 Anatomy, Bony Pelvis and Lower Limb: Calf Peroneus Longus Muscle
Anatomy, Bony Pelvis and Lower Limb: Calf Peroneus Longus Muscle
Introduction
The peroneus longus, also known as the fibularis longus, is 1 of 2 muscles in the lateral compartment of the lower limb, along with the peroneus (fibularis) brevis (see Image. Muscles of the Anterior Leg Compartment and the Foot Dorsum).[1] The lateral compartment receives innervation from the superficial peroneal (fibular) nerve (L5–S2) and vascular supply from the anterior tibial and peroneal (fibular) arteries. This muscle contributes to plantarflexion and eversion of the foot and ankle. Physiologic variants include accessory tendinous slips and variable insertions onto multiple metatarsals and cuneiforms, including the base of the 1st metatarsal and medial cuneiform.
The fibularis longus is susceptible to several pathologies, including tendinitis, tendon dislocation, subluxation, rupture, and acute and chronic compartment syndrome.[2][3] The muscle's tendon serves as a versatile autograft in ligament reconstruction and is used in tendon transfer procedures to restore foot and ankle biomechanics. Understanding the anatomy and physiology of the fibularis longus underpins the diagnosis of lateral ankle conditions and the selection of appropriate operative techniques.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The fibularis longus arises from the head and the proximal lateral surface of the fibula and inserts on the base of the 1st metatarsal and medial cuneiform. The muscle is adjacent to the fibularis brevis on the lateral aspect of the lower limb, coursing inferiorly and tapering into a long, slender tendinous portion that descends into the foot posterior to the lateral malleolus before crossing under the foot and attaching to the medial foot structures (see Image. Distal Path of the Peroneus Longus and Brevis). The primary functions of the fibularis longus are to plantarflex and evert the foot at the ankle. Contraction of the muscle produces upward plantarflexion and outward eversion due to its insertion on the medial aspect of the foot and course along the lateral leg. This movement contributes to foot eversion and is commonly injured during forced inversion and dorsiflexion of the ankle in traumatic settings.[4]
Embryology
Limb buds begin forming approximately in the 4th to 5th week after fertilization. Mesoderm migrates into the limb bud and forms dorsal and ventral muscle masses, which give rise to the muscular components of the lower limb and to the mesenchymal core that contributes to the skeletal elements. The dorsal condensation develops into extensor and abductor musculature of the lower limb, whereas the ventral condensation develops into flexor and adductor musculature of the lower limb.[5]
Several factors influence the formation of limb bud musculature, including retinoic acid and sonic hedgehog (Shh), as well as regulatory homeobox (HOX) genes. Additional organization of development is mediated by embryologic signaling centers, including the apical ectodermal ridge (AER) and the zone of polarizing activity (ZPA). Retinoic acid contributes to regional differentiation and limb polarization. The AER produces fibroblast growth factor (FGF), promoting limb bud outgrowth by stimulating mitosis.[6]
The specific FGF involved in hindlimb development is FGF10, which is stimulated by T-box transcription factor 4 (Tbx4). The ZPA produces Shh, which promotes organization of the limb bud along the anterior–posterior axis. Shh helps establish expression domains of specific HOX genes—HOXD9, HOXD10, HOXD11, HOXD12, and HOXD13—which are essential for limb polarization and regional specification.[7] These genes regulate patterning and, consequently, morphology of the developing limb in the human embryo. Errors in HOX gene expression can result in limb malformations.[8]
Blood Supply and Lymphatics
The anterior tibial and fibular arteries supply the fibularis longus. The anterior tibial artery arises from the popliteal artery, which originates from the superficial femoral artery, a branch of the common femoral artery of the external iliac artery (see Image. Arteries of the Lower Limb, Anterior and Posterior Views.).[9] The superficial femoral artery becomes the popliteal artery upon passage through the adductor hiatus into the popliteal fossa. The popliteal artery then bifurcates in the distal popliteal fossa into the anterior tibial artery and the tibiofibular trunk. The tibiofibular trunk subsequently divides into the posterior tibial and fibular arteries. The posterior tibial artery continues inferiorly to supply the posterior compartment of the leg. The fibular artery descends posteriorly along the fibula within the posterior compartment of the leg and gives rise to perforating branches that penetrate the intermuscular septum to supply the muscles of the lateral leg compartment.
