Introduction
Anorectal abscess is an acute suppurative infection of the soft tissues around the anal canal and rectum that can cause significant discomfort in patients. These abscesses most commonly result from obstruction and infection of the glands in the anal crypt, a condition termed cryptoglandular etiology. The condition is more common in males who present with perianal pain and swelling, along with other symptoms depending on the location of the abscess.[1][2] Although anorectal abscess is used as an umbrella term to describe all the suppurative infections around the anal canal and the rectum, there are more specific terminologies to describe them.[3]
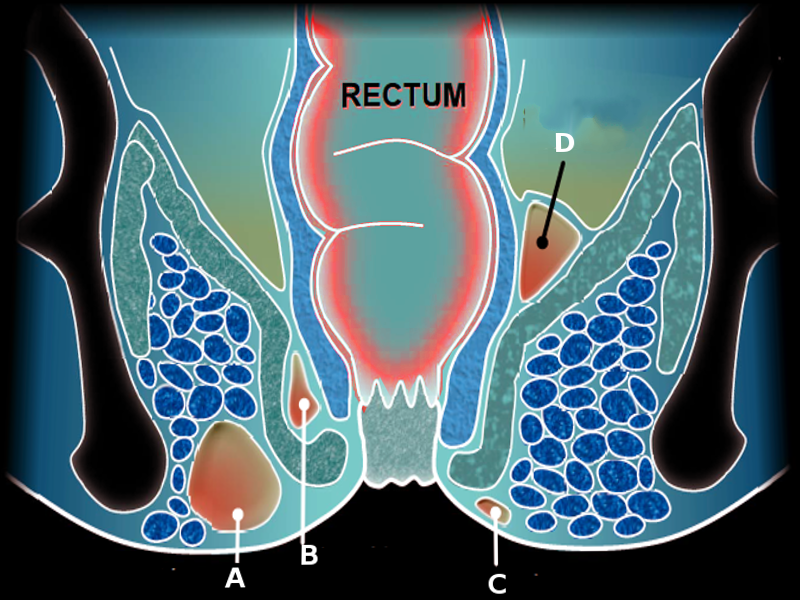
Anal glands are primarily located in the intersphincteric space; consequently, infection initially results in an intersphincteric abscess. This may either drain spontaneously through an internal opening in the anal canal or extend inferiorly into the perianal soft tissue, leading to a perianal abscess. When ruptured through the external sphincter into the ischiorectal or ischioanal fossa, it forms an ischiorectal or ischioanal abscess.
The cephalad extension of the interpshincteric abscess can result in a perirectal abscess or a supralevator abscess if it extends above the levator muscles. The posterior extension can cause a horseshoe abscess.[3][4] See Image. Perirectal Abscess. The diagnosis is often obvious on a thorough clinical examination, except for perirectal or supralevator abscesses that require imaging to establish an accurate diagnosis. Treatment almost always consists of surgical drainage of the abscess, and the approach varies based on the location and extent. Antibiotics are reserved for specific clinical scenarios only and are discussed below, along with the etiopathogenesis, evaluation, and treatment of anorectal abscess.[1]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The cryptoglandular hypothesis is the most common etiology of anorectal abscess. The risk factors for developing cryptoglandular anorectal abscess include smoking, obesity, and immunocompromised states, such as diabetes mellitus.[5] The pathogens commonly involved are Escherichia coli and Bacteroides species.[6] Patients with Crohn disease develop anorectal abscess secondary to a penetrating inflammation rather than infection.
Gram-positive bacteria, such as staphylococci and streptococci, are predominant in Crohn disease-associated perianal infections.[7][8] Locally advanced anorectal cancers, including anal canal and perianal squamous cell carcinoma, Buschke-Lowenstein tumor, basal cell carcinoma, anal melanoma, perianal Paget disease, mycosis fungoides, and anorectal adenocarcinoma, can lead to anorectal abscess.[9][10] See Image. Anal Carcinoma.
Similarly, perforation of the anorectum due to impacted chicken or fish bones, foreign bodies, or trauma can cause suppuration and abscess formation.[11] The other etiologies include perineal tuberculosis, perineal actinomycosis, and sexually transmitted infections such as lymphogranuloma venerum, and HIV.[12][13][14][15] Conditions causing pelvic sepsis, such as appendicitis, diverticulitis, and gynecological sepsis, can cause a supralevator abscess, which can extend inferiorly through the levators into the ischiorectal fossa.[11] Among patients presenting with an anorectal abscess, 30% to 70% have a concomitant fistula-in-ano, and those without an initial fistula will develop 1 in approximately 30% to 50% of cases within months to years.[2]
Epidemiology
The incidence of anorectal abscesses ranges from 68,000 to 96,000 cases per year in the United States.[11] However, the true incidence is likely higher due to multiple subclinical infections and spontaneous drainage. The common age of presentation is 20 to 60, with a mean age of 40 in both sexes. Men are affected twice as often as women.[11]
Pathophysiology
Cryptoglandular Abscess
Anal glands are located circumferentially within the internal sphincter, intersphincteric space, and the external sphincter, which drain into the crypts of Morgagni at the level of the dentate line. The cryptoglandular theory states that anorectal abscesses result from blockage of these glands, which increases pressure within them and allows bacterial translocation into the intersphincteric space (see Image. Anal Canal). Therefore, anorectal abscesses initially begin as intersphincteric abscesses, and the route of extension results in various types. The most common manifestation is a perianal abscess that occurs due to a downward extension of the abscess into the subcutaneous tissue around the anal verge. The second most common type is an ischiorectal abscess, which results from infection spreading into the ischiorectal fossa through the external sphincter. A submucosal abscess can occur due to the abscess penetrating the internal sphincter into the submucosal space of the anal canal. Rarely, the infection can extend upwards into the intersphincteric space, causing either a perirectal abscess or a supralevator abscess.[16][17]
Crohn Disease
The pathophysiology of anorectal abscesses secondary to Crohn disease depends on the host, microbial, and environmental factors. The luminal bacteria trigger an aberrant immune response, leading to persistent mucosal inflammation that promotes epithelial-mesenchymal transition and cell invasion, eventually causing abscess formation or fistulization.[18]
Tuberculosis
Mycobacteria reach the anorectal region either by direct inoculation or by hematogenous or lymphatic dissemination. The affected anoperineal region can present with suppuration and abscess formation, along with other presentations such as ulceration, verrucous, lupoid, and miliary lesions.[19]
Anorectal Malignancies
They lead to anorectal abscesses either by tumor obstruction of the anal glands, resulting in infection, or by direct infiltration into the perianal skin and soft tissue, causing necrosis and suppuration.[10]
Histopathology
Cryptoglandular anorectal abscess shows features such as inflammatory infiltrates, abundant neutrophils, and necrotic debris. However, those due to Crohn disease, tuberculosis, and malignancies demonstrate disease-specific features, including non-necrotizing granulomatous inflammation with giant cells (Crohn disease), tuberculoid granulomas with caseation necrosis and acid-fast bacilli (tuberculosis), and neoplastic cells (malignancies) (see Image. Histopathology of Cutaneous Crohn Disease). Therefore, histopathological examination is crucial in evaluating anorectal abscesses, especially those with recurrent infections, atypical presentations, or other high-risk features.
