Introduction
Normal pressure hydrocephalus (NPH) is a condition characterized by a symptomatic communicating hydrocephalus, with cerebrospinal fluid pressure often within the conventionally defined normal range. Idiopathic, or primary, NPH lacks an identifiable underlying cause. Idiopathic normal pressure hydrocephalus (iNPH), represented by the ICD-10 code of G91.2, is the most common form of hydrocephalus in adults and is a potentially reversible cause of dementia. Typically, iNPH primarily affects older adults and characteristically presents with progressive gait impairment, cognitive deficits, and urinary urgency or incontinence, a constellation known as the Hakim–Adams triad, first described by Colombian neurosurgeon Salomon Hakim and R D Adams in 1965.[1]
The presence of gait disturbance accompanied by 1 additional feature supports clinical suspicion of iNPH; however, confirmation requires further supportive evaluation through neuroimaging and cerebrospinal fluid drainage studies. Diagnostic reliance on symptoms alone remains insufficient due to variability in presentation and overlap with other neurologic disorders. Some experts have questioned the appropriateness of the term iNPH because intracranial pressure does not consistently remain normal across affected patients. As a result, the designation idiopathic adult hydrocephalus syndrome (iAHS) has been proposed as an alternative term.[2]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
NPH occurs in 2 recognized forms. Idiopathic, or primary, NPH lacks an identifiable underlying cause. Symptomatic, or secondary, NPH includes cases associated with prior brain infection, intracranial hemorrhage, traumatic brain injury, or exposure to radiation that contributes to the development of hydrocephalus. Both idiopathic and secondary forms represent communicating types of hydrocephalus and share a similar overall prognosis. A key distinction is the affected population: secondary NPH occurs across all age groups, whereas iNPH primarily affects older adults.
Best conceptualized as a disorder of aging, iNPH disease development reflects a convergence of age-related vulnerability and disrupted cerebrospinal fluid dynamics rather than a single focal lesion. Mean lumbar opening pressure commonly falls within the conventionally defined normal range; therefore, a single normal lumbar puncture does not exclude the diagnosis. Current consensus emphasizes impaired cerebrospinal fluid circulation and clearance combined with reduced intracranial compliance, rather than dependence on a sustained high-pressure phase.[3][4]
Epidemiology
The largest population-based study evaluating the prevalence of idiopathic normal pressure hydrocephalus in Western Sweden reported that 0.2% of individuals aged 70 to 79 years and 5.9% of those aged 80 years and older met guideline criteria for probable iNPH. Most identified patients exceeded 80 years of age.[5] The average age at symptom onset approximates 70 years, with equal distribution between men and women. Idiopathic normal pressure hydrocephalus accounts for an estimated 6% of all dementia cases.[6]
Furthermore, epidemiologic data estimate the incidence of NPH at 0.2 to 5.5 per 100,000 person-years. Reported prevalence rates range from 0.003% among individuals younger than 65 years to 0.2% to 2.9% among those aged 65 years or older.[7][8][9]
Pathophysiology
The condition of iNPH likely represents a final common pathway characterized by impaired cerebrospinal fluid circulation and clearance combined with reduced craniospinal compliance. These alterations promote ventriculomegaly and periventricular white matter injury through axonal stretch and ischemia within gait–frontal circuits, explaining the frequent emergence of gait disturbance as the earliest and most treatment-responsive symptom.[4][10]
A unifying conceptual model describes reduced cerebrospinal fluid clearance and altered pulsatility, which drive ventricular enlargement.[4] Periventricular tissue stress, accompanied by interstitial fluid accumulation, contributes to gait slowing and executive dysfunction.[10] Coexisting neurodegenerative pathology frequently limits cognitive recovery despite meaningful gait improvement following treatment.[11]
Although the precise pathophysiologic cascade remains incompletely defined, multiple mechanisms have been implicated in the development of NPH.[12][13][14][15][16] Proposed contributors include hyperdynamic cerebrospinal fluid flow through the aqueduct, reduced compliance of the subarachnoid space, increased cerebrospinal fluid pulse pressure, and impaired venous reabsorption secondary to elevated outflow resistance. Alternative reabsorption pathways, eg, transependymal flow rather than Pacchionian granulations, further disrupt normal cerebrospinal fluid dynamics.
Reductions in cerebral blood flow, along with altered expression of cerebrospinal fluid tumor necrosis factor-alpha and transforming growth factor-beta, influence cerebrospinal fluid production and regulation. Abnormalities in cerebrospinal fluid turnover impair clearance of vasoactive metabolites and neurotoxic proteins, including amyloid-β peptides and tau, creating an environment hostile to neuronal function and survival, as described by Silverberg in 2004. Loss of the Windkessel effect within skull base arteries reflects increased resistance to cerebrospinal fluid outflow rather than overproduction. Vascular stiffening from atherosclerosis or reduced craniospinal compliance limits arterial expansion, increasing brain pulsatility and generating compressive and shearing forces within the cerebral parenchyma.
Structural and physiological differences between superficial and deep periventricular tissues predispose these regions to early damage through cerebral autocompression, resulting in ventriculomegaly. Concurrent reductions in cerebral blood flow further decrease cerebrospinal fluid turnover, linking iNPH with cerebral hypoperfusion. Emerging evidence from Mendelian randomization analyses suggests associations between iNPH risk and gut microbiota, including the class Melainabacteria and the genetically predicted abundance of the genus Adlercreutzia, highlighting potential metabolic, preventive, and therapeutic implications.[17][18][19][20][21][22][23]
Gait Abnormality Etiologies
Gait abnormalities arise from stretching and compression of corticospinal tract fibers within the corona radiata supplying the lower extremities, which course adjacent to the lateral ventricles and become vulnerable to interstitial edema. Additional contributors include reduced perfusion of periventricular white matter and prefrontal regions, as well as compression of brainstem structures, eg, the pedunculopontine nucleus.
Dementia and Bladder Incontinence Etiologies
Progressive ventricular enlargement generates radial shearing forces as the cerebral cortex abuts the inner table of the calvarium, leading to cognitive decline and dementia. Bladder dysfunction initially results from stretching of periventricular sacral corticospinal fibers, producing loss of supraspinal inhibition of detrusor contractions, as described by Gleason in 1993. In later disease stages, cognitive impairment further contributes to urinary incontinence, as noted by Corkill in 1999.
Assessment of iNPH requires careful consideration of comorbid conditions in accordance with guidance from the International Society for Hydrocephalus and Cerebrospinal Fluid Disorders.[24][25] Systematic identification and management of coexisting pathologies enable the optimization of individualized care plans and the maximization of clinical outcomes.[26][27]
Histopathology
Although iNPH has no single pathognomonic lesion, the periventricular region shows a reproducible injury pattern across hydrocephalus states: disruption of the ependymal lining with periventricular edema, followed by axonal injury, secondary myelin disruption, and reactive astrocytosis or gliosis. These changes support the clinical emphasis on early diagnosis, as advanced white matter injury may become less reversible.[28]
In vivo imaging-pathology correlates also support white matter damage consistent with axonal loss and gliosis in anterior frontal pathways, which map to gait planning and initiation. This provides a mechanistic bridge for why gait often improves after cerebrospinal fluid drainage, while cognitive recovery can be incomplete.[29]
Given the high frequency of concomitant Alzheimer-type pathology in cortical biopsies taken at shunt surgery, histopathology also informs prognosis. Alzheimer disease neuropathologic change is common and should be considered when counseling about cognitive recovery.[11]
History and Physical
The classic clinical syndrome of iNPH includes gait impairment, cognitive dysfunction that often follows a frontal–subcortical or executive pattern, and urinary urgency or incontinence. Many patients demonstrate an incomplete presentation, with gait disturbance accompanied by at least 1 additional domain, frequently representing the earliest diagnostic pattern.
Diagnostic Frameworks
Contemporary diagnostic frameworks clinically categorize iNPH as possible, probable, or definite, emphasizing it as a clinicoradiologic diagnosis. Possible iNPH may be considered in patients older than 60 years who exhibit at least 2 components of the classic triad, whose symptoms lack a more plausible neurologic or systemic explanation, and whose ventriculomegaly lacks a clear antecedent cause, eg, meningitis or head trauma.
Probable iNPH requires fulfillment of criteria for possible disease, a lumbar cerebrospinal fluid opening pressure of 200 mm H2O or less with otherwise normal cerebrospinal fluid studies, and either supportive neuroimaging consistent with disproportionately enlarged subarachnoid space hydrocephalus with characteristic gait impairment or demonstrable clinical improvement following cerebrospinal fluid removal through a tap test or drainage trial. Demonstrated improvement after shunt placement establishes the diagnosis as definite iNPH.[3] Given the high prevalence of comorbid conditions that may limit response in specific symptom domains, evaluation and counseling require systematic assessment for concurrent neurodegenerative disease, vascular burden, and Parkinsonism.
