Introduction
A Pancoast tumor is a neoplasm arising in the superior sulcus (apex) of the lung that invades adjacent structures of the thoracic inlet. The superior sulcus is an anatomic pleuropulmonary groove formed by the subclavian artery as it curves anterior to the pleura and courses upward and laterally beneath the lung apex. Because of this location, Pancoast tumors frequently extend into the chest wall, brachial plexus, and sympathetic nerves, producing a characteristic pattern of local invasion and symptoms not typically seen with other lung cancers.[1][2]
The natural history of Pancoast tumors often involves a prolonged asymptomatic period, with symptoms typically arising only when the tumor becomes large enough to invade nearby structures. Common symptoms include shoulder pain, Horner syndrome, and weakness or atrophy of the hand muscles, also referred to as Pancoast-Tobias syndrome.[3] Local invasion of the tumor into the brachial plexus and sympathetic chain produces these manifestations. Sympathetic nervous system involvement leads to the classic signs of Horner syndrome (ptosis, miosis, and anhidrosis on the affected side). Although initially localized, Pancoast tumors can be biologically aggressive and may metastasize to regional lymph nodes and distant organs, contributing to substantial morbidity and, if untreated, a poor prognosis. Pancoast tumors represent a distinct subset of lung cancer defined by their apical location, neurovascular involvement, and unique symptom complex. Early recognition and timely, interdisciplinary evaluation, including thoracic surgery, medical oncology, and radiation oncology, are essential to optimize staging, enable curative multimodality therapy, and improve patient outcomes.[4]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Pancoast tumors are primary lung cancers arising in the apical region of the lung, also known as the superior sulcus, and account for approximately 3% to 5% of all lung cancers. Most Pancoast tumors are non–small cell lung cancers (NSCLC), which represent more than 95% of reported cases. Consequently, Pancoast tumors are best regarded as a distinct clinical and anatomical subset of NSCLC that warrants special consideration due to their proximity to the brachial plexus, sympathetic chain, and chest wall.
Pancoast syndrome, the characteristic constellation of shoulder and arm pain, Horner syndrome, and hand muscle weakness, is most commonly caused by apical lung cancer but is not exclusive to this etiology. Other etiologies include pleural mesothelioma, metastatic disease to the lung apex (such as from malignant neoplasms or lymphomas of the thyroid), and inflammatory or infectious processes involving the apical pleura or chest wall (for example, infections due to Pseudomonas, Staphylococcus, or Actinomyces spp). Recognizing this differential diagnosis is important, as nonmalignant conditions can occasionally mimic the clinical picture of a Pancoast tumor.[5]
Epidemiology
According to the American Society of Clinical Oncology, an estimated 234,580 new cases of lung cancer were diagnosed in 2024, making it the second most common cancer and the main cause of oncological mortality in both sexes. Lung cancer is also the most lethal cancer in the US, with approximately 125,070 deaths annually. Pancoast tumors account for roughly 3% to 5% of all lung cancers.[6] The average age of presentation of a Pancoast tumor is in the sixth decade, and it occurs more commonly in men than in women.
