Introduction
The neurohypophysis (pars posterior) is the posterior lobe of the pituitary gland, located at the base of the brain. The embryological origin of this structure is the neuroectodermal infundibulum. The neurohypophysis comprises 2 primary regions, the pars nervosa and the infundibular stalk. The pars intermedia and median eminence are sometimes included. The neurohypophysis secretes the 2 peptide hormones, oxytocin and vasopressin. Oxytocin stimulates uterine contractions and milk ejection. Vasopressin, also known as antidiuretic hormone (ADH), prevents diuresis.[1] These hormones are synthesized by magnocellular neurosecretory cells of the hypothalamus, specifically within the paraventricular and supraoptic nuclei. Axons from these neurons project to the neurohypophysis, transporting the hormones for storage and subsequent release into the neurohypophyseal capillaries, which deliver these neuropeptides to systemic circulation.[2]
Dysfunction of the posterior pituitary disrupts hormonal homeostasis, causing arginine vasopressin deficiency (AVP-D) and the syndrome of inappropriate antidiuresis (SIAD). Disorders resulting from oxytocin deficiency are rare and primarily associated with pregnancy, lactation difficulties, osteopenia, and hyperphagia.[3]
The posterior pituitary contains pituicytes. In the pars nervosa, these cells function as glial cells, providing structural support and modulating hormone release.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Etiology
Several etiologies contribute to neurohypophyseal dysfunction. These factors disrupt hormone synthesis, transport, or release, leading to impaired posterior pituitary function.
Neoplastic causes include pituitary adenoma, hypothalamic glioma, craniopharyngioma, pituicytoma, granular cell tumors, and germ cell tumors. These lesions may compress or infiltrate the hypothalamic–neurohypophyseal axis, impairing hormone synthesis, transport, or release.
Traumatic brain injury (TBI) may disrupt hypothalamic or pituitary connections, leading to impaired neurohypophyseal function. Brain surgery represents an iatrogenic cause, with potential damage to the pituitary stalk or surrounding structures. Radiation exposure may similarly result in delayed injury to neuroendocrine tissues.
Inflammatory causes include sarcoidosis, multiple sclerosis, pituitary hypophysitis, Langerhans cell histiocytosis, and hemochromatosis. These conditions involve infiltration or immune-mediated damage to the hypothalamic–pituitary axis, resulting in hormonal dysregulation.
Infectious etiologies include meningitis, encephalitis, acquired immunodeficiency syndrome, abscess, septic shock, and subarachnoid hemorrhage. These processes may directly injure neurohypophyseal structures or disrupt vascular supply.
Hypoxic and vascular insults include Sheehan syndrome, pituitary apoplexy, cardiac arrest, and hydrocephalus. Reduced perfusion or increased intracranial pressure may impair posterior pituitary function. Anorexia may also contribute through metabolic and hypothalamic dysregulation. Aneurysm of the anterior communicating artery may compress adjacent neuroendocrine structures.
Congenital causes include pituitary stalk interruption syndrome, characterized by abnormal development of the hypothalamic–pituitary connection. Genetic disorders such as Prader–Willi syndrome and multiple endocrine neoplasia type 1 may involve hypothalamic or pituitary dysfunction through inherited mechanisms.
Pharmacologic etiologies include phenothiazines, carbamazepine, valproic acid, omeprazole, selective serotonin reuptake inhibitors, morphine, 3,4-methylenedioxymethamphetamine (ecstasy), vincristine, amitriptyline, immune checkpoint inhibitors, opioids, and megestrol acetate. These agents may alter the secretion or action of neurohypophyseal hormones through central or peripheral mechanisms.
Epidemiology
Disorders of the neurohypophysis have variable etiologies that affect populations from a young age to late adulthood; the etiology influences the condition's frequency. The prevalence of hypopituitarism is 29 to 45 per 100,000, with an incidence of 4.2 new cases per 100,000 per person per year, with no gender predominance.[4] Most studies evaluate the dysfunction of the entire pituitary gland.