Gait Disturbance
Gait disturbance commonly represents the earliest and most frequent presenting symptom and often shows the most rapid postoperative improvement.[27] Reports associate gait abnormality preceding cognitive decline with a more favorable prognosis following shunt placement.[30] Typical gait descriptors include shuffling, magnetic, and wide-based patterns, accompanied by increased mediolateral variability during quiet standing.[31] Progressive disease leads to further gait deterioration characterized by slow speed, short steps, broad-based stance, and a glue-footed or astasia–abasia pattern.
Additional features include:
- External rotation in foot posture
- Poor foot clearance (festination, shuffling, tripping)
- Notable difficulty turning on the body’s long axis (multistep turns)
- Gait initiation failure or freezing of gait
Postural instability in NPH worsens with eye closure, although patients often require a widened stance even with eyes open. Upper body posture appears mildly stooped, with retropulsion occurring spontaneously or during provocation. Upper limb motor abnormalities remain mild or absent and generally reflect bradykinesia. Shunt surgery frequently improves gait velocity and limb movement, whereas extremity tremor, present in approximately 40% of patients, shows minimal response to shunting. Gait severity assessment benefits from combining subjective grading using the iNPH grading scale with objective quantitative measures, eg, the Timed Up and Go test and short-distance straight walking tests, to support baseline evaluation and postintervention comparisons.
Urinary Symptoms and Dementia
Urinary symptoms arise primarily from detrusor overactivity, producing urinary frequency, urgency, or frank incontinence. Cognitive impairment in iNPH reflects a subcortical dementia pattern characterized by inertia, forgetfulness, and impaired executive function.[27] Early cognitive manifestations include psychomotor slowing, reduced attention, and executive and visuospatial dysfunction resulting from frontal and subcortical involvement.
Apathy frequently accompanies cognitive decline. Shunt placement may yield meaningful improvement across these cognitive features, although multiple vascular risk factors worsen cognitive severity. Despite radiologic evidence of advanced hydrocephalus, clinicians often defer surgical intervention in patients with severe dementia, even when gait dysfunction and urinary incontinence coexist.
Objective cognitive evaluation requires formal psychometric testing to assess subcortical frontal lobe dysfunction. Commonly used instruments include the grooved pegboard test, Stroop test, digit span test, trail-making A and B tests, and the Rey auditory verbal learning test.
Idiopathic Normal Pressure Hydrocephalus Grading Scale
Symptom severity across gait, cognition, and urinary domains can be systematically quantified using the iNPH grading scale, which provides a structured framework for baseline assessment and longitudinal monitoring (see Table 1).[3] The iNPH grading scale is a clinician-rated symptom severity scale scored 0 to 4 in each domain (cognition, gait, urinary), based on clinical observation and patient or caregiver report. Higher scores reflect greater impairment.
Table 1. Idiopathic Normal Pressure Hydrocephalus Grading Scale
| Grade | Gait | Cognition | Urinary incontinence |
| 0 | Normal | Within normal range | Absent |
| 1 | Unsteadiness without objective abnormality | No clear dementia, but apathy present | Frequency and or urgency without incontinence |
| 2 | Needs a cane | Needs support in social functioning, but remains independent at home | Occasional episodes at night |
| 3 | Needs 2 canes or a walker | Requires partial assistance at home | Intermittent episodes during the daytime |
| 4 | Unable to ambulate | Fully dependent | Frequent urinary incontinence |
Evaluation
Evaluation Overview
The evaluation of suspected iNPH follows a structured 3-step process that integrates clinical, functional, and prognostic information.
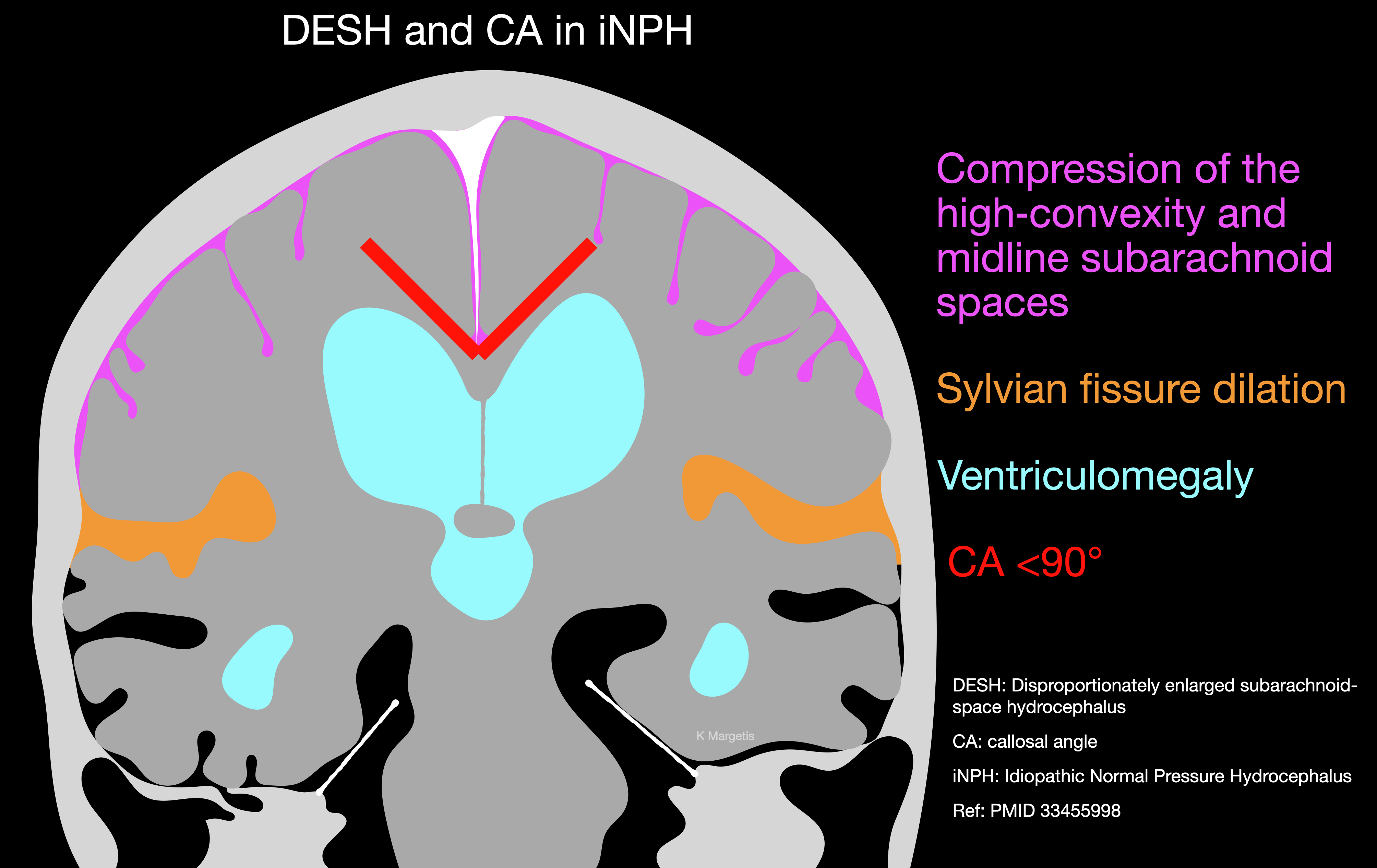
The first step focuses on establishing convergent clinical and imaging evidence. Diagnosis depends on concordant findings from the clinical history, neurologic examination, and neuroimaging rather than reliance on any single test.[3][32] Disproportionately enlarged subarachnoid space hydrocephalus, characterized by ventriculomegaly, enlargement of the Sylvian fissures, and compression of the high-convexity and midline subarachnoid spaces, represents a specific imaging phenotype of iNPH with strong positive but weak negative predictive value. Steepening of the callosal angle serves as an indirect marker of this morphologic pattern and contributes to diagnostic confidence as well as the prediction of shunt responsiveness (see Image. Normal Pressure Hydrocephalus).[3]
The second step involves a structured evaluation of baseline function. Objective gait metrics, including the Timed Up and Go test, gait speed, and number of steps required to turn, should be recorded alongside a brief cognitive assessment emphasizing executive function. Pairing these measures with the iNPH grading scale supports longitudinal symptom tracking and assessment of treatment response.
The third step uses cerebrospinal fluid removal or drainage tests to enrich prognostic information. The lumbar tap test remains the most commonly used method. External lumbar drainage may be considered when tap test results remain equivocal and clinical suspicion persists.
Diagnostic Imaging
Computed tomography
Computed tomography (CT) contributes to the visualization of anatomic brain changes but lacks sufficient specificity for diagnosis when used in isolation (see Images. Normal Pressure Hydrocephalus Imaging and Normal Pressure Hydrocephalus CT). To improve inter-reader consistency and communication among neurology, radiology, and neurosurgery, structured CT assessment offers advantages over narrative description alone. When available, the iNPH Radscale provides a standardized framework for CT interpretation by quantifying key imaging features associated with iNPH. Structured scoring improves reproducibility across centers and enhances clarity during interprofessional decision-making regarding further testing or shunt candidacy.[33] The Radscale was developed as a screening and communication tool rather than a stand-alone diagnostic test and summarizes multiple morphologic signs into a single reproducible score correlated with clinical symptom burden. Validation was performed using noncontrast head CT, although magnetic resonance imaging (MRI) may provide superior characterization of selected features.
