Introduction
Acute mesenteric ischemia (AMI) is a condition due to a sudden decline in blood flow through the mesenteric vessels. Without appropriate and timely treatment, necrosis of the small and large intestine results, leading to sepsis and potentially death. Due to the difficulty of diagnosis and the rapid progression, the condition is life-threatening if not identified and treated early. Diagnosis is difficult because symptoms are nonspecific, and the index of suspicion must be high. Mortality rates for AMI range between 60% and 80%. AMI is classified as either occlusive or nonocclusive mesenteric ischemia (NOMI). Occlusive mesenteric arterial ischemia (OMI) is subdivided into acute thromboembolism and acute thrombosis. Please see StatPearls' companion resource, "Mesenteric Venous Thrombosis," for further information on this condition.[1][2][3]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Embolic patients commonly have a positive medical history of cardiovascular diseases, including recent myocardial infarction, congestive heart failure, and atrial fibrillation. Causes include peripheral arterial emboli, cardiac emboli, and a ruptured or dislodged atheromatous plaque after surgery.[4][5][6] The typical thrombotic patient experiences a history of postprandial abdominal pain, leading to food avoidance and weight loss. Causes include atheromatous vascular disease (eg, atherosclerosis, aortic aneurysm, aortic dissection) and decreased cardiac output due to a secondary cause (eg, dehydration, myocardial infarction, congestive heart failure).
The NOMI patient is typically critically ill, presents with several severe comorbidities, and is hemodynamically unstable. Causes include drugs that reduce blood flow (eg, vasopressors and ergotamines), hypotension from severe medical conditions (eg, myocardial infarction, sepsis, CHF, and renal disease), and patients who have recently undergone major surgery (eg, cardiac and abdominal surgery). NOMI accounts for approximately 20% of AMI cases but is associated with the highest mortality due to its insidious onset, diagnostic complexity, limited therapeutic window, and frequent association with multisystem organ dysfunction.[7][8][9]
Epidemiology
AMI is an uncommon but highly morbid condition, with an estimated prevalence of approximately 1 per 1,000 hospital admissions. Among all cases, arterial embolism accounts for 40% to 50%, arterial thrombosis for 25% to 30%, and NOMI for approximately 20%. AMI most frequently affects older adults, with a higher incidence observed in women and in patients with significant underlying comorbidities.
Pathophysiology
An acute mesenteric arterial embolism is often cardiogenic in origin and primarily affects the superior mesenteric artery (SMA). Preceding events include atrial tachyarrhythmia, congestive heart failure, myocardial ischemia or infarction, cardiomyopathy, and ventricular aneurysm, which results in thrombus formation that later embolizes to cause ischemia. Patients with acute mesenteric arterial thrombosis commonly have a preexisting atherosclerotic disease. Vasospasm in the SMA often accompanies NOMI secondary to cardiac failure, peripheral hypoxemia, or reperfusion injury.
Toxicokinetics
In rare instances, vasopressors (eg, cocaine and norepinephrine) and ergotamines may cause NOMI. These agents cause vasoconstriction and reduced blood flow in the mesentery, which may result in bowel ischemia.
History and Physical
AMI patients typically present with abdominal pain that does not correlate with physical exam findings. Abdominal tenderness to palpation occurs when the entire bowel wall is involved, which is a later presentation as necrosis begins. Patients with an embolic disease typically have a history of bowel emptying violently, followed by severe pain. The syndrome rapidly advances to ischemia and necrosis because collateral blood flow is limited.
Thrombosis may take days or weeks to progress, with abdominal pain gradually worsening. Patients also may have a combination of diarrhea, distention, bloody stool, and, most importantly, a history of postprandial pain, suggesting chronic mesenteric ischemia. NOMI progresses slowly, and the associated abdominal pain is not localized and varies in severity and consistency. These patients are critically ill (eg, septic shock, cardiac disease, and respiratory failure), hypotensive, and usually on vasopressor agents.
Evaluation
Laboratory values and biomarkers for AMI are nonspecific and lack diagnostic power. Elevated D-lactate and lactate dehydrogenase are seen in late-stage AMI. Computed tomography (CT) angiography is the preferred method for imaging all types of AMI (see Image. CT Angiogram of the Superior Mesenteric Artery. Sensitivities for CT range from 96% to 100%, and specificities from 89% to 94%. While standard CT angiography provides adequate visualization of the visceral vasculature, a biphasic CT angiography protocol, comprising both arterial and delayed phases, offers improved sensitivity by capturing dynamic perfusion of the portal venous system and bowel wall.
