Introduction
Any intrinsic or extrinsic compression that is present along the optic nerve can produce compressive optic neuropathy (CON). Other than damage by compression, optic nerve damage can occur as a result of demyelination, ischemia, metabolic, and traumatic insults.[1] The most common sign of injury to the nerve is a slow, progressive monocular visual loss often associated with headaches. Bilateral visual loss can result from midline lesions, eg, a pituitary adenoma, craniopharyngioma, meningioma, and giant cerebral aneurysms, or bilateral orbital lesions associated with thyroid disease and sarcoidosis. Correctly identifying the cause of the CON is essential as the underlying etiology guides management, and the wide-ranging differential diagnoses, which have overlapping clinical features, must be excluded.
Anatomical Structures of the Optic Nerve
The optic nerve contains over 1 million nerve fibers.[2][3] This quantity of fibers demonstrates the complexity and importance that the visual system has had during our evolution. The visual pathway begins in the retina and ends in the visual cortex of the occipital lobe. The retina consists of 2 functional parts: the optic portion and the nonvisual retina. The optic portion of the retina consists of the neural and pigmented layers. In contrast, the nonvisual retina is an extension of the pigmented layer and ends in the ciliary and iridial parts of the retina.[4]
The lamina cribrosa of the sclera forms the optic nerve head and exits the orbit through the optic canal. As it leaves the orbit, the optic nerve head is encased by an extension of the cranial dura and the subarachnoid layer, which forms the optic nerve sheath. The axons of the ganglion cells project as the optic nerve and decussate in the optic chiasm before continuing as the optic tract, which courses to the lateral geniculate ganglion and then projects to the primary visual cortex as the optic radiations. The optic nerve averages 50 mm in length and includes a 1 mm intraocular segment, 25 mm intraorbital segment, 9 mm intracanalicular segment, and 16 mm intracranial segment.[5]
The optic nerve is a unique white matter tract of the central nervous system (CNS), comprised of over 1 million axons of retinal ganglion cells. Its anatomical course is divided into 4 segments: intraocular, intraorbital, intracanalicular, and intracranial. This trajectory renders the optic nerve susceptible to compressive injuries at multiple levels. In the orbit, lesions (eg, cavernous hemangiomas, optic nerve sheath meningiomas, and gliomas) can exert localized compression. Within the optic canal, the rigid bony confines predispose the nerve to significant functional impairment from even minimal expansion due to trauma, mucocele, or meningioma. Intracranially, lesions at the suprasellar region—including pituitary adenomas, craniopharyngiomas, and tuberculum sellae meningiomas—often compress the optic chiasm or proximal optic nerves, leading to characteristic patterns of visual field loss.[6]
Clinical Course of Compressive Optic Neuropathy
The natural history of CON varies according to etiology, rate of growth, and the degree of compression. Slow-growing tumors (eg, meningiomas) may initially present with subtle visual deficits, progressive optic atrophy, or slowly enlarging scotomas. In contrast, rapidly expanding lesions, eg, aneurysms or aggressive malignancies, may cause acute or subacute vision loss. In thyroid eye disease, optic neuropathy typically arises in the setting of orbital apex crowding by hypertrophied extraocular muscles, representing a compressive-inflammatory pathophysiology. Left untreated, CON can lead to irreversible optic nerve damage due to chronic ischemia, demyelination, and axonal degeneration.[7]
Patterns of spread in CON are closely linked to the anatomical relationships of the optic nerve and visual pathways. Lesions at the orbital apex and optic canal typically produce unilateral vision loss, afferent pupillary defects, and optic disc pallor. Suprasellar masses may affect the optic chiasm, resulting in bitemporal hemianopia due to compression of the crossing nasal fibers. More posteriorly, involvement of the optic tracts can cause incongruous homonymous hemianopic defects. These characteristic field patterns aid localization and underscore the importance of meticulous perimetry in evaluation. Notably, progressive compression often demonstrates a sequence beginning with paracentral scotomas, enlargement of the blind spot, and eventual arcuate or altitudinal defects as axonal loss becomes widespread.[4]
From a clinical perspective, CON must be distinguished from other optic neuropathies. While optic neuritis often presents with acute, painful monocular vision loss in young adults, CON typically manifests with insidious, painless, progressive decline in vision. Color desaturation, relative afferent pupillary defect, and optic disc changes are shared features, but the hallmark of CON lies in its association with a compressive lesion, often accompanied by proptosis, motility restriction, or neurological deficits. Neuroimaging, particularly magnetic resonance imaging (MRI) with fat suppression, remains indispensable in delineating the lesion, assessing its relationship to the optic nerve, and planning intervention.[8]
The epidemiology of CON reflects the diversity of underlying etiologies. Orbital tumors are a leading cause in developed nations, whereas infectious and inflammatory lesions, such as tuberculosis, fungal granulomas, and mucormycosis, predominate in resource-limited settings. Thyroid-associated orbitopathy is now recognized as the most common cause of adult orbital disease globally and a significant contributor to compressive neuropathy, especially in populations with high rates of autoimmune thyroid disorders. Pituitary adenomas are the most frequent suprasellar lesions associated with compressive visual loss, with a prevalence estimated at 1 in 1000 individuals. Their indolent growth and predilection for the sellar-suprasellar region underscore the importance of periodic visual assessment in affected patients.[9]
The pathophysiology of visual impairment in CON is multifactorial. Primary mechanical compression causes direct disruption of axonal conduction, while secondary ischemia from compromised pial vasculature exacerbates injury. Chronic compression impairs orthograde and retrograde axoplasmic transport, leading to axonal swelling, demyelination, and eventual atrophy. The degree of reversibility depends on the chronicity of compression: acute lesions with preserved axons may recover after decompression, whereas longstanding cases with optic atrophy generally have poor visual prognosis. This dichotomy highlights the critical importance of early diagnosis.[10]
Patterns of spread are particularly important in localizing lesions and predicting outcomes. In the orbital segment, tumors or inflammatory masses tend to displace rather than infiltrate the nerve, producing eccentric compression. Within the optic canal, even small lesions exert disproportionate pressure due to the confined bony space. At the chiasm, midline lesions (eg, pituitary macroadenomas) compress crossing fibers, while lateral lesions (eg, aneurysms or meningiomas) selectively impact ipsilateral fibers. Posteriorly, optic tract lesions may produce homonymous hemianopias with relative sparing of acuity. These predictable patterns form the cornerstone of clinical neuro-ophthalmology.[11]
The natural history of untreated CON is generally unfavorable, progressing from subtle deficits to severe, irreversible blindness. However, modern interventions have dramatically altered outcomes. Surgical resection or decompression, radiotherapy, medical management of thyroid eye disease, and targeted therapies for specific tumors have all improved visual prognosis. Nevertheless, treatment outcomes are heavily contingent on early detection. Once optic atrophy is established, visual recovery is minimal. Therefore, a thorough understanding of the disease’s progression and anatomical nuances allows clinicians to identify cases earlier and intervene before irreversible damage ensues.[8]
Therefore, CON is a complex condition that exemplifies the interplay between anatomy, pathophysiology, and clinical presentation. Its natural history, though potentially devastating, offers windows of reversibility when promptly identified and treated. The patterns of spread, dictated by the location and type of compressive lesion, serve as diagnostic beacons in clinical evaluation. As advances in imaging, neurosurgery, orbital surgery, and radiotherapy continue, the outlook for patients with CON is improving. However, success ultimately depends on clinician awareness, timely recognition, and an integrated interprofessional approach. A detailed appreciation of general information, anatomical susceptibility, natural history, and characteristic spread patterns remains indispensable in optimizing care for these patients.[12]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
CON arises when the optic nerve or its surrounding structures are subjected to sustained mechanical pressure. This compression can be due to intrinsic lesions of the optic nerve itself or extrinsic processes from adjacent orbital, intracranial, or vascular pathology. Chronic compression disrupts axonal transport, compromises vascular perfusion, and triggers secondary inflammatory cascades, ultimately leading to axonal degeneration, demyelination, and progressive visual loss.
Etiologies can be broadly divided into infectious, inflammatory, vascular, traumatic, neoplastic, osseous, and miscellaneous causes, each with distinct clinical and radiological profiles (see Tables 1 and 2). Recognition of the underlying etiology is crucial, as prognosis and therapeutic options vary significantly.
Infectious Causes
The following infectious causes of granulomatous or mass-like lesions may compress the optic nerve:
- Fungal infections: Aspergilloma is the most frequently implicated, especially in immunocompromised hosts. Chronic invasive fungal sinusitis can extend into the orbital apex, leading to optic nerve compression.[3][13]
- Tuberculosis: Orbital or intracranial tuberculomas may rarely exert pressure on the nerve.[14]
Clinicians should bear in mind that infectious CON often progresses rapidly and requires urgent antimicrobial and sometimes surgical decompression.
Inflammatory Causes
Several inflammatory diseases present with orbital or meningeal masses that cause optic nerve compression, including:
- Idiopathic orbital inflammation (orbital pseudotumor): These etiologies are characterized by diffuse infiltration of orbital tissues, occasionally encasing the optic nerve.[14]
- Thyroid-associated orbitopathy (Graves’ disease): Extraocular muscle hypertrophy (especially inferior and superior recti) can compress the optic nerve at the orbital apex, one of the most common causes of CON worldwide.[15][16][17]
- Sarcoidosis: This condition develops due to granulomatous involvement of the orbit, meninges, or optic nerve sheath.[18]
- IgG4-related disease: Pachymeningitis and orbital pseudotumor are increasingly recognized contributors.[19][20][21][22]
Vascular Causes
The following vascular malformations and aneurysms may cause a compressive effect:
- Intracranial aneurysms, particularly those of the internal carotid, anterior communicating, or ophthalmic arteries [23][24]
- Carotid-cavernous fistulas secondary to venous congestion and enlargement of orbital veins, resulting in secondary CON.[25]
- Venous malformations, varices, and lymphangiomas, producing intermittent compression, often exacerbated by Valsalva maneuvers [26][27]
- Dolichoectasia or ectatic carotid arteries (may exert mass effect at the optic chiasm or canal) [28][29]
Traumatic Causes
Traumatic etiologies that may lead to CON include:
- Orbital fractures with bony displacement impinging on the optic canal [30][31]
- Subperiosteal hematomas or orbital hematomas following trauma resulting in acute, sight-threatening CON [32][33]
- Postsurgical scarring or implants (rare)
Neoplastic Causes
Neoplasms represent the most common category of chronic CON, which usually manifests insidiously, with progressive visual decline and occasionally proptosis. These neoplastic etiologies include:
- Benign tumors: Meningiomas (optic nerve sheath meningiomas), schwannomas, cavernous hemangiomas, and dermoid cysts [34][35][36][37]
- Primary malignant tumors: Optic gliomas (especially in NF-1), lymphomas, sarcomas [38][39][40]
- Secondary tumors: Pituitary adenomas, craniopharyngiomas, and metastases from systemic cancers (breast, lung, prostate)
Osseous (Bone-Related) Causes
Bony disorders can narrow the optic canal, leading to chronic compression, including:
- Fibrous dysplasia: Abnormal bone remodeling can narrow the optic canal [41][42]
- Paget’s disease of bone: Expansile lesions affecting the skull base [43]
- Osteopetrosis: Thickened, sclerotic bones compressing the optic nerve canal [44][45]
- Osteomas and hyperostosis: Localized bony overgrowths [46]
- Langerhans cell histiocytosis: Lesions involving skull base bones [47]
Other Causes
- Mucoceles: Expansion of paranasal sinus mucoceles (commonly ethmoidal or sphenoidal) into the orbital apex [48][49][50][51]
- Granulomatous meningitis: Tuberculosis or fungal infections, encases the optic nerve [52]
- Postradiation fibrosis: Late complication of cranial radiotherapy
Table 1. Etiologies of Compressive Optic Neuropathy
|
Category |
Examples |
Mechanism of Compression |
|
Infectious |
Aspergilloma, Tuberculoma |
Mass effect from granuloma or invasive fungal sinusitis |
|
Inflammatory |
Thyroid orbitopathy, Sarcoidosis, IgG4 pachymeningitis, Orbital pseudotumor |
Muscle hypertrophy, granulomatous or fibrotic encasement |
|
Vascular |
Aneurysm, Carotid-cavernous fistula, Orbital varix, Dolichoectasia |
Mass effect, venous engorgement |
|
Traumatic |
Orbital fracture, Hematoma |
Bony impingement or compressive bleed |
|
Neoplastic |
Meningioma, Glioma, Lymphoma, Pituitary adenoma, Metastases |
Direct invasion or extrinsic compression |
|
Bone Lesions |
Fibrous dysplasia, Paget’s disease, Osteopetrosis, Osteoma, LCH |
Canal narrowing, expansile bone lesions |
|
Others |
Mucoceles, Granulomatous meningitis, Post-radiation fibrosis |
Expansile lesions, fibrotic encasement |
Table 2. Distinctive Clinical and Imaging Features by Etiology
|
Etiology |
Clinical Features |
Imaging Features (CT/MRI) |
|
Thyroid Orbitopathy |
Proptosis, restrictive myopathy, compressive optic neuropathy |
Fusiform muscle enlargement, tendon-sparing |
|
Meningioma |
Optic disc pallor, progressive visual loss |
"Tram-track" sign on contrast MRI |
|
Glioma |
Slow, painless vision loss in children (NF-1 associated) |
Fusiform enlargement of the optic nerve |
|
Aneurysm |
Sudden vision loss, cranial nerve palsies |
Flow voids or vascular dilation on MRI/MRA |
|
Mucocele |
Proptosis, sinus-related symptoms |
Expansile sinus lesion with bone thinning |
|
Fibrous Dysplasia |
Childhood onset, craniofacial deformities |
"Ground glass" appearance on CT |
|
Aspergilloma |
Rapid visual loss, sinus involvement |
Hyperdense sinus lesion with orbital extension |
Additionally, the leading causes of CON can vary by region. In Western countries, neoplasms and thyroid-associated orbitopathy represent the most frequent etiologies, while in Asia and Africa, infectious processes such as aspergilloma and tuberculosis occur more commonly. Neoplastic and osseous causes typically produce a slowly progressive course, while trauma, hematomas, and infections more often result in acute or subacute presentations. Patterns of spread can also vary by etiology. Paranasal sinus disease frequently extends into the orbital apex, whereas pituitary and parasellar masses exert pressure on the optic chiasm before involving the optic canal.
These distinctions are clinically relevant. Early identification of CON remains essential, as sustained compression leads to irreversible optic atrophy. Furthermore, timely intervention with medical therapy or surgical decompression offers the potential to preserve or restore vision when initiated before permanent damage occurs.
Epidemiology
Overall estimates from reported cases of CON are 1.14 to 4 cases per 100,000 individuals per year. Gender, race, ethnicity, and age vary depending on the specific etiology.[53] Due to the numerous etiologies that can cause CON, the estimates of its incidence vary depending on the etiology.