The iNPH Radscale integrates 7 imaging features into a composite score ranging from 0 to 12. Evans’ index assigns a score of 0 to values of 0.25 or less, 1 to values between 0.25 and 0.30, and 2 to values greater than 0.30. Narrowing of the high-convexity or parasagittal sulci receives a score of 0 when absent, 1 when parafalcine, and 2 when extending to the vertex. Sylvian fissures receive a score of 0 when normal and 1 when enlarged. Focally enlarged sulci receive a score of 0 when absent and 1 when present. Temporal horn width receives a score of 0 for measurements less than 4 mm, a score of 1 for measurements between 4 and 6 mm, and a score of 2 for widths measuring 6 mm or larger. The callosal angle receives a score of 0 when the angle is greater than 90 degrees, a score of 1 when the angle is between 90 degrees and 60 degrees, and a score of 2 when the angle is 60 degrees or less. Periventricular hypodensities receive a score of 0 when absent, 1 when limited to frontal horn caps, and 2 when confluent. Higher total scores indicate a greater burden of imaging features consistent with iNPH.
Magnetic resonance imaging
Magnetic resonance imaging (MRI) plays a central role in the evaluation of suspected iNPH by documenting ventriculomegaly and characteristic morphologic features that support diagnosis within the appropriate clinical context (see Images. Normal Pressure Hydrocephalus MRI and Imaging Hallmarks of Idiopathic Normal Pressure Hydrocephalus). MRI findings suggestive of NPH include:
- Evans index: An Evans index is defined as the maximal frontal horn width divided by the transverse inner skull diameter, with values 0.30 or greater supporting ventricular enlargement, although values of 0.30 or less do not exclude iNPH.
- Callosal angle: The callosal angle typically ranges from 40 to 90 degrees in affected patients.
- Size of temporal horns: Disproportionate ventricular enlargement relative to cortical sulci, dilation of temporal horns not fully attributable to hippocampal atrophy, and preserved fourth ventricle size despite lateral and third ventricular enlargement support the diagnosis and do not imply aqueductal stenosis.
- Narrow high-convexity sulci: Coronal imaging at the level of the posterior commissure often demonstrates narrowed high-convexity subarachnoid spaces and constricted medial cisterns, producing a tight convexity appearance. Additional features include dilated Sylvian fissures and focally enlarged sulci consistent with disproportionately enlarged subarachnoid space hydrocephalus.[34]
- Dilated Sylvian fissures: The disproportionately enlarged subarachnoid space hydrocephalus (DESH) sign demonstrates a positive predictive value of 77% and a negative predictive value of 25%.
- Quantitative DESH uses volumetric analysis of T1-weighted MRI images to calculate cerebrospinal fluid volume ratios between the Sylvian fissures and the high convexities, using semi-automated segmentation and manual outlining.[35]
- The MRI-based DESH score aggregates 5 radiologic features, each rated from 0 to 2, for a maximum score of 10. Included features encompass ventriculomegaly, dilated Sylvian fissures, tight high-convexity sulci, acute callosal angle, and focal sulcal dilation.
- Higher scores correlate with a greater likelihood of postoperative improvement, greater symptom severity, and alterations in white matter tracts on diffusion tensor imaging.[36]
- Periventricular hypodensities: Periventricular hypodensities on CT or T2/fluid-attenuated inversion recovery hyperintensities on MRI reflect transependymal edema related to elevated cerebrospinal fluid pressure, although similar findings may occur in small vessel ischemic disease. Upward bowing and stretching of the corpus callosum indicate bulging of the lateral ventricular roof.
Advanced magnetic resonance imaging techniques
Advanced MRI techniques provide supportive but nonessential information and should not replace clinical assessment and standard imaging. Arterial spin-labeling MRI demonstrates reduced cerebral blood flow in the thalamus, basal ganglia, and periventricular white matter compared with healthy controls.[37] Diffusion tensor imaging reveals reduced fractional anisotropy and increased mean diffusivity within periventricular regions, particularly the corpus callosum and corona radiata, suggesting demyelination or axonal injury.[38] Diffusion tensor imaging analysis along the perivascular space offers a promising noninvasive method for assessing glymphatic system function and may serve as a prognostic biomarker for preoperative evaluation.[39]
Magnetic resonance elastography demonstrates increased stiffness in the parietal, occipital, and sensorimotor cortices, with relative softening near the periventricular white matter, producing a concentric stiffness gradient. Decreased damping ratio predominates within the superior white matter. These findings remain adjunctive and lack utility as stand-alone diagnostic criteria.[40][41] Glymphatic MRI using gadobutrol contrast demonstrates delayed tracer distribution within subarachnoid spaces and ventricles, along with increased parenchymal uptake in regions, eg, the frontal horn and inferior frontal gyrus, reflecting impaired cerebrospinal fluid clearance.[42]
Machine Learning and Artificial Intelligence
Machine learning and artificial intelligence approaches analyze cerebrospinal fluid and ventricular segmentation, volumetric data extraction, and classification using automated algorithms. Recent frameworks include assessment of maximum eccentricity of the lateral ventricles, which improves CT-based screening accuracy for iNPH.[43]
Cerebrospinal fluid flow studies report flow rates >24.5 mL/min as 95% specific for normal-pressure hydrocephalus.[44] Aqueductal flow voids on T2-weighted imaging lack diagnostic utility.[45]
Several factors are associated with favorable shunt outcomes, including an aqueductal stroke volume greater than 42 µL, absence of white matter lesions on MRI, B-waves occupying greater than 50% of the intracranial pressure monitoring time, and cerebrospinal fluid outflow resistance exceeding 18 mm Hg. Factors associated with unfavorable outcomes include:
- Severe dementia
- Dementia as a presenting symptom
- MRI abnormalities, cerebral atrophy, and multiple white matter lesions
- Misdiagnosis and delayed recognition
- Hypertension
- Longer disease duration
- Severe urinary dysfunction
- Lower Evans’ index [46]
Nuclear Medicine Studies
Nuclear medicine studies demonstrate nonspecific findings, eg, heart-shaped lateral ventricles, prolonged tracer persistence within the ventricular system beyond 24 to 48 hours, absence of tracer extension over the superior lateral ventricles, and cerebrospinal fluid backflow into the lateral ventricles. Fludeoxyglucose positron emission tomography shows promise for identifying NPH and coexisting neurodegenerative disease, with a characteristic pattern of bilateral dorsal striatal hypometabolism and relative cortical preservation.[47][48][47] Dopamine transporter single-photon emission computed tomography demonstrates reduced striatal binding, potentially reflecting dopaminergic degeneration or secondary cerebrospinal fluid effects. Although useful for differentiating iNPHs from Parkinsonian syndromes, predictive value for shunt responsiveness remains limited.
Invasive Diagnostic Studies
Invasive diagnostic testing includes a large-volume lumbar puncture to assess clinical improvement, particularly in gait. A single tap test remains standard practice, with repeat testing reserved for equivocal responses. Observed improvement in gait quality and safety defines a positive response, supported by objective measures. A reduction of approximately 5 seconds on the Timed Up and Go test supports responsiveness, although clinical judgment predominates.[49] Probable iNPH criteria include a cerebrospinal fluid opening pressure ≤200 mm H2O, while higher values prompt exclusion of alternative diagnoses rather than automatic exclusion of iNPH.
Cerebrospinal Fluid Flow Study
Cerebrospinal fluid drainage tests increase diagnostic and prognostic accuracy beyond 80%. The spinal tap test typically involves removal of 30 to 50 mL of cerebrospinal fluid, followed by baseline and postprocedure assessment using both subjective and quantitative measures at 2 to 4 hours and again the following day, with delayed reassessment up to 1 week when appropriate. Negative results do not exclude iNPH, particularly in patients with prolonged symptom duration or compelling clinical and imaging features.
Continuous lumbar drainage involves removing 150 to 200 mL of cerebrospinal fluid daily for 2 to 7 days and demonstrates a sensitivity of 50% to 100%, with a positive predictive value of 80% to 100%. Evidence regarding superiority over the tap test remains mixed. The lumbar infusion test evaluates resistance to cerebrospinal fluid outflow through controlled infusion of 10 to 30 mL of isotonic saline with continuous pressure monitoring. Elevated resistance supports impaired cerebrospinal fluid absorption. Experienced clinicians should conduct all pre- and post-drainage evaluations.
