 Anatomy, Bony Pelvis and Lower Limb: Posterior Tibial Artery
Anatomy, Bony Pelvis and Lower Limb: Posterior Tibial Artery
Introduction
The leg is divided into 4 compartments: anterior, lateral, superficial posterior, and deep posterior. The anterior compartment contains the tibialis anterior, extensor hallucis longus, extensor digitorum longus, and fibularis (peroneus) tertius muscles. Innervation arises from the deep fibular (peroneal) nerve, while arterial supply derives from the anterior tibial artery (ATA). Anterior compartment muscles serve primarily as dorsiflexors of the ankle and extensors of the toes.
The lateral compartment contains the fibularis (peroneus) longus and brevis muscles, which receive innervation from the superficial fibular (peroneal) nerve. Muscular branches from the fibular (peroneal) artery supply the lateral compartment, although the artery itself is a structure of the posterior compartment. Lateral compartment muscles are primarily responsible for foot eversion and contribute minimally to ankle plantarflexion.
The superficial posterior compartment contains the gastrocnemius, soleus, and plantaris muscles. The deep posterior compartment contains the tibialis posterior, flexor digitorum longus, and flexor hallucis longus muscles. Arterial supply to both posterior compartments arises from the posterior tibial artery (PTA), while innervation is provided by the tibial nerve. These neurovascular structures course through the deep posterior compartment. Primary functions of the posterior compartment muscles include ankle plantarflexion and toe flexion.
Lower extremity arteries are susceptible to several pathologies, including atherosclerotic plaque formation, compartment syndrome, trauma, and, rarely, aneurysm. Only 33 cases of true infrapopliteal arterial aneurysms have been documented, 12 of which involve the PTA.[1] PTA injury during flap harvest or leg reconstruction may compromise plantar perfusion and delay wound healing. Familiarity with the anatomy and function of this blood vessel aids clinical evaluation of lower limb perfusion and procedural safety.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The arterial supply to the 4 compartments of the lower limb originates from the common femoral artery, a branch of the external iliac artery, which ultimately divides into deep and superficial branches. The deep branch, the profunda femoris artery, supplies the posterior thigh through the medial circumflex femoral and lateral circumflex femoral arteries. The superficial femoral artery continues inferiorly, passes through the adductor hiatus, and enters the popliteal fossa, where the vessel becomes the popliteal artery posterior to the knee. Near the distal extent of the popliteal fossa, the popliteal artery divides into the ATA and the tibioperoneal (tibiofibular) trunk. The tibioperoneal trunk subsequently bifurcates approximately 2.5 cm distal to its origin into the fibular artery and the PTA.
The PTA is the largest terminal branch of the popliteal artery (see Image. Arterial Supply of the Posterior Leg). The vessel courses with the tibial nerve through the deep posterior compartment of the leg along the fascial plane separating the deep and superficial posterior compartments. At the level of the ankle, the PTA assumes a more superficial course and is palpable posterior to the medial malleolus as the vessel passes through the tarsal tunnel. Distal branches include the posterior medial malleolar artery and the artery of the tarsal canal, the latter serving as the dominant arterial supply to the talar body. Within the foot, the PTA bifurcates into the medial and lateral plantar arteries after crossing the sustentaculum tali.[2]
Embryology
Lower limb buds begin to form approximately 4 to 5 weeks after fertilization as lateral plate mesoderm migrates into the limb bud region and condenses along the central axis to form the vascular and skeletal components of the lower limb. Multiple factors regulate the development of the limb bud vasculature and musculature, including retinoic acid, sonic hedgehog (Shh), HOX genes, the apical ectodermal ridge, and the zone of polarizing activity. Retinoic acid functions as a global organizing gradient and initiates transcription factor production required for regional differentiation and limb polarization. The apical ectodermal ridge produces fibroblast growth factor, which promotes limb bud outgrowth through stimulation of mitosis. The zone of polarizing activity produces Shh, which directs the organization of the limb bud along the anterior-posterior axis. Shh subsequently activates specific HOX genes—HOXD9, HOXD10, HOXD11, HOXD12, and HOXD13—which are essential for limb polarization and regional specification.[3]
The earliest arterial supply to the lower limb bud consists of the axis artery and the terminal plexus, both of which arise from the umbilical artery. The axis artery subsequently gives rise to branches that form the ATA and the PTA. The ATA continues distally as the dorsalis pedis artery, whereas the PTA gives rise to the medial and lateral plantar arteries. A second arterial channel arises independently from the external iliac artery and forms the femoral artery of the lower limb, which subsequently establishes continuity with the axis artery. Regression occurs in most of the axis artery during development. Persistent segments contribute to the formation of the inferior gluteal artery, sciatic artery, proximal portion of the popliteal artery, and distal portion of the fibular artery.[4]
Blood Supply and Lymphatics
Venous drainage of the lower leg parallels arterial supply within the 4 fascial compartments. The anterior compartment drains via the anterior tibial veins, the lateral compartment via the fibular veins, and the superficial and deep posterior compartments via the posterior tibial and fibular veins, which converge into the popliteal vein. Venous return is supported by deep and superficial lymphatic channels that accompany major vessels and drain toward popliteal and inguinal nodes. Compartmental organization facilitates efficient venous-lymphatic coupling but also predisposes to congestion in compartment syndrome.