Pathophysiology
More than 95% of lung cancers are classified into 4 major histologic types: adenocarcinoma, squamous cell carcinoma, large cell carcinoma, and small cell lung cancer. Approximately 80% to 85% of all lung cancers are non–small cell lung cancers, with adenocarcinoma now the most common subtype in many regions. Pancoast tumors represent a small subset of lung cancers, accounting for roughly 3% to 5% of cases and arising predominantly in the superior sulcus. More than 95% of Pancoast tumors are non–small cell lung cancers, most commonly adenocarcinoma and squamous cell carcinoma; small cell histology is distinctly uncommon, reported in up to 3% to 5% of cases. Historically, squamous cell carcinoma was the predominant histologic subtype in this location, but results from contemporary series demonstrate a shift toward adenocarcinoma predominance, mirroring broader trends in lung cancer epidemiology.[7]
Histopathology
Clinical symptoms and imaging findings can diagnose more than 90% of cases of Pancoast tumor. However, a biopsy is necessary for histologic confirmation and treatment planning before starting treatment. Currently, close to 95% of biopsies are performed via CT- or ultrasonography-guided percutaneous transthoracic needle biopsy.[8] Video-assisted thoracoscopy (VAT) or sometimes thoracotomy may be necessary when a percutaneous biopsy is inconclusive.[4]
Overall, the majority of Pancoast tumors are non–small cell lung carcinomas. Small cell carcinoma at this site is uncommon, accounting for no more than approximately 5% of cases. About half of Pancoast tumors are adenocarcinomas, with most of the remaining cases being squamous cell carcinomas. Historically, squamous cell carcinoma was the predominant histology, but results from contemporary series show adenocarcinoma to be more frequent, paralleling broader epidemiologic shifts in lung cancer.[9]
History and Physical
Most presenting symptoms are due to local tumor invasion. Given anatomical proximity, Pancoast tumors may cause symptoms secondary to neurological involvement (brachial plexus, Horner syndrome) and musculoskeletal symptoms (shoulder pain, vertebral, or rib pain).[1] The frequently deceptive nature of these symptoms poses a significant diagnostic challenge because pulmonary signs such as cough, dyspnea, and hemoptysis are often absent, especially in the early stages, prompting clinicians to consider orthopedic or neurological diagnoses first. Because of this, patients are often initially incorrectly diagnosed with cervical disc disease, rotator cuff pathology, or frozen shoulder.[10]
Shoulder pain is present in up to 96% of patients and is the most common initial presenting symptom. The pain may be secondary to invasion of the brachial plexus, pleural invasion, or extension into ribs or vertebral bodies, and is generally progressive. Shoulder pain may radiate to the head and neck, axilla, scapula, anterior chest, or arm (weakness in the ulnar nerve distribution and intrinsic muscles of the hand).
Horner syndrome is a combination of ipsilateral ptosis (drooping or falling of the upper eyelid), miosis (persistent constricted pupil), and anhidrosis (inability to sweat on the ipsilateral side). Pancoast tumor causes second-order (preganglionic) Horner syndrome (affecting the second-order neuron, traveling from the sympathetic trunk through the brachial plexus over the lung apex).[11] Ipsilateral facial flushing and sweating can occur before the development of full-blown Horner syndrome, likely due to tumor irritation of the sympathetic chain before invasion of the sympathetic trunk.[1]
In approximately 5% of patients, the tumor may extend into the intervertebral foramina, causing paraplegia and spinal cord compression.[1] Tumor extension into surrounding nerve roots, especially ulnar nerve roots (C8 and T1), occurs in approximately 8% to 22% of Pancoast tumors, which may result in weakness and atrophy of the intrinsic muscles of the hand, paresthesia over the distribution of the fourth and fifth digits of the hand, and the medial aspect of the arm and forearm. In some cases, the patient may exhibit a loss of the triceps reflex.[12]
Evaluation
Pancoast tumor constitutes a group of malignant neoplasms (as the tumor is classified based on location), which means no specific laboratory test exists to diagnose a Pancoast tumor. An initial plain radiological examination with a chest radiograph is generally used to screen a patient with a suspected Pancoast tumor or as an incidental finding showing soft tissue opacity at the apex of the lung (unilateral); an asymmetry in the apices greater than 5 mm can also be noted. Local rib extension can sometimes be appreciated (see Image. Pancoast Tumor). Lordotic chest views may be helpful. In the early stages, these findings are difficult to appreciate on the posteroanterior view of a chest radiograph because of difficulty in interpreting the overlying shadows at the apices (clavicle, scapula, acromion, and first rib).
