Introduction
Three types of muscle are present in the body: skeletal, smooth, and cardiac. Skeletal striated muscle is the most abundant type (more than 400 distinct muscles), is the only muscle under voluntary control, and in individuals with a normal body mass index, represents approximately 40% of their body weight.[1] Smooth muscle manages the contraction of involuntary muscles. The role of smooth muscle in human physiology is broader than that of skeletal muscle, with functions spanning from regulating vascular resistance to mediating uterine contractions.[2] Cardiac muscle, like smooth muscle, is not voluntarily controlled. The unique feature of this muscle type is its automaticity.[3] While these muscles differ at the cellular level, they all convert chemical energy into mechanical work and movement.[1]
Structure
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure
Across all 3 types of muscle, individual muscle fibers are arranged in parallel to enable contraction, as discussed in the function section. Skeletal striated muscles attach to a bone through dense connective tissue called the tendon. The most superficial layer of a muscle is the epimysium, which wraps together numerous fascicles wrapped with perimysium. Inside each fascicle are the individual muscle fibers wrapped around endomysium. Within the muscle fiber is the functional unit: the sarcomere. The sarcomere is where contraction occurs on the cellular level; all other layers are present to help facilitate tracking of these fibers.[4]
The sarcomere appears as a net of parallel lines. The lateral boundaries of each net, or sarcomere, are the Z-discs. The Z-discs anchor one set of parallel lines called the thin filaments. Running in the opposite direction is the other set of lines, called the thick filaments, which are between the thin filaments. This overlap between the thin and thick filaments is the basis of muscle physiology. The more the two filaments overlap, the more the muscle is contracted.[5]
Smooth muscle lacks the striations skeletal muscle has and instead has a fusiform shape. Cardiac muscle is more structurally similar to skeletal muscle in that it is striated and has sarcomeres. However, due to their automaticity and need for synchronization, cardiac muscle cells have intercalated discs, which electrically couple the cells.[3]
Function
Contraction brings the 2 attachment points of a muscle closer together. For example, the sternocleidomastoid muscle originates from the manubrium and the head of the clavicle and inserts on the ipsilateral mastoid process of the skull. Contraction here causes ipsilateral side-bending and contralateral rotation because the muscle works to bring these 2 bony processes closer together.