Physiologic Variants
Anatomical variations of the PTA most commonly result from alterations in popliteal artery branching. The 3 most frequently reported branching variations include a high origin of the ATA, trifurcation into the ATA, PTA, and fibular artery, and a hypoplastic or aplastic PTA. Reported frequencies and relative order of these variations vary slightly among literature reviews. However, all 3 consistently rank among the most common anatomical variants.[5]
Surgical Considerations
Lower limb arteries are particularly susceptible to atherosclerotic plaque accumulation and peripheral arterial disease (PAD). This condition involves progressive luminal narrowing resulting from atherosclerotic plaque deposition, leading to reduced arterial blood flow.[6][7] Initial PAD management includes lifestyle modification and pharmacologic therapy. Failure of conservative management may necessitate surgical intervention.[8] Common procedures for PAD include angioplasty, thrombectomy, and bypass surgery. PTA bypass surgery may be performed in cases of critical limb ischemia, typically characterized by rest pain and tissue loss in the form of ulceration, gangrene, or both.[9]
Surgical intervention involving the PTA also includes repair of PTA aneurysms. Aneurysms of the infrapopliteal region are extremely rare, with most cases associated with infectious or inflammatory processes.[10] Among infrapopliteal vessels, only 12 cases of true PTA aneurysmal dilation have been reported.[11][12] Management strategies for these aneurysms range from conservative treatment to surgical excision. However, standard management remains undefined due to the limited number of reported cases. Surgical excision with reconstruction via primary repair or interposition vein graft is the most frequently reported treatment approach in the literature.
Clinical Significance
The PTA becomes superficial and is readily palpable posterior to the medial malleolus. This anatomical accessibility supports its use in physical examination for assessment of peripheral vascular disease, which affects approximately 12% of the population. Palpation is performed by encircling the heel and applying pressure just posterior to the medial malleolus. A diminished or absent PTA pulse may indicate vascular insufficiency.[13]
The PTA may be involved in compartment syndrome. This condition may occur as an acute complication of blunt force injury or trauma, or a chronic exertional syndrome associated with repetitive physical exertion. Lower limb muscle groups are organized into compartments formed by strong, inelastic fascial membranes. Compartment syndrome develops when increased pressure within a fascial compartment compromises tissue perfusion and function. The posterior compartments contain muscles responsible for ankle plantarflexion and toe flexion, with innervation provided by the tibial nerve and vascular supply provided by the PTA. Increased pressure within the posterior compartment may result in plantar paresthesias, weakness of toe flexion, and pain on passive toe extension.[14] Compartment syndrome is a medical emergency requiring fasciotomy of the affected compartment.
PTA aneurysms, although rare, have been reported. False aneurysms (pseudoaneurysms) occur more frequently and are commonly associated with trauma. True aneurysms typically arise secondary to infectious or inflammatory processes and may present as an asymptomatic mass posterior to the ankle, proximal to the medial malleolus. Doppler ultrasonography may be used to confirm the presence of a true aneurysm. Only 12 cases of true PTA aneurysms have been reported. Consequently, no standardized treatment approach has been established. Published literature recommends early diagnosis and surgical management, typically via excision, to prevent further complications.