The lymphatic vessels of the lower limb are subdivided into superficial and deep groups. Superficial lymphatic vessels of the lower limb are further divided into medial and lateral groups. The medial group follows the greater saphenous vein, whereas the lateral group follows the small saphenous vein. Deep lymphatic vessels include the anterior tibial, posterior tibial, and fibular vessels, which follow the corresponding blood vessels. Lymphatic drainage of the lower limb proceeds through the popliteal, superficial inguinal, deep inguinal, external iliac, and lumbar (aortic) lymph nodes.
Nerves
The fibularis longus receives innervation from the superficial fibular nerve, a terminal branch of the common fibular nerve, which originates from the sciatic nerve (L4–S3).[10] The sciatic nerve bifurcates at the apex of the popliteal fossa into the tibial and common fibular nerves. The tibial nerve continues inferiorly in the posterior leg, posterior to the tibia, supplying the deep posterior compartment musculature. The terminal division of the tibial nerve gives rise to the medial and lateral plantar nerves.
The common fibular nerve courses along the medial border of the biceps femoris, traveling laterally and inferiorly toward the fibular head. The nerve wraps around the neck of the fibula, passing between the attachments of the fibularis longus to supply the lateral compartment of the leg. Terminal bifurcation gives rise to the superficial fibular nerve, which supplies the lateral compartment, and the deep fibular nerve, which provides motor impulses to the anterior compartment of the leg, including the extensor hallucis longus (see Image. Deep Fibular Nerve and Related Structures). Nerve roots that contribute to the superficial fibular nerve arise from L4 to S1. Injury to this nerve results in weak eversion and sensory loss over most of the dorsal foot and the anterolateral aspect of the distal leg.[11]
Physiologic Variants
The fibularis longus arises from the head and superolateral aspect of the fibula and inserts on the base of the 1st metatarsal and the medial cuneiform. The tendon passes inferior to the cuboid bone through a fibro-osseous tunnel termed the "cuboid tunnel" and continues to its insertion on the plantar aspect of the medial cuneiform. Several anatomic variants exist, including accessory tendinous slips with insertions into adjacent bones or tendons. These variants are clinically relevant because the fibularis longus is involved in several pathologies, including traumatic injury, tendinitis, dislocation, acute rupture, and chronic tear. Certain pathologies may demonstrate increased association with specific anatomic variants. A recent study described common anatomic variants in cadaveric specimens.
Distal fibularis longus tendon insertion demonstrates variable anatomic distribution in cadaveric specimens. The base of the 1st metatarsal is the most consistent insertion site, observed in 30 specimens, representing 100%. The medial cuneiform is involved in 26 specimens, representing 86.6%. The neck of the 1st metatarsal is observed in 3 specimens, representing 10%. The base of the 2nd metatarsal is observed in 6 specimens, representing 20%. The base of the 4th metatarsal is observed in 5 specimens, representing 16.6%. The base of the 5th metatarsal is observed in 7 specimens, representing 23.3%. These variations in insertion sites are clinically relevant in understanding symptom patterns associated with fibularis longus tendon pathology and in evaluating its contribution to the maintenance of the transverse and medial longitudinal arches of the foot.[12]
Surgical Considerations
In trauma and other mechanical injuries, the fibularis longus tendon may become dislocated, subluxated, or ruptured. In 2016, a research team surveyed foot and ankle surgeons nationally to evaluate management strategies for acute fibular tendon tears. Marked variability was observed in treatment protocols and operative techniques. Nonoperative management for greater than a year was selected by 22% of surgeons, whereas 33% proceeded directly to operative intervention. Among surgeons selecting operative management, 88% tubularized the tendon after repair, 33% excised redundant tissue, and 22% removed the fibular tubercle when hypertrophic.[13][14][15][16][17]
Surgical treatment is associated with improved return to activity and patient-reported outcome scores in symptomatic patients.[18] A personalized, comprehensive rehabilitation program is necessary to optimize recovery following surgical repair of fibular tendon tears and ruptures. Most fibular tendon tears occur in young, active patients and athletes, making early return to activity a primary treatment goal.