Thyroid orbitopathy associated with Graves’ disease occurs with an incidence of 16 cases per 100,000 in females and 2.9 cases per 100,000 in males.[54][55] Craniopharyngioma demonstrates an incidence ranging from 0.5 to 2 cases per 100,000 persons annually.[56] Fibrous dysplasia affects approximately 1 in 5,000 to 10,000 individuals.[57]
Orbital hemangiomas account for 8% to 10% of benign tumors in the pediatric population, showing a marked female predominance with a ratio of 5 to 1.[58][59] Pituitary adenomas appear with a frequency of 10.5%, yet these tumors produce visual symptoms only when they enlarge sufficiently to compress the optic nerve or the optic chiasm.[60] Optic gliomas, primarily affecting children, represent 3% to 5% of pediatric tumors.[61] A cerebral aneurysm involving the internal carotid artery near the optic nerve carries a prevalence of 3%.[62][63]
CON is not a single disease but a final common pathway caused by a wide spectrum of orbital, intracranial, vascular, infectious, inflammatory, and osseous disorders. As such, the epidemiology of CON reflects the underlying etiologies rather than a unified disease entity. Nonetheless, population-level studies and disease registries provide important insights into its frequency, demographic distribution, and global variation.[53]
Global Burden
The precise global incidence and prevalence of CON remain undefined due to the diverse etiologies and variable diagnostic practices. Available data suggest that CON accounts for 5% to 15% of all optic neuropathies. In developed regions, neoplasms, eg, meningiomas, pituitary adenomas, and craniopharyngiomas, along with thyroid-associated orbitopathy, represent the leading causes. In low-income and middle-income countries (LMICs), particularly in South Asia and Africa, infectious processes such as invasive fungal sinusitis caused by Aspergillus or Mucor, and granulomatous diseases, including tuberculosis and sarcoidosis, occur more frequently.[64]
Age Distribution
In children, optic pathway gliomas—often linked with neurofibromatosis type 1—constitute the most common cause of CON, while craniopharyngiomas represent another important etiology, especially in late childhood and adolescence. Among young to middle-aged adults, thyroid-associated orbitopathy peaks in the third to fifth decade with a strong female predominance, and pituitary adenomas occur most often between ages 30 and 50. In older adults, meningiomas, particularly optic nerve sheath meningiomas, and metastatic disease appear more commonly after age 50 (see Table 4). Bony disorders, eg, Paget’s disease or osteopetrosis, usually present in middle-to-late adulthood.[65]
Sex Distribution
Thyroid-associated orbitopathy demonstrates a female-to-male ratio of approximately 5 to 6:1, and optic nerve sheath meningioma shows a ratio of 3 to 4:1. Pituitary adenomas display a slight male predominance in macroadenomas, while microadenomas occur more frequently in women. Trauma-related CON disproportionately affects males, consistent with global injury patterns. Gliomas, sarcoidosis, and infectious causes, eg, invasive aspergillosis, exhibit no significant sex bias (see Table 4).[66]
Epidemiology in Various Regions
Thyroid eye disease affects approximately 16 per 100,000 women and 3 per 100,000 men annually, with complications occurring in about 3% to 8% of cases. Pituitary adenomas account for 10% to 15% of intracranial tumors, and nearly 50% present with visual pathway compression. Meningiomas represent the most common primary intracranial tumor, with an incidence of 8 to 9 per 100,000 annually; optic nerve sheath meningiomas comprise about 2% of orbital tumors. Trauma-related CON, though uncommon, arises in 0.5% to 5% of closed head injuries, particularly when hematomas or fractures cause compression.[67]
In India and Southeast Asia, thyroid eye disease remains prevalent but often receives delayed treatment, resulting in higher rates of CON. Invasive fungal sinusitis, particularly aspergillosis and mucormycosis, disproportionately affects diabetic and immunocompromised patients. During the COVID-19 pandemic, thousands of mucormycosis-related CON cases were reported. In Africa, infectious etiologies, eg, tuberculosis and fungal sinusitis, contribute significantly due to higher endemic rates and limited access to specialty care. In Japan and East Asia, thyroid orbitopathy occurs less frequently than in Western populations, while orbital inflammatory disease and IgG4-related disease are more common (see Table 3).[68]
Patterns of Spread
Paranasal sinus disease, including mucoceles and invasive fungal infections, often extends into the orbital apex and compresses the optic nerve. Sellar and suprasellar tumors, eg, pituitary adenomas and craniopharyngiomas, primarily compress the optic chiasm and retrochiasmal pathways. Lesions of the orbital apex, including inflammation, lymphoma, and sarcoidosis, cause direct optic nerve compression. Bony canal lesions (eg, fibrous dysplasia and osteopetrosis) progressively narrow the optic canal.[69]
Natural History and Prognostic Relevance
Slowly progressive etiologies, including meningioma, thyroid eye disease, and fibrous dysplasia, provide a window for recognition and timely intervention. Rapidly progressive causes, including invasive fungal sinusitis, hemorrhage, and metastases, carry a high risk of irreversible blindness unless addressed with urgent treatment.
Table 3. Major Compressive Optic Neuropathy Etiologies in Different Regions
|
Etiology |
United States and Europe |
India and Eastern Asia |
Africa |
|
Thyroid Orbitopathy |
Most commonly, 3%–8% develop CON |
Common, higher untreated cases |
Common but underdiagnosed |
|
Pituitary Adenoma |
10%–15% of intracranial tumors |
Frequent, often late diagnosis |
Increasing with better neuroimaging |
|
Meningioma |
2% of orbital tumors |
Common, especially optic nerve sheath |
Rare, but seen with late presentation |
|
Infectious (fungal/TB) |
Rare |
Common (aspergillosis, mucormycosis, TB) |
Very common (TB, fungal) |
|
Trauma |
0.5%–5% of head trauma cases |
Moderate, higher in young males |
High due to road traffic injuries |
|
Bone Disorders |
Uncommon |
Rare |
Rare |
Table 4. Demographic Patterns of Compressive Optic Neuropathy Etiologies
|
Etiology |
Age Group |
Sex Predominance |
|
Optic Nerve Glioma |
Childhood |
Equal |
|
Craniopharyngioma |
Childhood and adolescence |
Slight male |
|
Thyroid Orbitopathy |
30–50 years |
Female (5–6:1) |
|
Pituitary Adenoma |
30–50 years |
Slight male |
|
Meningioma |
>50 years |
Female (3–4:1) |
|
Trauma |
Young adults |
Male |
|
Aspergilloma/Mucormycosis |
Any age, increased in diabetics |
Equal |
|
Fibrous Dysplasia, Paget’s Disease |
Adolescents and adults |
Equal |
Pathophysiology
The optic nerve is part of the CNS. The mammalian CNS lacks the ability for regeneration and axonal growth. When the optic nerve is exposed to axonal damage, glial scar tissue forms, limiting the diffusion of growth factors.[1] Inhibitory proteins of myelin (eg, Nogo and myelin-associated glycoprotein), low expression of growth factors, and lack of laminin are also some factors that hinder the ability for axonal regrowth.[70] The more proximal the damage of the optic nerve is to the eye, the faster apoptosis of the retinal ganglion cells will occur. Apoptosis will lead to a cascade of events involving p53, which will cause further cell death. A CON can occur by compressing the vascular supply and causing ischemia to the nerve, or by directly causing a mass effect on the axons, thereby impairing axonal transport and signal transmission. The areas most susceptible to compression are located where the nerve passes through small bone structures, eg, the orbital apex and the optic canal.
Optic nerve compression, observed in exophthalmos secondary to thyroid disease, results from the enlargement of extraocular muscles due to the proliferation of fibroblasts, increased extracellular matrix, and adipocyte proliferation and differentiation.[15][16] Furthermore, CON develops when mechanical pressure is exerted on the optic nerve or its vascular supply, disrupting its ability to transmit visual information effectively. The optic nerve is uniquely susceptible to compression because it traverses confined anatomical spaces (eg, the orbit, optic canal, and suprasellar cistern), where even small lesions can exert significant mass effect. The pathophysiology involves a combination of mechanical distortion, impaired axoplasmic transport, and vascular compromise.[53]
The first insult is often a disruption of axoplasmic flow within retinal ganglion cell axons. Orthograde (from retina to brain) and retrograde (from brain to retina) transport become impaired, leading to congestion, axonal swelling, and eventual stasis, which manifests clinically as visual field defects, particularly central, cecocentral, or junctional scotomas. If compression persists, the nerve fibers experience progressive degeneration.[71]
In parallel, compression may compromise the delicate vascular supply of the optic nerve. The optic nerve is nourished by branches of the ophthalmic artery, the central retinal artery, and the pial circulation. Sustained pressure reduces perfusion, creating zones of ischemia and hypoxia. This vascular insufficiency accelerates axonal injury, leading to functional deficits that may progress even with relatively mild mechanical pressure.[72]
Over time, the combined mechanical and ischemic insults lead to loss of retinal ganglion cell axons. Clinically, patients progress from early symptoms, eg, dyschromatopsia, relative afferent pupillary defect (RAPD), and subtle visual field loss, to more advanced features, including severe visual decline and optic disc pallor. Notably, the rate of progression varies with the nature of the compressive lesion; slow-growing meningiomas or pituitary adenomas often allow for partial adaptation, whereas rapidly expanding hematomas or aneurysms may cause abrupt and profound visual compromise. The natural history of CON follows a spectrum: initial axoplasmic stasis leads to vascular compromise, resulting in progressive axonal degeneration and ultimately, optic atrophy. Because axonal loss is irreversible, early recognition and timely decompression are essential to prevent permanent blindness.[4]
Histopathology
Histopathological changes in CON reflect the chronic mechanical stress exerted on the optic nerve fibers, their blood supply, and surrounding connective tissue structures. The primary pathological hallmark is axonal loss due to sustained compression, which leads to secondary degeneration of the retinal ganglion cells. This manifests as thinning of the retinal nerve fiber layer, ultimately progressing to optic atrophy if the underlying cause remains untreated.[73]
Microscopically, compressed optic nerves exhibit axonal degeneration and demyelination. Axons within the compressed segment appear attenuated and fragmented, and oligodendrocyte loss is observed, resulting in patchy demyelination. Chronic compression disrupts axoplasmic flow, causing intra-axonal accumulation of organelles and swelling proximal to the lesion. In advanced cases, the nerve parenchyma is replaced by fibrous gliotic tissue, reflecting irreversible scarring.[4]
Vascular compromise is a significant contributing factor. Compression of the pial vessels and central retinal artery branches leads to ischemic damage. Histological sections reveal thickened vessel walls, narrowed lumina, and perivascular gliosis, which supports the role of ischemia in disease progression. In some cases, especially with tumors (eg, meningiomas), a dense fibrous reaction in the optic nerve sheath further aggravates compression. The optic disc morphology also correlates with histopathology. Early stages may exhibit disc pallor with preserved cupping, whereas long-standing cases display sectoral or diffuse atrophy. Retrograde degeneration leads to the loss of retinal ganglion cells in the inner retina, which corresponds to the visual field defects observed clinically.[74]
Special stains and immunohistochemistry highlight glial proliferation (GFAP-positive astrocytes), loss of axonal markers (eg, neurofilament protein), and deposition of extracellular matrix components in chronic cases. Importantly, unlike glaucomatous optic neuropathy, the predominant mechanisms in CON are mechanical distortion and ischemia, rather than elevated intraocular pressure. Overall, the histopathological spectrum of CON ranges from reversible axonal edema in acute compression to irreversible axonal loss with gliosis in chronic cases, underscoring the importance of early diagnosis and decompression.[12]
Toxicokinetics
While CON is primarily structural in origin, toxicokinetic considerations become relevant when systemic or locally administered drugs and toxins interact with compromised optic nerve tissue. Toxicokinetics refers to the process by which substances are absorbed, distributed, metabolized, and excreted, ultimately influencing tissue exposure and toxicity. In CON, the restricted vascular supply and impaired axoplasmic flow caused by compression can alter the pharmacokinetics of neurotoxic or neuroprotective agents within the optic nerve microenvironment.[4]
Drug-Induced Potentiation of Compressive Optic Neuropathy
Certain medications, eg, ethambutol, isoniazid, linezolid, or amiodarone, are known to cause optic neuropathy. In a patient with existing compressive pathology (eg, from thyroid eye disease, meningioma, or aneurysm), reduced blood–nerve barrier integrity and impaired clearance mechanisms increase susceptibility to drug accumulation and toxicity. Toxicokinetics in these cases are altered by localized ischemia and edema, prolonging drug residence time within the optic nerve.[4]
Vascular-Toxic Interactions
Compression of the optic nerve sheath can compromise perineural vessels, altering perfusion and oxygen delivery. This reduced clearance capacity increases the exposure of the nerve to systemic toxins (eg, methanol metabolites, heavy metals), which, under normal circulation, may have been more efficiently metabolized or eliminated. Thus, compressive lesions can exacerbate the neurotoxic potential of systemically circulating agents.[6]
Implications for Neuroprotective Drugs
On the other hand, toxicokinetic barriers also limit penetration of protective drugs, eg, corticosteroids, anti-VEGF agents, or antioxidants. The fibrotic and compressed environment alters local drug distribution, necessitating higher or targeted delivery strategies (eg, periocular injections and sustained-release implants). Understanding toxicokinetics is crucial for balancing therapeutic benefits against the increased risk of neurotoxicity in compressed nerves.[10]
Clinical Relevance in India and Low-Income and Moderate-Income Countries
In regions with higher rates of tuberculosis and infectious orbital disease, ethambutol and linezolid are frequently prescribed. Patients with CON due to granulomatous inflammation or orbital tumors are therefore doubly at risk—both from structural compression and altered toxicokinetics of these drugs. Clinicians must remain vigilant about cumulative drug doses, treatment duration, and the potential synergistic harm when CON coexists with systemic therapy.[12]
History and Physical
Clinical History
Patients with CON usually present with chronic progressive vision loss that can be in 1 or both eyes. These patients can present with headaches, nausea, vomiting, diplopia, dyschromatopsia, exophthalmos, an afferent pupillary defect, photophobia, red eye, or unexplained weight loss. Sudden or rapid visual loss is rare except in cases caused by trauma. These cases are usually due to blunt trauma or a penetrating injury. The nerve can be injured at any location along its path, although the orbital apex and the optic canal are the most susceptible areas to damage.[75]
Obtaining a comprehensive history helps focus the broad differential diagnosis, including:
- Symmetric or asymmetric vision loss
- Slow versus rapid onset of visual loss
- Family history of cancer
- History of radiation therapy
- Cardiovascular risk factors that include hypertension, peripheral vascular disease, and tobacco use
- Metabolic disease
- Autoimmune history [76]
Patients with CON often present with a subacute or slowly progressive decline in visual function, although the onset may be acute in cases of trauma or vascular compression. A careful and detailed history is crucial for differentiating CON from other optic neuropathies, eg, those with inflammatory, ischemic, or toxic etiologies.[77]
Patients typically report a gradually worsening, painless loss of vision in 1 or both eyes. The progression may be asymmetric and is often associated with visual field defects such as central or cecocentral scotomas, altitudinal defects, or peripheral constriction, depending on the site of compression. Color vision loss, especially red desaturation, is an early and sensitive symptom. Diplopia may be reported if the compressive lesion also affects ocular motor nerves or extraocular muscles, as seen in thyroid orbitopathy or orbital tumors.
In cases of orbital or parasellar masses, patients may experience proptosis, periocular swelling, or facial numbness. Headache, particularly retro-orbital or periorbital pain, is more common in tumors, aneurysms, or inflammatory lesions, whereas thyroid-associated orbitopathy may present with a history of systemic hyperthyroidism. Traumatic causes are associated with a clear history of orbital or craniofacial injury. A family or personal history of neurofibromatosis, pituitary disease, or systemic malignancy may provide important diagnostic clues.[76]
Physical Examination
The hallmark finding in CON is optic nerve dysfunction, characterized by reduced visual acuity, impaired contrast sensitivity, and dyschromatopsia. Pupillary assessment may reveal a RAPD in unilateral or asymmetric cases. Clinical ophthalmic evaluation typically includes:
- Slit-lamp examination: This test evaluates the retina, retinal arteries and veins, cornea, fovea, optic cup.
- Tonometry: Intraocular pressure is assessed.
- Proptosis: Clincal assessment for the presence of unilateral or bilateral protrusion of the eyes.[78]
- Visual acuity testing: The Snellen chart is used to assess visual acuity at baseline and follow-up assessments; best corrected vision should be recorded.
- Color vision testing: Ishihara or Farnsworth-Munsell tests (evaluates if a color deficit is present); red desaturation is an early indicator.
- Pupillary examination: RAPD in asymmetric cases.
- Visual fields: Visual field testing differentiates central from peripheral visual loss. Automated perimetry (Humphrey 30-2, 24-2) or Goldmann perimetry detects early scotomas, bitemporal defects, and junctional scotomas.
- Fundus examination: Optic disc edema in acute lesions; temporal pallor or diffuse atrophy in chronic compression.
- Ocular motility assessment: Testing of extraocular eye movements helps identify restrictions or diplopia associated with orbital lesions.[79]
On fundus examination, early cases may show a normal disc (so-called "retrobulbar neuropathy"), while chronic compression often leads to optic disc pallor and atrophy. In some cases, particularly with orbital lesions, optic disc edema may be present initially. Visual field testing reveals defects corresponding to the site of compression, including junctional scotomas in parasellar tumors, bitemporal hemianopia in chiasmal compression from pituitary adenomas, or arcuate/peripheral defects in orbital mass lesions. Proptosis, lid retraction, or restrictive motility defects may be observed in thyroid eye disease and orbital tumors.