The sternocleidomastoid muscle is voluntarily controlled and thus a striated skeletal muscle. As mentioned above, the primary mechanism by which muscles operate is by overlapping of the thick and thin filaments. The proteins that predominantly make up the thin and thick filaments are actin and myosin, respectively. Myosin is like a person climbing a rope, with actin as the rope. Myosin continuously grabs actin, pulls it, releases, reaches, and repeats. Myosin in skeletal muscle cells activates by a rapid increase in calcium concentration released from the muscle cell’s intracellular store, the sarcoplasmic reticulum. Calcium works by binding to a protein called troponin, which moves tropomyosin. Tropomyosin is the protein that wraps around actin and prevents spontaneous binding of myosin to actin; only when calcium is at high enough concentrations can myosin bind to actin. Without calcium, myosin binds to ADP and inorganic phosphate. In the presence of calcium, this complex of myosin, ADP, and Pi binds to actin, forming a cross-bridge. The release of ADP and inorganic phosphate triggers the power stroke (the rope-pull analogy). ATP binds myosin, which allows it to release from actin (the letting go). ATP bound to myosin is split into ADP and Pi, and in the process, myosin is cocked back to start the cycle again (the reaching). Smooth and cardiac muscle work similarly to cause shortening; however, their activation is by different processes.[6]
Histochemistry and Cytochemistry
Hematoxylin is widely used to stain muscles. Hematoxylin stains nuclei either blue or purple, and eosin stains cytoplasm and extracellular matrix pink. With this stain alone, one can easily identify muscle fibers and distinguish between the architecture of the 3 types.[7]
Microscopy, Light
Light microscopy can be used to determine which muscle is being viewed. Skeletal muscle appears as long fibers organized with many repeating perpendicular Z-discs.[1] Smooth muscle has a repeating fusiform pattern. Cardiac muscle, while more similar in appearance to skeletal muscle, is distinguished by staggered, perpendicular lines representing intercalated discs and by more wavy fibers.[1]
Microscopy, Electron
Electron microscopy is extremely useful for linking physiology to histology because its resolution allows an average observer to appreciate critical structures that light microscopy can’t resolve. The following description can be used to understand an electron microscopy image of striated skeletal muscle. When viewing a sarcomere image, it is best to determine the boundaries: the Z-discs. These are lines on each fiber that run perpendicular to the fiber itself. From there, one can start to determine the areas. Between two Z-discs, there are seven distinct color changes, and the sarcomere is symmetric. The zone on either side of the Z-disc is named the I-band; this is where only thin filaments exist, which is why it is the lightest of the grayscale. The remaining 5 zones in the middle of the sarcomere are the A-band. The A-band is where the thick filament is. The A-band further divides into the H-zone and the M-line. The M-line is the central color gradient of the sarcomere and serves as an anchor for the thick filament. The zones on either side of the M-line are called the H-zones and indicate regions where there is only thick filament. The last part of the A-band, the darkest in electron microscopy, is where the thin and thick filaments overlap. During a contraction, this area increases in size, while the H-zone and I-band get smaller.