CT scan provides more information on the extent of the primary tumor, mediastinal lymphadenopathy, and satellite tumors, which is essential for staging the tumor. CT scan has poor sensitivity and specificity for accurate local staging, but is excellent at identifying bony involvement. Furthermore, MRI is far more sensitive and specific for local staging due to its superior delineation of the extent of involvement in lung tissue, surrounding blood vessels, spinal cord, and brachial plexus. Please see StatPearls' companion reference, "Pancoast Syndrome," for further information. Careful assessment of the brachial plexus is needed as the involvement extending beyond the lower trunk, or C8 nerve root, is deemed inoperable.[13]
Positron emission tomography–computed tomography (PET-CT) is valuable for baseline staging in patients with Pancoast tumors. PET-CT improves the detection of mediastinal nodal involvement and distant metastases, thereby altering resectability assessment and overall treatment strategy. Additionally, integrated PET-CT facilitates more accurate delineation of the gross tumor volume by distinguishing metabolically active tumor from adjacent atelectasis or normal tissue, thereby refining target definition for radiotherapy planning and potentially reducing interobserver variability.[14][15] Chest CT and PET-CT scans are considered mandatory before and after preoperative therapy, but recommendations vary on whether mediastinoscopy, endobronchial ultrasonography, or esophageal ultrasonography is necessary.[16]
Treatment / Management
In the late 1950s, bimodality therapy (external beam radiation therapy before surgery) was the standard of care. In the 1990s, induction chemoradiotherapy, which was followed by resection, was proven to be an effective regimen for pancoast tumors (stage III non-small cell lung cancer, NSCLC).[17] Since then, the standard treatment for superior sulcus tumors has included a combination of induction concurrent chemoradiotherapy followed by radical en bloc resection of the tumor, and then completion of the chemotherapy regimen. Please see StatPearls' companion reference, "Lung Pancoast Tumor," for further information.
Induction chemotherapy includes combination chemotherapeutic drugs such as cisplatin and etoposide, cisplatin and paclitaxel, or cisplatin and pemetrexed with concurrent radiotherapy. Usually, 2 cycles of chemotherapy are given with concurrent radiation, while 2 cycles are given after the surgical procedure in an adjuvant setting.[18] Thoracic radiotherapy is given at 45 to 50 Gy in 25 to 28 fractions over 5 to 6 weeks, followed by the surgical procedure 3 to 5 weeks after completion of chemoradiotherapy.[19](B2)
Differential Diagnosis
Several pathologies other than primary lung cancer may present as Pancoast tumors, including the following:
Surgical Oncology
Since the approval of induction chemoradiotherapy followed by a surgical procedure, en bloc resection of the chest wall lesion is recommended in all cases of pancoast tumors. [9] Determination of resectability, surgical staging, and pulmonary resection should be performed by thoracic surgeons who perform lung cancer procedures as a prominent part of their practice.[26]
Radiation Oncology
Previously, radiation therapy in the neoadjuvant or induction setting was delivered up to 45 Gy in 25 fractions, but beginning in 2018, technological advancements enabled the use of intensity-modulated arc therapy, allowing a dose escalation to 50.4 Gy in 28 fractions.[22]
Pertinent Studies and Ongoing Trials
Recently, medical oncologists have been evaluating the efficacy of immunotherapy as part of induction chemoradiotherapy for these patients.[27][28] So far, only early-phase 2 trials have been conducted due to the rarity of Pancoast tumors, and data are generally extrapolated from stage III lung cancer trials.
Medical Oncology
Treatment of Pancoast tumors is based on tumor, node, metastasis (TNM) staging and assessment of resectability. For resectable disease, standard treatment is induction concurrent chemoradiotherapy followed by surgical resection with negative margins.[29] Unresectable cases are treated with definitive concurrent chemoradiotherapy, with consideration of consolidation immunotherapy, as in the Patients With Unresectable Stage III Non–Small-Cell Lung Cancer (PACIFIC) trial.[30] Metastatic disease is managed with systemic therapy, including chemotherapy, immunotherapy, or targeted therapy based on molecular profile.[31] Interdisciplinary care and effective pain control are essential due to frequent chest wall and brachial plexus involvement.
