid arthritis. RMD open. 2022 Jun:8(2):. doi: 10.1136/rmdopen-2022-002383. Epub [PubMed PMID: 35701012]
Cowley S, McCarthy G. Diagnosis and Treatment of Calcium Pyrophosphate Deposition (CPPD) Disease: A Review. Open access rheumatology : research and reviews. 2023:15():33-41. doi: 10.2147/OARRR.S389664. Epub 2023 Mar 22 [PubMed PMID: 36987530]
Jarraya M, Roemer F, Kwoh CK, Guermazi A. Crystal arthropathies and osteoarthritis-where is the link? Skeletal radiology. 2023 Nov:52(11):2037-2043. doi: 10.1007/s00256-022-04246-8. Epub 2022 Dec 20 [PubMed PMID: 36538066]
Manigold T. [Calcium pyrophosphate deposition (CPPD) disease - more than just "pseudogout"]. Therapeutische Umschau. Revue therapeutique. 2024 Sep:81(5):156-159. doi: 10.23785/TU.2024.05.003. Epub [PubMed PMID: 39508814]
Cipolletta E, Francioso F, Smerilli G, Di Battista J, Filippucci E. Ultrasound reveals a high prevalence of CPPD in consecutive patients with knee pain. Clinical rheumatology. 2024 Jan:43(1):435-441. doi: 10.1007/s10067-023-06805-3. Epub 2023 Nov 17 [PubMed PMID: 37975949]
Abhishek A, Doherty M. Epidemiology of calcium pyrophosphate crystal arthritis and basic calcium phosphate crystal arthropathy. Rheumatic diseases clinics of North America. 2014 May:40(2):177-91. doi: 10.1016/j.rdc.2014.01.002. Epub 2014 Feb 20 [PubMed PMID: 24703342]
Higgins PA. Gout and pseudogout. JAAPA : official journal of the American Academy of Physician Assistants. 2016 Mar:29(3):50-2. doi: 10.1097/01.JAA.0000475472.40251.58. Epub [PubMed PMID: 26914781]
Richette P, Bardin T, Doherty M. An update on the epidemiology of calcium pyrophosphate dihydrate crystal deposition disease. Rheumatology (Oxford, England). 2009 Jul:48(7):711-5. doi: 10.1093/rheumatology/kep081. Epub 2009 Apr 27 [PubMed PMID: 19398486]
Abhishek A. Calcium pyrophosphate deposition disease: a review of epidemiologic findings. Current opinion in rheumatology. 2016 Mar:28(2):133-9. doi: 10.1097/BOR.0000000000000246. Epub [PubMed PMID: 26626724]
Level 3 (low-level) evidenceAbhishek A, Doherty M. Update on calcium pyrophosphate deposition. Clinical and experimental rheumatology. 2016 Jul-Aug:34(4 Suppl 98):32-8 [PubMed PMID: 27586801]
Yamamura M. Acute CPP Crystal Arthritis Causing Carpal Tunnel Syndrome. Internal medicine (Tokyo, Japan). 2018 Oct 1:57(19):2767-2768. doi: 10.2169/internalmedicine.0791-18. Epub 2018 May 18 [PubMed PMID: 29780133]
Parperis K, Papachristodoulou E, Kakoullis L, Rosenthal AK. Management of calcium pyrophosphate crystal deposition disease: A systematic review. Seminars in arthritis and rheumatism. 2021 Feb:51(1):84-94. doi: 10.1016/j.semarthrit.2020.10.005. Epub 2020 Dec 21 [PubMed PMID: 33360232]
Level 1 (high-level) evidenceSirotti S, Scanu A, Pascart T, Niessink T, Maroni P, Lombardi G, Filippou G. Calcium Pyrophosphate Crystal Formation and Deposition: Where Do we Stand and What Does the Future hold? Current rheumatology reports. 2024 Oct:26(10):354-365. doi: 10.1007/s11926-024-01161-w. Epub 2024 Aug 1 [PubMed PMID: 39088093]