In AVP-D, the reported incidence after traumatic brain injury (TBI) is between 3 to 50%. Its frequency varies widely, as the diagnostic parameter used in each study may underestimate its true incidence. Hyponatremia affects 15% of hospitalized patients. The SIADH secretion causing hyponatremia has been reported as the most common abnormality following a TBI in children and adults.[5] SIADH secretion is responsible for 46% of the cases of hyponatremia, which is the most common electrolyte abnormality in outpatient practise. For some neurological conditions, the presentation of SIAD is more than 70%. In neurosurgical units, SIADH occurs in 5% to 10% of cases due to disorders of the posterior neurohypophysis.[6]
The neurohypophysis is a popular site for germinomas, which are most commonly found in the pineal region. Presentation in the neurohypophyseal/pineal region is common in germinomas. Half of the patients with a combined tumor at the pineal and pituitary gland are germinomas.[7]
Pituitary stalk interruption syndrome presents with a triad that consists of the ectopic posterior pituitary, thin or absent pituitary stalk, and anterior pituitary hypoplasia. AVP-D occurs in up to 10% of cases. It is more prevalent in males (2:1). In patients with hypopituitarism, it can be the etiology in 4-8% of cases.[8][9][10][11][12][13]
Granular cell tumors arise primarily in the neurohypophysis and have been discovered in 9% of routine neurohypophysis autopsy specimens.[14][15] They are considered to be unique neoplasms of the neurohypophysis and pituitary stalk; they have been suggested to derive from pituicytes. They occur more frequently in women than in men (2:1).[16][17] Granular cell tumors comprise 0.17 % of resected sellar lesions in major transsphenoidal series.[18]
Sheehan syndrome is more prevalent in developing countries and is estimated to occur in approximately 3.1% of parous women, with home delivery being more common. Sheehan syndrome causes 6-8% of all causes of hypopituitarism.
Pathophysiology
The neurohypophysis secretes two neurohormones: oxytocin, which increases uterine contractions, and vasopressin, which increases water reabsorption by the distal tubules of the kidney. These hormones are packaged in secretory vesicles and granules within magnocellular neurosecretory cells in the hypothalamus. They are released from the paraventricular and supraoptic nuclei of the hypothalamus and travel down axons of magnocellular cells to the neurohypophysis.[19]
The hormones are then stored in the herring bodies of the neurohypophysis, which are the terminal ends of the axons. Upon release from the herring bodies, action potentials are produced, activating voltage-gated channels that allow calcium to enter and trigger the release of the hormone into the neurohypophyseal capillaries, which then transport the hormone into the systemic circulation. Predominantly, the paraventricular nucleus is related to oxytocin secretion, while the supraoptic nucleus is concerned with vasopressin secretion. Small amounts of each hormone are also produced at the other nuclei. The release of these hormones is triggered by afferent stimuli from neurons projecting to the magnocellular neurons of the hypothalamus.
The neurohypophysis receives its blood supply from the inferior hypophyseal artery, a branch of the cavernous internal carotid (ICA) artery. The cavernous ICA has a dorsal trunk, the meningohypophyseal trunk, which gives rise to 3 terminal branches: the inferior hypophyseal artery, the tentorial artery (artery of Bernasconi and Cassinari), and the dorsal meningeal artery. Venous drainage of the posterior pituitary gland is by the short portal and hypophyseal veins into the cavernous sinus.
Sheehan syndrome can develop AVP-D and hypernatremia due to ischemic necrosis damage to the posterior gland, causing impaired vasopressin secretion. Hyponatremia can also occur due to an increased ADH secretion as a response to hypotension and reduced cardiac output owing to glucocorticoid deficiency. Also, the cortisol deficit stimulated the secretion of corticotropin-releasing hormone, which further stimulates the ADH secretion.[20]
During septic shock, vasopressin secretion undergoes a biphasic pattern. Initially, there is an increased secretion to maintain homeostasis, but later, when hypotension is pronounced, there is an unexpected, significant decrease in the secretion. This decrease is thought to result from depletion of vasopressin stores in the neurohypophysis, autonomic dysfunction, and nitric oxide-mediated inhibition of secretion in the hypothalamus.[21]
In TBI, AVP-D is caused by direct damage to the neurohypophysis, pituitary stalk, hypothalamic nuclei, or the vascular supply, or by traumatic edema in the neurohypophysis or hypothalamus. These changes are usually reversible, but irreversible changes with gliosis can cause permanent DI.[22][23]
Histopathology
The neurohypophysis is made of the axons arising predominantly from magnocellular neurons of the supraoptic and paraventricular nuclei of the hypothalamus. They form the hypothalamohypophyseal tract, and these axons terminate near the sinusoids of the posterior lobe. The neurosecretory granules mostly contain oxytocin or vasopressin. The axon terminals are supported by pituicytes, which express the Thyroid transcription factor (TTF)-1 and demonstrate only patchy GFAP and S100 expression.[24]
Clinical Significance
History and Physical
For patients presenting with disorders of neurohypophysis, obtaining a detailed history, including previous medication, is prudent. It is essential to assess recent medical history for depression, psychosis, seizures, or cancer because some antidepressants, anticonvulsants, antipsychotic agents, and cytotoxic agents can cause SIADH secretion. Any previous history of stroke, malignancy, or trauma to the head should be obtained in detail. For patients who are unable to provide their history, questioning how the patient was immediately before the episode is essential. The most common presentation of SIAD is hyponatremia with euvolemic fluid status, with clinical features including normal blood pressure, regular heart rate, normal skin turgor, moist mucous membranes, absent jugular venous pulsations, no pitting edema, and normal central venous pressure if measured. Clinical manifestations include nausea, vomiting, restlessness, headache, lethargy, obtundation, seizures, coma, and respiratory arrest. These manifestations progress as the level of hyponatremia advances from mild to severe.
