Introduction
Drug-induced pigmentation (DIP) denotes abnormal cutaneous pigmentation resulting from exposure to specific medications through distinct pathophysiologic mechanisms. Hyperpigmentation comprises darkening of the skin relative to its baseline color. Numerous pharmacologic classes have been associated with pigmentation, including cytotoxic agents, analgesics, anticoagulants, antimicrobials, antivirals, antiarrhythmics, and heavy metals. Mechanisms implicated in DIP include chronic or acute inflammation leading to postinflammatory pigmentary alteration, stimulation of melanocytes with increased melanin synthesis, and, most frequently, direct deposition of the drug or its metabolites within the dermis or epidermis. Histopathologic findings are typically nonspecific and vary according to the mechanism involved.
Diagnosis of DIP requires a high index of clinical suspicion, detailed knowledge of commonly implicated medications, and evaluation of pigment distribution, anatomic localization, and hue, which may suggest a drug-related etiology. Further diagnostic and therapeutic advances are required to manage refractory or generalized cases, as well as dermal pigment deposition mimicking tattoo-like discoloration.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
DIP encompasses diverse etiologies and may affect the skin, mucous membranes, hair, and nails. Reported causative agents include the following (see Image. Pigmentation Effects Linked to Common Medications):
- Anticoagulants: Eltrombopag
- Antiepileptics: Phenytoin, valproic acid
- Antimalarials: Hydroxychloroquine (see Image. Hydroxychloroquine-Induced Pigmentation)
- Antimicrobials: Clofazimine, dapsone, minocycline, isoniazid, levofloxacin, penicillin, sulfonamides
- Antidepressants: Tricyclic antidepressants, mirtazapine
- Immunosuppressants: Tacrolimus, azathioprine
- Antifungals: Nystatin, voriconazole, amphotericin B
- Antipsychotics: Phenothiazines
- Antiretrovirals: Emtricitabine, zidovudine
- Antiarrhythmics: Amiodarone
- Anti-inflammatory agents: Nonsteroidal anti-inflammatory drugs, paracetamol
- Prostaglandin analogs: Bimatoprost, latanoprost
- Chemotherapeutic agents: Bleomycin, cisplatin, capecitabine, cyclophosphamide, doxorubicin, paclitaxel, hydroxyurea (see Image. Doxorubicin-Induced Mucosal Pigmentation)
- Heavy metals: Arsenic, iron, lead, silver, mercury, gold salts, bismuth subsalicylate
- Miscellaneous agents: Afamelanotide, hydroquinone, oral contraceptives, minoxidil, antimonial salts, iodides, niacin, pantoprazole, psoralens, simvastatin, deferoxamine, cetirizine.[1]
The clinical presentation varies according to the medication involved. Differences may be observed in distribution pattern, color hue, duration of persistence after drug withdrawal, and response to treatment.
Epidemiology
When evaluating the incidence of DIP, approximately 10% to 20% of all acquired pigmentation cases are attributed to medication use.[2] More than 50 pharmacologic agents have been reported as potential causes.
Identification of the causative drug requires assessment of several variables, including the interval between drug initiation and onset of pigmentation, the presence of preceding inflammation, and the anatomic distribution of discoloration. Evaluation should also determine whether pigmentation results from enhanced melanin synthesis— typically manifesting as photodistributed changes, diffuse tanning, or homogeneous darkening—or from dermal deposition of the drug or its metabolites, often localized to the face, legs, palms, soles, or mucosa.
While a broad range of medications have been implicated, identifying patients at risk and anticipating the severity of their symptoms remain challenging.[3] No significant sex-, age-, or race-related differences have been demonstrated, although individuals with darker skin types may develop more prominent hyperpigmentation. Further prospective studies are warranted to clarify these associations.[4][5]
Pathophysiology
The pathophysiology of DIP varies according to the underlying mechanism and the specific drug involved. The principal processes include increased melanin synthesis, direct drug or metabolite deposition within the skin, and pigmentary change secondary to inflammation, with additional contributory pathways involving vascular injury and lipofuscin accumulation.