Cranial nerve involvement, eg, ophthalmoplegia (III, IV, VI), trigeminal sensory loss (V1 distribution), or Horner’s syndrome, suggests a lesion extending into the cavernous sinus or orbital apex. Palpation of the orbit may occasionally reveal firm masses in superficial lesions, while auscultation can detect bruits in carotid–cavernous fistula. Systemic examination findings, including goiter, café-au-lait spots, or lymphadenopathy, may aid in identifying underlying systemic disease.[80]
Clinical Relevance
A structured history and detailed physical examination not only establish the suspicion of CON but also provide essential localizing information (see Table 6). Identifying associated systemic conditions, the rate of progression, and the presence of red-flag features, eg, rapidly progressive vision loss, severe headache, or neurological deficits, guides urgent imaging and intervention. In India and other low- and middle-income settings, the delayed recognition of subtle early signs often results in advanced disease at presentation, underscoring the importance of meticulous history-taking and comprehensive physical examination in preventing irreversible blindness.[81]
Table 6. Clinical Findings in Compressive Optic Neuropathy
|
Category |
History |
Physical Examination |
Likely Etiologies |
|
Visual Symptoms |
|
|
|
|
Field Defects |
|
|
|
|
Ocular Symptoms |
|
|
|
|
Orbital Features |
|
|
|
|
Systemic/Associated |
|
|
|
Evaluation
The evaluation of CON requires a structured, interprofessional approach combining clinical, laboratory, imaging, and functional tests to confirm the diagnosis, localize the lesion, and guide management (see Image. Compressive Optic Neuropathy Evaluation). The evaluation is guided by international standards while incorporating region-specific protocols.[82]
A comprehensive neurological examination, followed by a thorough ophthalmological evaluation, should be performed. The exam will provide a baseline visual acuity and allow the clinician to monitor for progression or improvement. The eye will have reduced visual acuity with CON. The eye can also exhibit a deficiency in color vision, known as dyschromatopsia, which can be evaluated using the Ishihara test plate. Proptosis or resistance to manual pressure suggests the presence of an intraorbital lesion. Ocular motility abnormalities are evaluated by assessing the function and coordination of the eye muscles. The optic disc can be atrophic, edematous, or appear healthy. Optociliary shunt vessels can be identified due to obstruction in the venous return from the orbit.[11]
Laboratory Studies
Laboratory studies should include complete blood count, comprehensive metabolic panel, lipid panel, thyroid-stimulating hormone (TSH), free thyroxine (T4), triiodothyronine (T3), luteinizing hormone, anti-thyroid antibodies, thyroid-releasing hormone, follicle-stimulating hormone, prolactin, adrenocorticotropic hormone, insulin growth factor-1, cortisol, bone-specific alkaline phosphatase, and prostate-specific antigen. The angiotensin-converting enzyme is usually elevated in more than half of the patients with active sarcoidosis.[83]
Inflammatory and autoimmune testing includes erythrocyte sedimentation rate (ESR), C-reactive protein, angiotensin-converting enzyme, antinuclear antibody, antineutrophil cytoplasmic antibody, and IgG4, which assist in diagnosing sarcoidosis, vasculitis, or IgG4–related disease. Endocrine evaluation incorporates thyroid-stimulating hormone, T4, T3, and thyroid-stimulating hormone receptor antibody for Graves orbitopathy, along with a pituitary hormone panel measuring prolactin, growth hormone, adrenocorticotropic hormone, and cortisol. Infectious assessment may involve fungal serology for aspergillosis, tuberculosis polymerase chain reaction, and syphilis screening when indicated. Cerebrospinal fluid analysis becomes necessary when granulomatous or carcinomatous meningitis is suspected.[84]
Imaging Studies
Imaging studies are the mainstay of CON diagnosis. Brain and orbit magnetic resonance imaging (MRI) scans provide detailed images of the optic nerves, parasellar region, and orbital contents. Therefore, MRI is the preferred modality for diagnostic evaluation. Fat suppression sequences are required to demonstrate enhancing lesions inside the orbit. Thin-slice MRI of the brain and orbits (1–2 mm) with gadolinium enhancement and fat suppression serves as the gold standard for evaluating CON. This modality effectively identifies meningiomas, gliomas, pituitary adenomas, craniopharyngiomas, orbital masses, and aneurysms. Optic nerve sheath meningiomas often display the characteristic “tram-track” or “doughnut” sign.[85]
Lesions involving the orbital bones should be examined using a computed tomographic (CT) scan of the head and orbit. CT demonstrates orbital fractures and concomitant injuries in traumatic cases. CT provides superior assessment of bony abnormalities, including fibrous dysplasia, osteoma, fractures, and osteopetrosis. Clinicians frequently employ CT when MRI is contraindicated or as a complementary tool in orbital trauma and the evaluation of calcified lesions.[86]
Ultrasonography can be used for intraorbital biopsy of anteriorly located lesions.[87] Angiographic studies are indicated when vascular causes are suspected, including aneurysms, carotid-cavernous fistulas, or ectatic internal carotid arteries.
Functional and Electrophysiological Tests
Visual evoked potentials (VEP) demonstrating delayed P100 latency or reduced amplitude suggest optic nerve dysfunction. Electroretinography (ERG) helps distinguish between retinal and optic nerve pathology.[88]
International and National Guidelines
The American Academy of Ophthalmology (AAO) Preferred Practice Patterns in Neuro-ophthalmology (2022) recommend MRI of the brain and orbits as the gold standard, in conjunction with visual field monitoring and endocrine/autoimmune evaluation in select cases. The European Neuro-ophthalmology Society (EUNOS) guidelines emphasize interprofessional collaboration, particularly in pituitary, orbital, and inflammatory disease. The All India Ophthalmological Society (AIOS) neuro-ophthalmology subspecialty group endorses early MRI, systemic evaluation for thyroid- and TB-related causes, and interprofessional tumor board discussions for neoplastic and vascular etiologies.[89]
Differential Diagnosis Exclusion
Noncompressive optic neuropathies—including toxic, nutritional, demyelinating, ischemic, and hereditary forms—must be excluded through targeted history, blood testing, and imaging correlation. Comprehensive evaluation of CON integrates clinical examination, visual function testing, MRI or CT imaging, systemic investigations, and electrophysiology. Guidelines consistently highlight MRI with contrast as the diagnostic standard, supplemented by endocrine and autoimmune testing when clinically appropriate. Early detection through this interprofessional approach remains critical for preventing irreversible optic nerve damage.[90]
Treatment / Management
Compressive Optic Neuropathy Management Approaches
The first step in the management of CON is to treat the underlying causative condition. Corticosteroids are beneficial for inflammation associated with CON, eg, in sarcoidosis and thyroid disease. For these conditions, withdrawal of the steroid treatment can cause acute deterioration of vision. Surgical orbital decompression can help to improve CON caused by thyroid ophthalmoplegia.[91][92][93] For tumors intimately attached to the optic nerve (eg, optic nerve meningiomas), surgery can cause further loss of vision. Radiation therapy is beneficial for aggressive recurrent tumors and those located in areas adjacent to cranial nerves and eloquent brain tissue. Radiotherapy can also be used for surgically difficult-to-resect tumors, such as those located in the cavernous sinus. Radiation can rarely cause irreversible optic nerve damage; therefore, this therapy must be used judiciously.(A1)
In traumatic cases, conservative treatment is appropriate in patients with mild deficits because spontaneous improvement is often possible. Steroids have no benefit for CON caused by trauma. Surgery is used for patients with radiological evidence of CON.[33][94] Direct compression of the optic nerve by bone fragments or a subperiosteal hematoma is usually treated surgically.[94][95] However, surgery carries the risk of complications such as postoperative cerebrospinal fluid leak and meningitis.[96](A1)
The management of CON depends on the underlying etiology, the severity of optic nerve compromise, and the patient's overall systemic condition (see Table 7). The primary goal of therapy is to relieve pressure on the optic nerve, preserve visual function, and address the causative pathology. Early diagnosis and intervention are crucial, as prolonged compression often leads to irreversible optic atrophy. Additionally, optimal management of CON requires coordinated care (Please refer to the Consultations section for more information on interprofessional management).
Medical Management
High-dose intravenous corticosteroids play a central role in treating inflammatory or infiltrative causes, eg, thyroid eye disease, sarcoidosis, and idiopathic orbital inflammation. These agents reduce edema and mass effect around the optic nerve, often improving vision in the acute phase. For IgG4-related disease, granulomatous disorders, or refractory thyroid orbitopathy, clinicians employ steroid-sparing immunosuppressants and biologic therapies, including rituximab, azathioprine, methotrexate, and mycophenolate mofetil. In infectious cases, eg, aspergilloma or mucormycosis, targeted antifungal therapy must be combined with surgical debridement to achieve disease control. Management of Graves’ orbitopathy may also involve systemic corticosteroids, orbital radiotherapy, and newer biologics (eg, teprotumumab), which have demonstrated efficacy in reducing compressive effects at the orbital apex.[97]
Surgical Management
Orbital decompression represents the standard of care in thyroid eye disease complicated by sight-threatening optic neuropathy. Techniques include medial wall, orbital floor, and orbital fat decompression, which can be performed through external or endoscopic approaches. Neoplastic etiologies, including meningioma, glioma, pituitary adenoma, craniopharyngioma, and metastatic tumors, often require surgical resection, with adjuvant radiotherapy in select cases. Functional endoscopic sinus surgery offers effective decompression for patients with mucoceles or paranasal sinus lesions that affect the optic nerve. For vascular lesions (eg, aneurysms), neurosurgical clipping or endovascular interventions—including coiling or stenting—can relieve optic apparatus compression. Traumatic hematomas or fractures occasionally demand urgent surgical repair to prevent irreversible optic nerve injury.[98]
Radiotherapy
Fractionated stereotactic radiotherapy or Gamma Knife radiosurgery may be considered for unresectable or residual tumors such as meningiomas, craniopharyngiomas, and pituitary adenomas. These techniques stabilize or improve vision in selected patients.[99]
Observation and Monitoring
Patients with mild compressive lesions and preserved vision may be managed conservatively under close surveillance. Monitoring strategies include serial visual field testing, optical coherence tomography to assess retinal nerve fiber layer thickness, and contrast-enhanced magnetic resonance imaging to detect progression. Any evidence of deteriorating visual function necessitates prompt escalation to medical or surgical intervention.[100](A1)
National and International Guidelines
The European Group on Graves’ Orbitopathy (EUGOGO) recommends immediate intravenous methylprednisolone in sight-threatening thyroid eye disease, followed by urgent orbital decompression if no improvement occurs within 1 to 2 weeks. The AAO advocates for an interprofessional approach that involves ophthalmology, neurosurgery, otolaryngology, and radiology. Contrast-enhanced MRI remains the preferred modality, and surgical decompression is advised for progressive vision loss unresponsive to medical therapy. The National Comprehensive Cancer Network (NCCN) emphasizes individualized management of neoplastic causes, with tumor boards often recommending multimodal treatment strategies that combine surgery, radiotherapy, and, when indicated, chemotherapy.[100](A1)
Table 7. Etiology-Specific Treatment Approaches
|
Etiology |
First-Line Treatment |
Adjunct/Alternative |
|
Thyroid Eye Disease |
Intravenous steroids → orbital decompression |
Radiotherapy, biologics |
|
Meningioma, Glioma, Pituitary |
Surgical excision with or without radiotherapy |
Observation of slow-growing |
|
Mucocele, Sinus Pathology |
Endoscopic sinus surgery |
Systemic antibiotics if infected |
|
Vascular (aneurysm, fistula) |
Endovascular embolization or clipping |
Anticoagulation (select cases) |
|
Inflammatory (IgG4, sarcoidosis) |
Steroids, immunosuppressants |
Biologics (rituximab) |
|
Infectious (aspergilloma, mucor) |
Antifungals plus surgical debridement |
Long-term antifungal therapy |
|
Traumatic |
Evacuation of hematoma, fracture repair |
Supportive therapy |
Differential Diagnosis
Differential diagnoses (see Table 8) that should be considered when evaluating patients with suspected CON include:
When evaluating for the specific etiology, the following common disorders should be excluded, as their treatment management differs:
- Pituitary tumors
- Schwannoma
- Meningioma
- Aneurysm
- Arteriovenous malformation
- Lymphoma
- Sarcomas
- Metastasis
- Glioma
- Trauma
- Sarcoidosis [103]
Table 8. Differential Diagnosis of Compressive Optic Neuropathy
|
Condition/Disease |
Key Overlapping Features |
Distinguishing Features |
|
Optic Neuritis |
|
|
|
Ischemic Optic Neuropathy (AION/NAION) |
|
|
|
Toxic/Nutritional Optic Neuropathy |
|
|
|
Leber Hereditary Optic Neuropathy (LHON) |
|
|
|
Glaucoma (Chronic Open-Angle) |
|
|
|
Papilledema (Raised ICP) |
|
|
|
Central Retinal Vein Occlusion (CRVO) |
|
|
|
Demyelinating Disease (MS-Related) |
|
|
|
Infiltrative Optic Neuropathy (Leukemia, Lymphoma) |
|
|
|
Uveitis-Associated Optic Neuropathy |
|
|
|
Functional/Nonorganic Vision Loss |
|
|
Pertinent Studies and Ongoing Trials
The evidence base for managing CON has significantly expanded in the past 2 decades, with multiple observational studies, retrospective cohorts, and clinical trials evaluating treatment outcomes across infectious, inflammatory, vascular, and neoplastic causes. Much of the evidence stems from outcomes of surgical decompression, radiotherapy, and, more recently, combined multimodal approaches.
Surgical Decompression Studies
Several large case series and prospective cohorts have documented the role of orbital, optic canal, and intracranial decompression in CON. In thyroid eye disease–related conditions, randomized controlled trials (RCTs), such as the EUGOGO studies, have demonstrated that early decompression significantly improves visual acuity, color vision, and visual fields compared to conservative management. Endoscopic transnasal decompression has also been validated in multiple studies as a minimally invasive approach with reduced morbidity.[53]
Radiotherapy Outcomes
Radiotherapy has been evaluated extensively in compressive optic neuropathies secondary to meningiomas, lymphoma, and pituitary adenomas. Modern conformal radiotherapy and stereotactic radiosurgery (SRS) techniques, including Gamma Knife and CyberKnife, have shown tumor control rates exceeding 90%, with stabilization or improvement of vision in 60% to 80% of cases. Long-term follow-ups from institutions, eg, the Mayo Clinic and Johns Hopkins, confirm the durability of tumor shrinkage with a relatively low risk of radiation-induced optic neuropathy (RION) when fractionation and dose constraints are respected.[104]
Medical Therapy Studies
Glucocorticoids remain central for inflammatory causes such as sarcoidosis or idiopathic orbital inflammation. The CIRTED trial (UK, 2018) established the role of intravenous methylprednisolone as first-line treatment in thyroid-associated orbitopathy, showing superior outcomes over oral steroids. More recently, biologics, eg, teprotumumab (an IGF-1R inhibitor), have revolutionized CON management in thyroid orbitopathy, with phase 2 and 3 trials reporting dramatic improvements in proptosis, diplopia, and optic nerve compression relief.[105]
Ongoing Trials and Future Directions
Several ongoing clinical trials are addressing unresolved questions in CON management, including:
- Teprotumumab extension studies (OPTIC-X trial): assessing long-term efficacy and relapse rates
- Checkpoint inhibitors and immunotherapies: exploring their role in lymphoma- and sarcoma-related orbital CON
- Low-dose radiotherapy protocols: aiming to optimize tumor control while minimizing toxicity in meningiomas
- Advanced neuroimaging biomarkers: investigation of diffusion tensor imaging (DTI) and optical coherence tomography angiography (OCTA) as early predictors of therapeutic response [106]
Meta-Analyses and Guidelines
Recent meta-analyses (2020–2023) synthesizing outcomes from surgical, radiotherapeutic, and biologic interventions highlight the following:
- Surgery remains first-line in rapidly progressive CON.
- Radiotherapy is best suited for benign or malignant tumors with moderate growth rates.
- Medical therapies (particularly biologics) are transforming management in thyroid-associated cases.