In a presentation of AVP-D due to neurohypophysis dysfunction, it is essential to rule out other acquired etiologies, as treatment should address the primary etiology causing the symptoms. Neurosurgery is the most common cause, and these patients should be closely monitored. There is a triphasic presentation in these cases post-surgery: AVP-D in the first 48 hours, SIAD from day 3 to 7, and permanent AVP-D.[25] The most common symptoms of AVP-D include polyuria and polydipsia, with patients complaining of increased thirst that, at first, can be controlled by increasing water intake to maintain normal serum osmolality and volume status. Some patients with altered neurological status will not recognize the thirst sensation and will not be able to drink water, developing free water deficiency with hyperosmolarity, hypernatremia, and signs of dehydration that can progress to hypertonic encephalopathy with irritability, confusion, disorientation, muscle twitching, seizures, coma, and death. Other symptoms include weakness, fatigue, and myalgias.
Some patients may develop acute kidney failure, hypotension, muscle damage, and even hepatic failure. There is an increased incidence of subarachnoid hemorrhage, strokes, and deep vein thrombosis in the setting of hyperosmolar states.[26] Adipsic AVP-D is a condition that is crucial to recognize because patients lack the sensation of thirst. It is caused by infarction of the anterior hypothalamus, where osmoreceptors are located, impairing their normal homeostatic thirst mechanism despite the symptoms of AVP-D.[27] Despite being dehydrated, the patient will not drink an adequate amount of water.
Evaluation
When a patient presents with a disorder of the neurohypophysis, its manifestation is most commonly related to a disorder of the antidiuretic hormone. Antidiuretic hormone acts on the distal collecting duct, increasing free water reabsorption and promoting indirect sodium excretion. Any disturbances related to this hormone can create sodium electrolyte abnormalities.
Brain magnetic resonance imaging, the gold standard for visualizing the anterior and posterior pituitary, should be ordered to identify or rule out possible etiologies that can cause neurohypophysis dysfunction.
AVP Deficiency
Serum and urine sodium and osmolality, hourly urine output, 24-hour urine volume, and specific gravity must be obtained. AVP-D must be distinguished from AVP-R(Arginine Vasopressin Resistance, formerly known as Nephrogenic DI). A water deprivation test can be used with or without desmopressin injection. In AVP-D, the vasopressin will correct urine osmolality, while in AVP-R, the correction will be suboptimal.[28][29]
Criteria for the diagnosis of AVP-D:
- Polyuria in two consecutive hours of > 300 ml/hr or 4 to 5 ml/kg/hr in two consecutive hours
- Polyuria > 3L/24 hours or > 2ml/kg/hr in 24 hours
- Serum osmolality > 295 mOsm/kg
- Urine osmolality < 300 mOsm/kg
- Urine/plasma osmolality < 1
- The specific gravity is <1.005
- Serum sodium: >145 mmol/L
SIAD
The first step is to assess the fluid status and obtain laboratory tests to evaluate serum and urine sodium, serum and urine osmolality, blood sugar, potassium levels, and liver function. When SIAD is suspected, it is important to order thyroid-stimulating hormone and thyroxine levels (TSH/T4) and serum cortisol to rule out thyroid and glucocorticoid hormone deficiency. The most common presentation in SIAD is hyponatremia with a euvolemic fluid status. Patients will have decreased plasma osmolality and increased sodium excretion.[30][31] Other causes of hyponatremia (adrenal insufficiency, hypothyroidism, cardiac failure, hepatic damage, renal disease, pituitary dysfunction, drugs) must be excluded.
Criteria for the diagnosis of SIADH secretion:
- Serum sodium < 135 mEq/L
- Serum osmolality < 275 mOsm/kg
- Urine osmolality > 100 mOsm/kg
- Urine sodium > 30 mEq/L
- Normal dietary and water intake
- No recent use of diuretic agents
- Correction of the deficit with fluid restriction
- No signs of edema, heart failure, or renal dysfunction [32][33]
Treatment / Management
AVP-D
The medication recommended in the acute and chronic setting of AVP-D is desmopressin.[34][35] Desmopressin, D-amino D-arginine vasopressin (DDAVP), is given intranasally, orally, and intravenously with a half-life of 2 to 4 hours. It is crucial to establish the dose that improves the patient's polyuria and polydipsia without compromising plasma electrolytes. The water loss must be replaced. In acute DI after a TBI, it is mandatory to evaluate if the patient is conscious or unconscious. If the patient is conscious, encourage drinking. If the patient cannot drink, enforce fluid intake via nasogastric tube, guided by daily weight measurements. If the patient is unconscious, a 5% dextrose intravenous solution is administered. Treatment with DDAVP is administered at 10 mcg by nasal puff, or 0.4 to 4 mcg subcutaneously or intravenously. Maintenance is usually by 1 to 2 nasal puffs every 12 hours. Hypokalemia, if present, must be corrected. Urine volume, fluid balance, urine osmolality, plasma osmolality, and serum electrolytes must be monitored. The goal is to balance electrolytes and to have normal urine output. After desmopressin is given, it is essential to monitor sodium levels. In the management of hypernatremia in AVP-D, it is vital to use dextrose or nasogastric water at a rate that lowers plasma sodium concentration by 0.5 mEq/L/hr or less.
