Introduction
Charcot neuropathic osteoarthropathy is a progressive disorder characterized by joint destabilization, bone resorption, and deformity that develops in the setting of peripheral neuropathy. The underlying pathophysiology involves loss of protective sensation and impaired proprioception, allowing repetitive microtrauma to occur without patient awareness. Autonomic dysfunction contributes to increased local blood flow and osteoclastic activation, producing rapid bone demineralization and structural collapse. The resulting cycle of inflammation and mechanical instability leads to progressive joint destruction, most commonly affecting the midfoot, hindfoot, or ankle.[1]
Risk factors include long-standing diabetes mellitus—particularly with poor glycemic control—peripheral neuropathy of any etiology, renal failure, obesity, and prior foot trauma or ulceration. Patients typically present with a warm, swollen, and erythematous foot that may be mistaken for infection, delaying diagnosis.[1][2]
Management strategies focus on early recognition and immediate immobilization to halt further deformity. Total contact casting or other offloading methods remain the cornerstone of initial treatment until clinical inflammation resolves and radiographic stability is achieved. In cases of severe deformity, instability, or recurrent ulceration, surgical intervention, eg, realignment osteotomy or arthrodesis, may be required. Long-term success depends on patient adherence, vigilant surveillance, and optimization of underlying metabolic and neuropathic conditions.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Charcot neuropathic osteoarthropathy develops as a consequence of peripheral neuropathy, which impairs the normal protective mechanisms that maintain joint integrity. The etiology of this disorder is multifactorial, involving sensory, motor, and autonomic neuropathic components that collectively predispose the foot and ankle to progressive structural failure. Sensory neuropathy eliminates protective pain perception, allowing repetitive microtrauma during daily ambulation to occur unnoticed. Motor neuropathy contributes to muscular imbalance and altered joint loading, while autonomic neuropathy increases regional blood flow through arteriovenous shunting. This hyperemia stimulates osteoclastic activity, accelerating bone resorption and reducing structural strength.
Two primary theories describe the etiopathogenesis of Charcot neuropathic osteoarthropathy. The neurotraumatic theory proposes that unrecognized mechanical trauma in an insensate foot initiates the destructive process, with cumulative microinjuries leading to joint instability and collapse. However, the neurovascular theory emphasizes autonomic dysregulation, in which increased local blood flow and osteoclastic activation lead to rapid bone turnover, weakening the osseous framework and predisposing it to fragmentation even under normal physiological loads. In practice, both mechanisms likely interact, with neuropathy initiating susceptibility and continued weight-bearing amplifying the cycle of damage.
Diabetes mellitus is the most common underlying condition of Charcot neuropathic osteoarthropathy, particularly in patients with long-standing disease, poor glycemic control, or established peripheral neuropathy. Additional etiologies include alcoholism, peripheral nerve injury, spinal cord lesions, congenital insensitivity to pain, and other neuropathic disorders. Trauma—often minor or unrecognized—frequently precipitates the acute onset, acting as a trigger within an already vulnerable biomechanical environment.
Ultimately, the etiology of Charcot neuropathic osteoarthropathy reflects a convergence of neuropathic impairment, altered bone metabolism, and mechanical overload. This interplay creates a self-perpetuating cycle of inflammation, osteolysis, and instability that, without timely intervention, progresses to significant deformity and long-term functional compromise.[3][2][4][5]
Epidemiology
Among individuals with diabetes mellitus, the prevalence of Charcot neuropathic osteoarthropathy is commonly reported in the range of 0.1% to 0.9%. In high-risk patients, eg, people with diabetes with documented peripheral neuropathy, prevalence may increase to up to 29% to 35%.[6] Onset typically occurs in individuals aged 50 to 60 and is more common in those with a longer duration of diabetes.[7] The majority of studies suggest a slightly higher incidence in men.[6][8] Around 20% of those affected will have bilateral foot involvement.[8]
Pathophysiology
The pathophysiology of Charcot neuropathic osteoarthropathy has not yet been fully elucidated, and both neurotraumatic and neurovascular theories have been proposed. However, recent evidence points to a combination of both these theories underlying the pathogenesis of the disease.[9][10] Loss of protective sensation and proprioception leads to unrecognized repetitive microtrauma, triggering a proinflammatory cascade characterized by elevated cytokines, eg, TNF-α, IL-1β, and IL-6.[11][12]
This inflammatory milieu activates the RANK/RANKL/OPG pathway, promoting osteoclast differentiation and uncontrolled bone resorption.[13][9] Autonomic dysregulation increases blood flow to the foot, stimulating osteoclastic bone resorption, causing osteopenia and further structural weakening.[14] Collectively, these result in osteolysis, joint subluxation, and fragmentation, ultimately destabilizing the foot’s structural integrity.[4][10]
Histopathology
Histopathologic examination reveals features consistent with an active inflammatory and osteolytic process involving both bone and soft tissue. In the acute phase, bone biopsies demonstrate trabecular bone resorption, microfractures, marrow edema, and prominent osteoclastic activity. Woven bone is immature and structurally disorganized with decreased osteocytes and empty lacunae.[15][16]
History and Physical
Collectively, a comprehensive history and detailed examination provide the foundation for early diagnosis, appropriate imaging, and timely offloading—critical steps in preventing irreversible collapse and ensuring optimal long-term outcomes.