Review from left to right of a sarcomere:
- Z-line, dark perpendicular line: The sarcomere boundary and anchor for thin filament
- I-band, lightest: Thin filament alone
- A-band, thin and thick filament overlap: Dark area
- A-band, H-zone: Thick filament alone; second lightest area
- A-band, M-line: Anchoring protein for thick filament, second darkest line, middle of sarcomere
- A-band, H-zone: Thick filament alone, second lightest area
- A-band: Thin and thick filament overlap, dark area
- I-band: Lightest, thin filament alone
- Z-line, dark perpendicular line: The sarcomere boundary and anchor for thin filament [6]
Clinical Significance
Duchenne muscular dystrophy is an X-linked genetic disease caused by a mutation in the dystrophin protein that impedes proper muscle contraction. The dystrophin gene that encodes the protein and is one of the largest human genes identified to date. The protein connects actin to the extracellular matrix. Actin and myosin will overlap, but because there is no connection to the extracellular matrix, the overlap does not result in contraction.[8] After repetitive contractions, this disruption causes cellular death and leads to many clinical signs, including elevated creatine kinase levels and muscle weakness. The most affected muscles are the lower limbs and those affecting posture, causing a swayback, weak gluteal muscles, thin thighs, hyper-extended knees (to carry the load of the upper body), a protuberant abdomen (from a weak rectus abdominis), and poor balance. One of the most common signs of Duchenne muscular dystrophy is hypertrophy of the calves. While they may appear to show more muscle growth, this is actually due to chronic necrosis of muscle fibers that have been replaced by fat cells. A similar disease is Becker muscular dystrophy, which also involves a mutation to the dystrophin gene but with less severe sequelae.[7]
Troponin, the binding site for calcium that allows myosin to cause contraction, is also present in cardiac tissue. When cardiac tissue (myocardium) undergoes significant damage, troponin is released from cells and serves as a useful biomarker for diagnosing myocardial infarctions.[9] Conversely, rigor mortis is the hypercontracted state of a deceased organism. While it may seem counterintuitive that an organism without functional oxygen delivery could maintain contraction, the process boils down to the physiology described in the function section. Without ATP to bind to the myosin, myosin remains in the contracted state bound to actin. Only after newly bound ATP can myosin release actin, cease contraction, and relax.[10]
Media
(Click Image to Enlarge)