SIAD
Offending drugs or etiology should be treated first. Fluid restriction is the primary treatment for SIAD. Fluids should be reduced to 800 to 1000 mL/day. The correction should aim to reach a serum sodium of 130 mEq/L. If hyponatremia persists, patients could receive salt tablets and furosemide 20 mg twice a day. Isotonic fluids will not correct the deficit; therefore, 3% hypertonic (513 mOsm/kg) should be given for severe hypernatremia. A 100 mL bolus is given over 3 hours, and a repeat bolus may be given as needed based on serum electrolytes. In TBI, hypertonic saline will also help to reduce intracranial pressure. Correction should not be more than 8 mEq/L over 24 hours or 0.5 to 1 mEq/L per hour to prevent osmotic demyelination syndrome. The AVP receptor antagonists produce a selective water diuresis (aquaresis) without affecting sodium and potassium excretion. For persistent hyponatremia, oral tolvaptan or intravenous conivaptan, both vasopressin V2 receptor antagonists, are administered. Tolvaptan is hepatotoxic and can not be given to patients with liver disease. Demeclocycline, which is a tetracycline vasopressin inhibitor, can be given but can produce side effects of reversible azotemia, cirrhosis, and photosensitive skin rashes.[36] Urea has also been used to reduce natriuresis and has been comparable to vaptans in reversing hyponatremia in SIADH.
Differential Diagnosis
- Polydipsia
- Water intoxication
- Hypovolemia
- Arginine Vasopressin Resistance
- Congestive heart failure
- Cirrhosis
- Uncontrolled diabetes mellitus
- Chronic nausea/vomiting
- Cerebral salt wasting syndrome
- SIADH secretion
- Inappropriate intravenous therapy
- Glucocorticoid deficiency
- Hypothyroidism
- Pseudohyponatremia (hyperglycemic and hyperlipidemic patients)
- Drugs that affect ADH (carbamazepine, oxcarbazepine, chlorpropamide, cyclophosphamide, and selective serotonin reuptake inhibitors)
- Small-cell lung cancer
- Non-pulmonary tumors secreting ADH-like substances
- Hypercalcemia
- Hypokalemia
- Histiocytosis
Prognosis
The prognosis for AVP-D is excellent after the primary cause is treated. Hypernatremia can lead to cerebral herniation due to an increase in intracranial pressure. When AVP-D has been diagnosed in trauma patients, the majority recover in 2 to 4 days, and the remaining few recover during a 6-month timeframe, which provides good patient outcomes. Permanent AVP-D after TBI has a prevalence of 6%. Acute onset of AVP-D in TBI increases the mortality rate.
For acute SIAD, the prognosis is related to the level of hyponatremia and its response to treatment. Hyponatremia is a major contributing factor to severe morbidity and mortality. The management of SIAD is complex, and water restriction does not always correct the hyponatremia, requiring further investigations and second-line treatments.
Complications
Potential complications include the following:
- Hyponatremia
- Hypernatremia
- Confusion
- Seizures
- Muscle twitching
- Lethargy
- Coma
- Death
- Lack of breastfeeding
- Poor uterine contraction
- Poor cervical dilatation
- Poor sexual response
- Depression
Deterrence and Patient Education
The management of a patient with disorders of the neurohypophysis can be challenging in the hospital setting. In certain situations, complications can be avoided with early recognition of symptoms and close monitoring. The presentation due to sodium abnormalities can be varied but can progress to coma and death if untreated. The patient must be aware of any changes in urine volume or an increase in thirst sensation. The patient needs to recognize polyuria, increased thirst sensation, muscle weakness, twitching, and confusion. In the presence of any of those symptoms, immediate contact with the primary physician is recommended for further assessment and evaluation.
Enhancing Healthcare Team Outcomes
Disorders of the neurohypophysis frequently present a diagnostic dilemma. Patients may exhibit non-specific signs and symptoms such as vomiting, nausea, hypernatremia, hyponatremia, and diuresis. The cause of neurohypophysis disorders can be multiple, including tumoral, traumatic, inflammatory, infectious, and metabolic etiologies. The etiology is difficult to determine without a thorough history and imaging studies.