International guidelines, including those from the European Society of Endocrinology and North American Neuro-Ophthalmology Society (NANOS), now emphasize individualized, etiology-specific management, supported by robust clinical evidence.[107]
Treatment Planning
Treatment Planning Overview
Treatment planning for CON demands a highly individualized and interprofessional strategy that balances vision preservation, tumor or lesion control, and reduction of treatment-related morbidity. The choice of modality depends on the underlying etiology—whether neoplastic, inflammatory, vascular, or infectious—as well as lesion size, anatomical location, and the rate of disease progression. Treatment planning for CON relies on advanced radiotherapy modalities, eg, IMRT, SRS, and PBT, supported by precise imaging-based delineation and interprofessional coordination. Therefore, careful integration of surgical, medical, and radiotherapeutic strategies maximizes local control and visual preservation while minimizing morbidity.[108]
Simulation and Imaging
High-resolution MRI with orbital and skull base protocols serves as the gold standard for defining the extent of optic nerve compression, perineural spread, and involvement of adjacent structures. CT complements MRI, particularly in cases with bony abnormalities, eg, fibrous dysplasia, Paget’s disease, or osteomas. For radiotherapy planning, MRI-CT fusion is essential for delineating the gross tumor volume (GTV) and clinical target volume (CTV) while sparing critical structures, including the optic chiasm and the contralateral optic nerve.[109]
Radiation Therapy Techniques
Conventional external beam radiotherapy, once delivered with lateral opposed fields, is now used less frequently due to higher toxicity. Three-dimensional conformal radiotherapy (3DCRT) shapes beams to the tumor while sparing adjacent structures and remains an option where advanced technology is unavailable. Intensity-modulated radiotherapy (IMRT) has become the gold standard in many centers, providing steep dose gradients and precise targeting of irregular lesions such as sphenoid wing meningiomas and pituitary adenomas, while reducing the risk of radiation-induced optic neuropathy. SRS techniques, including Gamma Knife, CyberKnife, and LINAC-based systems, achieve local control rates exceeding 90% for small to medium benign tumors (eg, meningiomas and schwannomas), as well as selected metastases. Proton beam therapy (PBT), with its Bragg peak property, is particularly advantageous in pediatric and recurrent cases by minimizing long-term radiation sequelae.[110]
Prescription (Dose and Fractions)
For benign tumors such as meningiomas and schwannomas, fractionated radiotherapy typically delivers 50 to 54 Gy in 25 to 30 fractions, while SRS protocols include 12 to 15 Gy in a single fraction or 21 to 25 Gy in 3 to 5 hypofractionated treatments. Pituitary adenomas are treated with 45 to 50 Gy in 25 to 28 fractions for fractionated radiotherapy or 12 to 20 Gy in a single fraction with SRS, depending on lesion size and proximity to the optic nerve. Malignant tumors require different regimens: lymphoma receives 24 to 36 Gy in 12 to 18 fractions, often combined with chemotherapy. In comparison, metastases may be treated with 30 Gy in 10 fractions or 15 to 21 Gy in a single SRS session. Repeat irradiation protocols mandate strict adherence to cumulative dose limits, with exposure to the optic nerve and chiasm kept below 55 Gy.[111]
Target Volume Delineation
The gross tumor volume corresponds to the visible lesion on MRI. The clinical target volume encompasses areas of potential microscopic spread or perineural invasion, while the planning target volume includes additional margins of 2 to 3 mm to account for setup variability and motion. Organs at risk, including the optic nerves, optic chiasm, brainstem, pituitary gland, and contralateral eye, must be contoured carefully with strict dose constraints to protect vision and neurological function.[112]
Interprofessional Integration
Surgical intervention often precedes or complements radiotherapy in rapidly progressive or vision-threatening cases, eg, urgent decompression in thyroid orbitopathy or orbital apex tumors. Medical therapies, including corticosteroids and biologics (eg, teprotumumab), are integrated into treatment for inflammatory etiologies. Radiotherapy is planned when surgery is contraindicated, incomplete, or associated with a high risk of recurrence.[113]
Follow-Up and Adaptive Planning
Ongoing ophthalmic evaluation, including visual acuity, visual field testing, and optical coherence tomography of the retinal nerve fiber layer, is essential throughout therapy. Radiological reassessment with MRI is typically performed at 3 to 6 months post-treatment to evaluate response. Adaptive planning may become necessary in cases with substantial lesion shrinkage or anatomical change, particularly during IMRT or proton therapy.
Toxicity and Adverse Effect Management
Management of Toxicities in Compressive Optic Neuropathy
The management of CON frequently involves surgery, radiotherapy, chemotherapy, or multimodal approaches, each carrying distinct toxicities. Early recognition of complications and proactive intervention play a central role in optimizing outcomes and preserving visual function. Toxicity management in CON requires anticipation, prevention, and prompt intervention. Advances, eg, IMRT, proton therapy, minimally invasive surgery, and biologic agents have significantly reduced the incidence of treatment-related complications. Nevertheless, vigilant interprofessional follow-up remains essential for preserving function and maintaining quality of life.
Surgical Toxicities
Optic nerve injury may occur during decompression or tumor resection, leading to worsening vision loss. Preventive strategies include intraoperative neuro-monitoring, meticulous microsurgical techniques, and neuronavigation. High-dose corticosteroids can be administered postoperatively to reduce edema. CSF leaks and meningitis, especially after skull base or orbital apex surgeries, require lumbar drainage, watertight dural repair, and prophylactic antibiotics. Injury to cranial nerves III, IV, or VI may result in ocular motility disturbances. Management options include prism therapy, botulinum toxin injection, or strabismus surgery for persistent diplopia.[114]
Radiation-Related Toxicities
Radiation-induced optic neuropathy (RION), a dose-dependent complication typically occurring at cumulative doses above 55 Gy, presents with sudden, irreversible vision loss. Preventive measures include strict adherence to dosage limits (≤54 Gy for optic nerve and chiasm), fractionation strategies, and advanced techniques, eg, IMRT or proton therapy. Once RION develops, therapeutic options remain limited, although hyperbaric oxygen and anti-vascular endothelial growth factor (anti-VEGF) therapy have been attempted. Retinopathy and maculopathy, particularly after stereotactic radiosurgery, may be treated with anti-VEGF injections or laser photocoagulation in ischemic cases. Cataract formation often develops as a delayed effect of orbital irradiation and can be managed with phacoemulsification and intraocular lens implantation. Lacrimal gland irradiation may lead to dry eye syndrome or keratopathy, which can be best managed with lubricants, punctal plugs, or topical cyclosporine.[115]
Medical Therapy Toxicities
Corticosteroids, commonly used in thyroid orbitopathy and inflammatory conditions, may produce Cushingoid features, diabetes, hypertension, osteoporosis, and ocular hypertension. Management strategies include tapering to the lowest effective dose, providing bone protection with calcium, vitamin D, and bisphosphonates, and monitoring intraocular pressure. Biologic agents (eg, rituximab and teprotumumab) may cause infusion reactions, hearing loss in the case of teprotumumab, and immune suppression. Preventive measures include premedication with antihistamines or corticosteroids, audiometric monitoring, and prophylaxis for opportunistic infections. Chemotherapy for lymphoma may result in myelosuppression, neuropathy, or systemic toxicities, managed with growth factor support, dose modifications, and close systemic monitoring.[116]
Systemic and Supportive Toxicities
Endocrine dysfunction may follow radiotherapy for parasellar tumors due to pituitary damage, necessitating hormone replacement therapy with thyroxine, hydrocortisone, sex hormones, or growth hormone. Neurocognitive decline, though rare in fractionated radiotherapy, may occur in pediatric patients or those receiving high-dose regimens. Management strategies include neurorehabilitation, cognitive therapy, and minimizing radiation dose to the hippocampi with advanced treatment planning.[4]
Preventive and Monitoring Strategies
Multimodal imaging, combining MRI and OCT, enables the early detection of optic nerve and retinal changes. Regular visual function testing, including visual fields and contrast sensitivity, supports early identification of deficits. Strict dose constraints combined with modern radiotherapy planning protect the optic nerve, chiasm, and retina from excessive radiation. Patient education remains essential, with counseling focused on early recognition of vision changes, diplopia, and systemic drug toxicities to allow timely intervention.[117]
Staging
While CON is not universally staged in the same structured way as neoplasms or vascular disease, several frameworks have been proposed to stratify disease severity and guide treatment. These staging systems are primarily based on functional visual outcomes, structural optic nerve damage, and neuroimaging findings, rather than a single uniform pathological criterion.
Functional Staging (Vision-Based)
CON staging based on function uses the following ophthalmic evaluation findings to stratify disease severity:
- Stage 0 (preclinical/asymptomatic): Detected incidentally on imaging with no visual field defect, normal visual acuity, and no optic disc changes
- Stage I (early symptomatic): Mild visual field defect (central or paracentral scotomas, early arcuate defect), normal or slightly reduced visual acuity, subtle color vision loss
- Stage II (moderate): Significant visual field constriction, RAPD, and reduced contrast sensitivity. Optic disc pallor may begin to appear
- Stage III (advanced): Severe constriction of fields, marked optic atrophy, and reduced best-corrected visual acuity (<20/200 in severe cases)
- Stage IV (end-stage): No light perception or minimal residual light perception with complete optic atrophy [118]
Radiological Staging (Imaging-Based)
The following radiological staging is based on the site and degree of compression determined by MRI/CT evidence:
- Stage A (proximity): Lesion abutting the optic nerve or chiasm but without deformation
- Stage B (contact and deformation): Clear contact with optic nerve/chiasm with visible deformation
- Stage C (signal changes): Optic nerve demonstrates T2 hyperintensity (suggesting edema, ischemia, or demyelination)
- Stage D (atrophy): Chronic compression with optic nerve thinning and secondary changes in surrounding structures [119]
Disease-Specific Staging
Some conditions causing CON (eg, thyroid eye disease, optic nerve sheath meningioma) have their own staging systems that overlap with CON, including:
- Thyroid eye disease: The NOSPECS classification includes optic nerve dysfunction as a late-stage condition.
- Optic nerve sheath meningioma: Tumor volume and length of encasement on imaging help define progression and therapeutic thresholds.[67]
Proposed Composite Clinical-Radiological Staging
Several authors have suggested the following integrated staging system:
- Stage I (radiological): Lesion abutting optic nerve with no functional loss.
- Stage II (subclinical functional loss): Early color vision changes or subtle field defects, preserved acuity.
- Stage III (established functional loss): Clear field defect, RAPD, disc pallor, and documented compression.
- Stage IV (irreversible damage): Severe atrophy with profound functional loss, little chance of visual recovery even with decompression.[120]
Clinical Relevance of Staging on Management
CON does not follow a universally standardized staging system comparable to those used for neoplasms or vascular diseases. However, several frameworks have been developed to help determine disease severity and identify optimal individualized treatment approaches. Generally, in early stages (0–I), management emphasizes observation and close monitoring, with surgical intervention considered if disease progression occurs. Moderate stages (II–III) often require stronger consideration for optic nerve decompression, radiation therapy, or targeted medical therapy, depending on the underlying etiology. End-stage disease (IV) shifts the focus toward preventing contralateral involvement, implementing visual rehabilitation strategies, and providing comprehensive patient counseling to support quality of life.[121]
Prognosis
The prognosis for CON depends on the underlying pathophysiology (vascular insufficiency or axonal damage) present and the duration from the time of presentation to the time of treatment. The recovery of visual symptoms typically correlates with the length of time between presentation and the time to perform the decompression. The consensus in the literature is that the earlier the decompression, the better the ultimate clinical outcome. Complete visual recovery has been seen as early as 1 week.[23] Slow progressive vision improvements have also been reported. More than half of the patients will improve clinically, irrespective of their preoperative visual status.[122] Early decompression is recommended, but good results can still be obtained even if decompression is performed in a delayed manner.[122]
Moreover, the prognosis for visual recovery varies significantly depending on the etiology causing the optic nerve compression. For tumor-related etiologies, negative predictive factors for visual improvement are the severity of visual loss, the presence of disc atrophy, recurrent tumor resection, tumor extension to the cavernous sinus, firm tumor consistency, absence of an arachnoid plane around the tumor, extensive tumor resection, and the longer the duration of visual loss. Overall, 60% of patients with tumors will experience some improvement after optic nerve decompression.[123]
Factors Influencing Prognosis
The prognosis of CON depends on a multitude of factors, including etiology, duration of compression, severity at presentation, and timing of intervention. Unlike other optic neuropathies, CON has a potentially reversible component if diagnosed early and treated promptly, since axonal dysfunction may precede irreversible axonal loss. These factors are associated with the following influences on an individual's prognosis :
- Etiology: Benign lesions (eg, meningioma, pituitary adenoma) generally carry a better prognosis than malignant or infiltrative causes (eg, lymphoma, metastatic tumors).
- Duration of compression: Prolonged compression leads to permanent axonal degeneration and optic atrophy. Early intervention before the development of pallor is associated with better visual recovery.
- Severity of visual loss at presentation: Patients presenting with mild to moderate visual loss or subtle field defects are more likely to recover compared to those with profound vision loss or severe optic atrophy.
- Treatment modality
- Surgical decompression: Decompression (eg, for pituitary adenoma, tuberculum sellae meningioma) often results in stabilization or improvement of vision, especially if performed early.
- Medical therapy: Conservative therapies (eg, corticosteroids in inflammatory or infiltrative conditions, radiotherapy for radiosensitive tumors) may also restore function.
- Timing: Delay in intervention significantly worsens outcomes.
- Age and general health: Younger patients tend to have better regenerative capacity and visual recovery.[103]
Expected Outcomes of Compressive Optic Neuropathy
Visual recovery occurs in approximately 60% to 80% of patients following timely decompression, with outcomes closely tied to the preoperative status. Visual field improvement may continue for several months after treatment. Incomplete recovery remains common when patients present with optic atrophy or long-standing compression, as irreversible ganglion cell loss limits visual potential.
Recurrence risk persists in cases of residual or recurrent tumors, where repeat compression may develop. Long-term surveillance, including neuroimaging and monitoring of visual function, is essential to detect early signs of recurrence.[122]
Long-Term Considerations
Permanent visual disability often develops in patients with late presentation, missed diagnosis, or aggressive pathology, and in some cases, vision loss becomes bilateral. Early recognition and timely intervention preserve functional vision, maintaining independence and quality of life. In contrast, delayed treatment frequently results in lifelong visual handicap.
Prognostic indicators (see Table 9) further refine expectations into the following:
-
Favorable: Short duration of symptoms, absence of optic disc pallor, and mild to moderate visual field defects.
-
Unfavorable: Severe baseline visual loss, established optic atrophy, older age, and malignant etiology.[124]
The prognosis of compressive optic neuropathy ranges from excellent to poor, depending on how early the diagnosis is made and treatment initiated. With prompt decompression or appropriate medical therapy, many patients can achieve significant visual improvement. However, delayed intervention leads to irreversible optic nerve damage, optic atrophy, and permanent visual disability.[125]
Table 9. Prognostic Indicators in Compressive Optic Neuropathy
|
Factor |
Favorable Prognosis |
Unfavorable Prognosis |
|
Etiology |
Benign lesions (pituitary adenoma, meningioma) |
Malignant, metastatic, or infiltrative tumors |
|
Duration of Compression |
Short duration (<6 months) |
Long-standing compression (>6–12 months) |
|
Baseline Visual Status |
Mild/moderate visual loss, no disc pallor |
Severe visual loss, optic disc pallor/atrophy |
|
Age |
Younger patients (better regenerative capacity) |
Older age (limited recovery potential) |
|
Treatment Timing |
Early decompression or medical therapy |
Delayed intervention |
|
Treatment Response |
Tumor shrinkage, good recovery after surgery or steroids |
Poor response, recurrence, or progression |
|
Follow-Up/Surveillance |
Regular imaging and visual field testing (prevents late damage) |
Missed follow-up, recurrent compression |
Complications
Complications of Compressive Optic Neuropathy
CON may lead to complications, eg, papilledema, blurry vision, an afferent pupillary defect, diplopia, nausea, vomiting, permanent vision loss, impaired extraocular motility, and significant limitations in daily activities due to vision impairment.[126] Decompressive surgery, although effective in many cases, carries risks that include hemorrhage, infection, complete vision loss, prolonged intubation, coma, and death. Untreated or late-diagnosed CON can produce a broad spectrum of ocular, neurological, systemic, and treatment-related complications. These complications may arise from the disease itself or from therapeutic interventions (eg, surgery, medical therapy, or radiotherapy).[127] Consequently, early diagnosis and timely intervention remain essential to reduce the risk of these potentially devastating outcomes.
Ocular Complications
Permanent visual loss frequently develops as progressive and irreversible optic atrophy results from chronic compression, with complete blindness occurring in untreated cases. Visual field defects, including scotomas and hemianopic field loss, may persist or worsen despite decompression. These defects often result in the loss of binocular vision and severe impairment of quality of life.
Additionally, optic disc changes, including secondary optic atrophy with marked thinning of the retinal nerve fiber layer, remain common in advanced stages of the disease. Ocular motility disorders result from compression or infiltration of cranial nerves III, IV, or VI, or involvement of the cavernous sinus, producing diplopia and strabismus. Tumors involving the orbit or surgical manipulation may also cause proptosis and lagophthalmos, leading to exposure keratopathy and secondary corneal damage.[128]
Neurological Complications
Endocrine dysfunction frequently follows pituitary adenomas or their treatment, manifesting as panhypopituitarism, diabetes insipidus, or Cushing’s disease. Moreover, intracranial extension of aggressive or malignant lesions can affect adjacent brain structures, causing seizures, hemiparesis, or altered sensorium. Tumors that obstruct cerebrospinal fluid pathways may lead to hydrocephalus and increased intracranial pressure. Parasellar lesions often compress nearby cranial nerves (III, IV, VI, V1, V2), producing ophthalmoplegia, trigeminal neuropathy, or facial numbness.[129]
Treatment-Related Complications
Surgical complications include optic nerve injury during decompression, cerebrospinal fluid leakage, meningitis, hemorrhage, and postoperative visual decline due to ischemia or edema. Radiotherapy may cause delayed toxicities, eg, radiation-induced optic neuropathy, retinopathy, dry eye, cataracts, or secondary neoplasia with high cumulative doses. Furthermore, medical therapy also carries risks, including corticosteroids, which may lead to systemic complications, eg, weight gain, hypertension, hyperglycemia, osteoporosis, and immunosuppression, while targeted therapies for thyroid eye disease may produce systemic toxicities, including liver dysfunction and gastrointestinal intolerance.[130]
Psychosocial and Functional Complications
Vision loss often results in diminished productivity and impaired quality of life, affecting the ability to drive, read, and work. Psychological consequences, eg, anxiety, depression, and social isolation, are common in patients living with chronic visual disability. Many patients require long-term rehabilitation, including low-vision aids, structured follow-up, and coordinated interprofessional care to maintain function and independence.[131]
Postoperative and Rehabilitation Care
Postoperative and long-term rehabilitation care play a central role in optimizing visual outcomes, preventing recurrence, and maintaining functional independence in patients with CON. Effective management requires coordinated interprofessional collaboration among ophthalmologists, neurosurgeons, endocrinologists, radiation oncologists, and rehabilitation specialists. Comprehensive management integrates visual rehabilitation, lifelong hormonal support when required, psychosocial interventions, and structured long-term surveillance to preserve functional independence and quality of life.[132]
Immediate Postoperative Care
Close monitoring of visual function remains critical during the early recovery phase. Daily assessments of visual acuity, pupillary reflexes, and visual fields should be performed to detect both improvement and deterioration in visual function. OCT of the retinal nerve fiber layer and visual evoked potentials provide objective documentation of structural and functional status.