Enhanced melanin production results from either direct stimulation of melanocytes or secondary hormonal effects. Oral contraceptives and afamelanotide stimulate melanocytes directly, while fluorouracil increases adrenocorticotropic hormone levels, leading to heightened melanocytic activity.[6] Direct deposition of drugs or their metabolites in the epidermis and dermis accounts for a substantial proportion of cases, particularly with hydroxychloroquine, amiodarone, and minocycline.[7][8]
Inflammatory mechanisms also contribute to pigmentation, as seen in bleomycin-induced flagellate erythema, which may evolve into residual hyperpigmentation (see Image. Flagellate Erythema). Drug-induced photosensitivity produces superficial burns followed by postinflammatory pigmentation, often compounded by metabolite deposition. Tetracyclines are a characteristic example due to their effect on UV tolerance. Vascular injury with subsequent accumulation of iron and metabolites comprises another contributory mechanism. Lipofuscin accumulation, resulting from the buildup of undegradable oxidized proteins and lipids, further promotes pigmentation in some cases.[9]
Histopathology
Histopathologic findings in DIP are variable and depend on the causative drug, the pathogenic mechanism, and the anatomic site of pigment deposition. Among commonly implicated agents, antimalarials localize intracellularly within the deep dermis and around capillaries. Amiodarone induces lipofuscin accumulation, with deposits observed in histiocytes and perivascular regions. Tetracyclines produce basal layer hyperpigmentation with pigment-laden dermal macrophages. Doxorubicin increases melanin deposition within the epidermis, whereas bleomycin enhances melanin concentration across the epidermal layers.
Deposition patterns of heavy metals exhibit distinct distributions. Mercury localizes in the upper dermis, basal epidermis, and dermal melanophages. Silver forms fine granules in the lamina propria and sweat glands, while gold accumulates as large, rounded granules surrounding dermal vessels.[10]
History and Physical
Evaluation of suspected DIP requires a systematic and comprehensive clinical approach. A thorough medication review is essential and should include all prescription, over-the-counter, and homeopathic agents, as nonsteroidal anti-inflammatory drugs and other commonly used medications may act as potential triggers. The onset of pigmentation should be characterized carefully, as DIP typically develops gradually with insidious progression. For certain drugs, such as hydroxychloroquine, the mean onset of pigmentation has been estimated at approximately 6 years of therapy.
Physical examination must include assessment of the skin, mucous membranes, nails, and hair, with particular attention to patterns involving photoexposed areas. Characteristic presentations may provide diagnostic clues, such as flagellate erythema associated with bleomycin therapy or photodistributed pigmentation resulting from tetracycline use.
Pigment color may also suggest the underlying mechanism. Melanin hyperproduction usually produces a brown hue, whereas drug or metabolite deposition more frequently yields gray, blue, or violaceous discoloration. Variation in hue may correspond to the depth of pigment deposition within the skin.
Evaluation should also consider dose dependence, as pigmentation intensity often increases with cumulative exposure to the causative drug.[11] DIP is a diagnosis of exclusion, requiring careful differentiation from other pigmentary disorders. With the growing number of medications associated with pigmentation, including novel agents and biologics, discontinuation of the suspected drug, when clinically feasible, combined with photoprotection and serial monitoring for improvement, assists in confirming causality.
Evaluation
Diagnostic tests for DIP hold limited but valuable roles. While clinical history and physical examination are fundamental, tools like dermoscopy and histological evaluation can help identify pigment types (eg, melanin, drug deposits, and iron) and exclude other causes.[12] Laboratory investigations and imaging studies may be employed to evaluate systemic effects of the offending drug.[13][14] However, diagnosis often relies on temporal association with drug use and response to drug discontinuation, as no single diagnostic test conclusively predicts or confirms DIP. Further research is needed to improve diagnostic precision and treatment options.
Treatment / Management
Initial management of DIP involves evaluating the feasibility of replacing the causative medication with an alternative agent that provides equivalent therapeutic efficacy. Gradual dose reduction may be considered when substitution is not possible, provided no contraindicating factors are present, and adequate control of the underlying condition is maintained.
A dose-dependent relationship has been demonstrated for several drugs, including amiodarone and hydroxychloroquine, in which higher cumulative doses correlate with greater pigment intensity. In such cases, dose reduction may lead to partial resolution or attenuation of dyschromia.
Preventive strategies include minimizing UV exposure and implementing protective measures, such as seeking shade and wearing photoprotective clothing. These measures are particularly important for individuals receiving antimalarial agents, psychotropic medications, amiodarone, or tetracyclines, which are frequently associated with photoaccentuated pigmentation.