Several nonvascular findings on CT imaging can herald AMI. One of these is pneumatosis intestinalis, which is the presence of gas dissecting through the layers of the bowel wall. Pneumatosis intestinalis may extend into the mesenteric venous system and eventually into the portal vein. This can be seen in 6% to 43% of cases; therefore, its presence warrants a detailed clinical examination. Other findings include changes in bowel wall thickness, which is found in 26% to 96% of AMI cases. Luminal dilatation and bowel air-fluid levels are more often seen in arterial AMI.[10]
Catheter-directed angiography has fallen out of favor during the initial stages of AMI diagnosis because the added surgical stress is a burden on an already critically ill patient when used in conjunction with endovascular interventions to treat AMI. Plain abdominal radiography, duplex ultrasonography, and magnetic resonance angiography have narrow indications in diagnosing AMI.
Treatment / Management
Medical Interventions
Initial medical treatment focuses on fluid resuscitation and correcting electrolyte imbalances. Avoid vasopressors and alpha-adrenergic agents, which may cause vasospasm. If vasopressor support is essential to optimize cardiac output, agents with minimal adverse effects on splanchnic perfusion, eg, low-dose dopamine, dobutamine, or milrinone, are preferred. Broad-spectrum antibiotics should be given before surgery to avoid abdominal sepsis if the necrotic bowel is resected.[11][12][13](B3)
Surgical Interventions
Early surgical exploration is required to assess the level of ischemia and spread of necrosis. Revascularization of the bowel is the primary goal of surgery, and excision of necrotic bowel is necessary. After revascularization, the bowel should be assessed for viability, including checking pulses with continuous-wave Doppler, peristalsis, and normal color. Depending on the type and location of the vessel occlusion, open or endovascular surgical interventions are indicated for the treatment of occlusive mesenteric arterial ischemia.
Bowel resection occurs in 53% of second-look surgeries and 31% during exploratory surgery at the first attempt to revascularize. The difficulty of assessing the extent of necrosis of the bowel warrants a second-look surgery 12 to 48 hours after revascularization. Revascularization options during open surgery include methods, eg, retrograde open mesenteric stenting, wherein the SMA is surgically exposed, and a soft anterior arterial wall segment is punctured, facilitating placement of a stent. The arteriotomy is closed either with interrupted transverse sutures or a patch. One can also consider a traditional SMA embolectomy as well if the embolus is large and organized.[14]
Endovascular Interventions
In patients without peritonitis, endovascular options can be considered. One of them is endovascular aspiration thrombectomy (EVT), in which the SMA is catheterized, and the thrombus is aspirated using a vacuum. Several passes may occur until the clot is sufficiently removed. Risks of this approach include distal propagation of the thrombus into smaller peripheral branches within the mesentery. Closely monitoring the patient is essential to detect clinical deterioration following thrombus aspiration promptly.[15]
As NOMI is secondary to vasospasm rather than occlusion, treatment is medically focused and relies upon reversing the underlying cause of the low-flow state. Catheter-directed papaverine (a phosphodiesterase inhibitor) delivered via a side-hole catheter or thrombolysis catheter is an interventional option.[16][17]
Differential Diagnosis
The early identification of AMI is paramount to reducing the likelihood of debilitating morbidity and high mortality. AMI has a vague presentation, and a high index of suspicion is necessary to diagnose suspected patients because of the life-threatening potential of the disease. Findings of abdominal pain out of proportion to a physical exam and cardiovascular risk factors that predispose a patient to embolism and peripheral thrombosis should alert the clinician to consider AMI. Diseases to consider in the differential diagnosis are those that cause acute abdominal pain and are therefore variable in presentation. These include acute colitis, ruptured abdominal aortic aneurysm, bowel obstruction, diabetic ketoacidosis, gastrointestinal perforation, and malignancy.
Prognosis
The prognosis of AMI is poor, with patients experiencing high morbidity and mortality rates. While a downward trend in mortality rates has occurred since the 1960s, AMI mortality remains high, at 60% to 80%. The specific AMI classification affects the likelihood of mortality, with acute embolism having a better prognosis, followed by NOMI and acute thrombosis. Factors associated with mortality include advanced age, bowel resection during second-look surgery, metabolic acidosis, renal insufficiency, and symptom duration.