The primary physician is usually responsible for the initial evaluation of the patient. The physician will determine whether it is an emergency or non-emergency situation, which depends on the presenting symptoms. Usually, an acute presentation is associated with more aggressive symptoms and treatment, while a chronic presentation can be managed more conservatively. The management will also depend on the type of neurohypophysis disorder.
While an endocrinologist is almost always involved in the care of patients with disorders of the neurohypophysis, it is essential to consult an interprofessional team of specialists, including a neurosurgeon and a neurologist. The nurses are also vital members of the interprofessional group, as they will monitor the patient's vital signs and assist with patient and family education. The pharmacist will provide analgesics, antiemetics, appropriate antibiotics, antiepileptics, and antidiuretic medications. The neuroradiologist can assist in determining the cause. Women of childbearing age presenting with disorders of the neurohypophysis can experience issues during labor and later with breastfeeding.
The outcomes of neurohypophyseal disorders depend on the cause. However, to improve outcomes, prompt consultation with an interprofessional group of specialists is recommended. The care provided to the patient must use an integrated care pathway, combined with an evidence-based approach to planning and evaluating activities.
Media
(Click Image to Enlarge)
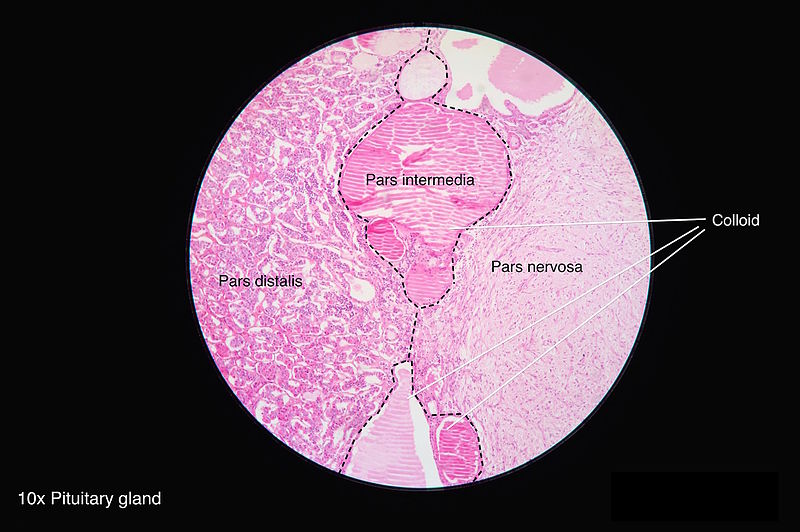
Microscopic Anatomy of the Hypophysis. Light micrograph at 10 times magnification demonstrates the distinct cellular regions of the hypophysis. The pars distalis represents the glandular anterior lobe, characterized by a dense population of chromophils and chromophobes. Centrally located, the pars intermedia contains follicles filled with colloid, serving as the boundary between the anterior and posterior sections. The pars nervosa appears as a paler, fibrous region composed of unmyelinated axons and pituicytes, forming the bulk of the posterior lobe.
Contributed by Wikimedia Commons (CC by 4.0) https://creativecommons.org/licenses/by/4.0/
(Click Image to Enlarge)
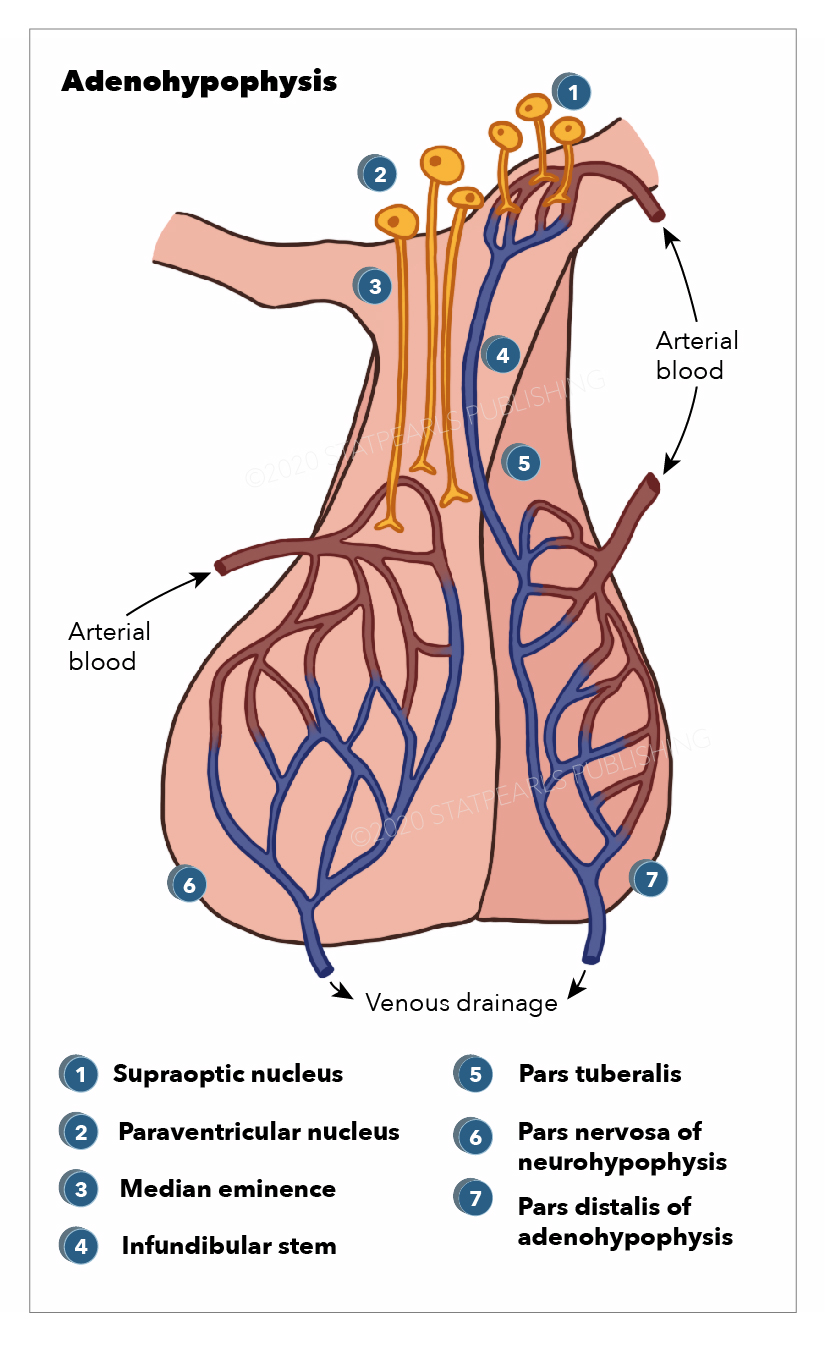
Anatomy, Adenohypophysis. Pars distalis of adenohypophysis, pars nervosa of neurohypophysis, pars tuberalisInfundibular stem, median eminence, paraventricular nucleus, and supraoptic nucleus.
Illustration by E Gregory
References
Iwasaki Y, Yamaguchi Y, Nishiyama M. Structure and function of neurohypophysial hormones. Peptides. 2024 Dec:182():171300. doi: 10.1016/j.peptides.2024.171300. Epub 2024 Oct 10 [PubMed PMID: 39395442]
Amar AP, Weiss MH. Pituitary anatomy and physiology. Neurosurgery clinics of North America. 2003 Jan:14(1):11-23, v [PubMed PMID: 12690976]