Clinical History
A high index of suspicion is essential for accurate diagnosis of Charcot neuropathic osteoarthropathy, as early clinical findings often mimic those of other inflammatory or infectious conditions. Patients typically present with a warm, erythematous, and edematous foot that is often unilateral and associated with minimal or absent pain due to underlying neuropathy. The onset is usually acute or subacute, frequently following minor trauma such as an ankle sprain or repetitive microtrauma from walking or ill-fitting footwear. The initial incident may not be perceived, leading the patient to continue walking and resulting in a severe inflammatory response.[17][2]
Physical Examination
Physical examination findings associated with Charcot neuropathic osteoarthropathy are characterized by pronounced swelling, erythema, and increased localized temperature, often exceeding that of the contralateral limb by 2 °C or more (as measured with infrared thermography). Importantly, pain is typically minimal or absent despite the apparent severity of findings. The foot may appear clinically unstable, with subtle or overt collapse of the medial or lateral column, depending on the stage at presentation. Palpation often reveals bony prominences, particularly along the midfoot, reflecting early subluxation or fragmentation. Joint effusion may be appreciated at the ankle or subtalar joints in hindfoot involvement.
A key feature distinguishing Charcot from infection is that erythema often decreases with elevation, whereas infectious processes tend to be less positional. Pulses are typically bounding due to autonomic dysregulation, despite the presence of significant edema. Sensory examination reveals loss of protective sensation to monofilament testing, diminished vibration perception, and reduced proprioception. Motor neuropathy may manifest as intrinsic muscle wasting or clawing of the toes. Assessment should include evaluation for deformities, eg, rocker-bottom foot or varus malalignment, as these indicate progression toward chronic stages.[18][19][20][19] Gait evaluation may reveal an antalgic pattern or midfoot instability. In later stages, ulceration may occur at areas of abnormal pressure. Careful inspection of the skin is required to identify preulcerative callus or subtle breakdown, which has significant implications for management.
Radiographic evaluation in early stages may be normal or show subtle subluxations and bone fragmentation. As the disease progresses, collapse of the midfoot with rocker-bottom deformity often becomes apparent. Importantly, osteomyelitis and Charcot arthropathy can coexist, and chronic infection may trigger Charcot activation by amplifying systemic and local inflammatory cytokine production, eg, TNF-α and IL-6. Postsurgical trauma or partial amputations may also precipitate Charcot neuropathic osteoarthropathy by altering biomechanical loading and plantar pressure distribution, resulting in new zones of microtrauma that perpetuate the inflammatory process.[21][17][9]
Evaluation
The evaluation of Charcot neuropathic osteoarthropathy relies on a combination of clinical assessment, laboratory testing, and advanced imaging, with an emphasis on early diagnosis to prevent irreversible deformity.
Laboratory Evaluation
Routine laboratory markers, eg, white blood cell count, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP), may or may not be elevated in acute Charcot. They are often significantly elevated in osteomyelitis, which has previously been suggested to aid differentiation. However, current International Working Group on the Diabetic Foot (IWGDF) recommendations do not recommend using these laboratory values to distinguish Charcot neuropathic osteoarthropathy, as strong evidence for their use does not exist.[22][23]
Imaging Evaluation
Plain radiographs
Plain radiographs are the initial imaging modality and are essential for evaluating structural changes. Early radiographs may appear normal or demonstrate only subtle periarticular osteopenia and soft-tissue swelling. As the condition progresses, fragmentation, subluxation, dislocation, and collapse of the medial or lateral column become evident. Weight-bearing radiographs are particularly useful for assessing alignment and structural integrity. Bilateral films should be obtained for comparison, and imaging should be obtained standing if possible.[23]
Magnetic resonance imaging
Magnetic resonance imaging (MRI) is the most sensitive modality for detecting early Charcot changes before radiographic abnormalities appear. MRI demonstrates bone marrow edema, subchondral cysts, joint effusion, and surrounding soft-tissue inflammation. Importantly, MRI helps distinguish Charcot from osteomyelitis: osteomyelitis typically shows diffuse marrow replacement with contiguous soft-tissue ulcers, whereas Charcot demonstrates periarticular edema without a direct ulcer tract. MRI should be performed when a strong clinical suspicion for Charcot neuropathic osteoarthropathy in the setting of normal radiographs exists.[23][24]
Nuclear imaging
Nuclear imaging (eg, labeled leukocyte or technetium scans) may be used when differentiating Charcot from infection remains challenging. Bone scans demonstrate increased uptake in both conditions, whereas labeled leukocyte scans are more specific for infection.[23][25]
Computed tomography
Weight-bearing computed tomography (CT) provides excellent visualization of cortical disruption, fragmentation, and subtle subluxation in advanced disease. CT is particularly helpful for surgical planning when joint reconstruction or arthrodesis is considered.[23]
Additional Diagnostic Studies
Temperature assessment is a valuable clinical adjunct, as acute Charcot typically demonstrates a temperature difference of greater than 2 °C between the affected and contralateral foot. Vascular evaluation, including Doppler studies, may be required when severe edema obscures pulse palpation. Neurological assessment, including monofilament and vibration testing, confirms the presence and extent of peripheral neuropathy, a prerequisite for diagnosis.