The lateral compartment of the leg is susceptible to acute compartment syndrome. Increased pressure within this region can compromise tissue perfusion, leading to irreversible muscle and nerve injury and subsequent necrosis of muscle and soft tissue. The most common etiologies include trauma, tight casts or dressings, postischemic swelling, and arterial injury. Chronic compartment syndrome may also occur and warrants consideration in patients presenting with lateral leg pain, tenderness, and firmness on palpation. Prompt recognition of compartment syndrome is essential to prevent ischemia and necrosis of the neurovascular structures and musculature.[19]
Patients with compartment syndrome often present with pain disproportionate to the clinical situation. Physical examination findings include pain on palpation of the involved musculature, pain with passive stretching of the affected muscle (the most sensitive finding prior to the onset of ischemia), and firmness of the compartment.[20]
Compartment syndrome primarily affects the venous system. Therefore, arterial pulses are usually intact. Definitive diagnosis requires measurement of intracompartmental pressures. A resting compartment pressure greater than 30 mm Hg confirms the diagnosis.[21] Time is critical in acute compartment syndrome. Treatment within 6 hours of ischemia is associated with complete recovery, whereas irreversible necrosis typically occurs after 6 hours of poor perfusion.[22] Definitive management of acute compartment syndrome consists of subcutaneous fasciotomy.
Clinical Significance
The fibularis longus contributes to plantarflexion and eversion of the foot at the ankle joint. Clinical examination includes assessment of ankle range of motion and motor strength. Reduced or absent strength may indicate injury to the fibularis longus or brevis or both.
Fibularis longus pathology includes tendinitis, subluxation, dislocation, and acute or chronic tendon tears. Most fibular tendon injuries occur in young, active patients and are commonly associated with sports such as football, soccer, and running. Injury to the fibularis longus tendon is a cause of lateral ankle pain and may contribute to ankle instability. Tendon tears are most commonly longitudinal due to subluxation over the fibula but may also be transverse.[23]
An isolated tear is more commonly found in the fibularis brevis but may also occur in the fibularis longus. Nonoperative treatment includes nonsteroidal anti-inflammatory drug administration, ice application, resting, immobilization, and physical therapy. Steroid injections are also used in cases refractory to prior conservative measures. Recent literature demonstrates increasing interest in platelet-rich plasma injections under ultrasound guidance. However, routine clinical adoption remains limited. Failure of conservative treatment may warrant operative intervention, including open debridement, synovectomy, and arthroscopic fibular tendon endoscopy for tendinitis. Operative management of fibular tendon tears includes end-to-end repair, side-to-side anastomosis, or Pulvertaft weave in chronic tears, as well as allograft reconstruction.[24][25]
The lateral compartment of the leg may be involved in compartment syndrome. The acute form most commonly involves the anterior compartment, though the lateral compartment may also be affected following blunt force injury or trauma. Chronic exertional compartment syndrome of the lateral compartment is also observed, particularly in athletes. Lower limb musculature is organized into compartments formed by strong, inelastic fascial septa. Compartment syndrome develops when increased pressure within a closed fascial compartment compromises circulation and tissue function within that space.
The lateral compartment contains muscles that primarily contribute to plantarflexion and eversion of the foot at the ankle joint. These muscles are innervated by the superficial fibular nerve and supplied by the fibular artery. Increased intracompartmental pressure may result in paresthesias, weakness of the involved muscle groups, and pain with passive stretch. Compartment syndrome constitutes a medical emergency requiring fasciotomy of the affected compartment.