Biomarkers
Cerebrospinal fluid biomarkers in iNPH include elevated levels of monocyte chemoattractant protein-1, interleukin-6, and vascular endothelial growth factor, reflecting chronic, low-grade neuroinflammation and altered cerebrospinal fluid dynamics. Additional markers, eg, aquaporin-4 and neurofilament light chain, suggest disrupted water transport and axonal injury.[37] A biomarker profile demonstrating low Aβ42 with normal tau supports iNPH over Alzheimer disease. Biomarkers alone demonstrate limited predictive value for shunt responsiveness.[50]
Asymptomatic Ventriculomegaly
Asymptomatic ventriculomegaly with iNPH MRI features has been described in older adults and carries a meaningful risk of progression to symptomatic disease. Selected individuals may benefit from education and periodic clinical surveillance.
Treatment / Management
Shunt surgery is the primary disease-modifying treatment for iNPH. Ventriculoperitoneal shunting (VPS) diverts cerebrospinal fluid from a ventricular catheter through a valve into the peritoneal cavity, reducing ventricular size and periventricular stress over time (decompresses vulnerable frontal-subcortical pathways).[3] VPS remains the most widely used approach and should be considered when ventricular access is straightforward and long-term adjustability via programmable valves is desired. However, a lumboperitoneal shunt is a validated alternative, supported by randomized trial evidence and commonly used in some regions. This type of shunt avoids intracranial catheter placement but requires attention to spinal anatomy and the risk of overdrainage.[51] (A1)
Selection between ventriculoperitoneal and lumboperitoneal shunting in clinical practice should reflect patient-specific and procedural factors, including anatomic considerations, surgeon experience, history of prior abdominal surgery, presence of spinal stenosis or spinal deformity, and anticipated need for ventricular catheter access for future monitoring. Comparative prospective data demonstrate effectiveness for both approaches, although each carries a distinct complication profile.[52]
Endoscopic third ventriculostomy does not represent routine therapy for classic iNPH due to insufficient supporting evidence and should remain limited to obstructive hydrocephalus phenotypes or carefully selected cases.[53] Use of programmable valves is preferred, as adjustable opening pressures allow titration according to symptom response and imaging findings, particularly in older adults with variable tolerance to cerebrospinal fluid drainage. When available, the addition of a gravitational unit or antisiphon device may further reduce the risk of upright overdrainage.[54] A pragmatic management approach begins with a higher opening pressure followed by stepwise reduction guided by gait improvement and imaging changes, minimizing the risk of subdural effusions and overdrainage-related symptoms.[55](A1)
Long-term care of patients treated with shunting should include scheduled clinical follow-up with gait-based metrics and, ideally, a quantifiable metric (eg, iNPH grading scale). The valve should be reprogrammed when symptoms persist or recur, or when overdrainage symptoms occur. Follow-up imaging is indicated when neurologic status changes, and early after major pressure adjustments to screen for subdural collections. The risk for shunt revision should be explained, as well as the signs of shunt malfunction. The complications usually cluster in the first postoperative year and then decline.[56][56]
A CSF shunt procedure using a programmable-pressure valve is medically and economically effective in treating iNPH.
Trials Related to Idiopathic Normal Pressure Hydrocephalus
Study of Idiopathic Normal Pressure Hydrocephalus on Neurological Improvement
Specific features in the MRI brain that suggest features of iNPH, as identified in the Study of Idiopathic Normal Pressure Hydrocephalus on Neurological Improvement (SINPHONI-1) (2010), included:
- Tight high convexity and medial subarachnoid spaces with ventriculomegaly
- DESH [34]
Patients having these features showed high responsiveness to ventriculoperitoneal shunt surgery. However, in the SINPHONI-2 (2015) trial, the findings favored lumboperitoneal shunt surgery in patients with iNPH. But the study suggested that larger studies are needed to consider the lumboperitoneal shunt as a first-line treatment for iNPH.[51](A1)
Shunt Valves plus shunt Assistant versus Shunt valves alone for controlling Overdrainage in idiopathic Normal pressure hydrocephalus in Adults
The Shunt Valves plus shunt Assistant versus Shunt valves alone for controlling Overdrainage in idiopathic Normal pressure hydrocephalus in Adults (SVASONA)(2013) study favored the use of the gravitational valve in patients undergoing VPS for iNPH. Implanting such valves rather than other types will avoid an additional over-drainage complication in about one-third of patients.[54](A1)
Clinical Effectiveness of Different Shunt Valve Settings
A double-blind, randomized trial on the clinical effectiveness of different shunt valve settings in idiopathic normal pressure hydrocephalus (2016) concluded the following:
- No difference in outcome was noted when the valve pressure was gradually reduced from 20 to 4 cm H2O or set at a fixed value of 12 cm H2O.
- Irrespective of the valve pressure setting, improvement after VPS was evident only within 3 months.[57] (A1)
SYGRAVA 2018
A study protocol for a randomized trial investigating the efficacy and safety of programmable versus fixed antisiphon devices for treating iNPH in adults is the first randomized trial to compare drainage-related complication rates between programmable and fixed antisiphon devices in patients with iNPH. This is an ongoing trial.[58](A1)
Dutch Evaluation Programme Strata Shunt Trial (2013)
A randomized trial of high and low-pressure level settings on an adjustable ventriculoperitoneal shunt valve for iNPH results of the Dutch evaluation programme Strata shunt (DEPSS) trial noted the following findings:
- To treat iNPH, a programmable shunt preset at a high opening pressure is better.
- The initial high pressure should be lowered until clinical improvement occurs or radiological features of shunt over-drainage occur.[55] (A1)
Dual-Center Trial
A randomized controlled dual-center trial on shunt complications in iNPH treated with gradually reduced or "fixed" pressure valve settings (2014) demonstrated no difference in the shunt- or overdrainage-related complications if the valve pressure was gradually lowered to a mean of 7 cm H2O and a fixed valve setting at a mean of 13 cm H2O, but the former one was associated with a significantly better outcome.
Dutch Normal-Pressure Hydrocephalus Study (1998)
A randomized comparison of low- and medium-pressure shunts demonstrated that a low-pressure valve shunt was associated with a better outcome than a medium-pressure shunt, although most differences were not statistically significant. The study concluded that iNPH treatment is better with a low-pressure valve shunt.[59](A1)
Endoscopic Third Ventriculostomy
Only 1 randomized trial comparing endoscopic third ventriculostomy with VPS using a nonprogrammable valve for iNPH has been conducted. However, the evidence from this study was inconclusive. Clinicians should be aware of the limitations of the evidence.[53] Recently suggested neurosurgical practice guidelines for determining whether or not to shunt a patient with iNPH include the following:(A1)
- If the CSF opening pressure is high, it should prompt an investigation to identify a secondary cause of NPH.
- If a good clinical response is noted after a 40- to 50-mL (high-volume) lumbar tap, it suggests a potential benefit from VPS.
- If the patient does not respond to a high-volume tap, extended lumbar drainage may be an option for further evaluation.
- No substantial predictive value for MRI cerebrospinal flow studies has been established.[60]
A recent survey among neurosurgeons in Japan revealed that the following factors were considered unfavorable for performing a VPS:
- Age of 90 years or older
- Comorbid Alzheimer disease and schizophrenia
- Absence of DESH
- Patients were not receiving appropriate care or were institutionalized.[61] (B3)
The standard treatment of iNPH is the implantation of a ventriculoperitoneal shunt with an adjustable valve. Lumboperitoneal shunts have also been widely used. Endoscopic third ventriculostomy is used only in those cases with a locally confined, infratentorial, extraventricular obstruction to CSF flow. Such an obstruction is usually characterized by a protrusion of the lamina terminalis and the floor of the third ventricle into the adjacent basal cisterns.
The negative predictors for endoscopic third ventriculostomy success in iNPH have been proposed to be as follows:
- Cognitive regression is the dominant symptom
- Long duration of symptoms
- Severe symptoms (high Kiefer score)
- Age older than 65 years
- Absence of third ventricle floor pulsations
- Pathological Rout in both lumbar and ventricular compartments
- Low peak systolic aqueductal CSF flow on phase-contrast MRI (<5 cm/s) [62] (A1)
Carbonic anhydrase inhibitors and serial drainage lumbar punctures have a role only in nonsurgical candidates.