Staging
Pancoast tumors are staged according to the standard TNM system for non–small cell lung cancer because they represent an anatomic subset of NSCLC. Pancoast tumors are most often classified as T3 or T4 owing to their apical location and propensity for local invasion into adjacent structures. T3 disease typically reflects invasion of the chest wall or parietal pleura, whereas T4 denotes more extensive involvement, such as invasion of the vertebral bodies, major subclavian vessels, or brachial plexus. Nodal status is categorized as N0 to N3 based on the presence and location of regional lymph node metastases, and distant metastatic spread is captured by the M category (M0 or M1). At presentation, most Pancoast tumors are stage 2B or stage 3, consistent with locally advanced disease driven by early involvement of chest wall and neurovascular structures.[4]
Prognosis
The main factors affecting prognosis in patients with Pancoast tumor undergoing trimodal treatment (surgery, chemotherapy, and radiotherapy) are:
- The T-status of the tumor (worse for T4 tumors)
- Response to induction treatment (better for complete responders)
- Completeness of resection (dependent on T-status of tumor and response of the tumor to induction treatment)[32]
Longer duration of disease, the presence of Horner syndrome, the extension of tumor into the base of the neck, vertebral bodies, or great vessels, the involvement of mediastinal lymph nodes, and resection of the tumor by a wide wedge resection are all associated with a worse prognosis.[33] Control of tumor burden by surgical procedure and chemoradiation, pain relief after treatment, and weight loss of less than 5% are suggestive of a better prognosis.[9]
Complications
Complications may occur from the disease itself or from the treatment. Neurological complications involving the upper extremity include:
- Extension of the tumor to C8 and T1 nerve roots results in weakness and atrophy of the intrinsic muscles of the hand or pain and paresthesia of the fourth and fifth digits and the medial aspect of the arm and forearm.[12]
- Extension to the T2 nerve root causes abnormal sensation and pain in the axilla and medial aspect of the upper arm, and the triceps reflex may be lost.
- In approximately 5% of patients, tumors may invade intervertebral foramina early in the course of the disease, causing spinal cord compression and paraplegia. Approximately 25% of patients ultimately develop spinal cord compression.
- In roughly 5% to 10% of patients, tumors may produce a phrenic or recurrent laryngeal neuropathy or superior vena cava syndrome.
Treatment complications include:
- Surgical removal of lung tumors may result in chylothorax, ulnar nerve paralysis (seen in resection of the C8 nerve root), Horner syndrome (resection of the stellate ganglion and sympathetic chain), cerebrospinal fluid leak, and meningitis (postsurgical complications). Surgical mortality rates are 4% to 10%.[34] After the surgical procedure, the quality of life is very poor, and patients often have debilitating pain.[35]
Common side effects from radiotherapy include:
- Localized lung fibrosis, fatigue, esophagitis, and skin irritation
- Less commonly, patients develop symptomatic pneumonitis
- Rare complications include skin fibrosis (leathery skin) with shoulder immobility
- Myelitis and brachial neuritis may cause weakness and pain in the hand, arm, or shoulder
Chemotherapy-related complications include diffuse interstitial pneumonitis, nephrotoxicity, and peripheral neuropathy.
Deterrence and Patient Education
Deterrence strategies for Pancoast tumors focus primarily on risk factor modification and early recognition of atypical symptoms. Tobacco cessation remains the most effective preventive strategy, given the strong association with lung malignant neoplasms. Patients should be educated to seek prompt evaluation for persistent shoulder pain, upper extremity weakness, or features suggestive of Horner syndrome, even in the absence of respiratory symptoms, as early presentation is often nonpulmonary. Early reporting and timely imaging can facilitate diagnosis at a potentially resectable stage, improving overall outcomes.
Pearls and Other Issues
Pancoast tumors are apical NSCLCs that often present with shoulder or arm pain long before respiratory symptoms; therefore, persistent unilateral shoulder pain in a patient with a significant smoking history warrants chest imaging to avoid diagnostic delay. Early MRI of the thoracic inlet and PET-CT–based staging, combined with interdisciplinary planning, are essential to define resectability and deliver curative trimodality therapy (induction chemoradiation followed by en bloc resection).