Other Issues
A fibularis longus tendon transfer involves harvesting the tendon, rerouting it through the foot or ankle, and anchoring it to replace a deficient tendon. The primary indication for this procedure is chronic foot drop due to irreversible loss of ankle dorsiflexion, although it is also used for irreparable tendon rupture or selected cases of neuromuscular weakness. Benefits of this intervention include improved gait and functional mobility. Risks include wound complications, donor-site weakness, overcorrection, and nerve injury.[26]
Media
(Click Image to Enlarge)
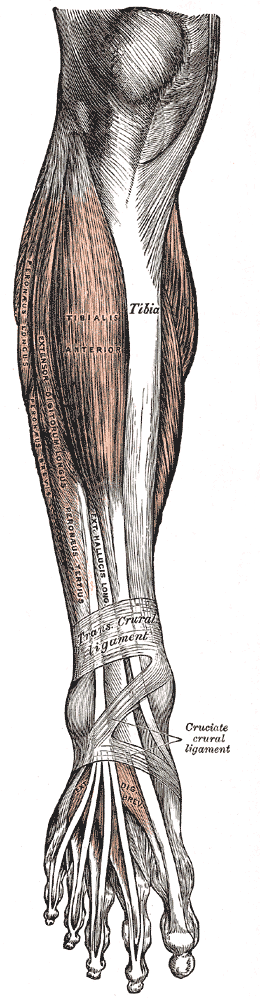
Muscles of the Anterior Leg Compartment and the Foot Dorsum. This anatomical plate illustrates the anterolateral musculature of the lower limb, specifically identifying the tibialis anterior, extensor digitorum longus, and extensor hallucis longus alongside the peroneus longus, peroneus brevis, and peroneus tertius. The diagram displays the relationship between the tibia and these muscle groups as they pass under the transverse crural and cruciate crural ligaments. On the foot, the extensor digitorum brevis is shown distally, completing the representation of the extrinsic and intrinsic muscles responsible for foot and toe movement.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
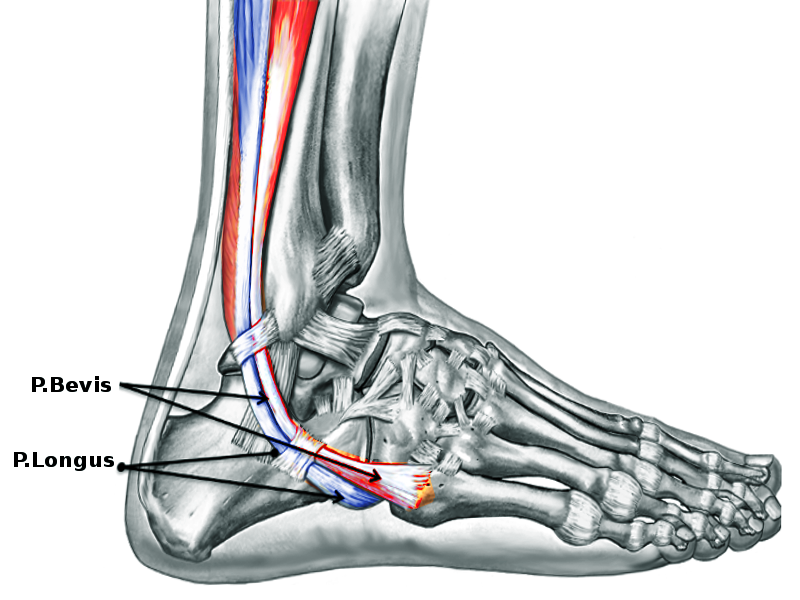
Distal Path of the Peroneus Longus and Brevis. This illustration shows the distal course of the peroneal tendons as they pass behind the lateral malleolus and into the foot. The labeled peroneus brevis lies more superiorly at the retromalleolar groove, while the peroneus longus courses more inferiorly and continues toward the cuboid and plantar midfoot.