Topical medications and laser-based interventions may be considered if substitution or dose reduction is ineffective. Topical agents are used in most DIP cases, with hydroquinone being the most frequently applied. However, prolonged use of hydroquinone may result in rebound pigmentation or ochronosis. Other reported therapies include high-potency corticosteroids, tacrolimus, and chemical peels containing strong α-hydroxy acids.[15] The efficacy of topical therapies depends on the underlying pigmentation mechanism—whether due to melanin overproduction or metabolite deposition—and the depth of pigment deposition, both of which influence treatment response.(B3)
Laser therapy has been described in multiple reports, particularly for psychotropic drug-induced pigmentation. Effective modalities include picosecond, Q-switched, alexandrite, and ruby lasers; carbon dioxide full-face resurfacing; and neodymium-doped yttrium aluminum garnet (Nd:YAG) systems. Dermabrasion, chelating agents, and intense pulsed light have also been employed.[16] Despite the availability of these modalities, pigmentation may persist for years after discontinuation of the causative drug, even with multimodal management.(B2)
Differential Diagnosis
DIP is primarily a diagnosis of exclusion. Therefore, other potential causes of hyperpigmentation must be evaluated first. The most common primary pigmentary disorder, melasma, should be ruled out, particularly when facial involvement is present. Metabolic and endocrine conditions, such as hemochromatosis, Addison disease, and Wilson disease, which may also involve visceral organs like the liver, should likewise be considered. Nutritional deficiencies, such as niacin deficiency manifesting as pellagra, can produce pigmentation in sun-exposed regions, including the chest, back, and arms. Additional dermatologic conditions, such as lichen planus pigmentosus and oral lichenoid reactions, may also result in diffuse or generalized pigmentation.[17]
Prognosis
The prognosis of DIP is generally favorable. However, involvement of extracutaneous sites can complicate management. Pigmentation affecting the nails or mucous membranes may present therapeutic challenges. DIP is not associated with increased mortality, but it can exert psychological or social effects, the magnitude of which varies among individual patients.[18]
Complications
DIP is generally regarded as an unavoidable adverse effect of certain medications. The most common complication is delayed recognition, as pigmentation typically develops gradually. Most cases are benign and asymptomatic, with the primary concern being cosmetic. Pigmentation arising secondary to inflammatory or symptomatic conditions may be classified as a separate disorder, such as fixed drug eruptions, flagellate erythema, or lichen planus pigmentosus with mucosal involvement.
DIP can also affect extracutaneous organs. For example, hydroxychloroquine may induce retinal pigmentation, particularly in the macula (bull’s-eye retinopathy), potentially resulting in vision loss. Minocycline-induced pigmentation of the heart valves is an uncommon, incidental observation reported in the literature.[19]
Deterrence and Patient Education
Patient education is critical throughout the management of DIP, from diagnosis through treatment. Accurate identification relies on a comprehensive medical history, requiring patients to provide complete and precise information regarding current and prior medication use. When modifying or discontinuing a drug associated with pigmentation, patients must understand the revised treatment plan to prevent exacerbation and maintain adequate control of the underlying condition. Despite available diagnostic tools, including clinical history, physical examination, and histopathology, identification of the causative medication may not always be achievable.
Strict sun avoidance and protective measures should be recommended for patients on medications with pigmentary effects intensified by UV radiation.[20] Clear communication regarding prognosis is essential. Pigmentation may persist for months to years, and multimodal interventions may not fully restore baseline skin coloration even after discontinuation of the offending agent.
Enhancing Healthcare Team Outcomes
A coordinated, interprofessional approach is essential for the management of DIP. Dermatologists should maintain active communication with primary care physicians, who often serve as the primary prescribers, to facilitate identification of the causative medication and development of strategies for dose reduction, discontinuation, or substitution. Documentation of a patient’s history of drug-related pigmentation is critical to guide future prescribing and prevent recurrence.
Management of pigmentation secondary to drug therapy requires collaboration among primary care physicians, dermatologists, specialty-trained nurses, and pharmacists. Effective interprofessional communication supports timely recognition of DIP and implementation of management strategies to minimize further pigmentary changes.