Differential Diagnosis
Clinical features that are atypical for iNPH and should prompt consideration of alternate or additional diagnoses (see Table 2),[37] including:
- Early prominent tremor, rigidity, or marked resting tremor (suggests Parkinsonism spectrum)
- Early visual hallucinations or REM sleep behavior disorder (suggests Lewy body disease spectrum)
- Early aphasia, apraxia, or cortical sensory loss (suggests cortical degenerative syndromes)
- Early focal motor weakness or sensory level (consider stroke, myelopathy)
- Severe headache with papilledema (consider raised ICP syndromes)
- Rapid progression over weeks to months (consider secondary causes or alternative diagnoses)
The differential diagnosis is extensive and includes the following conditions:
- Cortical dementias
- Alzheimer disease
- Frontotemporal dementia [63]
- Subcortical dementias
- Lewy-body dementia
- Parkinson disease and vascular Parkinsonism
- Progressive supranuclear palsy
- Corticobasal degeneration
- AIDS dementia complex
- Age-related depression
- Mixed dementias
- Vascular dementia
Table 2. Differentiating Normal Pressure Hydrocephalus From Other Neurodegenerative Disorders
|
Feature |
iNPH |
Alzheimer Disease |
Parkinson Disease |
Progressive Supranuclear Palsy |
Vascular Dementia |
|
Evans’ Index |
>0.3 (increased ventricles) |
Normal or mildly increased |
Normal |
Normal or mild increase |
Variable (can be increased) |
|
Callosal Angle |
Narrow <90 degrees |
Wide >100 degrees |
Wide |
Often narrow but less than iNPH |
Variable |
|
DESH Pattern |
Present |
Absent |
Absent |
Absent |
Absent |
|
Temporal Horns |
Disproportionately enlarged |
Medial temporal atrophy |
Normal |
Normal |
Normal or mild atrophy |
|
Periventricular Hyperintensities |
Common (transependymal flow) |
Rare or mild |
Rare |
Mild |
Common (ischemic origin) |
|
Hippocampal Atrophy |
Absent or mild |
Marked |
Mild |
Mild |
Mild/moderate |
|
FDG-PET Hypometabolism |
Frontal-dominant; improves post-shunt |
Parietotemporal, posterior cingulate |
Mild; basal ganglia |
Midbrain/hypometabolism |
Patchy, subcortical |
|
DAT-SPECT |
Usually normal or mild decrease |
Normal |
Decrease in the striatum |
Decrease in caudate + putamen |
Normal or mild decrease |
|
DTI |
Decreased fractional anisotropy in the corona radiata, internal capsule |
Decreased fractional anisotropy in temporal-parietal tracts |
Mild changes |
Decreased fractional anisotropy in the superior cerebellar peduncle |
Patchy changes |
|
ASL Perfusion MRI |
Decreased cerebral blood flow (CBF) in periventricular white matter, thalamus |
↓ in parietotemporal regions |
Normal |
Midbrain decreased |
Patchy decreased in subcortical areas |
|
Glymphatic MRI |
Delayed tracer clearance, reflux |
Normal or globally reduced |
Normal |
Not well studied |
Normal or mild changes |
|
CSF Aβ42 & tau |
Normal or mildly altered |
Decreased Aβ42, Increased tau |
Normal |
Mildly altered |
Mild alterations |
|
NfL |
Mild increase |
High increase |
Mild increase |
Increased |
Increased |
|
MCP-1, IL-6, IL-1β, VEGF |
Increased |
Usually normal |
Normal |
Not elevated |
Mild increase |
|
Clinical Gait |
Early, broad-based, magnetic |
Late onset |
Shuffling, festinating |
Early, postural instability |
Variable |
|
Cognitive Features |
Subcortical (attention, executive) |
Cortical (memory, language) |
Mild executive dysfunction |
Frontal-executive + gaze palsy |
Variable |
Prognosis
Most treated patients improve with shunting, with gait showing the highest probability and the earliest timing of benefit.[64] Cognitive and urinary outcomes are more variable and are strongly influenced by comorbid neurodegenerative disease burden.[32][3]
Predictors favoring cognitive recovery include:
-
Milder baseline cognitive impairment and shorter duration of cognitive symptoms
-
Clear executive dysfunction pattern rather than dominant amnestic dementia phenotype
-
Absence of strong evidence of comorbid Alzheimer pathology on biopsy or biomarker evaluation [65]
Predictors of limited cognitive recovery include:
-
Strong evidence of comorbid Alzheimer pathology
-
Advanced baseline dementia with loss of independence
-
Long symptom duration with severe imaging burden consistent with irreversible white matter injury [66]
Preoperative and postoperative shunt surgery outcomes are measurable with the following validated scales: the NPH Japanese Scale (NPH Scale), the Berg Balance Scale, the Dynamic Gait Index (DGI), the Functional Independence Measure (FIM), the Mini-Mental Status Examination (MMSE), and the Timed Up and Go (TUG).
Complications
Without treatment, patients often develop progressive gait impairment with falls, loss of independence, and complications of immobility. Urinary dysfunction increases the risk of incontinence-associated dermatitis and urinary tract infections. Cognitive decline can progress to dementia-level functional dependence.
Common significant complications include:
- Subdural hygroma or hematoma from overdrainage
- Shunt malfunction or obstruction with symptom recurrence
- Infection
- Overdrainage syndrome with orthostatic headache, nausea, or slit ventricles [64]
In a large iNPH registry, risk factors for subdural hematoma included male sex, antiplatelet therapy, and lower opening pressure at surgery. This supports choosing programmable valves and avoiding overly aggressive initial settings in higher-risk patients.[67]
Postoperative and Rehabilitation Care
Patients with programmable valves typically require gradual stepwise adjustments over weeks to months, guided by gait response, cognitive trajectory, urinary symptoms, and imaging signs of overdrainage or underdrainage. Starting higher and titrating down can reduce subdural effusions.[55]
Recommended follow-up elements include:
-
Early postoperative clinical review for delirium, infection, and wound status
-
Baseline postoperative CT or MRI if symptoms worsen or if there is concern for overdrainage
-
Repeat imaging after major valve setting changes or new headaches, confusion, or focal deficits
-
Physical therapy focused on gait initiation, turning, and balance.
Deterrence and Patient Education
The clinician should inform the patient that the following are the chances of improvement of symptoms following shunt surgery:
- Gait impairment: 85%
- Bladder disturbance: 80% in the early stage and 50% to 60% in the late stage
- Cognitive deficits: 80% [63]
In the postoperative phase, the patients and the caregivers should be educated about the early recognition of potential complications of delirium, infection, surgical wound issues, overdrainage, and subdural hematomas. Specifically, patients should seek medical advice if they have any wound-healing issues, fever, new headaches, confusion, or focal deficits.
Pearls and Other Issues
Do not use DESH as a single gatekeeper. DESH supports the diagnosis and often predicts shunt responsiveness, but iNPH should not be judged solely by DESH, as non-DESH imaging has limited negative predictive value.
A negative tap test does not exclude iNPH. Tap test performance is imperfect; delayed improvement can occur, and clinical/imaging context matters. Evans index is helpful but not absolute. If the Evans index is not greater than 0.3, yet suspicion is high, evaluate other supportive ventricular indices (eg, inferior horn enlargement, callosal angle of less than 90 degrees).
Enhancing Healthcare Team Outcomes
Idiopathic normal pressure hydrocephalus represents a potentially reversible cause of gait disturbance, cognitive dysfunction, and urinary symptoms in older adults. Diagnosis relies on integration of clinical features with neuroimaging findings such as ventriculomegaly, DESH, and callosal angle changes, supported by prognostic cerebrospinal fluid drainage testing. Management centers on careful patient selection for shunt surgery, use of programmable valves, and longitudinal monitoring to balance symptomatic improvement with complication risk. Timely recognition and standardized evaluation remain critical to reducing misdiagnosis and delayed treatment.
Optimal evaluation and management of iNPH depend on coordinated interprofessional care. Neurologists typically lead syndrome recognition, objective gait and cognitive assessment, and exclusion of alternative diagnoses, while radiologists contribute standardized imaging interpretation using structured frameworks that enhance diagnostic confidence and team communication. Neurosurgeons integrate clinical and prognostic data into shared decision-making regarding shunt candidacy, valve selection, and postoperative adjustment strategies. General practitioners and advanced practitioners support longitudinal monitoring, comorbidity management, and continuity of care across settings.
Physical therapists and rehabilitation specialists provide baseline and postshunt mobility assessment and targeted gait and balance interventions that inform treatment response. Nursing professionals and caregivers play a central role in perioperative safety through monitoring for delirium, infection, wound complications, and overdrainage symptoms, enabling early escalation. Pharmacists and other health professionals contribute to medication optimization, fall-risk reduction, and patient education, collectively enhancing patient-centered outcomes, safety, and team performance.
Media
(Click Image to Enlarge)
Normal Pressure Hydrocephalus. Disproportionately enlarged subarachnoid space hydrocephalus, characterized by ventriculomegaly, enlargement of the Sylvian fissures, and compression of the high-convexity and midline subarachnoid spaces, represents a specific imaging phenotype of iNPH with strong positive but weak negative predictive value.
Contributed by S Bhimji, MD
(Click Image to Enlarge)

Normal Pressure Hydrocephalus Imaging. Computed tomography (CT) contributes to the visualization of anatomic brain changes but lacks sufficient specificity for diagnosis when used in isolation.
Contributed by S Lange, MD
(Click Image to Enlarge)
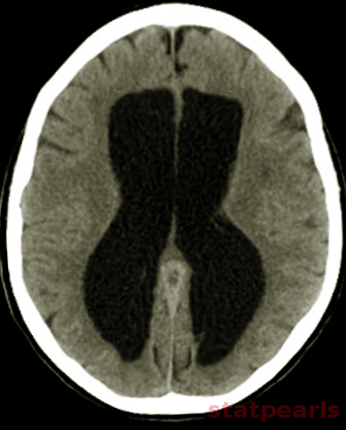
Normal Pressure Hydrocephalus CT. Computed tomography (CT) contributes to the visualization of anatomic brain changes but lacks sufficient specificity for diagnosis when used in isolation.