A study by Gupta et al found a 30-day morbidity rate of 56%. Major postoperative 30-day complications included ventilator use over 48 hours, septic shock, pneumonia, and sepsis. Follow-up surgical interventions were common, with 30% of patients revisiting the surgical department within 30 days and 14% having a hospital stay longer than 30 days.
Complications
AMI can lead to significant portions of the small bowel that are nonviable and need to be resected during laparotomy. Depending on how much bowel is resected, patients can end up having short bowel syndrome along with intestinal failure. Short bowel syndrome can significantly diminish quality of life and worsen morbidity. The creation of ostomies during these operations can also lead to difficult-to-manage fluid losses and electrolyte imbalances.[18]
Consultations
Several specialists should be involved as early as possible in the clinical course to prevent deleterious outcomes. General or acute care surgeons should be included for entry into the abdomen and evaluation of the bowel. Vascular surgeons can assist with revascularization techniques, both open and endovascular. Interventional radiologists parallel this approach with endovascular revascularization.
Clinical pharmacists can provide input on anticoagulation options both in the hospital and on discharge. Lastly, hematology and oncology teams can assist in working up suspected underlying coagulopathies that may have led to the condition. Additional supportive staff can include physical and occupational therapists to assist with mobility and strength recovery following treatment, and social work teams to assist with arranging services to ensure comprehensive patient success following discharge.
Deterrence and Patient Education
Following successful treatment of AMI, patients should be started on subcutaneous heparin to deter further thromboembolic complications. They may, in fact, need lifelong anticoagulation. Those who suffer from atherosclerotic AMI are recommended to be placed on lifelong platelet antiaggregation medication, eg, low-dose aspirin, in addition to modern medical therapy. In settings where SMA stents are placed, clopidogrel is also added.[19] In older adults prone to falls, shared decision-making should be conducted with the patient and their loved ones to ensure they are properly educated about the risks and benefits of anticoagulation.
Pearls and Other Issues
Maintaining a high clinical suspicion for AMI remains imperative in patients presenting with abdominal pain that is disproportionate to physical examination findings. CT angiography should be pursued whenever AMI is suspected, including in patients with acute kidney injury or compromised renal function, as the consequences of a missed diagnosis far outweigh the risks of contrast-induced nephropathy. Frequent, close monitoring is necessary, incorporating serial abdominal examinations performed by the same clinician, alongside laboratory assessments, eg, serial lactic acid levels, base deficit, anion gap, and bicarbonate, to detect clinical deterioration and guide timely intervention.
Enhancing Healthcare Team Outcomes
AMI represents a life-threatening vascular emergency characterized by a sudden reduction in intestinal blood flow, leading to ischemia, necrosis, sepsis, and high mortality. Diagnosis remains challenging due to nonspecific symptoms and rapid progression, often requiring a high index of suspicion and prompt imaging. Patients frequently present with severe abdominal pain out of proportion to examination findings, and delayed recognition contributes to poor outcomes. Management focuses on rapid hemodynamic resuscitation, early initiation of broad-spectrum antibiotics, and timely surgical or endovascular revascularization, often requiring intensive care support. Many affected individuals are older adults with significant comorbidities, further complicating management and prognosis, while extensive bowel necrosis may necessitate resection and result in ostomy creation or long-term complications such as short bowel syndrome.
Interprofessional collaboration plays a critical role in optimizing outcomes and ensuring patient-centered care. Emergency physicians and primary care clinicians facilitate early recognition and timely referral, while radiologists expedite diagnosis through advanced imaging. Surgeons and vascular specialists coordinate revascularization and operative management, with support from intensivists skilled in critical care resuscitation. Advanced practitioners and nurses perform continuous monitoring, serial assessments, and patient education, including ostomy care when needed.[1][20][21] Pharmacists guide anticoagulation therapy and medication safety, particularly for long-term management. Gastroenterologists contribute to diagnostic evaluation and follow-up care. Coordinated communication, shared decision-making, and early involvement of specialized services, including stoma care, reduce complications, improve safety, and enhance continuity of care across the treatment spectrum.
