Introduction
The pericardium is a tough, double-layered fibrous sac that encloses the heart and great vessels (see Images. Midline Thoracic Anatomy, Sagittal View; Anatomical Relations of the Superior Mediastinum and Diaphragm). The structure keeps the heart in a stable position within the mediastinum, facilitates cardiac movements, and separates the heart from the lungs and other mediastinal structures. The pericardium also contributes to physiological cardiac function.[1][2][3]
Knowledge of pericardial anatomy and function enables clinicians to identify and manage conditions such as pericarditis, pericardial effusion, cardiac tamponade, and constrictive pericarditis by understanding fluid dynamics, chamber constraints, and pressure-volume relationships. Surgical interventions, including pericardial incisions and pericardiocentesis, require precise anatomical awareness to avoid injury to the heart, great vessels, phrenic nerves, and surrounding structures. Understanding pericardial reflections, sinuses, and attachments guides safe access for catheter-based procedures, interpretation of imaging, and management of postsurgical complications.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The pericardium consists of 2 layers: fibrous and serous. The fibrous pericardium is a conical sac, with its apex fused to the roots of the great vessels at the base of the heart. The broad base overlies and fuses with the central fibrous area of the diaphragm. Weak sternopericardial ligaments attach the anterior aspect of the fibrous pericardium to the sternum. The serous pericardium is a layer of serosa lining the fibrous pericardium (parietal layer) and reflecting around the roots of the great vessels to cover the entire surface of the heart (visceral layer). A potential space exists between the parietal and visceral layers, which may contain a small amount of fluid. The portion of the visceral layer covering the heart, excluding the great vessels, is called the "epicardium."[4][5]
Reflections of the serous pericardium from various cardiac structures form 2 sinuses: transverse and oblique. The oblique sinus is a cul-de-sac extending superiorly from the inferior vena cava, positioned between the 2 left pulmonary veins on one side and the 2 right pulmonary veins on the other. The anterior wall of the oblique sinus is formed by the posterior wall of the left atrium, between the 4 pulmonary veins. The oblique sinus provides expansion space for the left atrium.
The transverse sinus is open at both ends and results from the reflection of the visceral serosal pericardium from the posterior aspects of the aorta and pulmonary trunk to the anterior aspect of the atrium (see Image. Anatomical Relationships of the Pulmonary Veins Within the Pericardium). Passage of a finger through the transverse sinus allows traversal behind the aorta and pulmonary trunks, anterior to the superior vena cava on the right, and lateral to the left atrial appendage on the left.
The pericardial sac positions the heart within the mediastinum and restricts excessive motion while providing a lubricated interface for cardiac contractions and pulmonary movements. The pericardium prevents excessive cardiac dilatation and, in pathological states, limits overfilling that would otherwise reduce cardiac output. Other functions of this fibrous structure include modulating the pressure–volume relationships of the cardiac chambers by confining the heart within a limited space; equalizing hydrostatic, inertial, and gravitational forces to maintain left ventricular geometry; and providing a mechanical barrier to infection.
Embryology
The fibrous pericardium originates from the septum transversum of the developing embryo. The septum transversum is a thick mass of cranial mesenchyme formed on day 22. During craniocaudal folding, the septum transversum assumes a position caudal to the developing heart. Both the diaphragm and the pericardium, among other structures, develop from the septum transversum (see Image. Development of the Body Cavities and Serous Membranes).
Blood Supply and Lymphatics
The pericardium receives arterial supply from the pericardiophrenic branches of the internal thoracic arteries. Lymph from the visceral pericardium drains into the tracheal and bronchial lymphatic chains. The parietal pericardium exhibits lymphatic drainage patterns similar to those of the sternum and diaphragm. Lymphatics from the ventral surface of the parietal pericardium ascend along the phrenic nerves. Lymphatic channels anastomose with the lymphatics of the reflected mediastinal pleura on the lateral and posterior surfaces.[6]
Nerves
The fibrous pericardium and the parietal layer of the serous pericardium receive innervation from the phrenic nerve. The visceral pericardium receives autonomic innervation from the cardiac plexus, including sympathetic fibers from spinal cord levels T1 to T4 and parasympathetic fibers from the vagus nerve. The visceral pericardium is insensitive to pain, in contrast to the parietal layer.