Contributed by S Munakomi, MD
(Click Image to Enlarge)
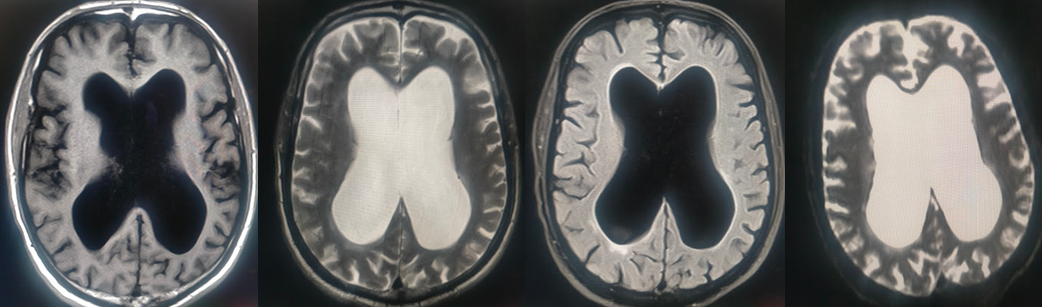
Imaging Hallmarks of Idiopathic Normal Pressure Hydrocephalus. Magnetic resonance imaging (MRI) plays a central role in the evaluation of suspected iNPH by documenting ventriculomegaly and characteristic morphologic features that support diagnosis within the appropriate clinical context.
Contributed by K Margetis, MD
References
Adams RD, Fisher CM, Hakim S, Ojemann RG, Sweet WH. SYMPTOMATIC OCCULT HYDROCEPHALUS WITH "NORMAL" CEREBROSPINAL-FLUID PRESSURE. A TREATABLE SYNDROME. The New England journal of medicine. 1965 Jul 15:273():117-26 [PubMed PMID: 14303656]
Shprecher D, Schwalb J, Kurlan R. Normal pressure hydrocephalus: diagnosis and treatment. Current neurology and neuroscience reports. 2008 Sep:8(5):371-6 [PubMed PMID: 18713572]
Nakajima M, Yamada S, Miyajima M, Ishii K, Kuriyama N, Kazui H, Kanemoto H, Suehiro T, Yoshiyama K, Kameda M, Kajimoto Y, Mase M, Murai H, Kita D, Kimura T, Samejima N, Tokuda T, Kaijima M, Akiba C, Kawamura K, Atsuchi M, Hirata Y, Matsumae M, Sasaki M, Yamashita F, Aoki S, Irie R, Miyake H, Kato T, Mori E, Ishikawa M, Date I, Arai H, research committee of idiopathic normal pressure hydrocephalus. Guidelines for Management of Idiopathic Normal Pressure Hydrocephalus (Third Edition): Endorsed by the Japanese Society of Normal Pressure Hydrocephalus. Neurologia medico-chirurgica. 2021 Feb 15:61(2):63-97. doi: 10.2176/nmc.st.2020-0292. Epub 2021 Jan 15 [PubMed PMID: 33455998]
Wang Z, Zhang Y, Hu F, Ding J, Wang X. Pathogenesis and pathophysiology of idiopathic normal pressure hydrocephalus. CNS neuroscience & therapeutics. 2020 Dec:26(12):1230-1240. doi: 10.1111/cns.13526. Epub 2020 Nov 26 [PubMed PMID: 33242372]
Jaraj D, Rabiei K, Marlow T, Jensen C, Skoog I, Wikkelsø C. Prevalence of idiopathic normal-pressure hydrocephalus. Neurology. 2014 Apr 22:82(16):1449-54. doi: 10.1212/WNL.0000000000000342. Epub 2014 Mar 28 [PubMed PMID: 24682964]
Level 2 (mid-level) evidenceKim MJ, Seo SW, Lee KM, Kim ST, Lee JI, Nam DH, Na DL. Differential diagnosis of idiopathic normal pressure hydrocephalus from other dementias using diffusion tensor imaging. AJNR. American journal of neuroradiology. 2011 Sep:32(8):1496-503. doi: 10.3174/ajnr.A2531. Epub 2011 Jun 23 [PubMed PMID: 21700790]
Brean A, Fredø HL, Sollid S, Müller T, Sundstrøm T, Eide PK. Five-year incidence of surgery for idiopathic normal pressure hydrocephalus in Norway. Acta neurologica Scandinavica. 2009 Nov:120(5):314-6. doi: 10.1111/j.1600-0404.2009.01250.x. Epub [PubMed PMID: 19832773]
Level 2 (mid-level) evidenceTanaka N, Yamaguchi S, Ishikawa H, Ishii H, Meguro K. Prevalence of possible idiopathic normal-pressure hydrocephalus in Japan: the Osaki-Tajiri project. Neuroepidemiology. 2009:32(3):171-5. doi: 10.1159/000186501. Epub 2008 Dec 19 [PubMed PMID: 19096225]
Level 2 (mid-level) evidenceKrauss JK, Halve B. Normal pressure hydrocephalus: survey on contemporary diagnostic algorithms and therapeutic decision-making in clinical practice. Acta neurochirurgica. 2004 Apr:146(4):379-88; discussion 388 [PubMed PMID: 15057532]
Level 3 (low-level) evidenceBonney PA, Briggs RG, Wu K, Choi W, Khahera A, Ojogho B, Shao X, Zhao Z, Borzage M, Wang DJJ, Liu C, Lee DJ. Pathophysiological Mechanisms Underlying Idiopathic Normal Pressure Hydrocephalus: A Review of Recent Insights. Frontiers in aging neuroscience. 2022:14():866313. doi: 10.3389/fnagi.2022.866313. Epub 2022 Apr 28 [PubMed PMID: 35572128]
Libard S, Alafuzoff I. Alzheimer's disease neuropathological change and loss of matrix/neuropil in patients with idiopathic Normal Pressure Hydrocephalus, a model of Alzheimer's disease. Acta neuropathologica communications. 2019 May 29:7(1):98. doi: 10.1186/s40478-019-0748-9. Epub 2019 May 29 [PubMed PMID: 31142354]
Bradley WG Jr, Scalzo D, Queralt J, Nitz WN, Atkinson DJ, Wong P. Normal-pressure hydrocephalus: evaluation with cerebrospinal fluid flow measurements at MR imaging. Radiology. 1996 Feb:198(2):523-9 [PubMed PMID: 8596861]
Bateman GA. The reversibility of reduced cortical vein compliance in normal-pressure hydrocephalus following shunt insertion. Neuroradiology. 2003 Feb:45(2):65-70 [PubMed PMID: 12592485]
Stephensen H, Tisell M, Wikkelsö C. There is no transmantle pressure gradient in communicating or noncommunicating hydrocephalus. Neurosurgery. 2002 Apr:50(4):763-71; discussion 771-3 [PubMed PMID: 11904027]
Børgesen SE, Gjerris F. The predictive value of conductance to outflow of CSF in normal pressure hydrocephalus. Brain : a journal of neurology. 1982 Mar:105(Pt 1):65-86 [PubMed PMID: 7066675]
Edwards RJ, Dombrowski SM, Luciano MG, Pople IK. Chronic hydrocephalus in adults. Brain pathology (Zurich, Switzerland). 2004 Jul:14(3):325-36 [PubMed PMID: 15446589]
Level 3 (low-level) evidenceWang W, Liu M, Wang Z, Ma L, Zhao Y, Ye W, Li X. Causal associations between gut microbiota, metabolites, and idiopathic normal pressure hydrocephalus: a two‑sample Mendelian randomization study. BMC neurology. 2025 Jun 9:25(1):249. doi: 10.1186/s12883-025-04187-4. Epub 2025 Jun 9 [PubMed PMID: 40490712]
Owler BK, Pickard JD. Normal pressure hydrocephalus and cerebral blood flow: a review. Acta neurologica Scandinavica. 2001 Dec:104(6):325-42 [PubMed PMID: 11903086]
Tarkowski E, Tullberg M, Fredman P, Wikkelsö C. Normal pressure hydrocephalus triggers intrathecal production of TNF-alpha. Neurobiology of aging. 2003 Sep:24(5):707-14 [PubMed PMID: 12885578]
Level 2 (mid-level) evidenceLi X, Miyajima M, Jiang C, Arai H. Expression of TGF-betas and TGF-beta type II receptor in cerebrospinal fluid of patients with idiopathic normal pressure hydrocephalus. Neuroscience letters. 2007 Feb 14:413(2):141-4 [PubMed PMID: 17194537]
Level 3 (low-level) evidenceSilverberg GD. Normal pressure hydrocephalus (NPH): ischaemia, CSF stagnation or both. Brain : a journal of neurology. 2004 May:127(Pt 5):947-8 [PubMed PMID: 15111447]
Bateman GA. Vascular compliance in normal pressure hydrocephalus. AJNR. American journal of neuroradiology. 2000 Oct:21(9):1574-85 [PubMed PMID: 11039334]
Greitz D. Radiological assessment of hydrocephalus: new theories and implications for therapy. Neurosurgical review. 2004 Jul:27(3):145-65; discussion 166-7 [PubMed PMID: 15164255]
Level 3 (low-level) evidenceMalm J, Graff-Radford NR, Ishikawa M, Kristensen B, Leinonen V, Mori E, Owler BK, Tullberg M, Williams MA, Relkin NR. Influence of comorbidities in idiopathic normal pressure hydrocephalus - research and clinical care. A report of the ISHCSF task force on comorbidities in INPH. Fluids and barriers of the CNS. 2013 Jun 10:10(1):22. doi: 10.1186/2045-8118-10-22. Epub 2013 Jun 10 [PubMed PMID: 23758953]