Other Issues
Traumatic Injury of the Posterior Tibial Artery
The PTA is vulnerable to injury during below-knee and ankle trauma, particularly in medial malleolar, posterior malleolar, and distal tibial fractures due to the artery’s close anatomical relationship to the posteromedial tibia and tarsal tunnel.[15] High-energy trauma, open fractures, crush injuries, fracture displacement, and delayed vascular assessment increase the risk of arterial compromise. Mechanisms of injury include direct laceration, thrombosis, compression, or iatrogenic ligation during surgical repair. Potential complications include acute limb ischemia, pseudoaneurysm formation, impaired distal perfusion, delayed wound healing, and graft failure following revascularization.[16]
Posterior Tibial Artery and Perforator Flaps
PTA flaps are axial-pattern fasciocutaneous flaps based on the PTA and its venae comitantes, typically harvested as pedicled or propeller configurations for coverage of distal leg, ankle, heel, and medial hindfoot defects. PTA perforator flaps are perforator-based variants that preserve the main PTA and rely on septocutaneous or musculocutaneous perforators arising from this vessel.[17][18] PTA perforator flaps reduce donor-site morbidity and maintain primary limb perfusion but require precise perforator identification and meticulous intramuscular dissection. Both flap types need adequate inflow through a patent PTA, competent venous drainage, and reliable perforator anatomy, often evaluated preoperatively using Doppler ultrasonography or computed tomography angiography.[19]
Vascular compromise, including PAD, diabetes mellitus, crush or degloving injury, venous congestion, and prior trauma, increases the risk of failure of these flaps. Anatomical variation in perforator number, caliber, or branching pattern may limit flap reach, reduce perfusion reliability, or result in partial or complete flap necrosis. Recent literature emphasizes careful patient selection and individualized vascular planning to optimize outcomes and minimize ischemic complications.
Media
(Click Image to Enlarge)
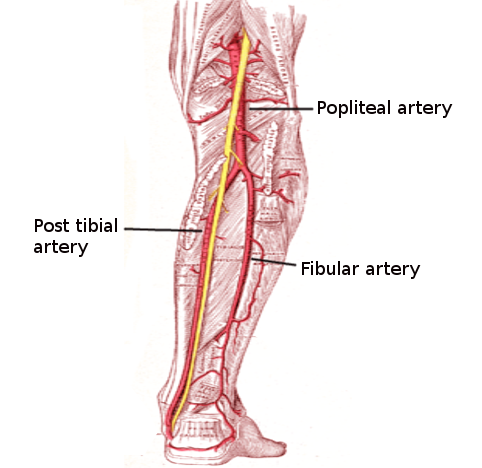
Arterial Supply of the Posterior Leg. This anatomical diagram illustrates the primary vascular pathways of the lower limb, originating from the popliteal artery as it passes through the popliteal fossa. The image highlights the bifurcation into the posterior tibial artery, which descends medially toward the ankle, and the fibular artery, which branches to supply the lateral compartment of the leg.
Contributed by S Bhimji, MD
References
Tshomba Y, Papa M, Marone EM, Kahlberg A, Rizzo N, Chiesa R. A true posterior tibial artery aneurysm--a case report. Vascular and endovascular surgery. 2006 May-Jun:40(3):243-9 [PubMed PMID: 16703214]
Level 3 (low-level) evidenceChmielewski P, Warchoł Ł, Gala-Błądzińska A, Mróz I, Walocha J, Malczak M, Jaworek J, Mizia E, Walocha E, Depukat P, Bachul P, Bereza T, Kurzydło W, Gach-Kuniewicz B, Mazur M, Tomaszewski K. Blood vessels of the shin - posterior tibial artery - anatomy - own studies and review of the literature. Folia medica Cracoviensia. 2016:56(3):5-9 [PubMed PMID: 28275266]
Mróz I, Kielczewski S, Pawlicki D, Kurzydło W, Bachul P, Konarska M, Bereza T, Walocha K, Kaythampillai LN, Depukat P, Pasternak A, Bonczar T, Chmielewski P, Mizia E, Skrzat J, Mazur M, Warchoł Ł, Tomaszewski K. Blood vessels of the shin - anterior tibial artery - anatomy and embryology - own studies and review of the literature. Folia medica Cracoviensia. 2016:56(1):33-47 [PubMed PMID: 27513837]
Gros J, Tabin CJ. Vertebrate limb bud formation is initiated by localized epithelial-to-mesenchymal transition. Science (New York, N.Y.). 2014 Mar 14:343(6176):1253-6. doi: 10.1126/science.1248228. Epub [PubMed PMID: 24626928]