Guideline Recommendations
Both the IWGDF and the American Diabetes Association (ADA) recommend the following:
-
Maintaining high clinical suspicion for Charcot neuropathic osteoarthropathy in any neuropathic patient presenting with a red, hot, swollen foot.
-
Performing bilateral imaging for comparison and using MRI when plain radiographs are inconclusive.
Treatment / Management
Immobilization and Offloading Strategies
Management of acute Charcot neuropathic osteoarthropathy focuses on immobilization and offloading, followed by staged return to protected weight-bearing and, in select cases, reconstructive surgery. The IWGDF 2023 guideline recommends a nonremovable knee-high device (total contact cast) or a removable knee-high device altered to be irremovable. These should be initiated as soon as clinical suspicion arises, even before confirmatory imaging. A removable knee-high device worn at all times may be considered for patients who cannot wear or tolerate a nonremovable device. Immobilization should be continued until clinical remission (resolution of warmth/edema, ≤2 °C temperature difference between the extremities, and radiographic consolidation). Full remission may take months, and immobilization should continue until 4 to 6 weeks past remission.[23][26][27](A1)
Pharmacologic Therapy
Pharmacologic adjuncts have limited and mixed evidence and are not first-line. No strong evidence exists for their use, and so they are not currently recommended. In addition, potential harmful effects on bone healing and iatrogenic fractures exist. Supplementation with calcium and vitamin D is recommended concurrently with immobilization in those with or at risk of deficiency. Doses should follow international guidelines.[23][28][27] When a foot infection or osteomyelitis occurs at the same time as Charcot neuropathic osteoarthropathy, management should occur following IWGDF 2023 infection guideline (bone culture, appropriate targeted antibiotics, and early source control), in parallel with immobilization.(A1)
Surgical Management
Surgical management is reserved for nonbraceable deformity, instability, recurrent/impending ulceration, refractory pain, or failed conservative care. Skin breakdown at the lateral or medial malleolus with ulceration places the patient at a significant risk of osteomyelitis, and these patients should be considered for primary arthrodesis. Numerous reconstruction techniques exist, all associated with high complication rates.
Procedures range from exostectomy of bony prominences to midfoot beaming or arthrodesis and hindfoot or ankle fusion. No matter the procedure performed, the goal of surgical intervention is to restore plantigrade foot alignment and reduce the likelihood of recurrent ulceration. Ideally, surgical intervention occurs after a period of immobilization to allow inflammation to decrease.[2][23][27][29] Medical optimization, including smoking cessation, HbA1c control under 7% to 8%, and recognizing microvascular or macrovascular disease, can lessen potential complications postoperatively.[30](A1)
Differential Diagnosis
The most important differential diagnosis of Charcot is osteomyelitis as both can appear clinically and radiographically similar. Cellulitis, septic arthritis, gout, pseudogout, foot/ankle sprain or fracture, and deep vein thrombosis are also important differentials. Charcot is misdiagnosed 25% of the time, which can cause significant delay in treatment.[31][32]
Pertinent Studies and Ongoing Trials
Evidence supporting the recommended management of Charcot neuropathic osteoarthropathy emphasizes early offloading and immobilization. Randomized trials demonstrate that nonremovable knee-high devices, eg, total contact casts, significantly improve healing rates and time to remission compared with removable devices. Emerging denosumab trials targeting the RANKL pathway show early promise but remain investigational.[23]
Staging
Stages of Charcot
Common classifications that map the phases of Charcot include the Eichenholtz classification and the Sanders and Frykberg classification.
Eichenholtz classification
The Eichenholtz classification describes the following 3 stages of disease progression based on clinical and radiographic findings:
- Stage 0: pre-Charcot/prodromal
- Clinically: red, hot, swollen foot. No deformity.