Cucca A, Biagioni MC, Sharma K, Golomb J, Gilbert RM, Di Rocco A, Fleisher JE. Comorbid Normal Pressure Hydrocephalus with Parkinsonism: A Clinical Challenge and Call for Awareness. Case reports in neurological medicine. 2018:2018():2513474. doi: 10.1155/2018/2513474. Epub 2018 Jan 21 [PubMed PMID: 29610690]
Level 3 (low-level) evidenceGleason PL, Black PM, Matsumae M. The neurobiology of normal pressure hydrocephalus. Neurosurgery clinics of North America. 1993 Oct:4(4):667-75 [PubMed PMID: 8241789]
Corkill RG, Cadoux-Hudson TA. Normal pressure hydrocephalus: developments in determining surgical prognosis. Current opinion in neurology. 1999 Dec:12(6):671-7 [PubMed PMID: 10676746]
Level 3 (low-level) evidenceRubin RC, Hochwald GM, Tiell M, Mizutani H, Ghatak N. Hydrocephalus: I. Histological and ultrastructural changes in the pre-shunted cortical mantle. Surgical neurology. 1976 Feb:5(2):109-14 [PubMed PMID: 1257875]
Lenfeldt N, Larsson A, Nyberg L, Birgander R, Eklund A, Malm J. Diffusion tensor imaging reveals supplementary lesions to frontal white matter in idiopathic normal pressure hydrocephalus. Neurosurgery. 2011 Jun:68(6):1586-93; discussion 1593. doi: 10.1227/NEU.0b013e31820f3401. Epub [PubMed PMID: 21336219]
Graff-Radford NR, Godersky JC. Normal-pressure hydrocephalus. Onset of gait abnormality before dementia predicts good surgical outcome. Archives of neurology. 1986 Sep:43(9):940-2 [PubMed PMID: 3741212]
Park E, Kang K, Lee J, Lee JT, Park KS, Kim CH, Min YS. Characteristics of Postural Instability in Idiopathic Normal Pressure Hydrocephalus. Neurology and therapy. 2025 Oct:14(5):1961-1974. doi: 10.1007/s40120-025-00786-y. Epub 2025 Jul 13 [PubMed PMID: 40653591]
Relkin N, Marmarou A, Klinge P, Bergsneider M, Black PM. Diagnosing idiopathic normal-pressure hydrocephalus. Neurosurgery. 2005 Sep:57(3 Suppl):S4-16; discussion ii-v [PubMed PMID: 16160425]
Kockum K, Lilja-Lund O, Larsson EM, Rosell M, Söderström L, Virhammar J, Laurell K. The idiopathic normal-pressure hydrocephalus Radscale: a radiological scale for structured evaluation. European journal of neurology. 2018 Mar:25(3):569-576. doi: 10.1111/ene.13555. Epub 2018 Feb 2 [PubMed PMID: 29281156]
Hashimoto M, Ishikawa M, Mori E, Kuwana N, Study of INPH on neurological improvement (SINPHONI). Diagnosis of idiopathic normal pressure hydrocephalus is supported by MRI-based scheme: a prospective cohort study. Cerebrospinal fluid research. 2010 Oct 31:7():18. doi: 10.1186/1743-8454-7-18. Epub 2010 Oct 31 [PubMed PMID: 21040519]
Behndig S, Lalou A, Axelsson J, Larsson J, Wåhlin A, Ryska P, Slezak O, Riklund K, Zizka J, Malm J, Eklund A. qDESH: a method to quantify disproportionately enlarged subarachnoid space hydrocephalus. Fluids and barriers of the CNS. 2025 Jul 1:22(1):67. doi: 10.1186/s12987-025-00677-2. Epub 2025 Jul 1 [PubMed PMID: 40597328]
Shinoda N, Hirai O, Hori S, Mikami K, Bando T, Shimo D, Kuroyama T, Kuramoto Y, Matsumoto M, Ueno Y. Utility of MRI-based disproportionately enlarged subarachnoid space hydrocephalus scoring for predicting prognosis after surgery for idiopathic normal pressure hydrocephalus: clinical research. Journal of neurosurgery. 2017 Dec:127(6):1436-1442. doi: 10.3171/2016.9.JNS161080. Epub 2017 Feb 3 [PubMed PMID: 28156249]
Roşu AI, Andrei D, Ghenciu LA, Bolintineanu SL. Hydrocephalus: Molecular and Neuroimaging Biomarkers in Diagnosis and Management. Biomedicines. 2025 Jun 20:13(7):. doi: 10.3390/biomedicines13071511. Epub 2025 Jun 20 [PubMed PMID: 40722587]
Eleftheriou A, Blystad I, Tisell A, Gasslander J, Lundin F. Indication of Thalamo-Cortical Circuit Dysfunction in Idiopathic Normal Pressure Hydrocephalus: A Tensor Imaging Study. Scientific reports. 2020 Apr 9:10(1):6148. doi: 10.1038/s41598-020-63238-7. Epub 2020 Apr 9 [PubMed PMID: 32273554]
Broggi M, Barbieri EM, Gans A, Riccardo P, Redaelli V, Aquino D, Restelli F, Schiariti M, Acerbi F, Di Fede G, Ferroli P, Grisoli M, Doniselli F. Implications of the glymphatic system in the diagnostic and surgical workup of normal pressure hydrocephalus. Neurological sciences : official journal of the Italian Neurological Society and of the Italian Society of Clinical Neurophysiology. 2025 Sep:46(9):4433-4443. doi: 10.1007/s10072-025-08308-2. Epub 2025 Jun 16 [PubMed PMID: 40524080]
Fattahi N, Arani A, Perry A, Meyer F, Manduca A, Glaser K, Senjem ML, Ehman RL, Huston J. MR Elastography Demonstrates Increased Brain Stiffness in Normal Pressure Hydrocephalus. AJNR. American journal of neuroradiology. 2016 Mar:37(3):462-7. doi: 10.3174/ajnr.A4560. Epub 2015 Nov 5 [PubMed PMID: 26542235]
ElSheikh M, Arani A, Perry A, Boeve BF, Meyer FB, Savica R, Ehman RL, Huston J 3rd. MR Elastography Demonstrates Unique Regional Brain Stiffness Patterns in Dementias. AJR. American journal of roentgenology. 2017 Aug:209(2):403-408. doi: 10.2214/AJR.16.17455. Epub 2017 Jun 1 [PubMed PMID: 28570101]
Ringstad G, Vatnehol SAS, Eide PK. Glymphatic MRI in idiopathic normal pressure hydrocephalus. Brain : a journal of neurology. 2017 Oct 1:140(10):2691-2705. doi: 10.1093/brain/awx191. Epub [PubMed PMID: 28969373]
Kadaba Sridhar S, Kuang R, Dysterheft Robb J, Samadani U. A ventriculomegaly feature computational pipeline to improve the screening of normal pressure hydrocephalus on CT. Journal of neurosurgery. 2024 Sep 1:141(3):822-832. doi: 10.3171/2023.12.JNS231780. Epub 2024 Mar 8 [PubMed PMID: 38457801]
Al-Zain FT, Rademacher G, Lemcke J, Mutze J, Meier U. [Idiopathic normal-pressure hydrocephalus. Flow measurement of cerebrospinal fluid using phase contrast MRI and its diagnostics importance]. Der Nervenarzt. 2007 Feb:78(2):181-7 [PubMed PMID: 17225144]
Krauss JK, Regel JP, Vach W, Jüngling FD, Droste DW, Wakhloo AK. Flow void of cerebrospinal fluid in idiopathic normal pressure hydrocephalus of the elderly: can it predict outcome after shunting? Neurosurgery. 1997 Jan:40(1):67-73; discussion 73-4 [PubMed PMID: 8971826]
Kobayashi E, Kanno S, Kawakami N, Narita W, Saito M, Endo K, Iwasaki M, Kawaguchi T, Yamada S, Ishii K, Kazui H, Miyajima M, Ishikawa M, Mori E, Tominaga T, Tanaka F, Suzuki K. Risk factors for unfavourable outcomes after shunt surgery in patients with idiopathic normal-pressure hydrocephalus. Scientific reports. 2022 Aug 17:12(1):13921. doi: 10.1038/s41598-022-18209-5. Epub 2022 Aug 17 [PubMed PMID: 35978079]
Graff-Radford NR, Jones DT. Normal Pressure Hydrocephalus. Continuum (Minneapolis, Minn.). 2019 Feb:25(1):165-186. doi: 10.1212/CON.0000000000000689. Epub [PubMed PMID: 30707192]