Physiologic Variants
In rare cases, congenital absence of the pericardium occurs, typically involving a portion or the entire left parietal pericardium. Pericardial cysts represent uncommon remnants of abnormal embryologic development and are benign. The clinical significance of these cysts arises from the need to distinguish them from neoplasms.[7]
Surgical Considerations
Cardiac surgery requires an incision through the pericardium to access the heart. Handling of the pericardium during surgery can induce inflammation and thickening. Pericardial thickening may result in adhesion to the posterior aspect of the sternum at the incision site, complicating repeat surgical procedures.
A needle inserted just below and to the left of the xiphoid process, directed toward the left shoulder, passes above the diaphragm to enter the pericardial space adjacent to the right ventricle. This approach permits drainage of pericardial effusions and provides access for catheter-based procedures on the epicardial surface of the heart, including catheter ablation for arrhythmias.[8][9][10]
Clinical Significance
Pericarditis
Inflammation of the pericardium is termed "pericarditis."[11] Causes may include infectious, immunologic, metabolic, neoplastic, traumatic, or idiopathic origins. Myocardial infarction can induce localized pericarditis over the infarcted area. Postinfectious fibrinous pericarditis develops within 1 to 3 days after myocardial infarction, whereas Dressler syndrome arises weeks to months postinfarction.
Acute pericarditis commonly produces fever, pleuritic chest pain radiating to the back, and a pericardial friction rub on auscultation. Pain intensity increases when the patient lies flat and decreases when the patient sits upright. Electrocardiography typically demonstrates diffuse ST-segment elevation and PR-segment depression. The condition is usually self-limited and treated with nonsteroidal anti-inflammatory drugs and colchicine. Nonsteroidal anti-inflammatory drugs inhibit cyclooxygenase enzyme activity, while colchicine interferes with mitotic cell division during metaphase.[12]
Pericardial Effusion
The pericardium normally contains only a few milliliters of fluid, which serves as a lubricant. Pericarditis and other pathological conditions can result in the accumulation of hundreds of milliliters of exudative or transudative fluid within the pericardial space. Accumulation of pericardial fluid is termed "pericardial effusion" and may be readily identified using echocardiography. A chest radiograph may demonstrate an enlarged, bag-like cardiac silhouette when a significant pericardial effusion is present.[13]
Cardiac Tamponade
Pericardial effusion or hemorrhage into the pericardial space, resulting from injury, reduces the volume available for cardiac expansion. Sufficient impairment of venous return markedly decreases cardiac output because the heart cannot fill adequately. Accumulation of fluid or blood in the pericardial space, causing these effects, is termed "cardiac tamponade."[14]
Cardiac tamponade constitutes a life-threatening emergency and often requires urgent intervention. Clinical recognition relies on the triad of hypotension, muffled heart sounds, and jugular venous distension. Patients may also present with pulsus paradoxus, defined as a decrease in systolic blood pressure greater than 10 mm Hg during inspiration. Echocardiography is the first-line imaging modality for diagnosis. Management options include pericardial fluid drainage via needle, placement of a pericardial catheter for continuous drainage, and surgical creation of a pericardial–pleural window.
Constrictive Pericarditis
Constrictive pericarditis develops when chronic inflammation of the pericardium produces thickening, fibrosis, and, often, calcification, restricting diastolic filling of the ventricles.[15][16] The condition may complicate acute pericarditis, particularly when the underlying cause is neoplastic, bacterial, or radiation-induced. Constrictive pericarditis also occurs in association with tuberculosis and recent cardiac surgery. Clinical presentation typically includes signs of fluid overload, such as jugular venous distension, hepatomegaly, and peripheral edema. Additional findings comprise the Kussmaul sign, characterized by a paradoxical rise in jugular venous pressure during inspiration, and a pericardial knock, an extrasystolic heart sound immediately following S1.