Pain management, wound care, and vigilance for complications, eg, infection or cerebrospinal fluid leakage, support safe recovery. Short courses of corticosteroids may be prescribed to reduce postoperative edema around the optic nerve. Patients undergoing pituitary surgery require immediate endocrine evaluation with hormone profiling, followed by replacement therapy for cortisol, thyroid hormones, or vasopressin when indicated.[133]
Intermediate and Long-Term Follow-up
Ongoing surveillance is essential to detect recurrence and track disease stability. MRI or CT imaging at 3 to 6 months postoperatively, followed by annual studies, monitors for tumor regrowth or residual disease. Ophthalmic follow-up, including serial visual field testing and OCT, helps assess the progression or stabilization of optic nerve function. Endocrine management may require lifelong hormone replacement in pituitary-related cases. Patients receiving adjuvant radiotherapy benefit from long-term monitoring for radiation-induced complications, eg, optic neuropathy, retinopathy, and cataracts.[134]
Visual Rehabilitation
Rehabilitation strategies aim to maximize residual vision and restore functional independence. Low-vision aids, including magnifiers, telescopic lenses, high-contrast reading materials, and adaptive technologies, enhance daily activities. Occupational therapy provides training in mobility, self-care, and professional adaptations to mitigate visual field loss. Clinicians should counsel patients regarding driving and work decisions based on assessments of fitness for driving, workplace modification needs, and access to social assistance programs.[124]
Psychological and Social Support
Psychological care remains integral to recovery, as patients frequently experience anxiety, depression, or reduced quality of life related to vision loss. Counseling services help address these challenges, while support groups provide opportunities to share experiences, develop coping strategies, and improve social connectedness.[4]
Preventive and Lifestyle Measures
Preventive strategies include regular eye examinations to detect contralateral or recurrent involvement at an early stage. Lifestyle optimization, including smoking cessation and management of systemic conditions like diabetes and hypertension, enhances recovery and overall health. Patient education reinforces adherence to follow-up schedules, endocrine therapy, and recognition of warning signs indicating recurrence.
Consultations
The management of compressive optic neuropathy requires an interprofessional approach, as the condition often involves not only the optic nerve but also adjacent neurological, endocrine, and orbital structures. Appropriate consultations ensure comprehensive care, optimize visual outcomes, and address systemic and psychosocial aspects, which frequently include the following specialties:
- Ophthalmology/neuro-ophthalmology
- Primary consultation for diagnosis, baseline documentation of vision, color vision, contrast sensitivity, and visual fields.
- Ongoing monitoring of optic disc status (OCT, fundus exam) and visual function post-intervention.
- Guidance on visual rehabilitation and low vision aids if deficits persist.[39]
- Neurosurgery
- Crucial for patients with tumors (pituitary adenomas, meningiomas, craniopharyngiomas) or bony compressive lesions.
- Surgical planning for optic nerve decompression, tumor resection, or skull base approaches.
- Postoperative follow-up for complications such as CSF leaks, infections, or neurological deficits.[11]
- Endocrinology
- Evaluation of pituitary and hypothalamic function in sellar and parasellar lesions.
- Hormonal replacement therapy where required (thyroid, adrenal, gonadal, or vasopressin).
- Long-term monitoring for endocrine dysfunctions after surgery or radiotherapy.[135]
- Radiation oncology
- For patients who are not suitable for surgery or have residual/recurrent tumors. Planning and delivery of stereotactic radiosurgery or fractionated radiotherapy.
- Monitoring for radiation-induced complications (radiation optic neuropathy, retinopathy, cataract).[130]
- Medical oncology/hematology
- In cases of malignant, metastatic, or infiltrative lesions (eg, lymphoma, leukaemia, metastasis)
- Coordination of systemic chemotherapy or targeted therapy [136]
- Otolaryngology (ENT)/skull base surgery
- In cases of paranasal sinus tumors, nasopharyngeal masses, or lesions with orbital extension requiring combined surgical approaches [137]
- Rehabilitation medicine
- Guidance on visual rehabilitation, mobility training, and occupational adjustments.
- Prescription of low-vision aids and assistive technology.[138]
- Psychiatry/psychology
- Counseling to address depression, anxiety, and adjustment issues secondary to visual disability.
- Supportive therapy for coping with long-term consequences.
- Primary care/family physician
- Coordination of interprofessional care.
- Monitoring systemic comorbidities (eg, diabetes, hypertension) that may worsen prognosis.
- Ensuring compliance with follow-up schedules and referrals.
Consultations for compressive optic neuropathy should always be interprofessional, involving ophthalmology, neurosurgery, endocrinology, and other specialties as dictated by the etiology. This integrated approach ensures not just vision preservation, but also systemic stability, functional rehabilitation, and psychological well-being.[4]
Deterrence and Patient Education
Deterrence and patient education in compressive optic neuropathy depend on early detection, timely referral, and comprehensive patient empowerment. By fostering awareness of warning signs, ensuring consistent long-term follow-up, and facilitating access to rehabilitative and supportive resources, clinicians can significantly lower the risk of irreversible blindness while improving overall quality of life.[139]
When vision is significantly affected, the patient should be educated to use safety glasses to protect the unaffected eye. All patients who developed CON should attend their regular ophthalmologist care visits to evaluate for visual improvement or deterioration. As the etiologies of CON are multiple, the patient requires a comprehensive evaluation by an interprofessional team to determine the cause of CON and receive urgent treatment to improve clinical outcomes.
Early decompression is recommended for CON, but good results can still be obtained even if decompression is delayed. Patients should see an ophthalmologist as soon as they experience symptoms. More than half of the patients improve irrespective of their pre-operative visual status.[122][123] For tumor-related etiologies, 60% of patients will experience some improvement after optic nerve decompression.
Although compressive optic neuropathy often arises from unavoidable structural causes such as tumors or inflammatory lesions, early recognition, preventive strategies, and patient education play a pivotal role in preserving vision and improving long-term outcomes. Effective deterrence focuses on timely diagnosis, risk reduction, adherence to therapy, and empowerment through education.
Deterrence Strategies
Early detection and proactive screening remain essential in reducing morbidity from CON. Patients with pituitary adenomas, meningiomas, thyroid eye disease, or orbital tumors benefit from regular ophthalmic and neuroimaging evaluations to identify optic nerve compromise at an early stage. Routine visual field testing and OCT facilitate recognition of subtle progression before irreversible vision loss occurs.
Prompt referral to neurosurgery or oncology when compressive lesions are identified lowers the likelihood of permanent optic atrophy. Optimizing management of systemic conditions, eg, thyroid dysfunction, diabetes, and hypertension, further decreases secondary risks while supporting postoperative recovery. Education of both general practitioners and patients about warning signs, eg, progressive vision loss, field defects, color desaturation, or proptosis, prevents delayed presentations, promotes earlier specialist referral, and facilitates timely intervention.[140]
Patient Education
Patient education plays a central role in disease management. Patients must understand that CON represents a potentially reversible cause of vision loss when treated early, but becomes irreversible when neglected. Clinicians should clarify treatment goals with clear discussions of treatment expectations, emphasizing that therapy often aims to stabilize or improve vision rather than guarantee full recovery, particularly in advanced cases. Patients should also be informed about the range of available options, including surgical, medical, and radiation-based therapies, along with their associated risks and benefits.
Lifelong surveillance remains essential, requiring periodic ophthalmic assessments and repeat imaging even after successful surgical treatment due to the risk of recurrence or progression. Rehabilitation strategies, including low-vision aids, adaptive technologies, and occupational adjustments, help maintain independence in daily life. Counseling services and family involvement support psychological well-being, promoting effective coping with vision loss.[141]
Lifestyle and Preventive Guidance
Preventive measures enhance long-term outcomes by supporting neurological and vascular health. Smoking cessation, regular exercise, a balanced diet, and effective management of metabolic disorders all contribute to improved recovery potential and a reduced disease burden. Patients at higher risk, eg, those with thyroid eye disease, should receive education regarding eye safety and protection to prevent complications such as exposure keratopathy. Adherence to endocrine therapy remains critical in both pituitary and thyroid-related disease.
Pearls and Other Issues
The most important clinical insight in CON is that visual recovery is time-sensitive—prompt recognition and treatment dramatically alter outcomes. The biggest pitfall is delayed or missed diagnosis due to nonspecific presentations. A structured, interprofessional approach that combines vigilance, timely imaging, and patient education is key to preventing irreversible blindness.[121]
Additional key factors clinicians should bear in mind include:
- Early diagnosis is critical: Visual loss in CON can be reversible if intervention occurs before optic atrophy develops.
- Subtle clues matter: Progressive visual field defects, especially bitemporal hemianopia, decreased color vision, and relative afferent pupillary defect (RAPD) may precede overt visual loss.
- Imaging is indispensable: MRI with contrast is the gold standard for detecting compressive lesions; OCT and perimetry provide adjunctive monitoring.
- Not all visual loss is glaucomatous: Misdiagnosis of CON as glaucoma or optic neuritis is a common pitfall, especially in patients with normal IOP but progressive field defects.
- Interprofessional care: Collaboration of care between various specialties (neuro-ophthalmology, neurosurgery, endocrinology, oncology) yields the best long-term outcomes.[142]
Disposition
Patients with suspected CON require urgent referral for neuroimaging and specialist evaluation. Timely intervention with surgical decompression or medical therapy often preserves vision and prevents permanent deficits. Long-term management extends beyond the acute phase, requiring structured neuro-ophthalmic follow-up, routine imaging surveillance, and comprehensive systemic care, with particular emphasis on endocrine support when pituitary or parasellar disease is involved.[143]
Common Pitfalls
Several pitfalls frequently complicate the management of CON. Delayed referral remains a major concern, often resulting from misattribution of vision loss to refractive error, cataract, or glaucoma. Exclusive reliance on visual acuity also contributes to underdiagnosis, as many patients retain central vision until late in the disease, while peripheral field loss often goes unnoticed without the use of perimetry. Failure to examine both eyes can lead to missed contralateral involvement, which is common in pituitary and parasellar tumors. Inadequate follow-up after treatment carries a significant risk of missed recurrence or progressive visual decline. Neglecting systemic factors such as hormonal dysfunction or intracranial hypertension may further worsen prognosis and compromise long-term outcomes.[144]
Prevention and Long-Term Considerations
Preventive strategies and long-term planning strengthen patient outcomes. Education regarding early warning signs—including progressive field loss, color desaturation, diplopia, and proptosis—enhances timely recognition and intervention. Screening protocols for high-risk groups, eg, patients with pituitary adenomas, thyroid eye disease, or orbital tumors, support earlier detection of optic nerve compromise. Regular interprofessional follow-up fosters comprehensive care, reduces the risk of long-term complications, and facilitates timely retreatment when necessary. Integration of vision rehabilitation services should be initiated at an early stage to benefit patients with irreversible deficits by helping preserve independence and quality of life.
Enhancing Healthcare Team Outcomes
CON arises from lesions that mechanically compromise the optic nerve, leading to progressive vision loss if untreated. Causes range from benign tumors such as pituitary adenomas and meningiomas to infiltrative malignancies, orbital disease, and thyroid eye disease. Early recognition and prompt management are essential, as vision may be recoverable in the initial stages but irreversible once optic atrophy develops. Diagnosis requires careful clinical assessment, neuroimaging, and systemic evaluation, while long-term management focuses on surgical, medical, and rehabilitative strategies tailored to the underlying etiology.
The management of CON depends on coordinated interprofessional teamwork to optimize diagnostic accuracy, therapeutic outcomes, and patient safety. Ophthalmologists and neuro-ophthalmologists lead in early detection and monitoring, while neurosurgeons perform decompression or tumor resection.[53][145][53] Endocrinologists manage pituitary and hypothalamic dysfunction, and radiation or medical oncologists address residual or malignant disease.[146][147][146] Neuroradiologists play a critical role in determining etiology and monitoring treatment response. Nurses and advanced practitioners reinforce education, perioperative care, and continuity, as well as acting as liaisons between specialists.[148] Pharmacists ensure safe pharmacological therapy and support adherence, providing counseling on potential adverse effects, drug interactions, and adherence strategies, while also supporting cost-effective medication choices and access to specialty therapies.[149][150][151][150][149] Rehabilitation specialists, psychologists, and social workers all contribute to long-term functional recovery, effective coping strategies, and overall quality of life.
High-quality outcomes depend on clear communication, shared decision-making, and defined responsibilities among physicians, nurses, pharmacists, and allied health professionals. Regular case conferences and coordinated follow-up prevent delays, misdiagnoses, or treatment complications. By integrating surgical precision, medical expertise, rehabilitative interventions, and psychosocial support, the interprofessional team safeguards vision, enhances safety, and promotes independence for patients living with CON.[152]
Media
(Click Image to Enlarge)
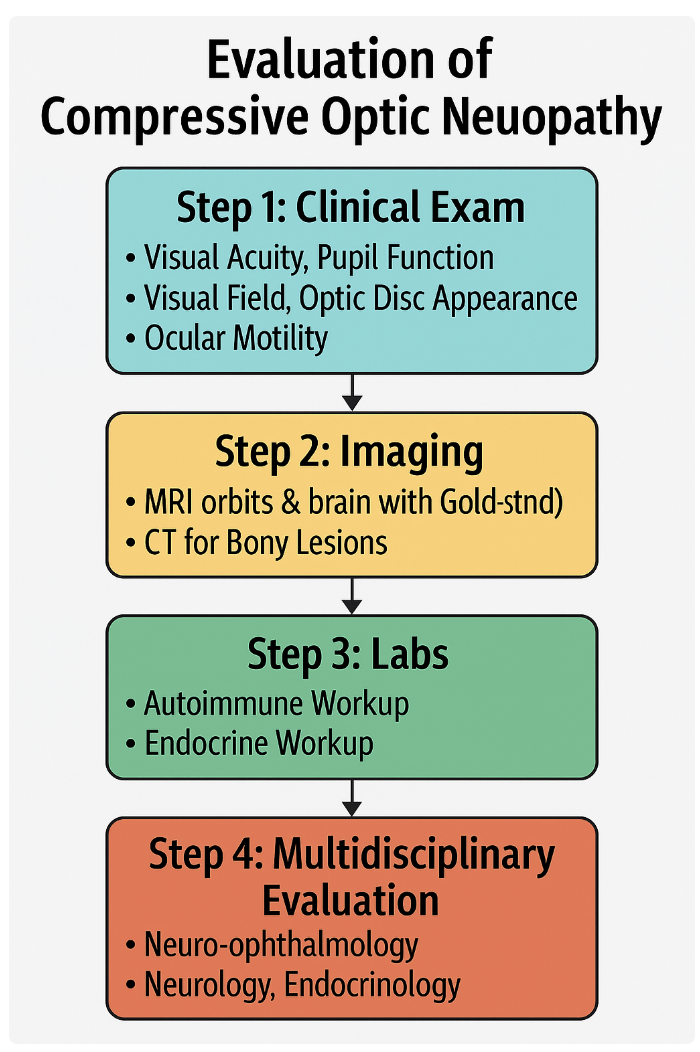
Compressive Optic Neuropathy Evaluation. This image depicts the evaluation approach for compressive optic neuropathy.