Townley RA, Botha H, Graff-Radford J, Boeve BF, Petersen RC, Senjem ML, Knopman DS, Lowe V, Jack CR Jr, Jones DT. (18)F-FDG PET-CT pattern in idiopathic normal pressure hydrocephalus. NeuroImage. Clinical. 2018:18():897-902. doi: 10.1016/j.nicl.2018.02.031. Epub 2018 Feb 28 [PubMed PMID: 29876274]
Yamada S, Ishikawa M, Miyajima M, Nakajima M, Atsuchi M, Kimura T, Tokuda T, Kazui H, Mori E. Timed up and go test at tap test and shunt surgery in idiopathic normal pressure hydrocephalus. Neurology. Clinical practice. 2017 Apr:7(2):98-108. doi: 10.1212/CPJ.0000000000000334. Epub [PubMed PMID: 29185546]
Cihlo M, Trávníček P, Tichá A, Hyšpler R, Kalousová M, Řehák S, Zadrobílek K, Kukrálová L, Póczoš P, Pospíšil J, Dostál P, Dostálová V. Value of biomarkers in the prediction of shunt responsivity in patients with normal pressure hydrocephalus. Neurosurgical review. 2025 Jun 3:48(1):474. doi: 10.1007/s10143-025-03581-3. Epub 2025 Jun 3 [PubMed PMID: 40457021]
Kazui H, Miyajima M, Mori E, Ishikawa M, SINPHONI-2 Investigators. Lumboperitoneal shunt surgery for idiopathic normal pressure hydrocephalus (SINPHONI-2): an open-label randomised trial. The Lancet. Neurology. 2015 Jun:14(6):585-94. doi: 10.1016/S1474-4422(15)00046-0. Epub 2015 Apr 28 [PubMed PMID: 25934242]
Level 1 (high-level) evidenceMiyajima M, Kazui H, Mori E, Ishikawa M, , on behalf of the SINPHONI-2 Investigators. One-year outcome in patients with idiopathic normal-pressure hydrocephalus: comparison of lumboperitoneal shunt to ventriculoperitoneal shunt. Journal of neurosurgery. 2016 Dec:125(6):1483-1492 [PubMed PMID: 26871203]
Tudor KI, Tudor M, McCleery J, Car J. Endoscopic third ventriculostomy (ETV) for idiopathic normal pressure hydrocephalus (iNPH). The Cochrane database of systematic reviews. 2015 Jul 29:2015(7):CD010033. doi: 10.1002/14651858.CD010033.pub2. Epub 2015 Jul 29 [PubMed PMID: 26222251]
Level 1 (high-level) evidenceLemcke J, Meier U, Müller C, Fritsch MJ, Kehler U, Langer N, Kiefer M, Eymann R, Schuhmann MU, Speil A, Weber F, Remenez V, Rohde V, Ludwig HC, Stengel D. Safety and efficacy of gravitational shunt valves in patients with idiopathic normal pressure hydrocephalus: a pragmatic, randomised, open label, multicentre trial (SVASONA). Journal of neurology, neurosurgery, and psychiatry. 2013 Aug:84(8):850-7. doi: 10.1136/jnnp-2012-303936. Epub 2013 Mar 1 [PubMed PMID: 23457222]
Level 1 (high-level) evidenceDelwel EJ, de Jong DA, Dammers R, Kurt E, van den Brink W, Dirven CM. A randomised trial of high and low pressure level settings on an adjustable ventriculoperitoneal shunt valve for idiopathic normal pressure hydrocephalus: results of the Dutch evaluation programme Strata shunt (DEPSS) trial. Journal of neurology, neurosurgery, and psychiatry. 2013 Jul:84(7):813-7. doi: 10.1136/jnnp-2012-302935. Epub 2013 Feb 13 [PubMed PMID: 23408069]
Level 1 (high-level) evidenceMerkler AE, Ch'ang J, Parker WE, Murthy SB, Kamel H. The Rate of Complications after Ventriculoperitoneal Shunt Surgery. World neurosurgery. 2017 Feb:98():654-658. doi: 10.1016/j.wneu.2016.10.136. Epub 2016 Nov 5 [PubMed PMID: 27826086]
Farahmand D, Sæhle T, Eide PK, Tisell M, Hellström P, Wikkelsö C. A double-blind randomized trial on the clinical effect of different shunt valve settings in idiopathic normal pressure hydrocephalus. Journal of neurosurgery. 2016 Feb:124(2):359-67. doi: 10.3171/2015.1.JNS141301. Epub 2015 Aug 28 [PubMed PMID: 26315004]
Level 1 (high-level) evidenceScholz R, Lemcke J, Meier U, Stengel D. Efficacy and safety of programmable compared with fixed anti-siphon devices for treating idiopathic normal-pressure hydrocephalus (iNPH) in adults - SYGRAVA: study protocol for a randomized trial. Trials. 2018 Oct 17:19(1):566. doi: 10.1186/s13063-018-2951-6. Epub 2018 Oct 17 [PubMed PMID: 30333067]
Level 1 (high-level) evidenceBoon AJ, Tans JT, Delwel EJ, Egeler-Peerdeman SM, Hanlo PW, Wurzer HA, Avezaat CJ, de Jong DA, Gooskens RH, Hermans J. Dutch Normal-Pressure Hydrocephalus Study: randomized comparison of low- and medium-pressure shunts. Journal of neurosurgery. 1998 Mar:88(3):490-5 [PubMed PMID: 9488303]
Level 1 (high-level) evidenceMarmarou A, Bergsneider M, Klinge P, Relkin N, Black PM. The value of supplemental prognostic tests for the preoperative assessment of idiopathic normal-pressure hydrocephalus. Neurosurgery. 2005 Sep:57(3 Suppl):S17-28; discussion ii-v [PubMed PMID: 16160426]
Kawai R, Kazui H, Ueba T, Nakamura N, Minami M, Nakajima M, Yamada S, Kishima H, Kanemoto H, Iseki C, Mori E. Characteristics of patients with idiopathic normal pressure hydrocephalus for whom neurosurgeons hesitate to perform shunt surgery: a nationwide hospital-based survey in Japan. Fluids and barriers of the CNS. 2025 Jul 4:22(1):69. doi: 10.1186/s12987-025-00681-6. Epub 2025 Jul 4 [PubMed PMID: 40616109]
Level 3 (low-level) evidencePištěk K, Sameš M, Radovnický T. Endoscopic third ventriculostomy in idiopathic normal pressure hydrocephalus. Efficacy and possible positive predictors: a systematic review. Brain & spine. 2025:5():104311. doi: 10.1016/j.bas.2025.104311. Epub 2025 Jul 7 [PubMed PMID: 40704134]
Level 1 (high-level) evidenceKiefer M, Unterberg A. The differential diagnosis and treatment of normal-pressure hydrocephalus. Deutsches Arzteblatt international. 2012 Jan:109(1-2):15-25; quiz 26. doi: 10.3238/arztebl.2012.0015. Epub 2012 Jan 9 [PubMed PMID: 22282714]
Giordan E, Palandri G, Lanzino G, Murad MH, Elder BD. Outcomes and complications of different surgical treatments for idiopathic normal pressure hydrocephalus: a systematic review and meta-analysis. Journal of neurosurgery. 2019 Oct 1:131(4):1024-1036. doi: 10.3171/2018.5.JNS1875. Epub 2018 Nov 23 [PubMed PMID: 30497150]
Level 1 (high-level) evidenceHamilton R, Patel S, Lee EB, Jackson EM, Lopinto J, Arnold SE, Clark CM, Basil A, Shaw LM, Xie SX, Grady MS, Trojanowski JQ. Lack of shunt response in suspected idiopathic normal pressure hydrocephalus with Alzheimer disease pathology. Annals of neurology. 2010 Oct:68(4):535-40. doi: 10.1002/ana.22015. Epub [PubMed PMID: 20687117]
Koivisto AM, Alafuzoff I, Savolainen S, Sutela A, Rummukainen J, Kurki M, Jääskeläinen JE, Soininen H, Rinne J, Leinonen V, Kuopio NPH Registry (www.uef.finph). Poor cognitive outcome in shunt-responsive idiopathic normal pressure hydrocephalus. Neurosurgery. 2013 Jan:72(1):1-8;discussion 8. doi: 10.1227/NEU.0b013e31827414b3. Epub [PubMed PMID: 23037817]
Gasslander J, Sundström N, Eklund A, Koskinen LD, Malm J. Risk factors for developing subdural hematoma: a registry-based study in 1457 patients with shunted idiopathic normal pressure hydrocephalus. Journal of neurosurgery. 2021 Feb 1:134(2):668-677. doi: 10.3171/2019.10.JNS191223. Epub 2020 Jan 10 [PubMed PMID: 31923893]