Media
(Click Image to Enlarge)
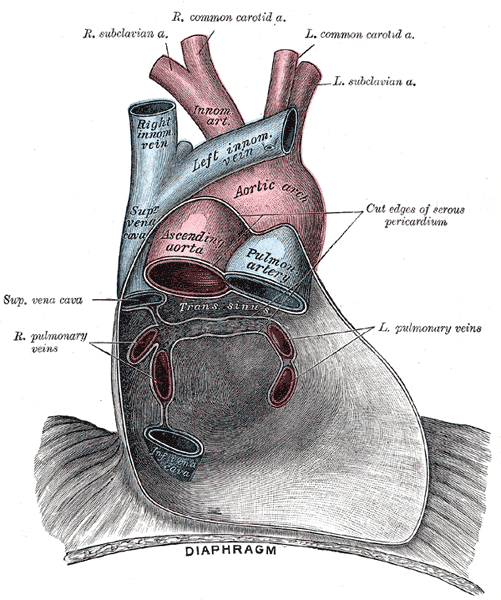
Anatomical Relationships of the Pulmonary Veins Within the Pericardium. This anterior view illustrates the major thoracic vessels enclosed by the serous pericardium, including the left and right pulmonary veins draining into the posterior wall of the left atrium. The ascending aorta, aortic arch, pulmonary artery, and superior vena cava are shown in relation to the pulmonary venous return. The image also depicts the great arterial branches and the anatomical continuity between the pericardium and diaphragm.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
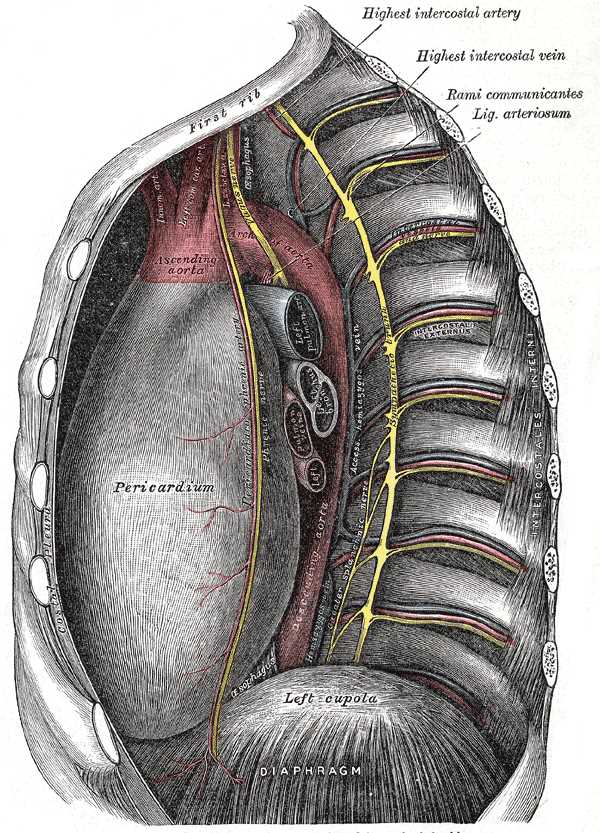
Midline Thoracic Anatomy, Sagittal View. This illustration shows a detailed sagittal view of thoracic structures, including the heart in the pericardium, ribs, intercostal nerves, highest intercostal and bronchial arteries, internal mammary vessels, great arteries (aorta, pulmonary trunk), superior vena cava, pulmonary veins, esophagus, diaphragm, tracheal bifurcation, phrenic nerve, and sternal attachments.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
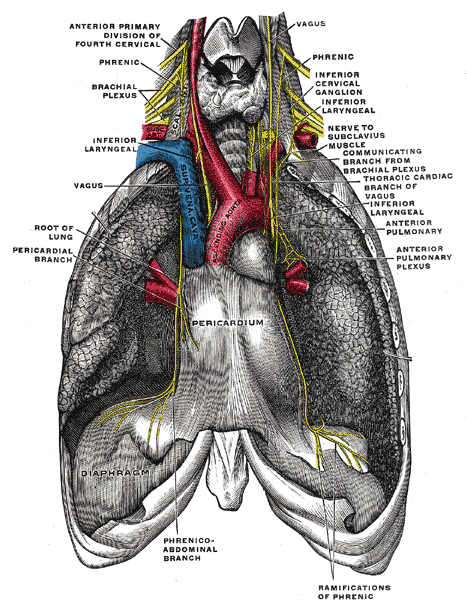
Anatomical Relations of the Superior Mediastinum and Diaphragm. This illustration highlights the structural connections between the cervical ganglia, the brachial plexus, and the major thoracic organs, including the pericardium and the root of the lung.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
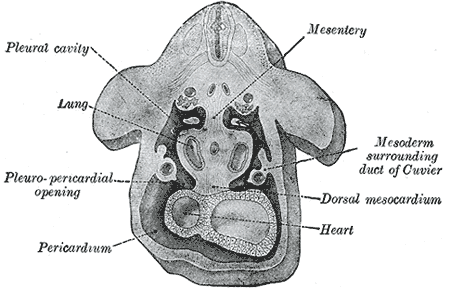
Development of the Body Cavities and Serous Membranes. This illustration details the internal organization of the developing body, including the mesentery, lungs, heart, and the critical pleuropericardial and pleuroperitoneal junctions.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Mahabadi N, Goizueta AA, Bordoni B. Anatomy, Thorax, Lung Pleura And Mediastinum. StatPearls. 2025 Jan:(): [PubMed PMID: 30085590]
Volpe JK, Makaryus AN. Anatomy, Thorax, Heart and Pericardial Cavity. StatPearls. 2025 Jan:(): [PubMed PMID: 29494059]
Oliver KA, Ashurst JV. Anatomy, Thorax, Phrenic Nerves. StatPearls. 2025 Jan:(): [PubMed PMID: 30020697]