Image courtesy O.Chaigasame
(Click Image to Enlarge)
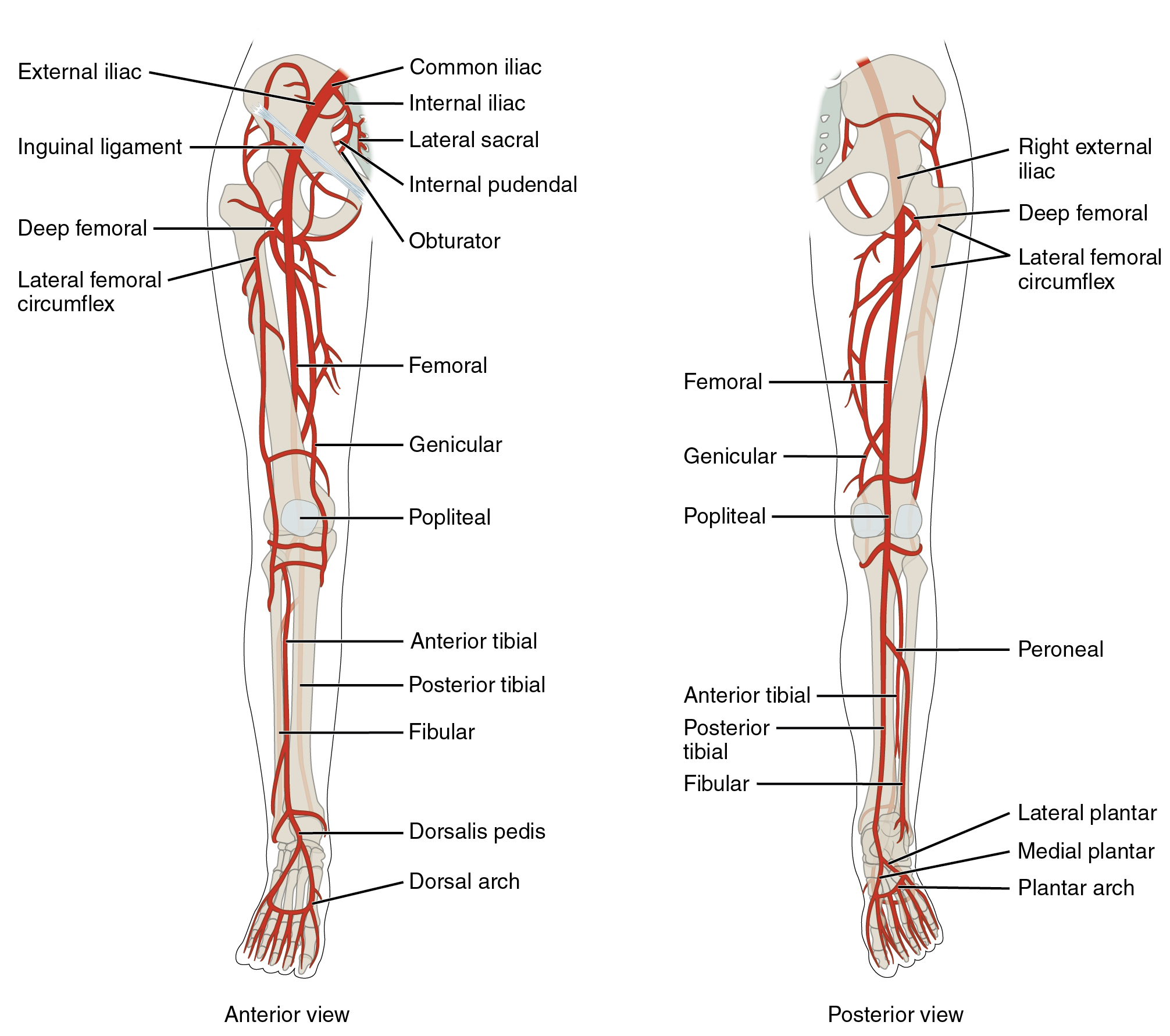
Arteries of the Lower Limb, Anterior and Posterior Views. This detailed illustration shows the arterial anatomy of the lower limb from both anterior and posterior perspectives. Labeled vessels include the common, external, and internal iliac arteries, femoral artery, profunda femoris (deep femoral) artery with its lateral and medial circumflex branches, genicular artery, popliteal artery, anterior and posterior tibial arteries, fibular (peroneal) artery, dorsalis pedis artery, medial and lateral plantar arteries, and the dorsal and plantar arches.