History and Physical
A disease-specific history and a complete physical examination, including perineal and digital rectal examination, should be performed in patients with suspected anorectal abscess. The clinical manifestations depend on the abscess location and any associated complications. Most patients present with perianal throbbing pain and swelling, which is generally not related to defecation. This is a hallmark symptom of a perianal abscess.[20]
Patients with intersphincteric and perirectal abscesses can, however, present with pain that is exacerbated during defecation. The pain may be referred to the perineum, lower back, or gluteal region.[21] There may be a history of spontaneous discharge of pus from the perianal region or from the anal canal.[22] Ischiorectal abscesses are usually large and can be associated with systemic features of sepsis.
Supralevator abscesses generally present with deep-seated pelvic pain along with fever and urinary symptoms such as increased frequency, dysuria, or urinary retention. Acute urinary retention can also occur due to mechanical obstruction or surrounding inflammation from a perianal and ischiorectal abscess.[23] History should also focus on determining baseline anal sphincter function, past anorectal operations, obstetric history, high-risk behavior, use of blood thinners, urinary and gynecological pathologies, and personal and family history of inflammatory bowel diseases and cancers.[2]
Physical examination should assess for systemic features of sepsis, such as fever, tachycardia, and malaise. The perineal examination will reveal erythema, warmth, induration, tenderness, and a fluctuant swelling in the perianal and ischiorectal fossa in respective abscesses. Previous surgical scars, external openings of a fistula, signs of perianal Crohn disease, and spontaneous discharge of pus or blood from the anal canal should also be checked.[24]
A gentle digital rectal examination (DRE) should be performed unless the patient is in severe pain; when indicated, consider performing anoscopy or proctoscopy, as deeper abscesses may have relatively unrevealing external findings. Severe tenderness with bogginess, typically at the 6 o'clock position on a DRE, is characteristic of an intersphincteric abscess.[25] Similarly, a tender fluctuant swelling at or above the level of the anorectal ring can be a subtle sign of a supralevator abscess.[26] Physical examination should also aid in ruling out the common causes of anal and perianal pain, such as anal fissure, hemorrhoids, hidradenitis, pilonidal sinus and abscess, sexually transmitted infections, and benign and malignant anorectal neoplasms.[2]
Evaluation
The evaluation of patients with anorectal abscesses includes laboratory investigations (including microbiology and histopathology when indicated) to determine the severity of infection, underlying risk factors, and etiology, as well as imaging studies for clinically occult abscesses. Laboratory studies should consist of a complete blood count, serum creatinine, inflammatory markers such as C-reactive protein, blood glucose levels, and HbA1c, even in patients with undetected diabetes mellitus.[27]
Routine diagnostic imaging is not recommended for all patients with an anorectal abscess. However, patients with occult abscesses, the presence of concomitant fistula, recurrent infections, immunocompromised states, and perineal Crohn disease should undergo imaging.[2] The modalities include perineal and anal endoscopic ultrasound (EUS), computed tomography (CT), and magnetic resonance imaging (MRI). The American College of Radiology appropriateness criteria recommends the use of MRI pelvis and CT pelvis as 'usually appropriate', EUS as 'may be appropriate', and radiography and fluoroscopy as 'usually not appropriate'.[3]
Ultrasound
Transperineal ultrasound is a noninvasive, readily available, and cost-effective diagnostic tool with high accuracy for diagnosing perianal, ischiorectal, and intersphincteric abscesses.[28] However, it does not provide any additional information beyond a good clinical examination and is not useful for deeper locations, such as supralevator or deep postanal abscesses. EUS has the advantage of identifying intersphincteric, perirectal, and supralevator abscesses with localization of the internal opening in the presence of a fistula. Still, it can be very painful for patients.[29] Both transperineal and EUS are operator-dependent and lack high-quality data to support their widespread use in anorectal abscesses.[30]
CT
A CT scan is useful for patients presenting with clinical symptoms of an anorectal abscess but without characteristic findings on examination. They are also useful for evaluating suspected supralevator, deep postanal, horseshoe, and perirectal abscesses and can guide the appropriate route for abscess drainage. The sensitivity of a CT scan in diagnosing anorectal abscess is approximately 77% and is even lower in immunocompromised individuals.[31] CT is inferior to MRI in the identification of an internal opening or the fistula tract. Despite these drawbacks, CT is an essential investigation that can be performed quickly, cost-effectively, and is readily available in emergencies.