Media
(Click Image to Enlarge)
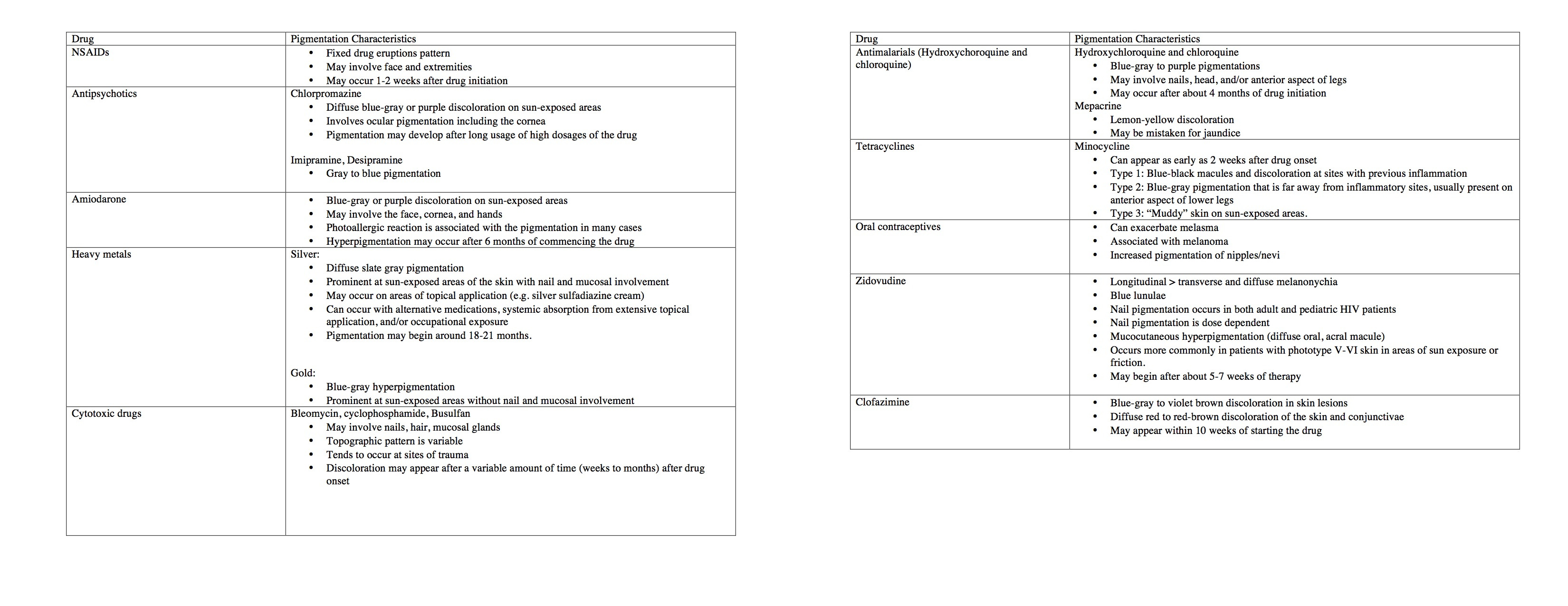
Pigmentation Effects Linked to Common Medications. The table outlines the pigmentation features associated with various medications, providing key details on coloration, affected sites, and duration after starting treatment.
Contributed by Shahzeb Hassan
(Click Image to Enlarge)

Flagellate Erythema. Hyperpigmented linear streaks are present on the lumbosacral region in a patient undergoing bleomycin therapy for a mediastinal germinal tumor.
Contributed by Tatiana Camayo, MD
(Click Image to Enlarge)

Hydroxychloroquine-Induced Pigmentation. The image shows hyperpigmented skin lesions distributed across the neck and anterior chest in a patient receiving hydroxychloroquine.
Contributed by Tatiana Camayo, MD
(Click Image to Enlarge)

Doxorubicin-Induced Mucosal Pigmentation. This image shows mucosal pigmentation on the tongue resulting from doxorubicin therapy. Pigmentary changes in the oral mucosa occur as a known side effect of this chemotherapeutic agent.
Contributed by Tatiana Camayo, MD
References
Tisack A, Mohammad TF. Drug-Induced Pigmentation: A Review. Drugs. 2024 Sep:84(9):1071-1091. doi: 10.1007/s40265-024-02062-z. Epub 2024 Aug 1 [PubMed PMID: 39085684]
Giménez García RM, Carrasco Molina S. Drug-Induced Hyperpigmentation: Review and Case Series. Journal of the American Board of Family Medicine : JABFM. 2019 Jul-Aug:32(4):628-638. doi: 10.3122/jabfm.2019.04.180212. Epub [PubMed PMID: 31300585]
Level 2 (mid-level) evidenceNahhas AF, Braunberger TL, Hamzavi IH. An Update on Drug-Induced Pigmentation. American journal of clinical dermatology. 2019 Feb:20(1):75-96. doi: 10.1007/s40257-018-0393-2. Epub [PubMed PMID: 30374894]
Halder RM, Nandedkar MA, Neal KW. Pigmentary disorders in ethnic skin. Dermatologic clinics. 2003 Oct:21(4):617-28, vii [PubMed PMID: 14717403]
Dereure O. Drug-induced skin pigmentation. Epidemiology, diagnosis and treatment. American journal of clinical dermatology. 2001:2(4):253-62 [PubMed PMID: 11705252]
Schaefer JK, Ramnath N. Fluorouracil-Induced Hyperpigmentation. The New England journal of medicine. 2020 Jan 23:382(4):e6. doi: 10.1056/NEJMicm1909329. Epub [PubMed PMID: 31971682]
Peng JP, Yang XY, Luo F, Yuan XM, Xiong H, Ma WK, Yao XM. Hydroxychloroquine-induced hyperpigmentation of the skin and bull's-eye maculopathy in rheumatic patients: a case report and literature review. Frontiers in immunology. 2024:15():1383343. doi: 10.3389/fimmu.2024.1383343. Epub 2024 Apr 10 [PubMed PMID: 38660312]
Level 3 (low-level) evidenceNishikubo M, Yamashita D, Nishioka H. Minocycline-induced skin hyperpigmentation. BMJ case reports. 2025 Mar 25:18(3):. pii: e264463. doi: 10.1136/bcr-2024-264463. Epub 2025 Mar 25 [PubMed PMID: 40132928]