Level 3 (low-level) evidenceDay CP, Orme R. Popliteal artery branching patterns -- an angiographic study. Clinical radiology. 2006 Aug:61(8):696-9 [PubMed PMID: 16843754]
Level 2 (mid-level) evidenceDing C, Chai Q, Zhu J, Liu Y, Zhou K, Du Y, Cui J, Li L, Zhang W, Chen L. Perioperative alteration of posterior tibial artery perfusion by contrast-enhanced ultrasound in patients with peripheral artery disease after endovascular therapy. Quantitative imaging in medicine and surgery. 2025 Dec 1:15(12):12257-12266. doi: 10.21037/qims-2025-426. Epub 2025 Nov 21 [PubMed PMID: 41367733]
Level 2 (mid-level) evidencePolonsky TS, McDermott MM. Lower Extremity Peripheral Artery Disease Without Chronic Limb-Threatening Ischemia: A Review. JAMA. 2021 Jun 1:325(21):2188-2198. doi: 10.1001/jama.2021.2126. Epub [PubMed PMID: 34061140]
Olin JW, Sealove BA. Peripheral artery disease: current insight into the disease and its diagnosis and management. Mayo Clinic proceedings. 2010 Jul:85(7):678-92. doi: 10.4065/mcp.2010.0133. Epub [PubMed PMID: 20592174]
El-Sayed HF. Bypass surgery for lower extremity limb salvage: vein bypass. Methodist DeBakey cardiovascular journal. 2012 Oct-Dec:8(4):37-42 [PubMed PMID: 23342187]
Sagar J, Button M. Posterior tibial artery aneurysm: a case report with review of literature. BMC surgery. 2014 Jun 16:14():37. doi: 10.1186/1471-2482-14-37. Epub 2014 Jun 16 [PubMed PMID: 24934412]
Level 3 (low-level) evidenceSinjeri D, Papeš D, Lovaković J, Antabak A. Posterior tibial artery pseudoaneurysm after titanium elastic nailing for tibial shaft fracture in a 7-year-old boy. Acta chirurgica Belgica. 2026 Feb:126(1):15-17. doi: 10.1080/00015458.2025.2605480. Epub 2025 Dec 20 [PubMed PMID: 41404826]
Crisp J, Ahmad M, Crockett S, Mohamed A, Hamady M, Bernstein O, Shalhoub J. Spontaneous bilateral superficial femoral artery pseudoaneurysms and a unilateral posterior tibial artery aneurysm in an immunocompromised patient. Clinical case reports. 2024 Mar:12(3):e8686. doi: 10.1002/ccr3.8686. Epub 2024 Mar 20 [PubMed PMID: 38515996]
Level 3 (low-level) evidenceWalker HK, Hall WD, Hurst JW, Hill RD, Smith RB III. Examination of the Extremities: Pulses, Bruits, and Phlebitis. Clinical Methods: The History, Physical, and Laboratory Examinations. 1990:(): [PubMed PMID: 21250191]
Mabvuure NT, Malahias M, Hindocha S, Khan W, Juma A. Acute compartment syndrome of the limbs: current concepts and management. The open orthopaedics journal. 2012:6():535-43. doi: 10.2174/1874325001206010535. Epub 2012 Nov 30 [PubMed PMID: 23248724]
Croman M, Lamberton T, Covington A, Keeley JA. Outcomes Following Below Knee Arterial Trauma. The American surgeon. 2023 Oct:89(10):4045-4049. doi: 10.1177/00031348231175502. Epub 2023 May 13 [PubMed PMID: 37177882]
Kim HJ, Hwang D. Posterior Tibial Artery Pseudoaneurysm Following Thrombectomy in a Patient with Traumatic Tibiofibular Fracture. Vascular specialist international. 2023 Mar 27:39():4. doi: 10.5758/vsi.230015. Epub 2023 Mar 27 [PubMed PMID: 36970760]
Perry WC, Masadeh S, Thione A. The Distally Based Posterior Tibial Artery Flap. Clinics in podiatric medicine and surgery. 2020 Oct:37(4):671-680. doi: 10.1016/j.cpm.2020.05.003. Epub 2020 Aug 13 [PubMed PMID: 32919597]
Gupta S, Gupta P, Khichar P, Mohammad A, Escandón JM, Kalra S. Perforator propeller flaps for lower extremity soft-tissue defect reconstruction: Shortening the learning curve. Journal of clinical orthopaedics and trauma. 2022 Apr:27():101831. doi: 10.1016/j.jcot.2022.101831. Epub 2022 Mar 10 [PubMed PMID: 35296056]
Agrawal NK, Bhattacharya V, Dubepuria R. Radiological Evaluation of Postsurgical Course of Perforators in Retrograde Posterior Tibial Fasciocutaneous Flaps for Distal Leg and Foot Defects. Indian journal of plastic surgery : official publication of the Association of Plastic Surgeons of India. 2021 Sep:54(3):272-277. doi: 10.1055/s-0041-1734568. Epub 2021 Sep 2 [PubMed PMID: 34667510]