MRI
MRI is the gold-standard imaging modality for most anorectal pathologies. This modality can help identify concealed tracts and abscesses and provide excellent anatomical orientation of the anal sphincter complex. Although its use in emergencies is not feasible due to cost, time, and availability constraints, it can assist in evaluating complex and recurrent abscesses, especially supralevator abscesses. Certain patient groups, such as those with Crohn disease, anorectal malignancies, and radiation proctitis, specifically benefit from MRI before surgical management (see Image. Anorectal Abscess on Magnetic Resonance Imaging).[32]
Treatment / Management
Patients with acute anorectal abscesses should be treated promptly with incision and drainage. The timing should be based on the presence and severity of sepsis, ideally within 24 hours.[27] Although this can be performed in the clinic setting as an outpatient or in the emergency department with local anesthetic infiltration (for small, superficial abscesses), all efforts should be made to perform an examination under anesthesia (EUA) before abscess drainage.[33] Extensive infections, deep-seated abscesses, and patient risk factors such as the use of blood thinners and multiple comorbid illnesses should be managed under anesthesia. Study results have shown reduced rates of recurrence and fistula formation when anorectal abscesses are managed in the operating room.[34] Needle aspiration of anorectal abscesses is not recommended due to the high rate of recurrence.[35](A1)
Operative Technique
For perianal and ischiorectal abscesses being managed in the outpatient setting, the patient is either placed in the lateral decubitus or knee-elbow position. For larger and deeper abscesses, and for those requiring EUA, lithotomy, Lloyd-Davies, or prone jackknife positions are preferred. In general, an incision should be made as close as possible to the anal verge to minimize potential fistula tract length, must be large enough to provide adequate drainage, and must avoid anal sphincter injury.[2] (A1)
Radial incisions from the anus are preferred, and the loculi must be broken either with a hemostat or a blunt probe.[36] To prevent premature closure of the skin, the incision can be made cruciate for an ischiorectal abscess, and an ellipse of skin can be excised for a perianal abscess. The cavity should be irrigated with saline, with or without hydrogen peroxide and povidone iodine, and hemostasis should be achieved using direct pressure, cautery, or lignocaine with adrenaline.[1] Following the drainage, the cavity can either be left open or a drain can be placed.[37] Study results show increased rates of postoperative pain with perianal packing after abscess drainage without any benefit in healing or fistula formation.[38] Therefore, routine postoperative packing, unless for hemostasis, is not recommended.(A1)
An intersphincteric abscess should be drained under sedation. This type of abscess can be felt as a posterior bulge in the anal canal, and the overlying mucosa should be incised to expose the internal sphincter. A right-angled or a Kelly forceps is used to gently spread the fibers of the internal sphincter to drain the abscess. This can be accompanied by dividing the internal sphincter muscle up to the dentate line to maintain the patency of the abscess cavity. The cavity can then be irrigated, and the wound left open.[39]
The surgical management of a supralevator abscess depends on its etiology and anatomical extent. Those occurring via the extension of the intersphincteric abscess superiorly can be drained internally into the anal canal. Supralevator abscesses that are formed due to the spread of ischiorectal abscess through the levators should be drained externally with a transperineal incision.[40] Rarely, supralevator abscesses can occur due to the spread of pelvic etiologies such as appendicitis, diverticulitis, and gynecological disorders. This may require ultrasound- or CT-guided transabdominal drain placement or, sometimes, laparotomy or a laparoscopic lavage.[1]
Horseshoe abscesses require specialized techniques as they most often involve the deep postanal space and extend laterally into the ischiorectal spaces. The modified Hanley procedure involves division of the anococcygeal ligament and placement of counter-incisions over the ischiorectal fossae, with multiple setons from the midline to the counter-incisions to aid drainage. If an internal opening is identified, another seton is placed from the midline to the internal opening.[41] Deep postanal abscesses without horseshoe extension can be managed like an intersphincteric abscess, accessing the cavity from the posterior anal canal.[42]
In general, it is not recommended to probe the abscess cavity with an attempt to identify a fistula tract.[2] However, when a fistula is evident during the drainage of anorectal abscess, the role of primary fistulotomy is controversial. Although fistulotomy can result in effectively managing the primary pathology, inflammatory edema and induration can cause false tracts while probing, and a risk of sphincter injury.[43] While simple fistulas may benefit from primary fistulotomy and have a negligible recurrence rate, complex and recurrent fistulas with abscesses carry a higher risk of postoperative fecal incontinence.[44](A1)
Therefore, primary fistulotomy with anorectal abscess drainage should be selected carefully based on the location and severity of the abscess and surgical expertise.[44] Partial fistulotomy and placement of a draining seton can be considered in patients with complex fistulas with abscesses. The procedure carries a low risk of sphincter injury, but needs to be followed by a staged fistulotomy subsequently.[45] Similarly, the role of ligation of the intersphincteric fistula tract (LIFT) during the index procedure has been studied in a small series, with results showing lower rates of nonhealing in patients undergoing LIFT.[46](A1)
Routine antibiotic use after adequate drainage of an anorectal abscess in a healthy patient is not recommended, as it does not improve healing rates or prevent recurrence. Antibiotics are reserved for patients with complications such as cellulitis, systemic sepsis, or immunocompromised states.[27] Prophylactic antibiotics before abscess drainage are recommended for patients with prosthetic valves, congenital heart disease, and previous bacterial endocarditis.[47] Most anorectal abscesses are polymicrobial, and culture results do not predict abscess recurrence, fistula formation, or change clinical management.[48] However, in immunocompromised patients and those with severe infections or nonhealing wounds, cultures may be obtained to guide antibiotic therapy, especially for methicillin-resistant Staphylococcus aureus, which is seen in up to 34.8% of patients.[49](B2)
Differential Diagnosis
The following conditions should be included in the differential diagnosis for anorectal abscesses:
- Perianal skin and soft tissue infections
- These include cellulitis, simple subcutaneous abscesses, carbuncles, folliculitis, Bartholin abscess, and infected sebaceous cysts. The clinical presentation is similar to that of an anorectal abscess, with acute pain, erythema, and fever. Local examination usually does not reveal any tender, fluctuant swelling in the perianal or ischorectal region, and DRE is often unremarkable.[50]
- Pilonidal abscess
- A pilonidal abscess can be misdiagnosed as a posterior or deep anal abscess. However, a pilonidal abscess is characteristically located in the midline at the natal cleft; the induration does not extend up to the anal verge, and DRE will be unremarkable.[51]
- Hidradenitis suppurativa
- This can be differentiated from an anorectal abscess by its features of deep-seated nodules, draining tracts, and indurated fibrotic scars.[52]
- Thrombosed external hemorrhoid
- This condition appears as a purplish swelling associated with enlarged external or internal hemorrhoids at the anal verge. The patient will have a long-standing history of a mass descending per rectum and bleeding during defecation. Pain may be an acute symptom exacerbated by straining or constipation.[53]
- Acute anal fissure
- This causes a sudden, sharp pain during defecation associated with the passage of fresh blood, with a throbbing pain lasting minutes to hours after defecation. Local examination reveals a longitudinal tear in the anoderm, usually at the 6 o'clock position of the anal verge, with a spasm of the anal sphincter.[54]
- Perianal Crohn disease
- The lesions appear as erosions over the perianal skin, inflammatory skin tags, or multiple external openings. DRE reveals indurated anal mucosa with an internal opening.[55]
- Anorectal malignancies
- Squamous cell carcinoma of the anal canal and the perianal skin, and anorectal adenocarcinoma present with ulceroproliferative growth at the anal verge associated with pain, bleeding, discharge, and anal incontinence. Clinical examination, imaging, and histopathological examination confirm the diagnosis.[9]
- Sexually transmitted infections
- They include gonorrhea, chlamydia, syphilis, herpes, and HIV infections. The clinical features include anorectal pain, tenesmus, pruritus ani, perianal vesicles and other skin lesions, and inguinal lymphadenopathy.[56]
Prognosis
With early and appropriate management, anorectal abscesses have a good prognosis. However, in immunocompromised individuals, those with Crohn disease, or those where the abscess is detected late and has progressed to a potentially life-threatening complication such as Fournier gangrene, morbidity and mortality can be significant.[57][58] Of patients presenting with an anorectal abscess, 30% to 70% have concomitant fistula-in-ano, and among those without an initial fistula, approximately 30% to 50% will develop 1 within subsequent months to years.[2]
Complications
The complications of anorectal abscess include sepsis, perineal cellulitis, necrotizing soft tissue infection, and Fournier gangrene, formation of fistula in ano, and fecal incontinence. Recurrence of anorectal abscesses and fistula formation could be as high as 50%.[59] The causes include inadequate drainage of the primary abscess, premature closure of the skin edges, missed abscesses, horseshoe abscesses, and obesity.[60][61][62] Surgical and postoperative complications include reactionary or secondary hemorrhage, acute urinary retention, surgical site infection, incontinence to feces or flatus, pudendal nerve injury, and anal stricture.[63]
Postoperative and Rehabilitation Care
Following the drainage of anorectal abscess, the patients need adequate analgesics, laxatives or fiber supplements to avoid constipation, and instructions regarding wound care. If intraoperative cultures or biopsies are taken, they must be followed up and discussed with the patients. Those managing their own wounds postoperatively should be advised to use absorbent dressings to cover the area, maintain proper hygiene, and use sitz baths to promote healing.[64]
Patients with transient dysfunction of the anal sphincter should be taught Keigle exercises and referred for physiotherapy. Use of a doughnut pillow should be encouraged while sitting to avoid direct pressure on the wound and associated pain. Because of a high recurrence rate, all patients should be followed postoperatively until the wound has completely healed, which may take up to 8 weeks. If there is a recurrent abscess or fistula formation, further evaluation is needed to identify underlying factors that may be contributing to poor healing, including Crohn disease, HIV, neoplasm, or other etiology.