Contributed by B Gurnani, MD
References
Bastakis GG, Ktena N, Karagogeos D, Savvaki M. Models and treatments for traumatic optic neuropathy and demyelinating optic neuritis. Developmental neurobiology. 2019 Aug:79(8):819-836. doi: 10.1002/dneu.22710. Epub 2019 Jul 25 [PubMed PMID: 31297983]
Jonas JB, Müller-Bergh JA, Schlötzer-Schrehardt UM, Naumann GO. Histomorphometry of the human optic nerve. Investigative ophthalmology & visual science. 1990 Apr:31(4):736-44 [PubMed PMID: 2335441]
Jonas JB, Schmidt AM, Müller-Bergh JA, Schlötzer-Schrehardt UM, Naumann GO. Human optic nerve fiber count and optic disc size. Investigative ophthalmology & visual science. 1992 May:33(6):2012-8 [PubMed PMID: 1582806]
Rakusiewicz-Krasnodębska K, Bogusz-Wójcik A, Moszczyńska E, Jaworski M, Kowalczyk P, Hautz W. Evaluation of the Effect of Optic Nerve Compression by Craniopharyngioma on Retinal Nerve Fiber Layer Thickness in Pediatric Patients. Cancers. 2025 Aug 5:17(15):. doi: 10.3390/cancers17152574. Epub 2025 Aug 5 [PubMed PMID: 40805268]
Wang L, Tan Y, Li F, Liang Y, Chen G, Huang AM, Li L, Wang J, Liu Z. Unilateral Painless Visual Loss in Sphenoid Mucoceles with Optic Neuropathy. Case reports in ophthalmology. 2025 Jan-Dec:16(1):559-566. doi: 10.1159/000546758. Epub 2025 Jul 7 [PubMed PMID: 40800573]
Level 3 (low-level) evidenceBourke C, Panteli V, Marmoy OR, Thompson DA, Mankad K, Sudhakar S, James G, Garnham J, Connor A, Cheung MS, Bowman R. Optic neuropathy associated with vitamin A deficiency in children: a case series. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2025 Aug:29(4):104277. doi: 10.1016/j.jaapos.2025.104277. Epub 2025 Jul 31 [PubMed PMID: 40752868]
Level 2 (mid-level) evidenceHuq S, McDowell MM, Alattar AA, Stefko ST, Gardner PA. Supraorbital craniotomy for microvascular decompression of optic nerve due to neurovascular conflict with anterior cerebral artery: 2-Dimensional operative video. Clinical neurology and neurosurgery. 2025 Oct:257():109062. doi: 10.1016/j.clineuro.2025.109062. Epub 2025 Jul 22 [PubMed PMID: 40743657]
Pinzon RT, Afifudin M, Digdoyo A, Naibaho FKC, Parikesit PG, Allendio YS. Foster Kennedy Syndrome from Frontal Lobe Meningioma: A Rare Case Report. Romanian journal of ophthalmology. 2025 Apr-Jun:69(2):271-274. doi: 10.22336/rjo.2025.43. Epub [PubMed PMID: 40698105]
Level 3 (low-level) evidenceFearington FW, Peraza LR, Hernandez-Herrera GA, Awadallah AS, Stokken JK, Wagner LH, Bradley EA, Stan MN, Bothun ED, Tooley AA. Predicting visual acuity recovery in orbital decompression surgery for dysthyroid optic neuropathy. Thyroid research. 2025 Jul 1:18(1):33. doi: 10.1186/s13044-025-00248-5. Epub 2025 Jul 1 [PubMed PMID: 40588768]
Ranjan A, Chhabra AK, Kumar M. Orbital venous lymphatic malformations: case series on minimally invasive treatment approach. Romanian journal of ophthalmology. 2025 Apr-Jun:69(2):280-286. doi: 10.22336/rjo.2025.45. Epub [PubMed PMID: 40698103]
Level 2 (mid-level) evidenceDonovan K, Murdock N, Mahan M, Mehta V. Sinonasal mucosal melanoma presenting with ocular symptoms: Two case reports and a literature review. European journal of ophthalmology. 2025 Aug 25:():11206721251370912. doi: 10.1177/11206721251370912. Epub 2025 Aug 25 [PubMed PMID: 40853363]
Level 3 (low-level) evidenceLevine DN, Rapalino AI. The Pathogenesis of Papilledema: Review of the Literature and a New Hypothesis. Bulletin of mathematical biology. 2025 Jun 25:87(8):101. doi: 10.1007/s11538-025-01465-7. Epub 2025 Jun 25 [PubMed PMID: 40560479]
Brown P, Demaerel P, McNaught A, Revesz T, Graham E, Kendall BE, Plant G. Neuro-ophthalmological presentation of non-invasive Aspergillus sinus disease in the non-immunocompromised host. Journal of neurology, neurosurgery, and psychiatry. 1994 Feb:57(2):234-7 [PubMed PMID: 8126516]
Level 3 (low-level) evidenceKhochtali S, Zayani M, Ksiaa I, Ben Meriem I, Zaouali S, Jelliti B, Khairallah M. [Idiopathic orbital inflammatory syndrome: Report of 24 cases]. Journal francais d'ophtalmologie. 2018 Apr:41(4):333-342. doi: 10.1016/j.jfo.2017.09.013. Epub 2018 Apr 21 [PubMed PMID: 29685738]
Level 3 (low-level) evidenceSaeed P, Tavakoli Rad S, Bisschop PHLT. Dysthyroid Optic Neuropathy. Ophthalmic plastic and reconstructive surgery. 2018 Jul/Aug:34(4S Suppl 1):S60-S67. doi: 10.1097/IOP.0000000000001146. Epub [PubMed PMID: 29927882]
Daldoul N, Knani L, Gatfaoui F, Mahjoub H. [Management of moderate and severe dysthyroid orbitopathy: about 22 cases]. The Pan African medical journal. 2017:27():257. doi: 10.11604/pamj.2017.27.257.13008. Epub 2017 Aug 7 [PubMed PMID: 29187926]
Level 3 (low-level) evidenceLi Z. Novel perspectives on the pharmacological treatment of thyroid-associated ophthalmopathy. Frontiers in endocrinology. 2024:15():1469268. doi: 10.3389/fendo.2024.1469268. Epub 2025 Jan 13 [PubMed PMID: 39872310]
Level 3 (low-level) evidenceLally E, Murchison AP, Moster ML, Bilyk JR. Compressive optic neuropathy from neurosarcoidosis. Ophthalmic plastic and reconstructive surgery. 2015 May-Jun:31(3):e79. doi: 10.1097/IOP.0000000000000342. Epub [PubMed PMID: 25427128]
Level 3 (low-level) evidenceYoshinaga T, Kurokawa T, Uehara T, Nitta J, Horiuchi T, Sekijima Y. [Optic neuropathy from connected intra- and extraorbital lesions in IgG4-related disease]. Rinsho shinkeigaku = Clinical neurology. 2019 Nov 8:59(11):746-751. doi: 10.5692/clinicalneurol.cn-001342. Epub 2019 Oct 26 [PubMed PMID: 31656266]
Hwang G, Jin SY, Kim HS. IgG4-related disease presenting as hypertrophic pachymeningitis and compressive optic neuropathy. Joint bone spine. 2016 Oct:83(5):601-2. doi: 10.1016/j.jbspin.2015.07.016. Epub 2016 Apr 7 [PubMed PMID: 27068616]
Oh JK, Chandhoke DK, Shinder R. Compressive optic neuropathy with vision loss due to IgG4-related orbital disease. Orbit (Amsterdam, Netherlands). 2020 Dec:39(6):455. doi: 10.1080/01676830.2019.1672752. Epub 2019 Oct 8 [PubMed PMID: 31590594]
Takeishi M, Oshitari T, Ota S, Baba T, Yamamoto S. The Case of IgG4-related Ophthalmic Disease Accompanied by Compressive Optic Neuropathy. Neuro-ophthalmology (Aeolus Press). 2018 Aug:42(4):246-250. doi: 10.1080/01658107.2017.1389962. Epub 2017 Oct 25 [PubMed PMID: 30042797]
Level 3 (low-level) evidenceFukiyama Y, Oku H, Hashimoto Y, Nishikawa Y, Tonari M, Sugasawa J, Miyachi S, Ikeda T. Complete Recovery from Blindness in Case of Compressive Optic Neuropathy due to Unruptured Anterior Cerebral Artery Aneurysm. Case reports in ophthalmology. 2017 Jan-Apr:8(1):157-162. doi: 10.1159/000458753. Epub 2017 Mar 7 [PubMed PMID: 28611648]
Level 3 (low-level) evidenceLischynski JR, Molot-Toker S, Mansouri B, Kaufmann AM. Compressive optic neuropathy caused by a nonectatic internal carotid artery: illustrative case. Journal of neurosurgery. Case lessons. 2025 Mar 31:9(13):. pii: CASE24623. doi: 10.3171/CASE24623. Epub 2025 Mar 31 [PubMed PMID: 40164001]
Level 3 (low-level) evidenceTan AC, Farooqui S, Li X, Tan YL, Cullen J, Lim W, Leng SL, Looi A, Tow S. Ocular manifestations and the clinical course of carotid cavernous sinus fistulas in Asian patients. Orbit (Amsterdam, Netherlands). 2014 Feb:33(1):45-51. doi: 10.3109/01676830.2013.851253. Epub 2013 Nov 6 [PubMed PMID: 24195725]
Level 2 (mid-level) evidencePatel SR, Rosenberg JB, Barmettler A. Interventions for orbital lymphangioma. The Cochrane database of systematic reviews. 2019 May 15:5(5):CD013000. doi: 10.1002/14651858.CD013000.pub2. Epub 2019 May 15 [PubMed PMID: 31094450]
Level 1 (high-level) evidenceBerthout A, Jacomet PV, Putterman M, Galatoire O, Morax S. [Surgical treatment of diffuse adult orbital lymphangioma: two case studies]. Journal francais d'ophtalmologie. 2008 Dec:31(10):1006-17 [PubMed PMID: 19107078]
Level 3 (low-level) evidenceCaton MT Jr, Zamani AA, Du R, Prasad S. Optic Neuropathy Due to Compression by an Ectatic Internal Carotid Artery Within the Orbital Apex. Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society. 2021 Mar 1:41(1):e103-e104. doi: 10.1097/WNO.0000000000000975. Epub [PubMed PMID: 32366760]
Fargen KM, Blackburn S. Surgical decompression for optic neuropathy from carotid artery ectasia: case report with technical considerations. World neurosurgery. 2014 Jul-Aug:82(1-2):239.e9-12. doi: 10.1016/j.wneu.2013.06.023. Epub 2013 Jul 10 [PubMed PMID: 23851213]
Level 3 (low-level) evidenceKong DS, Shin HJ, Kim HY, Chung SK, Nam DH, Lee JI, Park K, Kim JH. Endoscopic optic canal decompression for compressive optic neuropathy. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia. 2011 Nov:18(11):1541-5. doi: 10.1016/j.jocn.2011.02.042. Epub 2011 Sep 15 [PubMed PMID: 21924915]
Blanch RJ, Joseph IJ, Cockerham K. Traumatic optic neuropathy management: a systematic review. Eye (London, England). 2024 Aug:38(12):2312-2318. doi: 10.1038/s41433-024-03129-7. Epub 2024 Jun 11 [PubMed PMID: 38862644]
Level 1 (high-level) evidenceSabermoghaddam A, Sardabi M, Kiarudi MY, Shokoohi-Rad S. The role of early office-based needle aspiration in the management of subperiosteal hematoma. Orbit (Amsterdam, Netherlands). 2019 Oct:38(5):387-389. doi: 10.1080/01676830.2018.1528618. Epub 2018 Oct 18 [PubMed PMID: 30335540]
Zhilin G, Huoniu O, Zhihua C, Guorong D. Wide optic nerve canal decompression for the treatment of blindness resulting from an indirect optic nerve injury. The Journal of craniofacial surgery. 2011 Jul:22(4):1463-5. doi: 10.1097/SCS.0b013e31821d184a. Epub [PubMed PMID: 21772157]
Level 2 (mid-level) evidenceSheremet NL, Khanakova NA. [Etiology and diagnostics of compressive optic neuropathies]. Vestnik oftalmologii. 2018:134(6):72-82. doi: 10.17116/oftalma201813406172. Epub [PubMed PMID: 30721204]
Kang H, Takahashi Y, Nishimura K, Yasuda M, Akutsu H, Kakizaki H. Improved Vision from Severe Compressive Optic Neuropathy by Apical Cavernous Hemangioma. Case reports in ophthalmology. 2016 Jan-Apr:7(1):179-83. doi: 10.1159/000445316. Epub 2016 Mar 31 [PubMed PMID: 27099610]
Level 3 (low-level) evidenceDalle Ore CL, Magill ST, Rodriguez Rubio R, Shahin MN, Aghi MK, Theodosopoulos PV, Villanueva-Meyer JE, Kersten RC, Idowu OO, Vagefi MR, McDermott MW. Hyperostosing sphenoid wing meningiomas: surgical outcomes and strategy for bone resection and multidisciplinary orbital reconstruction. Journal of neurosurgery. 2021 Mar 1:134(3):711-720. doi: 10.3171/2019.12.JNS192543. Epub 2020 Mar 6 [PubMed PMID: 32114535]
Keilani C, Abada S. An Uncommon Case of Symptomatic Multiple Meningiomas with Bilateral Compressive Optic Neuropathy Rapidly Induced under Cyprotero ne Acetate Treatment. Current drug safety. 2017:12(2):134-139. doi: 10.2174/1574886312666170523154548. Epub [PubMed PMID: 28545357]
Level 3 (low-level) evidenceJiang L, Shi J, Liu W, Kang J, Wang N. [Clinical feature of chronic compressive optic neuropathy without optic atrophy]. [Zhonghua yan ke za zhi] Chinese journal of ophthalmology. 2014 Dec:50(12):889-93 [PubMed PMID: 25619179]
Level 2 (mid-level) evidenceZiaei MM, Ziaei H. Compressive Optic Neuropathy Caused by Orbital Non-Hodgkin's Lymphoma. Case reports in ophthalmological medicine. 2012:2012():894062. doi: 10.1155/2012/894062. Epub 2012 Feb 14 [PubMed PMID: 22606505]
Level 3 (low-level) evidenceLee MJ, Kang MH, Yeom JH, Yeom H, Seong M, Cho H, Shin YU. Compressive optic neuropathy secondary to Ewing sarcoma in the paranasal sinus: A case report. Medicine. 2018 Nov:97(44):e13027. doi: 10.1097/MD.0000000000013027. Epub [PubMed PMID: 30383663]
Level 3 (low-level) evidenceDeKlotz TR, Stefko ST, Fernandez-Miranda JC, Gardner PA, Snyderman CH, Wang EW. Endoscopic Endonasal Optic Nerve Decompression for Fibrous Dysplasia. Journal of neurological surgery. Part B, Skull base. 2017 Feb:78(1):24-29. doi: 10.1055/s-0036-1584078. Epub 2016 Jun 2 [PubMed PMID: 28180039]
MacNally SP, Ashida R, Williams TJ, King AT, Leatherbarrow B, Rutherford SA. A case of acute compressive optic neuropathy secondary to aneurysmal bone cyst formation in fibrous dysplasia. British journal of neurosurgery. 2010 Dec:24(6):705-7. doi: 10.3109/02688697.2010.500409. Epub 2010 Jul 22 [PubMed PMID: 20649393]
Level 3 (low-level) evidenceEretto P, Krohel GB, Shihab ZM, Wallach S, Hay P. Optic neuropathy in Paget's disease. American journal of ophthalmology. 1984 Apr:97(4):505-10 [PubMed PMID: 6720822]
Loke JY, Mohd Ali H, Kamalden TA. Osteopetrosis craniopathy: a rare cause of bilateral compressive optic neuropathy and facial nerve palsy. Postgraduate medical journal. 2019 Sep:95(1127):513. doi: 10.1136/postgradmedj-2019-136527. Epub 2019 Jul 10 [PubMed PMID: 31292279]
Medsinge A, Sylvester C, Tyler-Kabara E, Stefko ST. Bilateral endoscopic optic nerve decompression in an infant with osteopetrosis. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2019 Feb:23(1):40-42. doi: 10.1016/j.jaapos.2018.05.012. Epub 2018 Aug 29 [PubMed PMID: 30171897]
Pletcher SD, Metson R. Endoscopic optic nerve decompression for nontraumatic optic neuropathy. Archives of otolaryngology--head & neck surgery. 2007 Aug:133(8):780-3 [PubMed PMID: 17709616]
Level 2 (mid-level) evidenceBae JW, Kim YH, Kim SK, Wang KC, Shin HY, Kang HJ, Park SH, Phi JH. Langerhans cell histiocytosis causing acute optic neuropathy. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 2015 Apr:31(4):615-9. doi: 10.1007/s00381-014-2610-5. Epub 2015 Jan 8 [PubMed PMID: 25566821]
Level 3 (low-level) evidenceTzamalis A, Diafas A, Riga P, Konstantinidis I, Ziakas N. Onodi Cell Mucocele-Associated Optic Neuropathy: A Rare Case Report and Review of the Literature. Journal of current ophthalmology. 2020 Jan-Mar:32(1):107-113. doi: 10.1016/j.joco.2019.08.006. Epub 2020 Mar 23 [PubMed PMID: 32510023]