Aulinas A, Lawson EA. The Oxytocin System and Implications for Oxytocin Deficiency in Hypothalamic-Pituitary Disease. Endocrine reviews. 2025 Jul 15:46(4):518-548. doi: 10.1210/endrev/bnaf008. Epub [PubMed PMID: 39985439]
Regal M, Páramo C, Sierra SM, Garcia-Mayor RV. Prevalence and incidence of hypopituitarism in an adult Caucasian population in northwestern Spain. Clinical endocrinology. 2001 Dec:55(6):735-40 [PubMed PMID: 11895214]
Level 2 (mid-level) evidenceTudor RM, Thompson CJ. Posterior pituitary dysfunction following traumatic brain injury: review. Pituitary. 2019 Jun:22(3):296-304. doi: 10.1007/s11102-018-0917-z. Epub [PubMed PMID: 30334138]
Cuesta M, Thompson CJ. The syndrome of inappropriate antidiuresis (SIAD). Best practice & research. Clinical endocrinology & metabolism. 2016 Mar:30(2):175-87. doi: 10.1016/j.beem.2016.02.009. Epub 2016 Feb 27 [PubMed PMID: 27156757]
Takami H, Graffeo CS, Perry A, Giannini C, Daniels DJ. Epidemiology, natural history, and optimal management of neurohypophyseal germ cell tumors. Journal of neurosurgery. 2021 Feb 1:134(2):437-445. doi: 10.3171/2019.10.JNS191136. Epub 2020 Feb 7 [PubMed PMID: 32032947]
Ruszała A, Wójcik M, Krystynowicz A, Starzyk J. Distinguishing between post-trauma pituitary stalk disruption and genetic pituitary stalk interruption syndrome - case presentation and literature overview. Pediatric endocrinology, diabetes, and metabolism. 2019:25(3):155-162. doi: 10.5114/pedm.2019.87708. Epub [PubMed PMID: 31769274]
Level 3 (low-level) evidenceXu C, Wang T, Feng Y. Pituitary Stalk Interruption Syndrome. The Journal of craniofacial surgery. 2019 Sep:30(6):e578-e580. doi: 10.1097/SCS.0000000000005580. Epub [PubMed PMID: 31756884]
Vergier J, Castinetti F, Saveanu A, Girard N, Brue T, Reynaud R. DIAGNOSIS OF ENDOCRINE DISEASE: Pituitary stalk interruption syndrome: etiology and clinical manifestations. European journal of endocrinology. 2019 Nov:181(5):R199-R209. doi: 10.1530/EJE-19-0168. Epub [PubMed PMID: 31480013]
Gosi SK, Kanduri S, Garla VV. Pituitary stalk interruption syndrome. BMJ case reports. 2019 Apr 14:12(4):. doi: 10.1136/bcr-2019-230133. Epub 2019 Apr 14 [PubMed PMID: 30988112]
Level 3 (low-level) evidenceLichiardopol C, Albulescu DM. PITUITARY STALK INTERRUPTION SYNDROME: REPORT OF TWO CASES AND LITERATURE REVIEW. Acta endocrinologica (Bucharest, Romania : 2005). 2017 Jan-Mar:13(1):96-105. doi: 10.4183/aeb.2017.96. Epub [PubMed PMID: 31149155]
Level 3 (low-level) evidenceVoutetakis A. Pituitary stalk interruption syndrome. Handbook of clinical neurology. 2021:181():9-27. doi: 10.1016/B978-0-12-820683-6.00002-6. Epub [PubMed PMID: 34238482]
Schaller B, Kirsch E, Tolnay M, Mindermann T. Symptomatic granular cell tumor of the pituitary gland: case report and review of the literature. Neurosurgery. 1998 Jan:42(1):166-70; discussion 170-1 [PubMed PMID: 9442519]