Consultations
Anorectal abscesses often require surgical intervention, even if they drain spontaneously. Therefore, a general or colorectal surgeon should be consulted to evaluate the patient. Alternatively, an emergency medicine clinician may perform the drainage procedure themselves for small and superficial abscesses. If the abscess is recurrent or complex, a workup for underlying causes, such as Crohn disease, anorectal malignancies, and HIV, should be performed, with appropriate consultations to gastroenterology, oncology, or the infectious diseases unit as needed.
Deterrence and Patient Education
There are a few effective strategies to prevent anorectal abscess in an otherwise healthy patient. A high-fiber diet promotes regular bowel movements, helps prevent constipation, straining, and anal gland obstruction. Similarly, maintaining good perineal hygiene and preventing skin breakdown or moisture can help prevent anorectal abscess. Patients with diabetes should maintain strict glycemic control since it is a significant risk factor for developing cryptoglandular abscess.
If a patient has an underlying etiology such as Crohn disease, treatment with anti-tumor necrosis factor agents, especially infliximab, is associated with improved healing rates of perianal fistulas and reduced recurrence of abscesses when combined with surgical drainage and seton placement. Patients with sexually transmitted infections should be promptly evaluated and managed, including their partners.[55][65] Since anorectal abscess is an acute surgical emergency, patients with risk factors should be warned regarding the high-risk symptoms and counseled to seek immediate medical care.
Enhancing Healthcare Team Outcomes
Patients with anorectal abscesses experience significant pain and distress due to the sudden onset, rapid progression, and debilitating effects. When managed in the emergency room, a quick but effective history and a focused, thorough examination are crucial for making an accurate diagnosis. Although most types of anorectal abscesses, such as perianal, ischiorectal, and intersphincteric abscesses, are clinically evident, the more complex ones, like supralevator or deep postanal with horseshoe abscesses, need the reliance on imaging for their diagnosis.[1]
Emergency medicine physicians, general surgeons, advanced practitioners, nurses, pharmacists, and other health professionals involved in managing these patients should possess the essential knowledge and clinical skills to adequately diagnose and manage anorectal abscesses. Early recognition and treatment of patients are crucial in reducing morbidity. Patient education about the risk factors, preventive measures, symptoms, and complications is imperative.
When necessary, appropriate referral pathways must be initiated, such as a gastroenterology consultation for suspected inflammatory bowel disease, colorectal surgery for recurrent or complex abscesses, an infectious disease specialty for sexually transmitted infections, and oncology for primary malignancies causing anorectal abscesses. Effective interprofessional communication fosters a collaborative environment where information is shared, questions are encouraged, and concerns are addressed promptly. Care coordination is pivotal in ensuring seamless and efficient patient care. The involved specialties, including the surgeons, physicians, advanced practitioners, nurses, pharmacists, and other healthcare professionals, must work together to streamline the patient's journey, from diagnosis through treatment and follow-up. This coordination minimizes errors, reduces delays, and enhances patient safety, ultimately leading to improved outcomes and patient-centered care that prioritizes the well-being and satisfaction of those diagnosed with anorectal abscess.
Media
(Click Image to Enlarge)
Perirectal Abscess.
Contributed by O Chaigasame, MD
(Click Image to Enlarge)
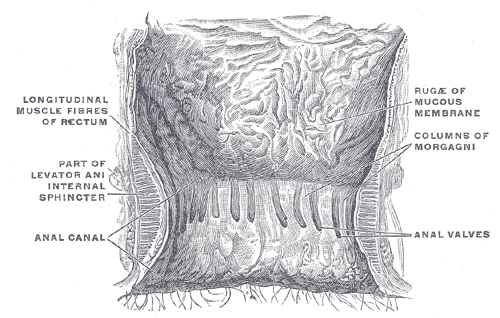
Anal Canal. This illustration shows a coronal view of the terminal rectum and anal canal. Prominent longitudinal muscle fibers of the rectum are visible. Other structures shown include the levator ani muscle, the internal sphincter, the anal canal, and the anal valves. The columns of Morgagni and the rugæ of the mucous membrane are also clearly depicted.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)

(Click Image to Enlarge)
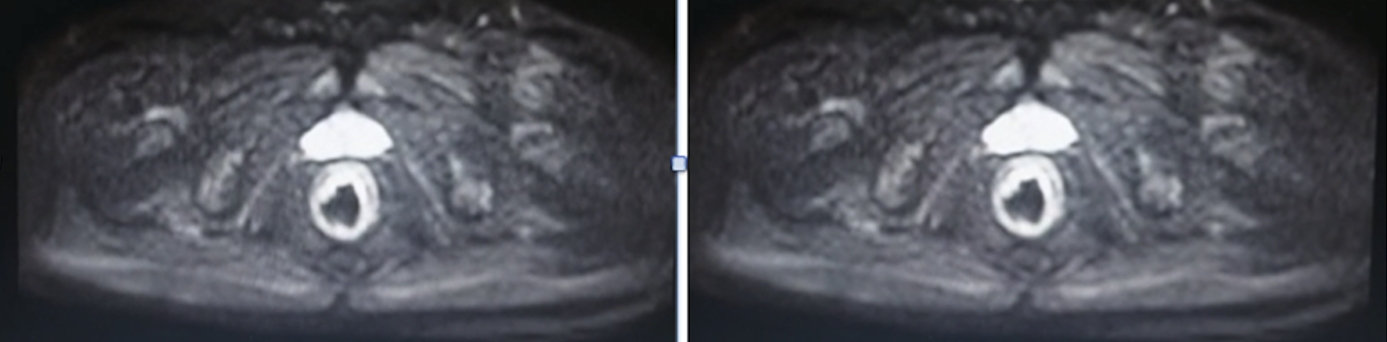
Anorectal Abscess on Magnetic Resonance Imaging. The MRI pelvis shows circumferential irregular thickening of the mucosa of the rectum with preserved stratification. The surrounding areas show increased inflammatory signs, including perirectal enhancement, fatty stranding, and edema.