Level 3 (low-level) evidenceLi E, Howard MA, Vining EM, Becker RD, Silbert J, Lesser RL. Visual prognosis in compressive optic neuropathy secondary to sphenoid sinus mucocele: A systematic review. Orbit (Amsterdam, Netherlands). 2018 Aug:37(4):280-286. doi: 10.1080/01676830.2017.1423087. Epub 2018 Jan 5 [PubMed PMID: 29303386]
Level 1 (high-level) evidenceBhattacharjee H, Soibam R, Deori N. Sphenoethmoidal mucocele presenting with unilateral visual loss. Eye and brain. 2010:2():117-120. doi: 10.2147/EB.S9719. Epub 2010 Sep 15 [PubMed PMID: 28539770]
Che SA, Lee YW, Yoo YJ. Compressive optic neuropathy due to posterior ethmoid mucocele. BMC ophthalmology. 2023 Oct 23:23(1):426. doi: 10.1186/s12886-023-03168-w. Epub 2023 Oct 23 [PubMed PMID: 37867195]
Sivadasan A, Alexander M, Mathew V, Mani S, Patil AK. Radiological evolution and delayed resolution of an optic nerve tuberculoma: Challenges in diagnosis and treatment. Annals of Indian Academy of Neurology. 2013 Jan:16(1):114-7. doi: 10.4103/0972-2327.107722. Epub [PubMed PMID: 23661979]
Level 3 (low-level) evidenceLiu A, Craver EC, Bhatti MT, Chen JJ. Population-Based Incidence and Outcomes of Compressive Optic Neuropathy. American journal of ophthalmology. 2022 Apr:236():130-135. doi: 10.1016/j.ajo.2021.10.018. Epub 2021 Oct 22 [PubMed PMID: 34695397]
Tanda ML, Piantanida E, Liparulo L, Veronesi G, Lai A, Sassi L, Pariani N, Gallo D, Azzolini C, Ferrario M, Bartalena L. Prevalence and natural history of Graves' orbitopathy in a large series of patients with newly diagnosed graves' hyperthyroidism seen at a single center. The Journal of clinical endocrinology and metabolism. 2013 Apr:98(4):1443-9. doi: 10.1210/jc.2012-3873. Epub 2013 Feb 13 [PubMed PMID: 23408569]
Level 2 (mid-level) evidenceHiromatsu Y, Eguchi H, Tani J, Kasaoka M, Teshima Y. Graves' ophthalmopathy: epidemiology and natural history. Internal medicine (Tokyo, Japan). 2014:53(5):353-60 [PubMed PMID: 24583420]
Bishokarma S , Shrestha S , Ranabhat K , Koirala S , Shrestha D , Panth R , Gongal DN . Outcome of Surgical Resection of Craniopharyngioma:Single Center 12 Years' Experience. Kathmandu University medical journal (KUMJ). 2018 Oct.-Dec.:16(64):328-332 [PubMed PMID: 31729348]
Pai B, Ferdinand D. Fibrous dysplasia causing safeguarding concerns. Archives of disease in childhood. 2013 Dec:98(12):1003. doi: 10.1136/archdischild-2013-304490. Epub 2013 Aug 21 [PubMed PMID: 23966029]
Level 3 (low-level) evidenceHaik BG, Karcioglu ZA, Gordon RA, Pechous BP. Capillary hemangioma (infantile periocular hemangioma). Survey of ophthalmology. 1994 Mar-Apr:38(5):399-426 [PubMed PMID: 8009426]
Level 3 (low-level) evidenceLéauté-Labrèze C, Harper JI, Hoeger PH. Infantile haemangioma. Lancet (London, England). 2017 Jul 1:390(10089):85-94. doi: 10.1016/S0140-6736(16)00645-0. Epub 2017 Jan 13 [PubMed PMID: 28089471]
Hattori Y, Tahara S, Aso S, Matsui H, Fushimi K, Yasunaga H, Morita A. Pituitary surgery's epidemiology using a national inpatient database in Japan. Acta neurochirurgica. 2020 Jun:162(6):1317-1323. doi: 10.1007/s00701-020-04270-4. Epub 2020 Mar 3 [PubMed PMID: 32125502]
Fried I, Tabori U, Tihan T, Reginald A, Bouffet E. Optic pathway gliomas: a review. CNS oncology. 2013 Mar:2(2):143-59. doi: 10.2217/cns.12.47. Epub [PubMed PMID: 25057976]
Level 3 (low-level) evidenceRevilla-Pacheco F, Escalante-Seyffert MC, Herrada-Pineda T, Manrique-Guzman S, Perez-Zuniga I, Rangel-Suarez S, Rubalcava-Ortega J, Loyo-Varela M. Prevalence of Incidental Clinoid Segment Saccular Aneurysms. World neurosurgery. 2018 Jul:115():e244-e251. doi: 10.1016/j.wneu.2018.04.027. Epub 2018 Apr 12 [PubMed PMID: 29656153]
Etminan N, Rinkel GJ. Unruptured intracranial aneurysms: development, rupture and preventive management. Nature reviews. Neurology. 2016 Dec:12(12):699-713. doi: 10.1038/nrneurol.2016.150. Epub 2016 Nov 3 [PubMed PMID: 27808265]
Zhao X, He M, Yang R, Geng N, Zhu X, Tang N. The global, regional, and national brain and central nervous system cancer burden and trends from 1990 to 2021: an analysis based on the Global Burden of Disease Study 2021. Frontiers in neurology. 2025:16():1574614. doi: 10.3389/fneur.2025.1574614. Epub 2025 Jun 18 [PubMed PMID: 40606128]
Campen CJ, Gutmann DH. Optic Pathway Gliomas in Neurofibromatosis Type 1. Journal of child neurology. 2018 Jan:33(1):73-81. doi: 10.1177/0883073817739509. Epub [PubMed PMID: 29246098]
Yang M, He W. Age and gender influence on clinical manifestations of thyroid-associated ophthalmopathy: a case series of 2479 Chinese patients. Frontiers in endocrinology. 2024:15():1434155. doi: 10.3389/fendo.2024.1434155. Epub 2024 Oct 3 [PubMed PMID: 39421533]
Level 2 (mid-level) evidenceMcAlinden C. An overview of thyroid eye disease. Eye and vision (London, England). 2014:1():9. doi: 10.1186/s40662-014-0009-8. Epub 2014 Dec 10 [PubMed PMID: 26605355]
Level 3 (low-level) evidenceGarg P, Ranjan V, Avnisha, Hembrom S, Goel S, Malhotra S. The changing trend of fungal infection in invasive rhinosinusitis in the COVID era. Journal of family medicine and primary care. 2024 Apr:13(4):1428-1433. doi: 10.4103/jfmpc.jfmpc_871_23. Epub 2024 Apr 22 [PubMed PMID: 38827671]
Sugiyama T, Kuroda S, Nakayama N, Houkin K. [Invasive paranasal sinus fungal infection developing orbital apex syndrome and causing internal carotid artery infiltration: reports of 3 cases]. No shinkei geka. Neurological surgery. 2011 Feb:39(2):155-61 [PubMed PMID: 21321374]
Level 3 (low-level) evidenceShum JW, Liu K, So KF. The progress in optic nerve regeneration, where are we? Neural regeneration research. 2016 Jan:11(1):32-6. doi: 10.4103/1673-5374.175038. Epub [PubMed PMID: 26981073]
Howell GR, Libby RT, Jakobs TC, Smith RS, Phalan FC, Barter JW, Barbay JM, Marchant JK, Mahesh N, Porciatti V, Whitmore AV, Masland RH, John SW. Axons of retinal ganglion cells are insulted in the optic nerve early in DBA/2J glaucoma. The Journal of cell biology. 2007 Dec 31:179(7):1523-37 [PubMed PMID: 18158332]
Flaharty PM, Sergott RC, Lieb W, Bosley TM, Savino PJ. Optic nerve sheath decompression may improve blood flow in anterior ischemic optic neuropathy. Ophthalmology. 1993 Mar:100(3):297-302; discussion 303-5 [PubMed PMID: 8459996]
Knox DL, Kerrison JB, Green WR. Histopathologic studies of ischemic optic neuropathy. Transactions of the American Ophthalmological Society. 2000:98():203-20; discussion 221-2 [PubMed PMID: 11190024]
Tongal S, Uyanik I, Karademir FP, Cakir I, Inal A. Olfactory Groove Meningioma Compressing the Optic Chiasm and Optic Nerve: Improvement of Visual Functions by Surgical Intervention. Romanian journal of ophthalmology. 2025 Apr-Jun:69(2):247-253. doi: 10.22336/rjo.2025.39. Epub [PubMed PMID: 40698106]
Azeem S, Al-Abri M, Al-Hinai A, Al-Fadhil N. Progressive visual loss with systemic symptoms in an adult. Oman journal of ophthalmology. 2017 Sep-Dec:10(3):262. doi: 10.4103/ojo.OJO_110_2017. Epub [PubMed PMID: 29118514]
Newman N, Biousse V. Diagnostic approach to vision loss. Continuum (Minneapolis, Minn.). 2014 Aug:20(4 Neuro-ophthalmology):785-815. doi: 10.1212/01.CON.0000453317.67637.46. Epub [PubMed PMID: 25099095]
Level 3 (low-level) evidenceVan Stavern GP. Metabolic, hereditary, traumatic, and neoplastic optic neuropathies. Continuum (Minneapolis, Minn.). 2014 Aug:20(4 Neuro-ophthalmology):877-906. doi: 10.1212/01.CON.0000453313.37143.9b. Epub [PubMed PMID: 25099099]
Sue S. Test distance vision using a Snellen chart. Community eye health. 2007 Sep:20(63):52 [PubMed PMID: 17971914]
Mikolajczyk B, Ritter A, Larson C, Connett J, Olson J, McClelland C, Lee MS. Red Desaturation Prevalence and Severity in Healthy Patients. Neurology. Clinical practice. 2022 Feb:12(1):1-5. doi: 10.1212/CPJ.0000000000001011. Epub [PubMed PMID: 36157619]
Broadway DC. How to test for a relative afferent pupillary defect (RAPD). Community eye health. 2012:25(79-80):58-9 [PubMed PMID: 23520419]
Feller D, Chiarotto A, Koes B, Maselli F, Mourad F. Red flags for potential serious pathologies in people with neck pain: a systematic review of clinical practice guidelines. Archives of physiotherapy. 2024 Jan-Dec:14():105-115. doi: 10.33393/aop.2024.3245. Epub 2024 Dec 4 [PubMed PMID: 39639931]
Level 1 (high-level) evidenceBoland MV, Quigley HA. Evaluation of a combined index of optic nerve structure and function for glaucoma diagnosis. BMC ophthalmology. 2011 Feb 11:11():6. doi: 10.1186/1471-2415-11-6. Epub 2011 Feb 11 [PubMed PMID: 21314957]
Deyrup AT, D'Ambrosio D, Muir J, Laboratory Test Working Group, Knollmann-Ritschel B. Essential laboratory tests for medical education. Academic pathology. 2022:9(1):100046. doi: 10.1016/j.acpath.2022.100046. Epub 2022 Sep 13 [PubMed PMID: 36133797]
Ghorishi A, Alayon A, Ghaddar T, Kandah M, Amundson PK. MR and CT angiography in the diagnosis of vasculitides. BJR open. 2023:5(1):20220020. doi: 10.1259/bjro.20220020. Epub 2023 Sep 25 [PubMed PMID: 37953869]
Watts J, Box G, Galvin A, Brotchie P, Trost N, Sutherland T. Magnetic resonance imaging of meningiomas: a pictorial review. Insights into imaging. 2014 Feb:5(1):113-22. doi: 10.1007/s13244-013-0302-4. Epub 2014 Jan 8 [PubMed PMID: 24399610]
Park SK, Lee IS, Choi JY, Cho KH, Suh KJ, Lee JW, Song JW. CT and MRI of fibrous dysplasia of the spine. The British journal of radiology. 2012 Jul:85(1015):996-1001. doi: 10.1259/bjr/81329736. Epub 2011 Dec 13 [PubMed PMID: 22167510]
Nagesh CP, Rao R, Hiremath SB, Honavar SG. Magnetic resonance imaging of the orbit, Part 1: Basic principles and radiological approach. Indian journal of ophthalmology. 2021 Oct:69(10):2574-2584. doi: 10.4103/ijo.IJO_3141_20. Epub [PubMed PMID: 34571597]
Marmoy OR, Viswanathan S. Clinical electrophysiology of the optic nerve and retinal ganglion cells. Eye (London, England). 2021 Sep:35(9):2386-2405. doi: 10.1038/s41433-021-01614-x. Epub 2021 Jun 11 [PubMed PMID: 34117382]
Kakaria AK. Imaging in neuro-ophthalmology: An overview. Oman journal of ophthalmology. 2009 May:2(2):57-61. doi: 10.4103/0974-620X.53033. Epub [PubMed PMID: 20671830]
Level 3 (low-level) evidenceMargolin E, Blair K, Shemesh A. Toxic and Nutritional Optic Neuropathy. StatPearls. 2025 Jan:(): [PubMed PMID: 29763154]
Gibson A, Kothapudi VN, Czyz CN. Graves Disease Orbital Decompression. StatPearls. 2025 Jan:(): [PubMed PMID: 29261978]
Woods RSR, Pilson Q, Kharytaniuk N, Cassidy L, Khan R, Timon CVI. Outcomes of endoscopic orbital decompression for graves' ophthalmopathy. Irish journal of medical science. 2020 Feb:189(1):177-183. doi: 10.1007/s11845-019-02043-2. Epub 2019 Jun 16 [PubMed PMID: 31203506]
Boboridis KG, Bunce C. Surgical orbital decompression for thyroid eye disease. The Cochrane database of systematic reviews. 2011 Dec 7:(12):CD007630. doi: 10.1002/14651858.CD007630.pub2. Epub 2011 Dec 7 [PubMed PMID: 22161415]
Level 1 (high-level) evidenceKumaran AM, Sundar G, Chye LT. Traumatic optic neuropathy: a review. Craniomaxillofacial trauma & reconstruction. 2015 Mar:8(1):31-41. doi: 10.1055/s-0034-1393734. Epub 2014 Nov 25 [PubMed PMID: 25709751]
Wilhelm H. [Traumatic optic neuropathy]. Laryngo- rhino- otologie. 2009 Mar:88(3):194-203; quiz 204-7. doi: 10.1055/s-0029-1192010. Epub 2009 Feb 26 [PubMed PMID: 19247896]
Yu-Wai-Man P, Griffiths PG. Surgery for traumatic optic neuropathy. The Cochrane database of systematic reviews. 2005 Oct 19:(4):CD005024 [PubMed PMID: 16235388]
Level 1 (high-level) evidenceCen LP, Park KK, So KF. Optic nerve diseases and regeneration: How far are we from the promised land? Clinical & experimental ophthalmology. 2023 Aug:51(6):627-641. doi: 10.1111/ceo.14259. Epub 2023 Jun 15 [PubMed PMID: 37317890]
Braun TL, Bhadkamkar MA, Jubbal KT, Weber AC, Marx DP. Orbital Decompression for Thyroid Eye Disease. Seminars in plastic surgery. 2017 Feb:31(1):40-45. doi: 10.1055/s-0037-1598192. Epub [PubMed PMID: 28255288]
Shin HJ, Costello F. Imaging the optic nerve with optical coherence tomography. Eye (London, England). 2024 Aug:38(12):2365-2379. doi: 10.1038/s41433-024-03165-3. Epub 2024 Jul 3 [PubMed PMID: 38961147]
Bartalena L, Kahaly GJ, Baldeschi L, Dayan CM, Eckstein A, Marcocci C, Marinò M, Vaidya B, Wiersinga WM, EUGOGO †. The 2021 European Group on Graves' orbitopathy (EUGOGO) clinical practice guidelines for the medical management of Graves' orbitopathy. European journal of endocrinology. 2021 Aug 27:185(4):G43-G67. doi: 10.1530/EJE-21-0479. Epub 2021 Aug 27 [PubMed PMID: 34297684]
Level 1 (high-level) evidenceCheour M, Mazlout H, Agrebi S, Falfoul Y, Chakroun I, Lajmi H, Kraiem A. [Compressive optic neuropathy secondary to a pituitary macroadenoma]. Journal francais d'ophtalmologie. 2013 Jun:36(6):e101-4. doi: 10.1016/j.jfo.2012.08.014. Epub 2013 Apr 25 [PubMed PMID: 23623769]
Level 3 (low-level) evidenceJayaraman M, Gandhi RA, Ravi P, Sen P. Multifocal visual evoked potential in optic neuritis, ischemic optic neuropathy and compressive optic neuropathy. Indian journal of ophthalmology. 2014 Mar:62(3):299-304. doi: 10.4103/0301-4738.118452. Epub [PubMed PMID: 24088641]
Level 2 (mid-level) evidencePekic S, Stojanovic M, Popovic V. Pituitary tumors and the risk of other malignancies: is the relationship coincidental or causal? Endocrine oncology (Bristol, England). 2022 Jan:2(1):R1-R13. doi: 10.1530/EO-21-0033. Epub 2022 Dec 22 [PubMed PMID: 37435457]
Sebastian P, Balakrishnan R, Yadav B, John S. Outcome of radiotherapy for pituitary adenomas. Reports of practical oncology and radiotherapy : journal of Greatpoland Cancer Center in Poznan and Polish Society of Radiation Oncology. 2016 Sep-Oct:21(5):466-72. doi: 10.1016/j.rpor.2016.06.002. Epub 2016 Jul 15 [PubMed PMID: 27489518]