- Radiographically: no changes are seen yet. Normal radiograph
- Stage I: development/destruction
- Clinically: Erythema, foot edema, elevated temperature, no pain
- Radiographically: Bony debris at joints, fragmentation of subchondral bone, joint subluxation, and/or fracture-dislocation
- Stage II: coalescence
- Clinically: Decreased signs of inflammation
- Radiographically: Worsening of stage 1 features. Absorption of bony debris with new bone formation. Coalescence of large fragments with sclerosis of bone ends. Some increased stability
- Stage III: consolidation
- Clinically: Resolution of inflammation. Changes in overall foot architecture due to underlying final bony remodeling that can lead to new pressure points, which are at risk of ulceration
- Radiographically: Remodeling of affected bones and joints [33]
Sanders and Frykberg
The Sanders and Frykberg classification is used to type and classify the following 5 common anatomical locations of Charcot in the foot:
- Metatarsophalangeal to interphalangeal joints: 15%
- Tarsometatarsal joints: 40%
- Naviculocuneiform joint, navicular-cuneiform, talonavicular, and calcaneocuboid joints: 30%
- Ankle and subtalar joints: 10%
- Calcaneus: 5% [7]
Prognosis
Prognosis depends largely on the timing of diagnosis, adherence to offloading, and metabolic control. When identified in the acute phase and managed with prompt immobilization, most patients achieve remission with preservation of a stable, plantigrade, ulcer-free foot. However, delayed or missed diagnosis can result in irreversible deformity, ulceration, recurrent infection, and a high risk of major amputation.[2][23]
Recurrence or new Charcot events occur in up to 25% to 30% of patients, often involving the contralateral limb within several years. Even with successful limb salvage, patients remain at lifelong risk for ulcer recurrence and reactivation, particularly if neuropathy, peripheral arterial disease, or poor glycemic control persist.[17][23]
Complications
Charcot neuropathic osteoarthropathy carries a high risk of long-term complications when not recognized and treated early. Progressive osseous destruction and joint instability lead to collapse of the foot architecture, resulting in the classic rocker-bottom deformity and altered biomechanics that redistribute plantar pressures to abnormal weight-bearing areas. These structural changes markedly increase the risk of skin breakdown, ulceration, infection, and eventual osteomyelitis.[2][9]
Soft-tissue and infectious complications are common. Chronic ulceration can progress to deep infection or sepsis, often necessitating partial or major amputation if not promptly controlled. Recurrent Charcot activity may occur in the same or contralateral limb, particularly if adherence to offloading is poor or metabolic control remains suboptimal.[10][5]
Offloading and immobilization may result in skin breakdown, pressure ulcers, joint stiffness, muscle atrophy, and deep vein thrombosis due to prolonged immobilization. Regular cast changes, skin inspection, and early therapy following remission are recommended.[23] Postsurgical complications include wound dehiscence, delayed union or nonunion, hardware failure, and recurrent ulceration, especially in patients with neuropathy or vascular compromise. Persistent edema and deformity can also impair balance, contributing to falls and mobility loss.[34][5] Complications may eventually result in limb amputation, which carries a 5-year mortality rate approaching 45% to 50%. Early detection, strict immobilization, glycemic optimization, and coordinated interprofessional management remain essential.[10][35]
Postoperative and Rehabilitation Care
Postoperative care starts with the immediate postoperative phase (0–8 weeks). Strict non-weight-bearing immobilization is mandatory to protect fixation and prevent reactivation of Charcot changes. A total contact cast or rigid knee-high immobilizer is typically used. Careful wound surveillance is critical, particularly in patients with neuropathy or vascular compromise.[34]
After radiographic and clinical signs of consolidation (decreased edema, normalized temperature, and stable alignment), the patient transitions to protected partial weight-bearing in a Charcot Restraint Orthotic Walker (CROW) boot or a custom-molded device. This typically occurs approximately 16 weeks after surgery. Weight-bearing radiographs guide the timing of progression.[36][23]
Once full weight bearing is achieved, the goal shifts to lifelong mechanical protection and functional restoration. Patients are fitted with custom shoes, orthotic inserts, and rocker-bottom soles to redistribute plantar pressures. Structured physical therapy focuses on proprioceptive retraining, balance, and gait correction to reduce falls and contralateral limb injury. Regular follow-up every 3 to 6 months, including skin inspection, callus management, and temperature monitoring, is advised.[23]
Consultations
Interprofessional care, including orthopaedic/podiatric surgery, endocrinology/diabetes education, vascular medicine, ID, wound care, and rehabilitation, is essential to optimize glycemic control, offloading adherence, nutritional status, smoking cessation, and surveillance to prevent reactivation.