Level 3 (low-level) evidenceTomita T, Gates E. Pituitary adenomas and granular cell tumors. Incidence, cell type, and location of tumor in 100 pituitary glands at autopsy. American journal of clinical pathology. 1999 Jun:111(6):817-25 [PubMed PMID: 10361519]
Cone L, Srinivasan M, Romanul FC. Granular cell tumor (choristoma) of the neurohypophysis: two cases and a review of the literature. AJNR. American journal of neuroradiology. 1990 Mar-Apr:11(2):403-6 [PubMed PMID: 2156414]
Level 3 (low-level) evidenceCohen-Gadol AA, Pichelmann MA, Link MJ, Scheithauer BW, Krecke KN, Young WF Jr, Hardy J, Giannini C. Granular cell tumor of the sellar and suprasellar region: clinicopathologic study of 11 cases and literature review. Mayo Clinic proceedings. 2003 May:78(5):567-73 [PubMed PMID: 12744543]
Level 3 (low-level) evidenceSaeger W, Lüdecke DK, Buchfelder M, Fahlbusch R, Quabbe HJ, Petersenn S. Pathohistological classification of pituitary tumors: 10 years of experience with the German Pituitary Tumor Registry. European journal of endocrinology. 2007 Feb:156(2):203-16 [PubMed PMID: 17287410]
SCHALLY AV, BOWERS CY, LOCKE W. NEUROHUMORAL FUNCTIONS OF THE HYPOTHALAMUS. The American journal of the medical sciences. 1964 Jul:248():79-101 [PubMed PMID: 14181154]
Karaca Z, Laway BA, Dokmetas HS, Atmaca H, Kelestimur F. Sheehan syndrome. Nature reviews. Disease primers. 2016 Dec 22:2():16092. doi: 10.1038/nrdp.2016.92. Epub 2016 Dec 22 [PubMed PMID: 28004764]
Giusti-Paiva A, Santiago MB. Neurohypophyseal dysfunction during septic shock. Endocrine, metabolic & immune disorders drug targets. 2010 Sep:10(3):247-51 [PubMed PMID: 20509843]
Level 3 (low-level) evidenceAgha A, Sherlock M, Phillips J, Tormey W, Thompson CJ. The natural history of post-traumatic neurohypophysial dysfunction. European journal of endocrinology. 2005 Mar:152(3):371-7 [PubMed PMID: 15757853]
Capatina C, Paluzzi A, Mitchell R, Karavitaki N. Diabetes Insipidus after Traumatic Brain Injury. Journal of clinical medicine. 2015 Jul 13:4(7):1448-62. doi: 10.3390/jcm4071448. Epub 2015 Jul 13 [PubMed PMID: 26239685]
Feingold KR, Adler RA, Ahmed SF, Anawalt B, Blackman MR, Chrousos G, Corpas E, de Herder WW, Dhatariya K, Dungan K, Hamilton E, Hofland J, Jan de Beur S, Kalra S, Kaltsas G, Kapoor N, Kim M, Koch C, Kopp P, Korbonits M, Kovacs CS, Kuohung W, Laferrère B, Levy M, McGee EA, McLachlan R, Muzumdar R, Purnell J, Rey R, Sahay R, Shah AS, Sperling MA, Stratakis CA, Trence DL, Wilson DP, Scott IS, Chattopadhyay A, Ansorge O. Development and Microscopic Anatomy of the Pituitary Gland. Endotext. 2000:(): [PubMed PMID: 28402619]
Sodoma AM, Bulba NS, Baginski M, Khan N. Triphasic Response of Pituitary Stalk Injury Secondary to Traumatic Brain Injury. Cureus. 2025 Jun:17(6):e87060. doi: 10.7759/cureus.87060. Epub 2025 Jun 30 [PubMed PMID: 40746808]