Contributed by S El-Nakeep, MD
(Click Image to Enlarge)
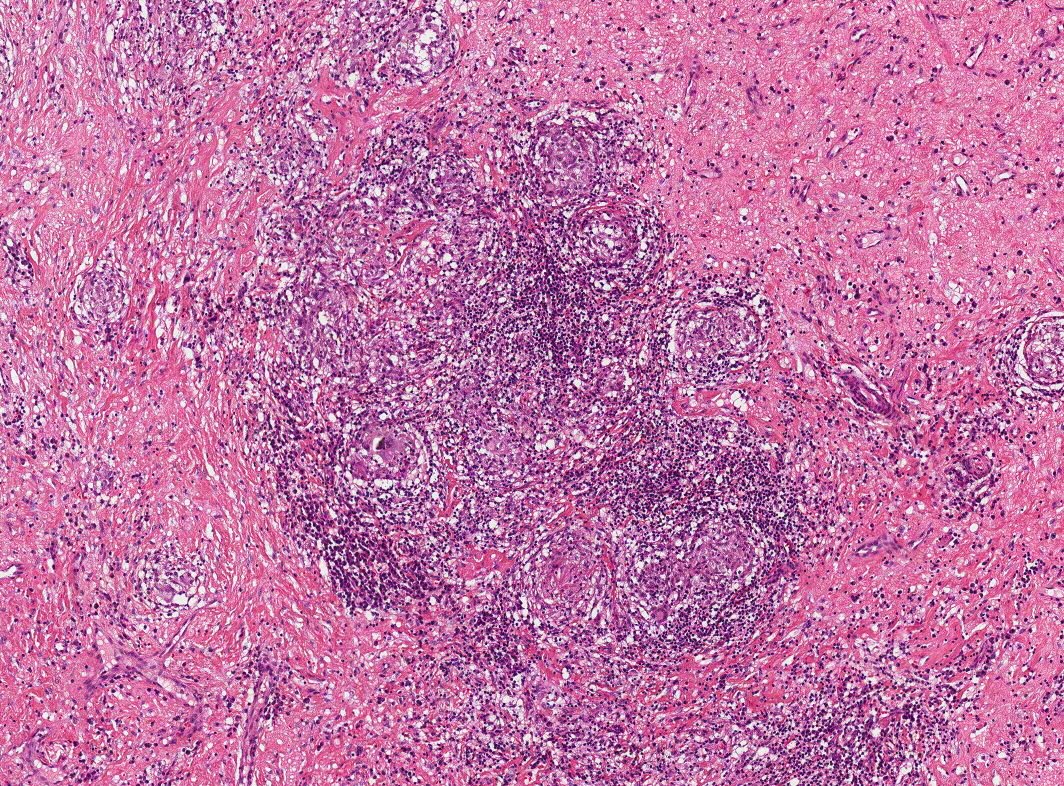
Histopathology of Cutaneous Crohn Disease. The image shows a histopathological biopsy of cutaneous lesions in Crohn disease, highlighting noncaseating granulomas.
Contributed by K Wanat, MD
References
Kata A, Abelson JS. Anorectal Abscess. Clinics in colon and rectal surgery. 2024 Nov:37(6):368-375. doi: 10.1055/s-0043-1777451. Epub 2023 Dec 8 [PubMed PMID: 39399133]
Gaertner WB, Burgess PL, Davids JS, Lightner AL, Shogan BD, Sun MY, Steele SR, Paquette IM, Feingold DL, Clinical Practice Guidelines Committee of the American Society of Colon and Rectal Surgeons. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Anorectal Abscess, Fistula-in-Ano, and Rectovaginal Fistula. Diseases of the colon and rectum. 2022 Aug 1:65(8):964-985. doi: 10.1097/DCR.0000000000002473. Epub 2022 Jul 5 [PubMed PMID: 35732009]
Level 1 (high-level) evidenceExpert Panel on Gastrointestinal Imaging, Levy AD, Liu PS, Kim DH, Fowler KJ, Bharucha AE, Chang KJ, Cilenti E, Gage KL, Garcia EM, Kambadakone AR, Korngold EK, Marin D, Moreno C, Pietryga JA, Santillan CS, Weinstein S, Wexner SD, Carucci LR. ACR Appropriateness Criteria® Anorectal Disease. Journal of the American College of Radiology : JACR. 2021 Nov:18(11S):S268-S282. doi: 10.1016/j.jacr.2021.08.009. Epub [PubMed PMID: 34794588]
Chawla A, Tan MO, Subramanian M, Bosco JI. The perianal "horseshoe". Abdominal radiology (New York). 2016 Jan:41(1):203-4. doi: 10.1007/s00261-015-0585-7. Epub [PubMed PMID: 26830625]
Adamo K, Gunnarsson U, Eeg-Olofsson K, Strigård K, Brännström F. Risk for developing perianal abscess in type 1 and type 2 diabetes and the impact of poor glycemic control. International journal of colorectal disease. 2021 May:36(5):999-1005. doi: 10.1007/s00384-020-03818-1. Epub 2020 Dec 17 [PubMed PMID: 33336291]
Sanchez-Haro E, Molinos S, Troya J, Tapiolas I, Vela S, Cardona PJ, Parés D. Bacteriology of Anorectal Abscess and Anal Fistula: A Systematic Review of the Literature. Surgical infections. 2025 Nov:26(9):707-719. doi: 10.1177/10962964251369451. Epub 2025 Aug 20 [PubMed PMID: 40833840]
Level 1 (high-level) evidenceWiese DM, Schwartz DA. Managing Perianal Crohn’s Disease. Current gastroenterology reports. 2012 Apr:14(2):153-61. doi: 10.1007/s11894-012-0243-y. Epub [PubMed PMID: 22302507]
West RL, Van der Woude CJ, Endtz HP, Hansen BE, Ouwedijk M, Boelens HA, Kusters JG, Kuipers EJ. Perianal fistulas in Crohn's disease are predominantly colonized by skin flora: implications for antibiotic treatment? Digestive diseases and sciences. 2005 Jul:50(7):1260-3 [PubMed PMID: 16047469]
Boaz E, Freund MR, Harbi A, Dagan A, Gilshtein H, Reissman P, Yellinek S. Anorectal Malignancies Presenting as a Perianal Abscess or Fistula. The American surgeon. 2023 Jun:89(6):2572-2576. doi: 10.1177/00031348221101481. Epub 2022 May 27 [PubMed PMID: 35621130]
Abbass MA, Valente MA. Premalignant and Malignant Perianal Lesions. Clinics in colon and rectal surgery. 2019 Sep:32(5):386-393. doi: 10.1055/s-0039-1687835. Epub 2019 Aug 22 [PubMed PMID: 31507349]
Abcarian H. Anorectal infection: abscess-fistula. Clinics in colon and rectal surgery. 2011 Mar:24(1):14-21. doi: 10.1055/s-0031-1272819. Epub [PubMed PMID: 22379401]
Kumari P, Datta A, Malik A, Sangma LCM, Sawale S, Arya AP, Das S. Anal tuberculosis presented as chronic perianal abscess in an immunocompetent adult: A rare case report. Journal of family medicine and primary care. 2024 Oct:13(10):4734-4736. doi: 10.4103/jfmpc.jfmpc_326_24. Epub 2024 Oct 18 [PubMed PMID: 39629447]
Level 3 (low-level) evidenceDosis A, Khan A, Leslie H, Musaad S, Smith A. Perianal Actinomycosis: A Surgeon's Perspective and Review of Literature. Annals of coloproctology. 2021 Oct:37(5):269-274. doi: 10.3393/ac.2021.00332.0047. Epub 2021 Oct 29 [PubMed PMID: 34731938]
Level 3 (low-level) evidenceGREAVES AB. THE FREQUENCY OF LYMPHOGRANULOMA VENEREUM IN PERSONS WITH PERIRECTAL ABSCESSES, FISTULAE IN ANO, OR BOTH. WITH PARTICULAR REFERENCE TO THE RELATIONSHIP BETWEEN PERIRECTAL ABSCESSES OF LYMPHOGRANULOMA ORIGIN IN THE MALE AND INVERSION. Bulletin of the World Health Organization. 1963:29(6):797-801 [PubMed PMID: 14107753]
Nadal SR, Manzione CR, Galvão VM, Salim VR, Speranzini MB. Perianal diseases in HIV-positive patients compared with a seronegative population. Diseases of the colon and rectum. 1999 May:42(5):649-54 [PubMed PMID: 10344688]