Deterrence and Patient Education
Preventing Charcot neuropathic osteoarthropathy and its complications requires early detection as well as patient compliance and education. Most important is patient awareness of neuropathy-related risk. Patients with diabetes and sensory loss must be taught to recognize early warning signs, eg, unexplained warmth, redness, or swelling of the foot, even in the absence of pain. Prompt reporting of these symptoms enables early intervention before irreversible deformity occurs.[2]
Additionally, patients should be counseled on the importance of daily foot inspection, temperature monitoring (using an infrared thermometer or a touch comparison), and consistent use of prescribed offloading or protective footwear. Education should also emphasize glycemic control, smoking cessation, and regular follow-up with an interprofessional foot care team.[23][27]
Enhancing Healthcare Team Outcomes
Charcot neuropathic osteoarthropathy is a progressive, limb-threatening condition arising in patients with peripheral neuropathy, most commonly due to long-standing diabetes. Loss of protective sensation, impaired proprioception, and autonomic dysfunction allow repetitive microtrauma to go unnoticed, triggering inflammation, rapid bone resorption, and joint instability. Early clinical signs often mimic infection, delaying diagnosis and increasing risk of deformity, ulceration, and amputation. Prompt recognition, immediate immobilization, and coordinated, evidence-based care are critical to preserving foot structure and function while minimizing long-term complications. Interprofessional management, guided by standardized care pathways, ensures timely intervention and optimized outcomes for high-risk patients.
Effective care requires the collaboration of multiple health professionals, each contributing specific expertise. Physicians and advanced practitioners lead early recognition, order imaging, and initiate immobilization. Nurses and wound-care teams perform ongoing skin and cast assessments, monitor for pressure injuries, and educate patients on DVT and fall prevention. Pharmacists optimize glycemic control, reconcile medications, and monitor renal function and drug-device interactions. Orthotists provide custom offloading devices to maintain a plantigrade, ulcer-free foot, while physical and occupational therapists restore mobility, gait, and home safety. Coordinated interprofessional communication and shared responsibilities enhance patient-centered care, improve safety, and strengthen overall team performance in managing this complex condition.
Media
(Click Image to Enlarge)
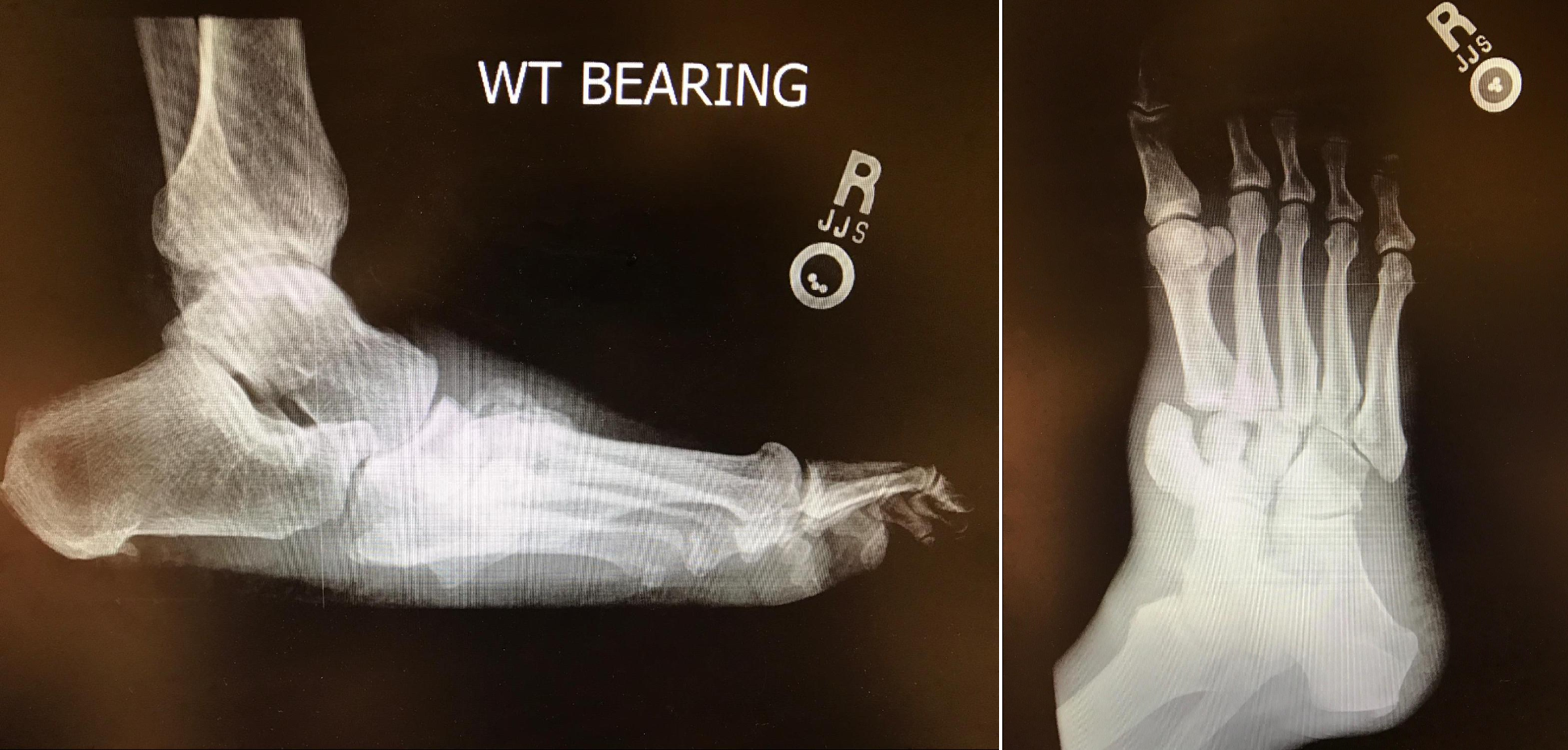
Charcot Neuropathic Osteoarthropathy. Lateral and oblique foot radiographs demonstrating Charcot foot of the midfoot. Note the osseous dislocations, destruction, debris, and rocker-bottom deformity.