Lu HA. Diabetes Insipidus. Advances in experimental medicine and biology. 2017:969():213-225. doi: 10.1007/978-94-024-1057-0_14. Epub [PubMed PMID: 28258576]
Level 3 (low-level) evidenceDalan R, Chin H, Hoe J, Chen A, Tan H, Boehm BO, Chua KS. Adipsic Diabetes Insipidus-The Challenging Combination of Polyuria and Adipsia: A Case Report and Review of Literature. Frontiers in endocrinology. 2019:10():630. doi: 10.3389/fendo.2019.00630. Epub 2019 Sep 18 [PubMed PMID: 31620086]
Level 3 (low-level) evidenceFaltado AL, Macalalad-Josue AA, Li RJS, Quisumbing JPM, Yu MGY, Jimeno CA. Factors Associated with Postoperative Diabetes Insipidus after Pituitary Surgery. Endocrinology and metabolism (Seoul, Korea). 2017 Dec:32(4):426-433. doi: 10.3803/EnM.2017.32.4.426. Epub 2017 Nov 21 [PubMed PMID: 29199401]
Hunter JD, Calikoglu AS. Etiological and clinical characteristics of central diabetes insipidus in children: a single center experience. International journal of pediatric endocrinology. 2016:2016():3. doi: 10.1186/s13633-016-0021-y. Epub 2016 Feb 11 [PubMed PMID: 26870137]
Peri A, Grohé C, Berardi R, Runkle I. SIADH: differential diagnosis and clinical management. Endocrine. 2017 Jan:55(1):311-319. doi: 10.1007/s12020-016-0936-3. Epub 2016 Mar 30 [PubMed PMID: 27025948]
Yasir M, Mechanic OJ. Syndrome of Inappropriate Antidiuretic Hormone Secretion. StatPearls. 2026 Jan:(): [PubMed PMID: 29939554]
Silveira MAD, Seguro AC, da Silva JB, Arantes de Oliveira MF, Seabra VF, Reichert BV, Rodrigues CE, Andrade L. Chronic Hyponatremia Due to the Syndrome of Inappropriate Antidiuresis (SIAD) in an Adult Woman with Corpus Callosum Agenesis (CCA). The American journal of case reports. 2018 Nov 12:19():1345-1349. doi: 10.12659/AJCR.911810. Epub 2018 Nov 12 [PubMed PMID: 30416193]
Level 3 (low-level) evidenceBerardi R, Antonuzzo A, Blasi L, Buosi R, Lorusso V, Migliorino MR, Montesarchio V, Zilembo N, Sabbatini R, Peri A. Practical issues for the management of hyponatremia in oncology. Endocrine. 2018 Jul:61(1):158-164. doi: 10.1007/s12020-018-1547-y. Epub 2018 Feb 7 [PubMed PMID: 29417373]
Baldeweg SE, Ball S, Brooke A, Gleeson HK, Levy MJ, Prentice M, Wass J, Society for Endocrinology Clinical Committee. SOCIETY FOR ENDOCRINOLOGY CLINICAL GUIDANCE: Inpatient management of cranial diabetes insipidus. Endocrine connections. 2018 Jul:7(7):G8-G11. doi: 10.1530/EC-18-0154. Epub [PubMed PMID: 29930026]
Hui C, Khan M, Khan Suheb MZ, Radbel JM. Arginine Vasopressin Disorder (Diabetes Insipidus). StatPearls. 2026 Jan:(): [PubMed PMID: 29262153]
Miell J, Dhanjal P, Jamookeeah C. Evidence for the use of demeclocycline in the treatment of hyponatraemia secondary to SIADH: a systematic review. International journal of clinical practice. 2015 Dec:69(12):1396-417. doi: 10.1111/ijcp.12713. Epub 2015 Aug 19 [PubMed PMID: 26289137]
Level 1 (high-level) evidence