Level 3 (low-level) evidenceBell AT, Roman JW, Gratrix ML, Brzezniak CE. Minocycline-Induced Hyperpigmentation in a Patient Treated with Erlotinib for Non-Small Cell Lung Adenocarcinoma. Case reports in oncology. 2017 Jan-Apr:10(1):156-160. doi: 10.1159/000452146. Epub 2017 Feb 15 [PubMed PMID: 28413391]
Level 3 (low-level) evidenceGranstein RD, Sober AJ. Drug- and heavy metal--induced hyperpigmentation. Journal of the American Academy of Dermatology. 1981 Jul:5(1):1-18 [PubMed PMID: 6268671]
Kounis NG, Frangides C, Papadaki PJ, Zavras GM, Goudevenos J. Dose-dependent appearance and disappearance of amiodarone-induced skin pigmentation. Clinical cardiology. 1996 Jul:19(7):592-4 [PubMed PMID: 8818442]
Level 3 (low-level) evidenceBehera B, Palit A, Sethy M, Nayak AK, Dash S, Ayyanar P. Dermoscopic features of clofazimine-induced pigmentation in a borderline tuberculoid leprosy plaque. Indian journal of dermatology, venereology and leprology. 2021 Jan-Feb:88(1):85-87. doi: 10.25259/IJDVL_1421_20. Epub [PubMed PMID: 34491673]
Hamri L. Hyperpigmentation Induced by Hydroxychloroquine. Dermatology practical & conceptual. 2023 Oct 1:13(4):. doi: 10.5826/dpc.1304a235. Epub 2023 Oct 1 [PubMed PMID: 37992335]
Baaklini C, Kesav N, Reinhart W. Minocycline-Induced Ocular Ochronosis. Cureus. 2023 Aug:15(8):e43307. doi: 10.7759/cureus.43307. Epub 2023 Aug 10 [PubMed PMID: 37700983]
Suvirya S, Agrawal A, Parihar A. 5-Fluorouracil-induced bilateral persistent serpentine supravenous hyperpigmented eruption, bilateral mottling of palms and diffuse hyperpigmentation of soles. BMJ case reports. 2014 Oct 21:2014():. doi: 10.1136/bcr-2014-206793. Epub 2014 Oct 21 [PubMed PMID: 25336557]
Level 3 (low-level) evidenceHamid RN, Yang RG, Munavalli GS. Treatment of imipramine-induced hyperpigmentation with quality-switched ruby and picosecond lasers. JAAD case reports. 2021 Nov:17():12-17. doi: 10.1016/j.jdcr.2021.09.004. Epub 2021 Sep 20 [PubMed PMID: 34646927]
Level 2 (mid-level) evidenceYamaguchi Y, Hearing VJ. Melanocytes and their diseases. Cold Spring Harbor perspectives in medicine. 2014 May 1:4(5):. doi: 10.1101/cshperspect.a017046. Epub 2014 May 1 [PubMed PMID: 24789876]
Level 3 (low-level) evidenceKleinegger CL, Hammond HL, Finkelstein MW. Oral mucosal hyperpigmentation secondary to antimalarial drug therapy. Oral surgery, oral medicine, oral pathology, oral radiology, and endodontics. 2000 Aug:90(2):189-94 [PubMed PMID: 10936838]
Level 3 (low-level) evidenceSant'Ambrogio S, Connelly J, DiMaio D. Minocycline pigmentation of heart valves. Cardiovascular pathology : the official journal of the Society for Cardiovascular Pathology. 1999 Nov-Dec:8(6):329-32 [PubMed PMID: 10615019]
Level 3 (low-level) evidenceWeiss SR, Lim HW, Curtis G. Slate-gray pigmentation of sun-exposed skin induced by amiodarone. Journal of the American Academy of Dermatology. 1984 Nov:11(5 Pt 1):898-900 [PubMed PMID: 6512044]
Level 3 (low-level) evidence