Contributed by MA Dreyer, DPM, FACFAS
References
Pinzur MS. Current concepts review: Charcot arthropathy of the foot and ankle. Foot & ankle international. 2007 Aug:28(8):952-9 [PubMed PMID: 17697664]
Rogers LC, Frykberg RG, Armstrong DG, Boulton AJ, Edmonds M, Van GH, Hartemann A, Game F, Jeffcoate W, Jirkovska A, Jude E, Morbach S, Morrison WB, Pinzur M, Pitocco D, Sanders L, Wukich DK, Uccioli L. The Charcot foot in diabetes. Diabetes care. 2011 Sep:34(9):2123-9. doi: 10.2337/dc11-0844. Epub [PubMed PMID: 21868781]
Dardari D. An overview of Charcot's neuroarthropathy. Journal of clinical & translational endocrinology. 2020 Dec:22():100239. doi: 10.1016/j.jcte.2020.100239. Epub 2020 Oct 28 [PubMed PMID: 33251117]
Level 3 (low-level) evidenceJeffcoate WJ, Game F, Cavanagh PR. The role of proinflammatory cytokines in the cause of neuropathic osteoarthropathy (acute Charcot foot) in diabetes. Lancet (London, England). 2005 Dec 10:366(9502):2058-61 [PubMed PMID: 16338454]
Argyropoulos M, Wynell-Mayow W, Johnson O, Faroug R, Johal KS, Deol RS, Hakmi A, Mordecai S. Charcot neuro-osteoarthropathy: a review of key concepts and an evidence-based surgical management algorithm. Frontiers in clinical diabetes and healthcare. 2024:5():1344359. doi: 10.3389/fcdhc.2024.1344359. Epub 2024 Aug 16 [PubMed PMID: 39219847]
Svendsen OL, Rabe OC, Winther-Jensen M, Allin KH. How Common Is the Rare Charcot Foot in Patients With Diabetes? Diabetes care. 2021 Apr:44(4):e62-e63. doi: 10.2337/dc20-2590. Epub 2021 Feb 1 [PubMed PMID: 33526427]
Rosskopf AB, Loupatatzis C, Pfirrmann CWA, Böni T, Berli MC. The Charcot foot: a pictorial review. Insights into imaging. 2019 Aug 5:10(1):77. doi: 10.1186/s13244-019-0768-9. Epub 2019 Aug 5 [PubMed PMID: 31385060]
Salini D, Harish K, Minnie P, Sundaram KR, Arun B, Sandya CJ, Mangalanandan TS, Vivek L, Praveen VP. Prevalence of Charcot Arthropathy in Type 2 Diabetes Patients Aged over 50 Years with Severe Peripheral Neuropathy: A Retrospective Study in a Tertiary Care South Indian Hospital. Indian journal of endocrinology and metabolism. 2018 Jan-Feb:22(1):107-111. doi: 10.4103/ijem.IJEM_257_17. Epub [PubMed PMID: 29535947]
Level 2 (mid-level) evidenceKaynak G, Birsel O, Güven MF, Oğüt T. An overview of the Charcot foot pathophysiology. Diabetic foot & ankle. 2013:4():. doi: 10.3402/dfa.v4i0.21117. Epub 2013 Aug 2 [PubMed PMID: 23919113]
Level 3 (low-level) evidenceGouveri E, Papanas N. Charcot osteoarthropathy in diabetes: A brief review with an emphasis on clinical practice. World journal of diabetes. 2011 May 15:2(5):59-65. doi: 10.4239/wjd.v2.i5.59. Epub [PubMed PMID: 21691556]
Petrova NL, Dew TK, Musto RL, Sherwood RA, Bates M, Moniz CF, Edmonds ME. Inflammatory and bone turnover markers in a cross-sectional and prospective study of acute Charcot osteoarthropathy. Diabetic medicine : a journal of the British Diabetic Association. 2015 Feb:32(2):267-73. doi: 10.1111/dme.12590. Epub 2014 Oct 17 [PubMed PMID: 25251588]
Level 2 (mid-level) evidenceBaumhauer JF, O'Keefe RJ, Schon LC, Pinzur MS. Cytokine-induced osteoclastic bone resorption in charcot arthropathy: an immunohistochemical study. Foot & ankle international. 2006 Oct:27(10):797-800 [PubMed PMID: 17054880]
Ndip A, Williams A, Jude EB, Serracino-Inglott F, Richardson S, Smyth JV, Boulton AJ, Alexander MY. The RANKL/RANK/OPG signaling pathway mediates medial arterial calcification in diabetic Charcot neuroarthropathy. Diabetes. 2011 Aug:60(8):2187-96. doi: 10.2337/db10-1220. Epub 2011 Jun 9 [PubMed PMID: 21659498]