OpenStax College, Public Domain, via Wikimedia Commons
{kind=link}
(Click Image to Enlarge)
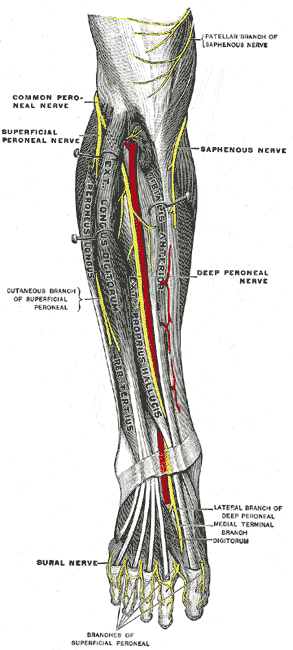
Deep Fibular Nerve and Related Structures. The deep fibular nerve courses through the anterior compartment of the leg in close association with the anterior tibial artery. Distal branching includes lateral and medial terminal branches on the dorsum of the foot. Adjacent nerves, such as the superficial fibular, saphenous, and sural nerves, are also illustrated.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Khan IA, Mahabadi N, D'Abarno A, Varacallo MA. Anatomy, Bony Pelvis and Lower Limb: Leg Lateral Compartment. StatPearls. 2026 Jan:(): [PubMed PMID: 30137811]
Chandwani D, Varacallo MA. Exertional Compartment Syndrome. StatPearls. 2026 Jan:(): [PubMed PMID: 31335004]
Varacallo M, Shirey L, Kavuri V, Harding S. Acute compartment syndrome of the hand secondary to propofol extravasation. Journal of clinical anesthesia. 2018 Jun:47():1-2. doi: 10.1016/j.jclinane.2018.01.020. Epub 2018 Feb 21 [PubMed PMID: 29476968]
Hallinan JTPD, Wang W, Pathria MN, Smitaman E, Huang BK. The peroneus longus muscle and tendon: a review of its anatomy and pathology. Skeletal radiology. 2019 Sep:48(9):1329-1344. doi: 10.1007/s00256-019-3168-9. Epub 2019 Feb 15 [PubMed PMID: 30770941]
Lezak B, Summers S. Anatomy, Bony Pelvis and Lower Limb: Leg Anterior Compartment. StatPearls. 2026 Jan:(): [PubMed PMID: 30969547]
Mróz I, Kielczewski S, Pawlicki D, Kurzydło W, Bachul P, Konarska M, Bereza T, Walocha K, Kaythampillai LN, Depukat P, Pasternak A, Bonczar T, Chmielewski P, Mizia E, Skrzat J, Mazur M, Warchoł Ł, Tomaszewski K. Blood vessels of the shin - anterior tibial artery - anatomy and embryology - own studies and review of the literature. Folia medica Cracoviensia. 2016:56(1):33-47 [PubMed PMID: 27513837]
Gros J, Tabin CJ. Vertebrate limb bud formation is initiated by localized epithelial-to-mesenchymal transition. Science (New York, N.Y.). 2014 Mar 14:343(6176):1253-6. doi: 10.1126/science.1248228. Epub [PubMed PMID: 24626928]
Level 3 (low-level) evidenceBarham G, Clarke NM. Genetic regulation of embryological limb development with relation to congenital limb deformity in humans. Journal of children's orthopaedics. 2008 Feb:2(1):1-9. doi: 10.1007/s11832-008-0076-2. Epub 2008 Feb 7 [PubMed PMID: 19308596]
Hyland S, Sinkler MA, Varacallo MA. Anatomy, Bony Pelvis and Lower Limb: Popliteal Region. StatPearls. 2026 Jan:(): [PubMed PMID: 30422486]
Miniato MA, Black AC, Varacallo MA. Anatomy, Back, Lumbosacral Trunk. StatPearls. 2026 Jan:(): [PubMed PMID: 30969700]
Garrett A, Black AC, Launico MV, Geiger Z. Anatomy, Bony Pelvis and Lower Limb: Superficial Peroneal Nerve (Superficial Fibular Nerve). StatPearls. 2026 Jan:(): [PubMed PMID: 30521214]
Patil V, Frisch NC, Ebraheim NA. Anatomical variations in the insertion of the peroneus (fibularis) longus tendon. Foot & ankle international. 2007 Nov:28(11):1179-82 [PubMed PMID: 18021587]