EISENHAMMER S. The internal anal sphincter and the anorectal abscess. Surgery, gynecology & obstetrics. 1956 Oct:103(4):501-6 [PubMed PMID: 13360660]
Winslett MC, Allan A, Ambrose NS. Anorectal sepsis as a presentation of occult rectal and systemic disease. Diseases of the colon and rectum. 1988 Aug:31(8):597-600 [PubMed PMID: 3402285]
Cao S, Colonna M, Deepak P. Pathogenesis of Perianal Fistulising Crohn's Disease: Current Knowledge, Gaps in Understanding, and Future Research Directions. Journal of Crohn's & colitis. 2023 Jun 16:17(6):1010-1022. doi: 10.1093/ecco-jcc/jjad008. Epub [PubMed PMID: 36655753]
Level 3 (low-level) evidenceBelhaj A, Omry A, Touati MD, Othmane MRB, Saidani A, Chebbi F. Diagnostic and therapeutic challenges in isolated perianal tuberculosis: A case report and comprehensive management overview. International journal of surgery case reports. 2024 Jun:119():109770. doi: 10.1016/j.ijscr.2024.109770. Epub 2024 May 17 [PubMed PMID: 38761692]
Level 3 (low-level) evidenceMarcus RH, Stine RJ, Cohen MA. Perirectal abscess. Annals of emergency medicine. 1995 May:25(5):597-603 [PubMed PMID: 7741334]
Chrabot CM, Prasad ML, Abcarian H. Recurrent anorectal abscesses. Diseases of the colon and rectum. 1983 Feb:26(2):105-8 [PubMed PMID: 6822168]
Read DR, Abcarian H. A prospective survey of 474 patients with anorectal abscess. Diseases of the colon and rectum. 1979 Nov-Dec:22(8):566-8 [PubMed PMID: 527452]
Updike SW, Sletten Z. Occult Perirectal Abscess Causing Acute Urinary Retention. Cureus. 2021 Jan 3:13(1):e12461. doi: 10.7759/cureus.12461. Epub 2021 Jan 3 [PubMed PMID: 33552778]
Klein JW. Common anal problems. The Medical clinics of North America. 2014 May:98(3):609-23. doi: 10.1016/j.mcna.2014.01.011. Epub 2014 Mar 21 [PubMed PMID: 24758964]
Parks AG, Thomson JP. Intersphincteric abscess. British medical journal. 1973 Jun 2:2(5865):537-9 [PubMed PMID: 4714472]
Prasad ML, Read DR, Abcarian H. Supralevator abscess: diagnosis and treatment. Diseases of the colon and rectum. 1981 Sep:24(6):456-61 [PubMed PMID: 7273983]
Tarasconi A, Perrone G, Davies J, Coimbra R, Moore E, Azzaroli F, Abongwa H, De Simone B, Gallo G, Rossi G, Abu-Zidan F, Agnoletti V, de'Angelis G, de'Angelis N, Ansaloni L, Baiocchi GL, Carcoforo P, Ceresoli M, Chichom-Mefire A, Di Saverio S, Gaiani F, Giuffrida M, Hecker A, Inaba K, Kelly M, Kirkpatrick A, Kluger Y, Leppäniemi A, Litvin A, Ordoñez C, Pattonieri V, Peitzman A, Pikoulis M, Sakakushev B, Sartelli M, Shelat V, Tan E, Testini M, Velmahos G, Wani I, Weber D, Biffl W, Coccolini F, Catena F. Anorectal emergencies: WSES-AAST guidelines. World journal of emergency surgery : WJES. 2021 Sep 16:16(1):48. doi: 10.1186/s13017-021-00384-x. Epub 2021 Sep 16 [PubMed PMID: 34530908]
Plaikner M, Loizides A, Peer S, Aigner F, Pecival D, Zbar A, Kremser C, Gruber H. Transperineal ultrasonography as a complementary diagnostic tool in identifying acute perianal sepsis. Techniques in coloproctology. 2014 Feb:18(2):165-71. doi: 10.1007/s10151-013-1031-x. Epub 2013 May 17 [PubMed PMID: 23681302]
Level 2 (mid-level) evidenceWeisman N, Abbas MA. Prognostic value of endoanal ultrasound for fistula-in-ano: a retrospective analysis. Diseases of the colon and rectum. 2008 Jul:51(7):1089-92. doi: 10.1007/s10350-008-9284-6. Epub 2008 May 7 [PubMed PMID: 18461397]
Level 2 (mid-level) evidenceBor R, Farkas K, Bálint A, Szűcs M, Ábrahám S, Milassin Á, Rutka M, Nagy F, Milassin P, Szepes Z, Molnár T. Prospective Comparison of Magnetic Resonance Imaging, Transrectal and Transperineal Sonography, and Surgical Findings in Complicated Perianal Crohn Disease. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 2016 Nov:35(11):2367-2372 [PubMed PMID: 27629757]
Caliste X, Nazir S, Goode T, Street JH 3rd, Hockstein M, McArthur K, Trankiem CT, Sava JA. Sensitivity of computed tomography in detection of perirectal abscess. The American surgeon. 2011 Feb:77(2):166-8 [PubMed PMID: 21337873]
Garcia-Granero A, Granero-Castro P, Frasson M, Flor-Lorente B, Carreño O, Espí A, Puchades I, Garcia-Granero E. Management of cryptoglandular supralevator abscesses in the magnetic resonance imaging era: a case series. International journal of colorectal disease. 2014 Dec:29(12):1557-64. doi: 10.1007/s00384-014-2028-2. Epub 2014 Oct 24 [PubMed PMID: 25339133]
Level 2 (mid-level) evidenceRobinson AM Jr, DeNobile JW. Anorectal abscess and fistula-in-ano. Journal of the National Medical Association. 1988 Nov:80(11):1209-13 [PubMed PMID: 3074175]