Chotard E, Blanchard A, Ostertag A, Latourte A, Gailly G, Frochot V, Lioté F, Bousson V, Richette P, Bardin T, Vargas-Poussou R, Ea HK. Calcium pyrophosphate crystal deposition in a cohort of 57 patients with Gitelman syndrome. Rheumatology (Oxford, England). 2022 May 30:61(6):2494-2503. doi: 10.1093/rheumatology/keab578. Epub [PubMed PMID: 34508565]
López-Navarro JM, Sandoval-Lopez DA, Popovic P, Karantzoulis V, Bittar Z, Santos E, Vazifehdan F. Lumbar Intraspinal Calcium Pyrophosphate Deposition: A Comprehensive Case Study. Journal of central nervous system disease. 2025:17():11795735251347335. doi: 10.1177/11795735251347335. Epub 2025 Jun 6 [PubMed PMID: 40488138]
Level 3 (low-level) evidenceRosales-Alexander JL, Balsalobre Aznar J, Magro-Checa C. Calcium pyrophosphate crystal deposition disease: diagnosis and treatment. Open access rheumatology : research and reviews. 2014:6():39-47 [PubMed PMID: 27790033]
Adinolfi A, Sirotti S, Sakellariou G, Cipolletta E, Filippucci E, Porta F, Zanetti A, Ughi N, Sarzi-Puttini P, Scirè CA, Keen H, Pineda C, Terslev L, D'Agostino MA, Filippou G. Which are the most frequently involved peripheral joints in calcium pyrophosphate crystal deposition at imaging? A systematic literature review and meta-analysis by the OMERACT ultrasound - CPPD subgroup. Frontiers in medicine. 2023:10():1131362. doi: 10.3389/fmed.2023.1131362. Epub 2023 Mar 9 [PubMed PMID: 36968827]
Level 1 (high-level) evidenceFerrone C, Andracco R, Cimmino MA. Calcium pyrophosphate deposition disease: clinical manifestations. Reumatismo. 2012 Jan 19:63(4):246-52. doi: 10.4081/reumatismo.2011.246. Epub 2012 Jan 19 [PubMed PMID: 22303531]
Abhishek A, Tedeschi SK, Pascart T, Latourte A, Dalbeth N, Neogi T, Fuller A, Rosenthal A, Becce F, Bardin T, Ea HK, Filippou G, Fitzgerald J, Iagnocco A, Lioté F, McCarthy GM, Ramonda R, Richette P, Sivera F, Andrés M, Cipolletta E, Doherty M, Pascual E, Perez-Ruiz F, So A, Jansen TL, Kohler MJ, Stamp LK, Yinh J, Adinolfi A, Arad U, Aung T, Benillouche E, Bortoluzzi A, Dau J, Maningding E, Fang MA, Figus FA, Filippucci E, Haslett J, Janssen M, Kaldas M, Kimoto M, Leamy K, Navarro GM, Sarzi-Puttini P, Scirè C, Silvagni E, Sirotti S, Stack JR, Truong L, Xie C, Yokose C, Hendry AM, Terkeltaub R, Taylor WJ, Choi HK. The 2023 ACR/EULAR classification criteria for calcium pyrophosphate deposition disease. Annals of the rheumatic diseases. 2023 Oct:82(10):1248-1257. doi: 10.1136/ard-2023-224575. Epub 2023 Jul 26 [PubMed PMID: 37495237]
Pascart T, Norberciak L, Legrand J, Becce F, Budzik JF. Dual-energy computed tomography in calcium pyrophosphate deposition: initial clinical experience. Osteoarthritis and cartilage. 2019 Sep:27(9):1309-1314. doi: 10.1016/j.joca.2019.05.007. Epub 2019 May 27 [PubMed PMID: 31146015]
Flood R, Stack J, McCarthy G. An Update on the Diagnosis and Management of Calcium Crystal Disease. Current rheumatology reports. 2023 Aug:25(8):145-151. doi: 10.1007/s11926-023-01106-9. Epub 2023 May 30 [PubMed PMID: 37249830]