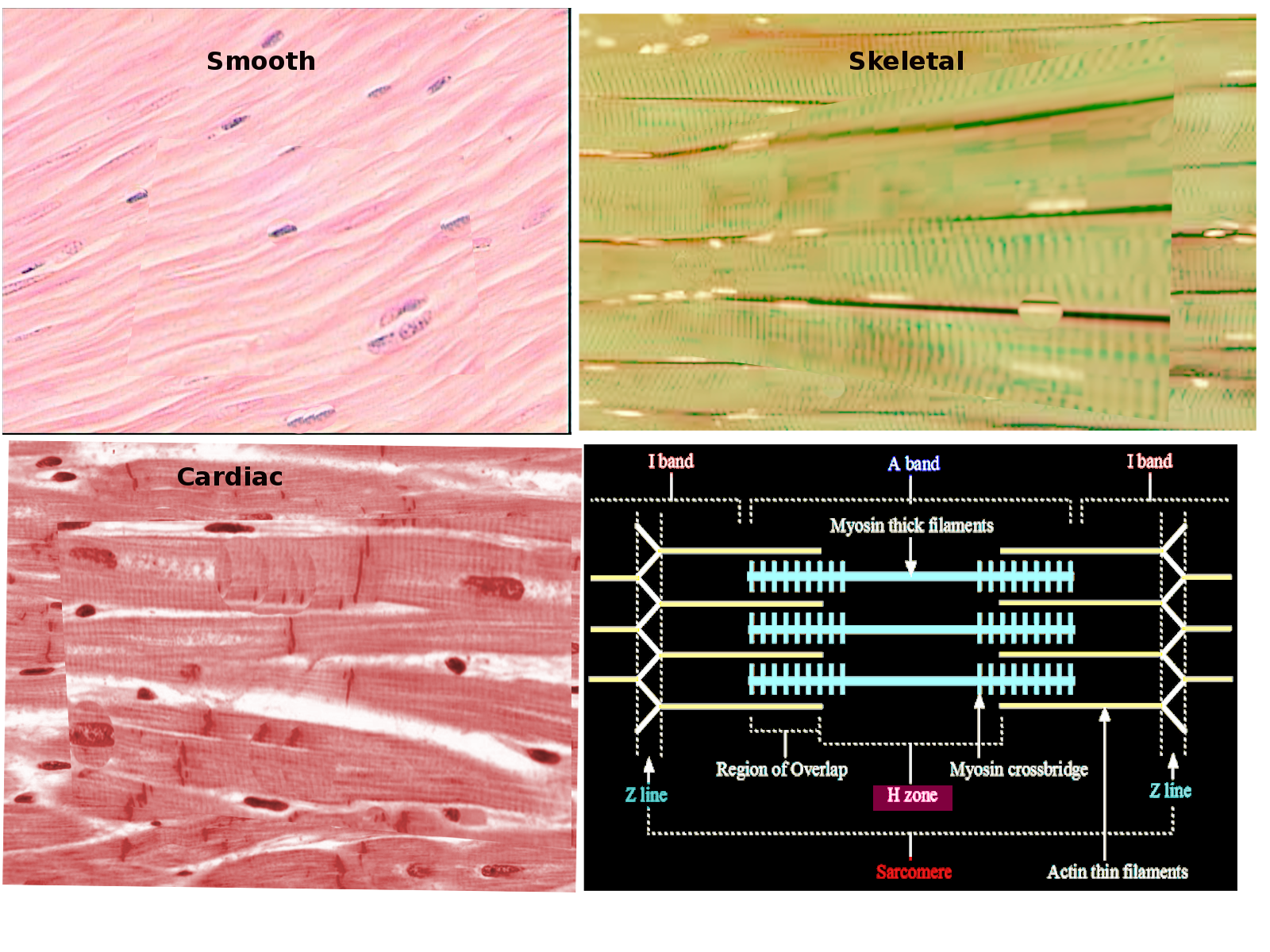
Muscle Types Image courtesy S Bhimji MD
References
Shadrin IY, Khodabukus A, Bursac N. Striated muscle function, regeneration, and repair. Cellular and molecular life sciences : CMLS. 2016 Nov:73(22):4175-4202 [PubMed PMID: 27271751]
Brozovich FV, Nicholson CJ, Degen CV, Gao YZ, Aggarwal M, Morgan KG. Mechanisms of Vascular Smooth Muscle Contraction and the Basis for Pharmacologic Treatment of Smooth Muscle Disorders. Pharmacological reviews. 2016 Apr:68(2):476-532. doi: 10.1124/pr.115.010652. Epub [PubMed PMID: 27037223]
Jafri MS. Models of excitation-contraction coupling in cardiac ventricular myocytes. Methods in molecular biology (Clifton, N.J.). 2012:910():309-35. doi: 10.1007/978-1-61779-965-5_14. Epub [PubMed PMID: 22821602]
McLoon LK, Vicente A, Fitzpatrick KR, Lindström M, Pedrosa Domellöf F. Composition, Architecture, and Functional Implications of the Connective Tissue Network of the Extraocular Muscles. Investigative ophthalmology & visual science. 2018 Jan 1:59(1):322-329. doi: 10.1167/iovs.17-23003. Epub [PubMed PMID: 29346490]
Henderson CA, Gomez CG, Novak SM, Mi-Mi L, Gregorio CC. Overview of the Muscle Cytoskeleton. Comprehensive Physiology. 2017 Jun 18:7(3):891-944. doi: 10.1002/cphy.c160033. Epub 2017 Jun 18 [PubMed PMID: 28640448]
Level 3 (low-level) evidenceSieck GC, Ferreira LF, Reid MB, Mantilla CB. Mechanical properties of respiratory muscles. Comprehensive Physiology. 2013 Oct:3(4):1553-67. doi: 10.1002/cphy.c130003. Epub [PubMed PMID: 24265238]
Level 3 (low-level) evidenceBirnkrant DJ, Bushby K, Bann CM, Apkon SD, Blackwell A, Brumbaugh D, Case LE, Clemens PR, Hadjiyannakis S, Pandya S, Street N, Tomezsko J, Wagner KR, Ward LM, Weber DR, DMD Care Considerations Working Group. Diagnosis and management of Duchenne muscular dystrophy, part 1: diagnosis, and neuromuscular, rehabilitation, endocrine, and gastrointestinal and nutritional management. The Lancet. Neurology. 2018 Mar:17(3):251-267. doi: 10.1016/S1474-4422(18)30024-3. Epub 2018 Feb 3 [PubMed PMID: 29395989]
Level 3 (low-level) evidenceBanks GB, Combs AC, Odom GL, Bloch RJ, Chamberlain JS. Muscle structure influences utrophin expression in mdx mice. PLoS genetics. 2014 Jun:10(6):e1004431. doi: 10.1371/journal.pgen.1004431. Epub 2014 Jun 12 [PubMed PMID: 24922526]
Level 3 (low-level) evidenceGoldstein SA, Newby LK, Cyr DD, Neely M, Lüscher TF, Brown EB, White HD, Ohman EM, Roe MT, Hamm CW. Relationship Between Peak Troponin Values and Long-Term Ischemic Events Among Medically Managed Patients With Acute Coronary Syndromes. Journal of the American Heart Association. 2017 Apr 11:6(4):. doi: 10.1161/JAHA.116.005334. Epub 2017 Apr 11 [PubMed PMID: 28400368]
Eakins F, Harford JJ, Knupp C, Roessle M, Squire JM. Different Myosin Head Conformations in Bony Fish Muscles Put into Rigor at Different Sarcomere Lengths. International journal of molecular sciences. 2018 Jul 18:19(7):. doi: 10.3390/ijms19072091. Epub 2018 Jul 18 [PubMed PMID: 30022010]