Narayanan S, Althans AR, Reitz KM, Allen LH, Kurukulasuriya C, Larkin TM, Reinert NJ, Cunningham KE, Watson AR, Celebrezze JP, Medich DS, Holder-Murray J. Drainage of anorectal abscesses in the operating room is associated with a decreased risk of abscess recurrence and fistula formation. American journal of surgery. 2023 Feb:225(2):347-351. doi: 10.1016/j.amjsurg.2022.09.005. Epub 2022 Sep 8 [PubMed PMID: 36150906]
Sørensen KM, Möller S, Qvist N. Needle aspiration treatment vs. incision of acute simple perianal abscess: randomized controlled study. International journal of colorectal disease. 2021 Mar:36(3):581-588. doi: 10.1007/s00384-021-03845-6. Epub 2021 Jan 15 [PubMed PMID: 33447866]
Level 1 (high-level) evidenceWhiteford MH. Perianal abscess/fistula disease. Clinics in colon and rectal surgery. 2007 May:20(2):102-9. doi: 10.1055/s-2007-977488. Epub [PubMed PMID: 20011384]
Zhu DA, Houlihan LM, Mohan HM, McCourt M, Andrews E. Packing versus mushroom catheters following incision and drainage in anorectal abscess. Irish journal of medical science. 2019 Nov:188(4):1343-1348. doi: 10.1007/s11845-018-01958-6. Epub 2019 Jan 23 [PubMed PMID: 30675692]
Newton K, Dumville J, Briggs M, Law J, Martin J, Pearce L, Kirwan C, Pinkney T, Needham A, Jackson R, Winn S, McCulloch H, Hill J, PPAC2 Collaborators. Postoperative Packing of Perianal Abscess Cavities (PPAC2): randomized clinical trial. The British journal of surgery. 2022 Sep 9:109(10):951-957. doi: 10.1093/bjs/znac225. Epub [PubMed PMID: 35929816]
Level 1 (high-level) evidenceMillan M, García-Granero E, Esclápez P, Flor-Lorente B, Espí A, Lledó S. Management of intersphincteric abscesses. Colorectal disease : the official journal of the Association of Coloproctology of Great Britain and Ireland. 2006 Nov:8(9):777-80 [PubMed PMID: 17032324]
Zinicola R, Cracco N. Draining an anal abscess: the skeletal muscle rule. Colorectal disease : the official journal of the Association of Coloproctology of Great Britain and Ireland. 2014 Jul:16(7):562. doi: 10.1111/codi.12651. Epub [PubMed PMID: 24774196]
Browder LK, Sweet S, Kaiser AM. Modified Hanley procedure for management of complex horseshoe fistulae. Techniques in coloproctology. 2009 Dec:13(4):301-6. doi: 10.1007/s10151-009-0539-6. Epub 2009 Oct 8 [PubMed PMID: 19813077]
Tan KK, Koh DC, Tsang CB. Managing Deep Postanal Space Sepsis via an Intersphincteric Approach: Our Early Experience. Annals of coloproctology. 2013 Apr:29(2):55-9. doi: 10.3393/ac.2013.29.2.55. Epub 2013 Apr 30 [PubMed PMID: 23700571]
McElwain JW, MacLean MD, Alexander RM, Hoexter B, Guthrie JF. Anorectal prlblems: experience with primary fistulectomy for anorectal abscess, a report of 1,000 cases. Diseases of the colon and rectum. 1975 Nov-Dec:18(8):646-9 [PubMed PMID: 1192907]
Level 3 (low-level) evidenceMalik AI, Nelson RL, Tou S. Incision and drainage of perianal abscess with or without treatment of anal fistula. The Cochrane database of systematic reviews. 2010 Jul 7:(7):CD006827. doi: 10.1002/14651858.CD006827.pub2. Epub 2010 Jul 7 [PubMed PMID: 20614450]
Level 1 (high-level) evidenceWang C, Rosen L. Management of low transsphincteric anal fistula with serial setons and interval muscle-cutting fistulotomy. Journal of integrative medicine. 2016 Mar:14(2):154-8. doi: 10.1016/S2095-4964(16)60229-7. Epub [PubMed PMID: 26988437]
Rojanasakul A, Booning N, Huimin L, Pongpirul K, Sahakitrungruang C. Intersphincteric Exploration With Ligation of Intersphincteric Fistula Tract or Attempted Closure of Internal Opening for Acute Anorectal Abscesses. Diseases of the colon and rectum. 2021 Apr 1:64(4):438-445. doi: 10.1097/DCR.0000000000001867. Epub [PubMed PMID: 33394781]
Wilson W, Taubert KA, Gewitz M, Lockhart PB, Baddour LM, Levison M, Bolger A, Cabell CH, Takahashi M, Baltimore RS, Newburger JW, Strom BL, Tani LY, Gerber M, Bonow RO, Pallasch T, Shulman ST, Rowley AH, Burns JC, Ferrieri P, Gardner T, Goff D, Durack DT, American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, American Heart Association Council on Cardiovascular Disease in the Young, American Heart Association Council on Clinical Cardiology, American Heart Association Council on Cardiovascular Surgery and Anesthesia, Quality of Care and Outcomes Research Interdisciplinary Working Group. Prevention of infective endocarditis: guidelines from the American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation. 2007 Oct 9:116(15):1736-54 [PubMed PMID: 17446442]
Level 2 (mid-level) evidenceXu RW, Tan KK, Chong CS. Bacteriological study in perianal abscess is not useful and not cost-effective. ANZ journal of surgery. 2016 Oct:86(10):782-784. doi: 10.1111/ans.13630. Epub 2016 May 25 [PubMed PMID: 27226422]