Brodsky JW, Zide JR, Kane JM. Acute Peroneal Injury. Foot and ankle clinics. 2017 Dec:22(4):833-841. doi: 10.1016/j.fcl.2017.07.013. Epub [PubMed PMID: 29078831]
Daigre J. Peroneal Longus to Brevis Transfer Augmentation With TeKBrace Synthetic Graft. Foot & ankle specialist. 2026 Apr 20:():19386400261441082. doi: 10.1177/19386400261441082. Epub 2026 Apr 20 [PubMed PMID: 42007849]
Wu K, Masschelein G, Suh N. Treatment of Sagittal Band Injuries and Extensor Tendon Subluxation: A Systematic Review. Hand (New York, N.Y.). 2021 Nov:16(6):854-860. doi: 10.1177/1558944719895622. Epub 2020 Jan 22 [PubMed PMID: 31965857]
Level 1 (high-level) evidenceHosack T, Perkins O, Bleibleh S, Singh R. Snapping ankles: peroneal tendon subluxation and dislocation. British journal of hospital medicine (London, England : 2005). 2023 Oct 2:84(10):1-7. doi: 10.12968/hmed.2022.0257. Epub 2023 Sep 29 [PubMed PMID: 37906073]
Zhang P, Li S, Liu Y, Lin Z, Deng Y, Zhou P. Modified posterior fibular groove deepening procedure with repair of the superior peroneal retinaculum for peroneal tendon subluxation. International orthopaedics. 2023 May:47(5):1259-1265. doi: 10.1007/s00264-023-05750-9. Epub 2023 Mar 7 [PubMed PMID: 36881154]
van Dijk PA, Lubberts B, Verheul C, DiGiovanni CW, Kerkhoffs GM. Rehabilitation after surgical treatment of peroneal tendon tears and ruptures. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA. 2016 Apr:24(4):1165-74. doi: 10.1007/s00167-015-3944-6. Epub 2016 Jan 23 [PubMed PMID: 26803783]
Alrayes MM, Alqudah M, Bani Hamad W, Sukeik M. Isolated lateral leg compartment syndrome: A case report. World journal of orthopedics. 2023 Jul 18:14(7):582-588. doi: 10.5312/wjo.v14.i7.582. Epub 2023 Jul 18 [PubMed PMID: 37485425]
Level 3 (low-level) evidenceTaylor RM, Sullivan MP, Mehta S. Acute compartment syndrome: obtaining diagnosis, providing treatment, and minimizing medicolegal risk. Current reviews in musculoskeletal medicine. 2012 Sep:5(3):206-13. doi: 10.1007/s12178-012-9126-y. Epub [PubMed PMID: 22644598]
Mabvuure NT, Malahias M, Hindocha S, Khan W, Juma A. Acute compartment syndrome of the limbs: current concepts and management. The open orthopaedics journal. 2012:6():535-43. doi: 10.2174/1874325001206010535. Epub 2012 Nov 30 [PubMed PMID: 23248724]
raza F, Mabrouk A, Kaiser K. Tibial Anterior Compartment Syndrome. StatPearls. 2026 Jan:(): [PubMed PMID: 30085512]
Walt J, Massey P. Peroneal Tendon Syndromes. StatPearls. 2026 Jan:(): [PubMed PMID: 31335074]
Davda K, Malhotra K, O'Donnell P, Singh D, Cullen N. Peroneal tendon disorders. EFORT open reviews. 2017 Jun:2(6):281-292. doi: 10.1302/2058-5241.2.160047. Epub 2017 Jun 22 [PubMed PMID: 28736620]
Philbin TM, Landis GS, Smith B. Peroneal tendon injuries. The Journal of the American Academy of Orthopaedic Surgeons. 2009 May:17(5):306-17 [PubMed PMID: 19411642]
Stevoska S, Pisecky L, Stadler C, Gahleitner M, Klasan A, Klotz MC. Tendon transfer in foot drop: a systematic review. Archives of orthopaedic and trauma surgery. 2023 Feb:143(2):773-784. doi: 10.1007/s00402-021-04162-x. Epub 2021 Sep 15 [PubMed PMID: 34524486]
Level 1 (high-level) evidence