Enhancing Healthcare Team Outcomes
Initially, patients may receive an incorrect diagnosis of bursitis and osteoarthritis (due to presenting concerns of neck and shoulder pain), which may lead to symptom persistence and a delay in diagnosis of up to 5 to 10 months in some cases.[36] High suspicion is necessary to diagnose these patients early, improving prognosis.[37] Adequate pain control measures are important when treating patients with superior sulcus tumors, as pain is the most debilitating symptom patients report. The overall prognosis of the disease is quite poor; therefore, the interprofessional team should focus on prevention measures and educating the population at risk (primarily patients who smoke).
An interprofessional approach to this disease is best, involving clinicians in multiple specialties, nursing, and pharmacy, as well as other ancillary personnel (respiratory and other therapists). Primary prevention education should begin with pharmacists, nurses, and primary care clinicians. Patients who smoke should be encouraged to quit tobacco use and have regular, guideline-determined, age-appropriate screening (annual low-dose CT scan in individuals 50 to 80 years of age with a 20 pack-year smoking history, as per the United States Preventive Services Task Force (USPSTF), National Comprehensive Cancer Network (NCCN) 2026 guidelines, and American Society of Clinical Oncology (ASCO) 2025 recommendations). Early diagnosis and treatment are associated with a better prognosis.
Media
(Click Image to Enlarge)
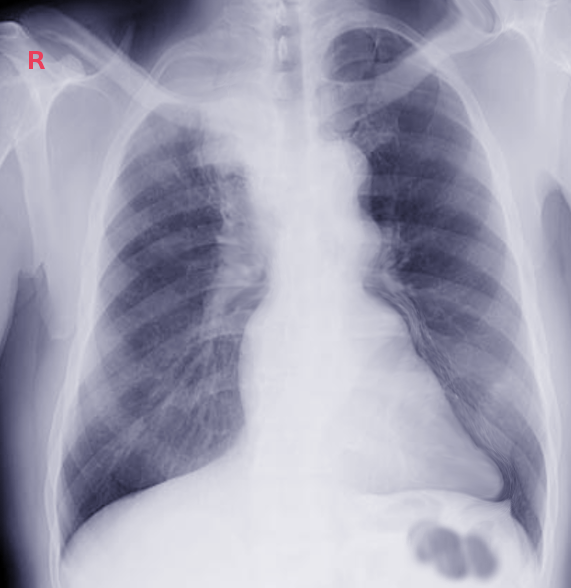
Pancoast Tumor. This frontal chest radiograph demonstrates a dense soft-tissue opacification in the right lung apex, which is characteristic of a superior sulcus (Pancoast) tumor.