Albright JB, Pidala MJ, Cali JR, Snyder MJ, Voloyiannis T, Bailey HR. MRSA-related perianal abscesses: an underrecognized disease entity. Diseases of the colon and rectum. 2007 Jul:50(7):996-1003 [PubMed PMID: 17525863]
Silverberg B. A Structured Approach to Skin and Soft Tissue Infections (SSTIs) in an Ambulatory Setting. Clinics and practice. 2021 Feb 1:11(1):65-74. doi: 10.3390/clinpract11010011. Epub 2021 Feb 1 [PubMed PMID: 33535501]
Surrell JA. Pilonidal disease. The Surgical clinics of North America. 1994 Dec:74(6):1309-15 [PubMed PMID: 7985066]
Ben-Aharon U, Fridland M, Chatsubi I, Wechsler U. [Hidradenitis suppurativa involving the perineal region]. Harefuah. 1991 Jan 15:120(2):74-6 [PubMed PMID: 2007493]
Sammarco G, Trompetto M, Gallo G. Thrombosed External Haemorrhoids: A Clinician's Dilemma. Reviews on recent clinical trials. 2019:14(4):232-234. doi: 10.2174/1574887114666190927163646. Epub [PubMed PMID: 31560294]
Fritz S, Kirsch J, Schneider N, Kirsch J, Reissfelder C, Herold A, Bussen D. Therapy and long-term outcomes of acute anal fissure: a high-volume referral centre experience with 623 patients. Techniques in coloproctology. 2026 Jan 6:30(1):14. doi: 10.1007/s10151-025-03238-9. Epub 2026 Jan 6 [PubMed PMID: 41493654]
Parian AM, Obi M, Fleshner P, Schwartz DA. Management of Perianal Crohn's Disease. The American journal of gastroenterology. 2023 Aug 1:118(8):1323-1331. doi: 10.14309/ajg.0000000000002326. Epub 2023 Jun 19 [PubMed PMID: 37207318]
Assi R, Hashim PW, Reddy VB, Einarsdottir H, Longo WE. Sexually transmitted infections of the anus and rectum. World journal of gastroenterology. 2014 Nov 7:20(41):15262-8. doi: 10.3748/wjg.v20.i41.15262. Epub [PubMed PMID: 25386074]
Mak WY, Mak OS, Lee CK, Tang W, Leung WK, Wong MTL, Sze ASF, Li M, Leung CM, Lo FH, Lam BCY, Chan KH, Shan EHS, Tsang SWC, Hui AJ, Chow WH, Chan FKL, Sung JJY, Ng SC. Significant Medical and Surgical Morbidity in Perianal Crohn's Disease: Results from a Territory-Wide Study. Journal of Crohn's & colitis. 2018 Nov 28:12(12):1392-1398. doi: 10.1093/ecco-jcc/jjy120. Epub [PubMed PMID: 30165543]
Chen Y, Wang X, Lin G, Xiao R. Successful treatment following early recognition of a case of Fournier's scrotal gangrene after a perianal abscess debridement: a case report. Journal of medical case reports. 2018 Jun 27:12(1):193. doi: 10.1186/s13256-018-1697-9. Epub 2018 Jun 27 [PubMed PMID: 29945675]
Level 3 (low-level) evidenceSanchez-Haro E, Vela E, Cleries M, Vela S, Tapiolas I, Troya J, Julian JF, Parés D. Clinical characterization of patients with anal fistula during follow-up of anorectal abscess: a large population-based study. Techniques in coloproctology. 2023 Oct:27(10):897-907. doi: 10.1007/s10151-023-02840-z. Epub 2023 Aug 7 [PubMed PMID: 37548781]
Yano T, Asano M, Matsuda Y, Kawakami K, Nakai K, Nonaka M. Prognostic factors for recurrence following the initial drainage of an anorectal abscess. International journal of colorectal disease. 2010 Dec:25(12):1495-8. doi: 10.1007/s00384-010-1011-9. Epub 2010 Jul 17 [PubMed PMID: 20640431]
Onaca N, Hirshberg A, Adar R. Early reoperation for perirectal abscess: a preventable complication. Diseases of the colon and rectum. 2001 Oct:44(10):1469-73 [PubMed PMID: 11598476]
Level 2 (mid-level) evidenceLu D, Lu L, Cao B, Li Y, Cao Y, Li Z, Wang Z, Lu J. Relationship Between Body Mass Index and Recurrence/Anal Fistula Formation Following Initial Operation for Anorectal Abscess. Medical science monitor : international medical journal of experimental and clinical research. 2019 Oct 23:25():7942-7950. doi: 10.12659/MSM.917836. Epub 2019 Oct 23 [PubMed PMID: 31642447]
Kunitake H, Poylin V. Complications Following Anorectal Surgery. Clinics in colon and rectal surgery. 2016 Mar:29(1):14-21. doi: 10.1055/s-0035-1568145. Epub [PubMed PMID: 26929747]
Smith SR, Newton K, Smith JA, Dumville JC, Iheozor-Ejiofor Z, Pearce LE, Barrow PJ, Hancock L, Hill J. Internal dressings for healing perianal abscess cavities. The Cochrane database of systematic reviews. 2016 Aug 26:2016(8):CD011193. doi: 10.1002/14651858.CD011193.pub2. Epub 2016 Aug 26 [PubMed PMID: 27562822]
Level 1 (high-level) evidenceLichtenstein GR, Loftus EV, Afzali A, Long MD, Barnes EL, Isaacs KL, Ha CY. ACG Clinical Guideline: Management of Crohn's Disease in Adults. The American journal of gastroenterology. 2025 Jun 3:120(6):1225-1264. doi: 10.14309/ajg.0000000000003465. Epub 2025 Jun 3 [PubMed PMID: 40701562]