Längericht J, Krämer I, Kahaly GJ. Glucocorticoids in Graves' orbitopathy: mechanisms of action and clinical application. Therapeutic advances in endocrinology and metabolism. 2020:11():2042018820958335. doi: 10.1177/2042018820958335. Epub 2020 Dec 14 [PubMed PMID: 33403097]
Level 3 (low-level) evidenceKahaly GJ, Subramanian PS, Conrad E, Holt RJ, Smith TJ. Long-Term Efficacy of Teprotumumab in Thyroid Eye Disease: Follow-Up Outcomes in Three Clinical Trials. Thyroid : official journal of the American Thyroid Association. 2024 Jul:34(7):880-889. doi: 10.1089/thy.2023.0656. Epub 2024 Jun 2 [PubMed PMID: 38824618]
Chen Y, Zhong NN, Cao LM, Liu B, Bu LL. Surgical margins in head and neck squamous cell carcinoma: A narrative review. International journal of surgery (London, England). 2024 Jun 1:110(6):3680-3700. doi: 10.1097/JS9.0000000000001306. Epub 2024 Jun 1 [PubMed PMID: 38935830]
Level 3 (low-level) evidenceXu F, Wan C, Zhao L, Liu S, Hong J, Xiang Y, You Q, Zhou L, Li Z, Gong S, Zhu Y, Chen C, Zhang L, Gong Y, Li L, Li C, Zhang X, Guo C, Lai K, Huang C, Ting D, Lin H, Jin C. Predicting Post-Therapeutic Visual Acuity and OCT Images in Patients With Central Serous Chorioretinopathy by Artificial Intelligence. Frontiers in bioengineering and biotechnology. 2021:9():649221. doi: 10.3389/fbioe.2021.649221. Epub 2021 Nov 23 [PubMed PMID: 34888298]
Berardi R, Morgese F, Rinaldi S, Torniai M, Mentrasti G, Scortichini L, Giampieri R. Benefits and Limitations of a Multidisciplinary Approach in Cancer Patient Management. Cancer management and research. 2020:12():9363-9374. doi: 10.2147/CMAR.S220976. Epub 2020 Sep 30 [PubMed PMID: 33061625]
Yadav J, Gupta S, Venugopal AK, Ghosh A, Gupta IJ. 3D Conformal Radiotherapy Versus the Conventional Box Technique for Cervical Cancer: A Dosimetric Observational Study. Cureus. 2025 Aug:17(8):e89799. doi: 10.7759/cureus.89799. Epub 2025 Aug 11 [PubMed PMID: 40937215]
Level 2 (mid-level) evidenceSoltys SG, Milano MT, Xue J, Tomé WA, Yorke E, Sheehan J, Ding GX, Kirkpatrick JP, Ma L, Sahgal A, Solberg T, Adler J, Grimm J, El Naqa I. Stereotactic Radiosurgery for Vestibular Schwannomas: Tumor Control Probability Analyses and Recommended Reporting Standards. International journal of radiation oncology, biology, physics. 2021 May 1:110(1):100-111. doi: 10.1016/j.ijrobp.2020.11.019. Epub 2020 Dec 26 [PubMed PMID: 33375955]
Shusharina N, Söderberg J, Edmunds D, Löfman F, Shih H, Bortfeld T. Automated delineation of the clinical target volume using anatomically constrained 3D expansion of the gross tumor volume. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology. 2020 May:146():37-43. doi: 10.1016/j.radonc.2020.01.028. Epub 2020 Feb 27 [PubMed PMID: 32114264]
Parrilla C, Mele DA, Gelli S, Zelano L, Bussu F, Rigante M, Savino G, Scarano E. Multidisciplinary approach to orbital decompression. A review. Acta otorhinolaryngologica Italica : organo ufficiale della Societa italiana di otorinolaringologia e chirurgia cervico-facciale. 2021 Apr:41(Suppl. 1):S90-S101. doi: 10.14639/0392-100X-suppl.1-41-2021-09. Epub [PubMed PMID: 34060524]
Leitner I, Andrianakis A, Gellner V, Kiss P, Andrianakis D, Tomazic PV. Optic nerve injury in preoperative imaging is associated with visual improvement outcome in endoscopic optic nerve decompression. Wiener klinische Wochenschrift. 2022 Mar:134(5-6):185-194. doi: 10.1007/s00508-021-01915-x. Epub 2021 Aug 3 [PubMed PMID: 34342713]
Ataídes FG, Silva SFBR, Baldin JJCMC. Radiation-Induced Optic Neuropathy: Literature Review. Neuro-ophthalmology (Aeolus Press). 2021:45(3):172-180. doi: 10.1080/01658107.2020.1817946. Epub 2020 Nov 4 [PubMed PMID: 34194124]
Tang C, Liang L, Zheng X, Hu H, Liu C, Long J. Glucocorticoid therapy reduces ocular hypertension in active moderate-severe thyroid-associated orbitopathy. BMC endocrine disorders. 2022 Sep 23:22(1):235. doi: 10.1186/s12902-022-01153-w. Epub 2022 Sep 23 [PubMed PMID: 36151558]
Zeppieri M, Marsili S, Enaholo ES, Shuaibu AO, Uwagboe N, Salati C, Spadea L, Musa M. Optical Coherence Tomography (OCT): A Brief Look at the Uses and Technological Evolution of Ophthalmology. Medicina (Kaunas, Lithuania). 2023 Dec 3:59(12):. doi: 10.3390/medicina59122114. Epub 2023 Dec 3 [PubMed PMID: 38138217]
Lucy KA, Wollstein G. Structural and Functional Evaluations for the Early Detection of Glaucoma. Expert review of ophthalmology. 2016:11(5):367-376. doi: 10.1080/17469899.2016.1229599. Epub 2016 Sep 14 [PubMed PMID: 28603546]
Gala F. Magnetic resonance imaging of optic nerve. The Indian journal of radiology & imaging. 2015 Oct-Dec:25(4):421-38. doi: 10.4103/0971-3026.169462. Epub [PubMed PMID: 26752822]
Bekollari M, Dettoraki M, Stavrou V, Skouroliakou A, Liaparinos P. Investigating the Structural and Functional Changes in the Optic Nerve in Patients with Early Glaucoma Using the Optical Coherence Tomography (OCT) and RETeval System. Sensors (Basel, Switzerland). 2023 May 5:23(9):. doi: 10.3390/s23094504. Epub 2023 May 5 [PubMed PMID: 37177707]
Burch HB, Perros P, Bednarczuk T, Cooper DS, Dolman PJ, Leung AM, Mombaerts I, Salvi M, Stan MN. Management of thyroid eye disease: a Consensus Statement by the American Thyroid Association and the European Thyroid Association. European thyroid journal. 2022 Dec 1:11(6):. pii: e220189. doi: 10.1530/ETJ-22-0189. Epub 2022 Dec 8 [PubMed PMID: 36479875]
Level 3 (low-level) evidenceBulters DO, Shenouda E, Evans BT, Mathad N, Lang DA. Visual recovery following optic nerve decompression for chronic compressive neuropathy. Acta neurochirurgica. 2009 Apr:151(4):325-34. doi: 10.1007/s00701-009-0192-x. Epub 2009 Mar 3 [PubMed PMID: 19255716]
Level 2 (mid-level) evidenceCarlson AP, Stippler M, Myers O. Predictive factors for vision recovery after optic nerve decompression for chronic compressive neuropathy: systematic review and meta-analysis. Journal of neurological surgery. Part B, Skull base. 2013 Feb:74(1):20-38. doi: 10.1055/s-0032-1329624. Epub 2012 Nov 26 [PubMed PMID: 24436885]
Level 1 (high-level) evidencevan Nispen RM, Virgili G, Hoeben M, Langelaan M, Klevering J, Keunen JE, van Rens GH. Low vision rehabilitation for better quality of life in visually impaired adults. The Cochrane database of systematic reviews. 2020 Jan 27:1(1):CD006543. doi: 10.1002/14651858.CD006543.pub2. Epub 2020 Jan 27 [PubMed PMID: 31985055]
Level 1 (high-level) evidenceCheng Z, Xu F, Gao M, Bi Y, Jiang Y, Yuan L, Wu S, Luo C. Analysis of Prognostic Factors and Treatment Outcomes in Indirect Traumatic Optic Neuropathy: A Retrospective Review of 105 Patients. Current eye research. 2025 Feb:50(2):231-238. doi: 10.1080/02713683.2024.2404599. Epub 2024 Sep 23 [PubMed PMID: 39313934]
Level 2 (mid-level) evidenceCook C. Emergency management: optic nerve compression. Community eye health. 2018:31(103):62 [PubMed PMID: 30487682]
Guy J, Sherwood M, Day AL. Surgical treatment of progressive visual loss in traumatic optic neuropathy. Report of two cases. Journal of neurosurgery. 1989 May:70(5):799-801 [PubMed PMID: 2709121]
Level 3 (low-level) evidenceRaharja A, Whitefield L. Clinical approach to vision loss: a review for general physicians. Clinical medicine (London, England). 2022 Mar:22(2):95-99. doi: 10.7861/clinmed.2022-0057. Epub [PubMed PMID: 35304366]
Naumova L, Milevska-Vovchuk L, Burak A, Krytskyy T, Pankiv I. NEUROLOGICAL MANIFESTATIONS OF PROLACTINOMA (CASE REPORT). Georgian medical news. 2021 May:(314):116-120 [PubMed PMID: 34248039]
Level 3 (low-level) evidenceKinaci-Tas B, Alderliesten T, Verbraak FD, Rasch CRN. Radiation-Induced Retinopathy and Optic Neuropathy after Radiation Therapy for Brain, Head, and Neck Tumors: A Systematic Review. Cancers. 2023 Mar 27:15(7):. doi: 10.3390/cancers15071999. Epub 2023 Mar 27 [PubMed PMID: 37046660]
Level 1 (high-level) evidenceDemmin DL, Silverstein SM. Visual Impairment and Mental Health: Unmet Needs and Treatment Options. Clinical ophthalmology (Auckland, N.Z.). 2020:14():4229-4251. doi: 10.2147/OPTH.S258783. Epub 2020 Dec 3 [PubMed PMID: 33299297]
Alhujaili HO, Alanazi AM, Alshehri WM, Alghamdi RA, Alqasem AA, Alhumaid FI, AlGhamdi RA, Almaymuni KK. Adherence to Eye Examination Guidelines Among Individuals With Diabetes in Saudi Arabia. Cureus. 2024 Jan:16(1):e51472. doi: 10.7759/cureus.51472. Epub 2024 Jan 1 [PubMed PMID: 38298281]
Krahulik D, Blazek F, Hampl M, Hrabalek L, Krahulik J, Karhanova M. Visual outcomes in patients with meningiomas compressing optic nerve. Frontiers in neurology. 2025:16():1606661. doi: 10.3389/fneur.2025.1606661. Epub 2025 Jun 13 [PubMed PMID: 40584534]
Heiden BT, Eaton DB, Chang SH, Yan Y, Schoen MW, Thomas TS, Patel MR, Kreisel D, Nava RG, Meyers BF, Kozower BD, Puri V. Association between imaging surveillance frequency and outcomes following surgical treatment of early-stage lung cancer. Journal of the National Cancer Institute. 2023 Mar 9:115(3):303-310. doi: 10.1093/jnci/djac208. Epub [PubMed PMID: 36442509]
Kremenevski N, Schnell O, Coras R, Buchfelder M, Hore N. Clinical, surgical, and endocrine outcome following treatment of posterior pituitary tumors: a retrospective cohort study. Pituitary. 2025 Apr 5:28(2):45. doi: 10.1007/s11102-025-01518-z. Epub 2025 Apr 5 [PubMed PMID: 40186832]
Level 2 (mid-level) evidenceWhiteley AE, Price TT, Cantelli G, Sipkins DA. Leukaemia: a model metastatic disease. Nature reviews. Cancer. 2021 Jul:21(7):461-475. doi: 10.1038/s41568-021-00355-z. Epub 2021 May 5 [PubMed PMID: 33953370]
Stefko ST. Combined Surgical Approaches In and Around the Orbit. Journal of neurological surgery. Part B, Skull base. 2020 Aug:81(4):472-479. doi: 10.1055/s-0040-1713938. Epub 2020 Sep 4 [PubMed PMID: 33072487]
Senjam SS, Tandon R, Vashist P, Mounica B, Gupta V, Aggarwal S. Guidelines for setting up low-vision and rehabilitation services in India. Indian journal of ophthalmology. 2024 Nov 1:72(11):1580-1585. doi: 10.4103/IJO.IJO_2712_23. Epub 2024 May 20 [PubMed PMID: 38767534]
Karimi N, Kashkouli MB, Keyhani A, Aghili S, Ghahvehchian H, Askari S, Akbarian S. Mitigating the risks: addressing smoking cessation in thyroid eye disease. BMJ open ophthalmology. 2025 Aug 31:10(1):. doi: 10.1136/bmjophth-2025-002226. Epub 2025 Aug 31 [PubMed PMID: 40889896]
Wang MTM, Meyer JA, Danesh-Meyer HV. Neuro-ophthalmic evaluation and management of pituitary disease. Eye (London, England). 2024 Aug:38(12):2279-2288. doi: 10.1038/s41433-024-03187-x. Epub 2024 Jul 22 [PubMed PMID: 39039214]
Feroze KB, Gurnani B, O'Rourke MC. Transient Loss of Vision. StatPearls. 2025 Jan:(): [PubMed PMID: 28613595]
Peli E,Satgunam P, Bitemporal hemianopia; its unique binocular complexities and a novel remedy. Ophthalmic [PubMed PMID: 24588535]
Level 3 (low-level) evidenceFehlings MG, Hachem LD, Tetreault LA, Skelly AC, Dettori JR, Brodt ED, Stabler-Morris S, Redick BJ, Evaniew N, Martin AR, Davies B, Farahbakhsh F, Guest JD, Graves D, Korupolu R, McKenna SL, Kwon BK. Timing of Decompressive Surgery in Patients With Acute Spinal Cord Injury: Systematic Review Update. Global spine journal. 2024 Mar:14(3_suppl):38S-57S. doi: 10.1177/21925682231197404. Epub [PubMed PMID: 38526929]
Level 1 (high-level) evidenceWudie D, Nigussie H, Gelana T. Prevalence of eye diseases, refractive errors and visual impairments in the Debre Markos referral hospital. Scientific reports. 2025 Aug 30:15(1):31953. doi: 10.1038/s41598-025-04262-3. Epub 2025 Aug 30 [PubMed PMID: 40885790]
Gurnani B, Kaur K. Biosensor-embedded wearables for dry eye monitoring and management. Expert review of medical devices. 2025 Oct:22(10):1073-1079. doi: 10.1080/17434440.2025.2555485. Epub 2025 Sep 1 [PubMed PMID: 40884106]
Gurnani B, Kaur K. Response to letter regarding "Evaluating the novel role of ChatGPT-4 in addressing corneal ulcer queries: An AI-powered insight". European journal of ophthalmology. 2026 May:36(3):NP5-NP7. doi: 10.1177/11206721251357376. Epub 2025 Jul 9 [PubMed PMID: 40629931]
Level 3 (low-level) evidenceBalamurugan S, Kaur K, Gurnani B, Agrawal A. Bilateral acute vision loss as the initial presentation of chronic myeloid leukemia in a young female. Indian journal of cancer. 2023 Oct 1:60(4):578-582. doi: 10.4103/ijc.ijc_573_21. Epub 2024 Jan 9 [PubMed PMID: 38206079]
Hashmi MF, Gurnani B, Benson S. Conjunctivitis. StatPearls. 2025 Jan:(): [PubMed PMID: 31082078]
Xu TT, Kung FF, Lai KE, Ko MW, Brodsky MC, Bhatti MT, Chen JJ. Interprofessional Electronic Consultations for the Diagnosis and Management of Neuro-Ophthalmic Conditions. Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society. 2023 Mar 1:43(1):34-39. doi: 10.1097/WNO.0000000000001643. Epub 2022 Jul 8 [PubMed PMID: 36166791]
. The International Headache Congress - IHS and EHF joint congress 2021: late breaking abstracts : Virtual. 8-12 September 2021. The journal of headache and pain. 2021 Nov 18:22(Suppl 2):130. doi: 10.1186/s10194-021-01319-2. Epub 2021 Nov 18 [PubMed PMID: 34794375]
Tadesse YB, Sendekie AK, Mekonnen BA, Denberu FG, Kassaw AT. Pharmacists' Medication Counseling Practices and Knowledge and Satisfaction of Patients With an Outpatient Hospital Pharmacy Service. Inquiry : a journal of medical care organization, provision and financing. 2023 Jan-Dec:60():469580231219457. doi: 10.1177/00469580231219457. Epub [PubMed PMID: 38131171]
Stewart M, Brown JB, Donner A, McWhinney IR, Oates J, Weston WW, Jordan J. The impact of patient-centered care on outcomes. The Journal of family practice. 2000 Sep:49(9):796-804 [PubMed PMID: 11032203]
Level 2 (mid-level) evidence