Contributed by S Bhimji, MD
References
Arcasoy SM, Jett JR. Superior pulmonary sulcus tumors and Pancoast's syndrome. The New England journal of medicine. 1997 Nov 6:337(19):1370-6 [PubMed PMID: 9358132]
Laouar L, Dammene Debbih N, Laouar N. When Patient and Clinician Miss the Signal: A Delayed Diagnosis of Pancoast Tumor. Cureus. 2025 Sep:17(9):e91732. doi: 10.7759/cureus.91732. Epub 2025 Sep 6 [PubMed PMID: 41058808]
Munir M, Jamil SB, Rehmani S, Borz-Baba C. Pancoast-Tobias Syndrome: A Unique Presentation of Lung Cancer. Cureus. 2021 Feb 3:13(2):e13112. doi: 10.7759/cureus.13112. Epub 2021 Feb 3 [PubMed PMID: 33728131]
Panagopoulos N, Leivaditis V, Koletsis E, Prokakis C, Alexopoulos P, Baltayiannis N, Hatzimichalis A, Tsakiridis K, Zarogoulidis P, Zarogoulidis K, Katsikogiannis N, Kougioumtzi I, Machairiotis N, Tsiouda T, Kesisis G, Siminelakis S, Madesis A, Dougenis D. Pancoast tumors: characteristics and preoperative assessment. Journal of thoracic disease. 2014 Mar:6 Suppl 1(Suppl 1):S108-15. doi: 10.3978/j.issn.2072-1439.2013.12.29. Epub [PubMed PMID: 24672686]
Vandenplas O, Mercenier C, Trigaux JP, Delaunois L. Pancoast's syndrome due to Pseudomonas aeruginosa infection of the lung apex. Thorax. 1991 Sep:46(9):683-4 [PubMed PMID: 1948800]
Level 3 (low-level) evidenceDetterbeck FC. Pancoast (superior sulcus) tumors. The Annals of thoracic surgery. 1997 Jun:63(6):1810-8 [PubMed PMID: 9205202]
Zhang Y, Vaccarella S, Morgan E, Li M, Etxeberria J, Chokunonga E, Manraj SS, Kamate B, Omonisi A, Bray F. Global variations in lung cancer incidence by histological subtype in 2020: a population-based study. The Lancet. Oncology. 2023 Nov:24(11):1206-1218. doi: 10.1016/S1470-2045(23)00444-8. Epub 2023 Oct 11 [PubMed PMID: 37837979]
Paulson DL, Weed TE, Rian RL. Cervical approach for percutaneous needle biopsy of Pancoast tumors. The Annals of thoracic surgery. 1985 Jun:39(6):586-7 [PubMed PMID: 4004404]
Komaki R, Mountain CF, Holbert JM, Garden AS, Shallenberger R, Cox JD, Maor MH, Guinee VF, Samuels B. Superior sulcus tumors: treatment selection and results for 85 patients without metastasis (Mo) at presentation. International journal of radiation oncology, biology, physics. 1990 Jul:19(1):31-6 [PubMed PMID: 2380092]
Level 2 (mid-level) evidenceGadikota P, Reddy VN, Ganti L. Pancoast tumor masquerading as musculoskeletal pain. Orthopedic reviews. 2025:17():143289. doi: 10.52965/001c.143289. Epub 2025 Aug 20 [PubMed PMID: 40860246]
Maloney WF, Younge BR, Moyer NJ. Evaluation of the causes and accuracy of pharmacologic localization in Horner's syndrome. American journal of ophthalmology. 1980 Sep:90(3):394-402 [PubMed PMID: 7425056]
Marangoni C, Lacerenza M, Formaglio F, Smirne S, Marchettini P. Sensory disorder of the chest as presenting symptom of lung cancer. Journal of neurology, neurosurgery, and psychiatry. 1993 Sep:56(9):1033-4 [PubMed PMID: 8410029]
Level 3 (low-level) evidenceGinsberg RJ, Martini N, Zaman M, Armstrong JG, Bains MS, Burt ME, McCormack PM, Rusch VW, Harrison LB. Influence of surgical resection and brachytherapy in the management of superior sulcus tumor. The Annals of thoracic surgery. 1994 Jun:57(6):1440-5 [PubMed PMID: 8010786]