Mabilleau G, Edmonds ME. Role of neuropathy on fracture healing in Charcot neuro-osteoarthropathy. Journal of musculoskeletal & neuronal interactions. 2010 Mar:10(1):84-91 [PubMed PMID: 20190384]
Sono T, Meyers CA, Miller D, Ding C, McCarthy EF, James AW. Overlapping features of rapidly progressive osteoarthrosis and Charcot arthropathy. Journal of orthopaedics. 2019 May-Jun:16(3):260-264. doi: 10.1016/j.jor.2019.02.015. Epub 2019 Mar 12 [PubMed PMID: 30936675]
La Fontaine J, Shibuya N, Sampson HW, Valderrama P. Trabecular quality and cellular characteristics of normal, diabetic, and charcot bone. The Journal of foot and ankle surgery : official publication of the American College of Foot and Ankle Surgeons. 2011 Nov-Dec:50(6):648-53. doi: 10.1053/j.jfas.2011.05.005. Epub 2011 Jun 25 [PubMed PMID: 21705241]
Level 2 (mid-level) evidenceLa Fontaine J, Lavery L, Jude E. Current concepts of Charcot foot in diabetic patients. Foot (Edinburgh, Scotland). 2016 Mar:26():7-14. doi: 10.1016/j.foot.2015.11.001. Epub 2015 Nov 25 [PubMed PMID: 26802944]
Wukich DK, Sung W, Wipf SA, Armstrong DG. The consequences of complacency: managing the effects of unrecognized Charcot feet. Diabetic medicine : a journal of the British Diabetic Association. 2011 Feb:28(2):195-8. doi: 10.1111/j.1464-5491.2010.03141.x. Epub [PubMed PMID: 21219429]
Armstrong DG, Todd WF, Lavery LA, Harkless LB, Bushman TR. The natural history of acute Charcot's arthropathy in a diabetic foot specialty clinic. Diabetic medicine : a journal of the British Diabetic Association. 1997 May:14(5):357-63 [PubMed PMID: 9171250]
Level 2 (mid-level) evidencePetrova NL, Edmonds ME. Charcot neuro-osteoarthropathy-current standards. Diabetes/metabolism research and reviews. 2008 May-Jun:24 Suppl 1():S58-61. doi: 10.1002/dmrr.846. Epub [PubMed PMID: 18442182]
Bobircă A, Musetescu AE, Bordianu A, Pantea Stoian A, Salmen T, Marinescu DC, Alexandru C, Florescu A, Radu R, Isac S, Patrascu T, Serban D, Bobircă F. Novel Biomarkers Predictive of Diabetic Charcot Foot-An Overview of the Literature. Life (Basel, Switzerland). 2022 Nov 21:12(11):. doi: 10.3390/life12111944. Epub 2022 Nov 21 [PubMed PMID: 36431079]
Level 3 (low-level) evidenceJudge MS. Infection and neuroarthropathy: the utility of C-reactive protein as a screening tool in the Charcot foot. Journal of the American Podiatric Medical Association. 2008 Jan-Feb:98(1):1-6 [PubMed PMID: 18202327]
Wukich DK, Schaper NC, Gooday C, Bal A, Bem R, Chhabra A, Hastings M, Holmes C, Petrova NL, Santini Araujo MG, Senneville E, Raspovic KM. Guidelines on the diagnosis and treatment of active Charcot neuro-osteoarthropathy in persons with diabetes mellitus (IWGDF 2023). Diabetes/metabolism research and reviews. 2024 Mar:40(3):e3646. doi: 10.1002/dmrr.3646. Epub 2023 May 23 [PubMed PMID: 37218537]
Chantelau E. The perils of procrastination: effects of early vs. delayed detection and treatment of incipient Charcot fracture. Diabetic medicine : a journal of the British Diabetic Association. 2005 Dec:22(12):1707-12 [PubMed PMID: 16401316]
Ahluwalia R, Bilal A, Petrova N, Boddhu K, Manu C, Vas P, Bates M, Corcoran B, Reichert I, Mulholland N, Kavarthapu V, Vivian G, Edmonds M. The Role of Bone Scintigraphy with SPECT/CT in the Characterization and Early Diagnosis of Stage 0 Charcot Neuroarthropathy. Journal of clinical medicine. 2020 Dec 21:9(12):. doi: 10.3390/jcm9124123. Epub 2020 Dec 21 [PubMed PMID: 33371286]