Rodriguez ER, Tan CD. Structure and Anatomy of the Human Pericardium. Progress in cardiovascular diseases. 2017 Jan-Feb:59(4):327-340. doi: 10.1016/j.pcad.2016.12.010. Epub 2017 Jan 4 [PubMed PMID: 28062264]
Hoit BD. Anatomy and Physiology of the Pericardium. Cardiology clinics. 2017 Nov:35(4):481-490. doi: 10.1016/j.ccl.2017.07.002. Epub [PubMed PMID: 29025540]
Eliskova M, Eliska O, Miller AJ. The lymphatic drainage of the parietal pericardium in man. Lymphology. 1995 Dec:28(4):208-17 [PubMed PMID: 8771014]
Kim HJ, Cho YS, Cho GY, Choi SI. Congenital absence of the pericardium. Journal of cardiovascular ultrasound. 2014 Mar:22(1):36-9. doi: 10.4250/jcu.2014.22.1.36. Epub 2014 Mar 31 [PubMed PMID: 24753808]
Level 3 (low-level) evidenceAbdelnaby M, Almaghraby A, Saleh Y, Abayazeed R. Pericardial sarcoma. BMJ case reports. 2018 Oct 7:2018():. pii: bcr-2018-226112. doi: 10.1136/bcr-2018-226112. Epub 2018 Oct 7 [PubMed PMID: 30297493]
Level 3 (low-level) evidenceSharma NK, Waymack JR. Acute Cardiac Tamponade. StatPearls. 2025 Jan:(): [PubMed PMID: 30521227]
Manda YR, Baradhi KM. Myopericarditis. StatPearls. 2025 Jan:(): [PubMed PMID: 30521197]
Peterson TA, Turner SP, Dolezal KA. Acute Pericarditis: Rapid Evidence Review. American family physician. 2024 May:109(5):441-446 [PubMed PMID: 38804758]
Ismail TF. Acute pericarditis: Update on diagnosis and management. Clinical medicine (London, England). 2020 Jan:20(1):48-51. doi: 10.7861/clinmed.cme.20.1.4. Epub [PubMed PMID: 31941732]
Vakamudi S, Ho N, Cremer PC. Pericardial Effusions: Causes, Diagnosis, and Management. Progress in cardiovascular diseases. 2017 Jan-Feb:59(4):380-388. doi: 10.1016/j.pcad.2016.12.009. Epub 2017 Jan 4 [PubMed PMID: 28062268]
Adler Y, Ristić AD, Imazio M, Brucato A, Pankuweit S, Burazor I, Seferović PM, Oh JK. Cardiac tamponade. Nature reviews. Disease primers. 2023 Jul 20:9(1):36. doi: 10.1038/s41572-023-00446-1. Epub 2023 Jul 20 [PubMed PMID: 37474539]
Nahass M, Kassotis J. Constrictive Pericarditis. The New England journal of medicine. 2023 Nov 30:389(22):2087. doi: 10.1056/NEJMicm2301671. Epub [PubMed PMID: 38048190]
Gillombardo CB, Hoit BD. Constrictive pericarditis in the new millennium. Journal of cardiology. 2024 Apr:83(4):219-227. doi: 10.1016/j.jjcc.2023.09.003. Epub 2023 Sep 13 [PubMed PMID: 37714264]