Tedeschi SK, Becce F, Pascart T, Guermazi A, Budzik JF, Dalbeth N, Filippou G, Iagnocco A, Kohler MJ, Laredo JD, Smith SE, Simeone FJ, Yinh J, Choi H, Abhishek A. Imaging Features of Calcium Pyrophosphate Deposition Disease: Consensus Definitions From an International Multidisciplinary Working Group. Arthritis care & research. 2023 Apr:75(4):825-834. doi: 10.1002/acr.24898. Epub 2022 Nov 23 [PubMed PMID: 35439343]
Level 3 (low-level) evidenceMiksanek J, Rosenthal AK. Imaging of calcium pyrophosphate deposition disease. Current rheumatology reports. 2015 Mar:17(3):20. doi: 10.1007/s11926-015-0496-1. Epub [PubMed PMID: 25761927]
Sanghavi PS, Jankharia BG. Applications of dual energy CT in clinical practice: A pictorial essay. The Indian journal of radiology & imaging. 2019 Jul-Sep:29(3):289-298. doi: 10.4103/ijri.IJRI_241_19. Epub 2019 Oct 30 [PubMed PMID: 31741598]
Zhang W, Doherty M, Pascual E, Barskova V, Guerne PA, Jansen TL, Leeb BF, Perez-Ruiz F, Pimentao J, Punzi L, Richette P, Sivera F, Uhlig T, Watt I, Bardin T. EULAR recommendations for calcium pyrophosphate deposition. Part II: management. Annals of the rheumatic diseases. 2011 Apr:70(4):571-5. doi: 10.1136/ard.2010.139360. Epub 2011 Jan 20 [PubMed PMID: 21257614]
Pascart T, Robinet P, Ottaviani S, Leroy R, Segaud N, Pacaud A, Grandjean A, Luraschi H, Rabin T, Deplanque X, Maciejasz P, Visade F, Mackowiak A, Baclet N, Maréchaux S, Lefebvre A, Budzik JF, Bardin T, Richette P, Norberciak L, Ducoulombier V, Houvenagel E. Evaluating the safety and short-term equivalence of colchicine versus prednisone in older patients with acute calcium pyrophosphate crystal arthritis (COLCHICORT): an open-label, multicentre, randomised trial. The Lancet. Rheumatology. 2023 Sep:5(9):e523-e531. doi: 10.1016/S2665-9913(23)00165-0. Epub 2023 Aug 8 [PubMed PMID: 38251496]
Level 1 (high-level) evidenceDamart J, Filippou G, Andrès M, Cipolletta E, Sirotti S, Carboni D, Filippucci E, Diez P, Abhishek A, Latourte A, Ea HK, Ottaviani S, Letarouilly JG, Desbarbieux R, Graf S, Norberciak L, Richette P, Pascart T. Retention, safety and efficacy of off-label conventional treatments and biologics for chronic calcium pyrophosphate crystal inflammatory arthritis. Rheumatology (Oxford, England). 2024 Feb 1:63(2):446-455. doi: 10.1093/rheumatology/kead228. Epub [PubMed PMID: 37216917]
Cai K, Fuller A, Hensey O, Grossberg D, Christensen R, Shea B, Singh JA, Abhishek A, Tedeschi S, Dalbeth N. Outcome domains reported in calcium pyrophosphate deposition studies: A scoping review by the OMERACT CPPD working group. Seminars in arthritis and rheumatism. 2020 Aug:50(4):719-727. doi: 10.1016/j.semarthrit.2020.05.015. Epub 2020 May 30 [PubMed PMID: 32521326]
Level 2 (mid-level) evidenceShen G, Su M, Liu B, Kuang A. A Case of Tophaceous Pseudogout on 18F-FDG PET/CT Imaging. Clinical nuclear medicine. 2019 Feb:44(2):e98-e100. doi: 10.1097/RLU.0000000000002308. Epub [PubMed PMID: 30325826]
Level 3 (low-level) evidenceMuthukumar N, Karuppaswamy U. Tumoral calcium pyrophosphate dihydrate deposition disease of the ligamentum flavum. Neurosurgery. 2003 Jul:53(1):103-8; discussion 108-9 [PubMed PMID: 12823879]
Level 2 (mid-level) evidence