Level 2 (mid-level) evidenceBruzzi JF, Komaki R, Walsh GL, Truong MT, Gladish GW, Munden RF, Erasmus JJ. Imaging of non-small cell lung cancer of the superior sulcus: part 1: anatomy, clinical manifestations, and management. Radiographics : a review publication of the Radiological Society of North America, Inc. 2008 Mar-Apr:28(2):551-60; quiz 620. doi: 10.1148/rg.282075709. Epub [PubMed PMID: 18349457]
Jelercic S, Rajer M. The role of PET-CT in radiotherapy planning of solid tumours. Radiology and oncology. 2015 Mar:49(1):1-9. doi: 10.2478/raon-2013-0071. Epub 2015 Mar 3 [PubMed PMID: 25810695]
Kozower BD, Larner JM, Detterbeck FC, Jones DR. Special treatment issues in non-small cell lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013 May:143(5 Suppl):e369S-e399S. doi: 10.1378/chest.12-2362. Epub [PubMed PMID: 23649447]
Level 1 (high-level) evidenceAlbain KS, Rusch VW, Crowley JJ, Rice TW, Turrisi AT 3rd, Weick JK, Lonchyna VA, Presant CA, McKenna RJ, Gandara DR. Concurrent cisplatin/etoposide plus chest radiotherapy followed by surgery for stages IIIA (N2) and IIIB non-small-cell lung cancer: mature results of Southwest Oncology Group phase II study 8805. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 1995 Aug:13(8):1880-92 [PubMed PMID: 7636530]
Li J, Dai CH, Shi SB, Bao QL, Yu LC, Wu JR. Induction concurrent chemoradiotherapy compared with induction radiotherapy for superior sulcus non-small cell lung cancer: a retrospective study. Asia-Pacific journal of clinical oncology. 2010 Mar:6(1):57-65. doi: 10.1111/j.1743-7563.2009.01265.x. Epub [PubMed PMID: 20398039]
Level 2 (mid-level) evidenceVillgran VD, Chakraborty RK, Cherian SV. Pancoast Syndrome. StatPearls. 2026 Jan:(): [PubMed PMID: 29489146]
Mankal S, Jacobs C. Apical Malignant Pleural Mesothelioma Presenting as Horner's Syndrome: A Case Report. Cureus. 2025 Oct:17(10):e94484. doi: 10.7759/cureus.94484. Epub 2025 Oct 13 [PubMed PMID: 41098930]
Level 3 (low-level) evidenceChang CF, Su WJ, Chou TY, Perng RP. Hepatocellular carcinoma with Pancoast's syndrome as an initial symptom: a case report. Japanese journal of clinical oncology. 2001 Mar:31(3):119-21 [PubMed PMID: 11336324]
Level 3 (low-level) evidenceMoser RP Jr, Davis MJ, Gilkey FW, Kransdorf MJ, Rosado de Christenson ML, Kumar R, Bloem JL, Stull MA. Primary Ewing sarcoma of rib. Radiographics : a review publication of the Radiological Society of North America, Inc. 1990 Sep:10(5):899-914 [PubMed PMID: 2217978]
Chong KM, Hennox SC, Sheppard MN. Primary hemangiopericytoma presenting as a Pancoast tumor. The Annals of thoracic surgery. 1993 Feb:55(2):9 [PubMed PMID: 8431033]
Level 3 (low-level) evidenceMills PR, Han LY, Dick R, Clarke SW. Pancoast syndrome caused by a high grade B cell lymphoma. Thorax. 1994 Jan:49(1):92-3 [PubMed PMID: 8153951]
Level 3 (low-level) evidenceChen KT, Padmanabhan A. Pancoast syndrome caused by extramedullary plasmacytoma. Journal of surgical oncology. 1983 Oct:24(2):117-8 [PubMed PMID: 6632892]
Level 3 (low-level) evidenceCannone G, Faccioli E, Busetto A, Lione L, Maggioni G, Nicotra S, Schiavon M, Rebusso A, Comacchio G, Mammana M, Sepulcri M, Pasello G, Calabrese F, Dell'Amore A, Rea F. Surgery for Pancoast Tumors in Multimodality Setting: Analysis of Outcomes and Risk Factors. Journal of clinical medicine. 2025 Apr 17:14(8):. doi: 10.3390/jcm14082758. Epub 2025 Apr 17 [PubMed PMID: 40283588]