Bus SA, Armstrong DG, Gooday C, Jarl G, Caravaggi C, Viswanathan V, Lazzarini PA, International Working Group on the Diabetic Foot (IWGDF). Guidelines on offloading foot ulcers in persons with diabetes (IWGDF 2019 update). Diabetes/metabolism research and reviews. 2020 Mar:36 Suppl 1():e3274. doi: 10.1002/dmrr.3274. Epub [PubMed PMID: 32176441]
Raspovic KM, Schaper NC, Gooday C, Bal A, Bem R, Chhabra A, Hastings M, Holmes C, Petrova NL, Santini Araujo MG, Senneville E, Wukich DK. Diagnosis and treatment of active charcot neuro-osteoarthropathy in persons with diabetes mellitus: A systematic review. Diabetes/metabolism research and reviews. 2024 Mar:40(3):e3653. doi: 10.1002/dmrr.3653. Epub 2023 May 14 [PubMed PMID: 37179484]
Level 1 (high-level) evidenceGreenhagen RM, Frykberg RG, Wukich DK. Serum vitamin D and diabetic foot complications. Diabetic foot & ankle. 2019:10(1):1579631. doi: 10.1080/2000625X.2019.1579631. Epub 2019 Feb 19 [PubMed PMID: 30815231]
Albright RH, Joseph RM, Wukich DK, Armstrong DG, Fleischer AE. Is Reconstruction of Unstable Midfoot Charcot Neuroarthropathy Cost Effective from a US Payer's Perspective? Clinical orthopaedics and related research. 2020 Dec:478(12):2869-2888. doi: 10.1097/CORR.0000000000001416. Epub [PubMed PMID: 32694315]
Level 3 (low-level) evidenceWukich DK, Crim BE, Frykberg RG, Rosario BL. Neuropathy and poorly controlled diabetes increase the rate of surgical site infection after foot and ankle surgery. The Journal of bone and joint surgery. American volume. 2014 May 21:96(10):832-9. doi: 10.2106/JBJS.L.01302. Epub [PubMed PMID: 24875024]
Level 2 (mid-level) evidenceTrieb K. The Charcot foot: pathophysiology, diagnosis and classification. The bone & joint journal. 2016 Sep:98-B(9):1155-9. doi: 10.1302/0301-620X.98B9.37038. Epub [PubMed PMID: 27587513]
Marmolejo VS, Arnold JF, Ponticello M, Anderson CA. Charcot Foot: Clinical Clues, Diagnostic Strategies, and Treatment Principles. American family physician. 2018 May 1:97(9):594-599 [PubMed PMID: 29763252]
Rosenbaum AJ, DiPreta JA. Classifications in brief: Eichenholtz classification of Charcot arthropathy. Clinical orthopaedics and related research. 2015 Mar:473(3):1168-71. doi: 10.1007/s11999-014-4059-y. Epub 2014 Nov 21 [PubMed PMID: 25413713]
Wukich DK, Raspovic KM, Hobizal KB, Sadoskas D. Surgical management of Charcot neuroarthropathy of the ankle and hindfoot in patients with diabetes. Diabetes/metabolism research and reviews. 2016 Jan:32 Suppl 1():292-6. doi: 10.1002/dmrr.2748. Epub [PubMed PMID: 26452590]
Armstrong DG, Swerdlow MA, Armstrong AA, Conte MS, Padula WV, Bus SA. Five year mortality and direct costs of care for people with diabetic foot complications are comparable to cancer. Journal of foot and ankle research. 2020 Mar 24:13(1):16. doi: 10.1186/s13047-020-00383-2. Epub 2020 Mar 24 [PubMed PMID: 32209136]
Schaper NC, van Netten JJ, Apelqvist J, Bus SA, Fitridge R, Game F, Monteiro-Soares M, Senneville E, IWGDF Editorial Board. Practical guidelines on the prevention and management of diabetes-related foot disease (IWGDF 2023 update). Diabetes/metabolism research and reviews. 2024 Mar:40(3):e3657. doi: 10.1002/dmrr.3657. Epub 2023 May 27 [PubMed PMID: 37243927]
Level 3 (low-level) evidence