Aokage K, Tsuboi M, Zenke Y, Horinouchi H, Nakamura N, Ishikura S, Nishikawa H, Kumagai S, Koyama S, Kanato K, Kataoka T, Wakabayashi M, Fukutani M, Fukuda H, Ohe Y, Watanabe SI, Lung Cancer Surgical Study Group of the Japan Clinical Oncology Group. Study protocol for JCOG1807C (DEEP OCEAN): a interventional prospective trial to evaluate the efficacy and safety of durvalumab before and after operation or durvalumab as maintenance therapy after chemoradiotherapy against superior sulcus non-small cell lung cancer. Japanese journal of clinical oncology. 2022 Apr 6:52(4):383-387. doi: 10.1093/jjco/hyab208. Epub [PubMed PMID: 34999817]
Remon J, Porez F, Clermidy H, Mercier O, Mitilian D, Guezour N, Caramella C, Pradère P, Saing S, de Montpreville VT, Botticella A, Fadel E. Induction immunotherapy plus chemotherapy for Pancoast lung cancer tumors: are we ready to shift our standards? ESMO open. 2025 Sep:10(9):105562. doi: 10.1016/j.esmoop.2025.105562. Epub 2025 Sep 4 [PubMed PMID: 40912046]
Zhang M, Hagan CT 4th, Foley H, Tian X, Yang F, Au KM, Mi Y, Medik Y, Roche K, Wagner K, Rodgers Z, Min Y, Wang AZ. Co-delivery of etoposide and cisplatin in dual-drug loaded nanoparticles synergistically improves chemoradiotherapy in non-small cell lung cancer models. Acta biomaterialia. 2021 Apr 1:124():327-335. doi: 10.1016/j.actbio.2021.02.001. Epub 2021 Feb 5 [PubMed PMID: 33556606]
Nam JH, Yeo CD, Park CK, Kim SK, Kim JS, Kim YH, Kim JW, Kim SJ, Lee SH, Kang HS. Identification of predictive factors for early relapse in patients with unresectable stage III non-small cell lung cancer receiving consolidation durvalumab after concurrent chemoradiation therapy. Thoracic cancer. 2023 Sep:14(26):2657-2664. doi: 10.1111/1759-7714.15050. Epub 2023 Jul 30 [PubMed PMID: 37519059]
Boby JM, Mohd Ghazali NN, Mani A, George M. Complete response to nivolumab in Kirsten rat sarcoma virus oncogene KRAS-G12C mutant metastatic lung adenocarcinoma: a case report. Journal of medical case reports. 2022 Nov 3:16(1):420. doi: 10.1186/s13256-022-03593-3. Epub 2022 Nov 3 [PubMed PMID: 36329437]
Level 3 (low-level) evidenceForoulis CN, Zarogoulidis P, Darwiche K, Katsikogiannis N, Machairiotis N, Karapantzos I, Tsakiridis K, Huang H, Zarogoulidis K. Superior sulcus (Pancoast) tumors: current evidence on diagnosis and radical treatment. Journal of thoracic disease. 2013 Sep:5 Suppl 4(Suppl 4):S342-58. doi: 10.3978/j.issn.2072-1439.2013.04.08. Epub [PubMed PMID: 24102007]
Attar S, Krasna MJ, Sonett JR, Hankins JR, Slawson RG, Suter CM, McLaughlin JS. Superior sulcus (Pancoast) tumor: experience with 105 patients. The Annals of thoracic surgery. 1998 Jul:66(1):193-8 [PubMed PMID: 9692463]
Level 2 (mid-level) evidenceRusch VW. Management of Pancoast tumours. The Lancet. Oncology. 2006 Dec:7(12):997-1005 [PubMed PMID: 17138221]
Glassman LR, Hyman K. Pancoast tumor: a modern perspective on an old problem. Current opinion in pulmonary medicine. 2013 Jul:19(4):340-3. doi: 10.1097/MCP.0b013e3283621b31. Epub [PubMed PMID: 23702478]
Level 3 (low-level) evidenceMiller JI, Mansour KA, Hatcher CR Jr. Carcinoma of the superior pulmonary sulcus. The Annals of thoracic surgery. 1979 Jul:28(1):44-7 [PubMed PMID: 287414]
Anderson TM, Moy PM, Holmes EC. Factors affecting survival in superior sulcus tumors. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 1986 Nov:4(11):1598-603 [PubMed PMID: 3772415]