Media
(Click Image to Enlarge)
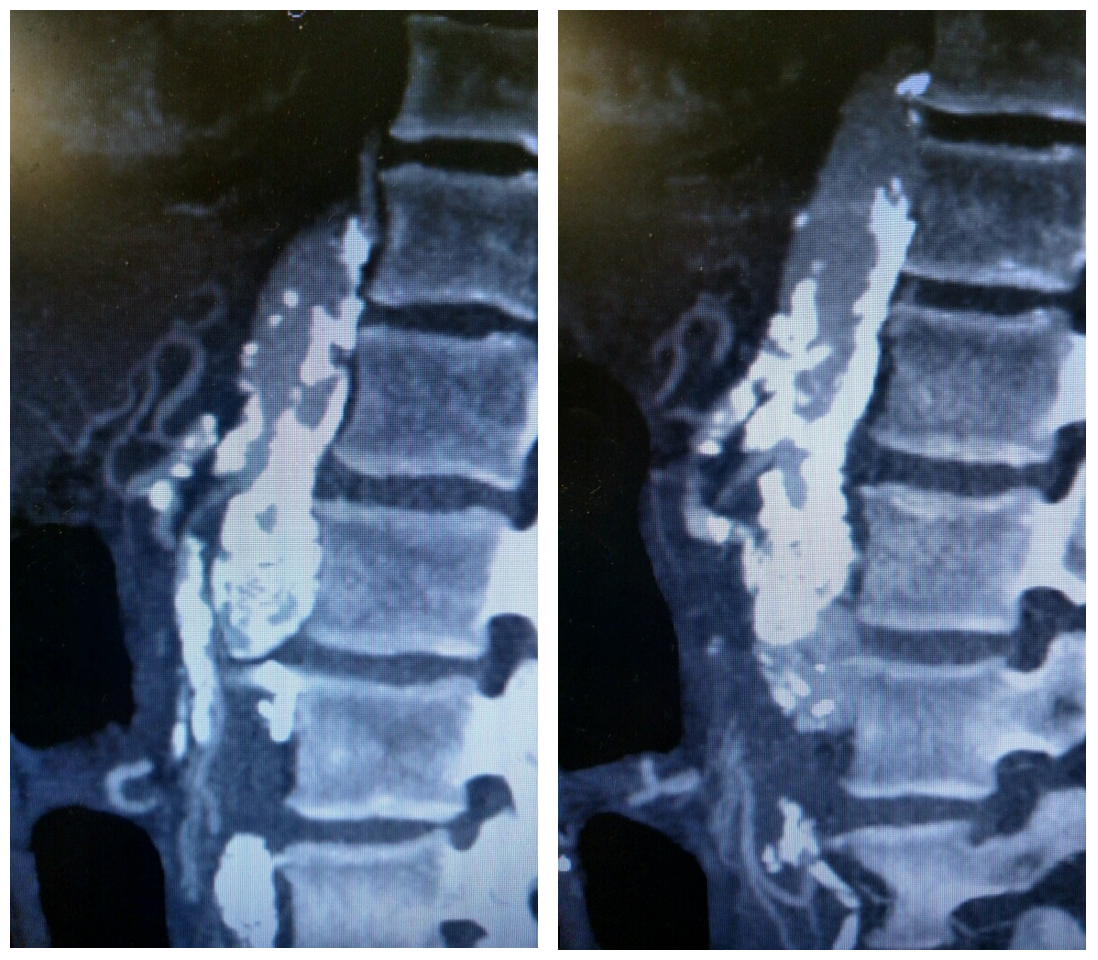
CT Angiogram of the Superior Mesenteric Artery. Sagittal view of a CT angiogram showing severe atherosclerotic disease of the SMA and celiac artery in a patient with acute mesenteric ischemia.
Contributed by L Gonzalez, MD
References
Bath J, Hartwig J, Dombrovskiy VY, Vogel TR. Trends in management and outcomes of vascular emergencies in the nationwide inpatient sample. VASA. Zeitschrift fur Gefasskrankheiten. 2020 Mar:49(2):99-105. doi: 10.1024/0301-1526/a000791. Epub 2019 Apr 25 [PubMed PMID: 31021300]
Khan SM, Emile SH, Wang Z, Agha MA. Diagnostic accuracy of hematological parameters in Acute mesenteric ischemia-A systematic review. International journal of surgery (London, England). 2019 Jun:66():18-27. doi: 10.1016/j.ijsu.2019.04.005. Epub 2019 Apr 16 [PubMed PMID: 30999055]
Level 1 (high-level) evidenceRobles-Martín ML, Reyes-Ortega JP, Rodríguez-Morata A. A Rare Case of Ischemia-Reperfusion Injury After Mesenteric Revascularization. Vascular and endovascular surgery. 2019 Jul:53(5):424-428. doi: 10.1177/1538574419839547. Epub 2019 Apr 14 [PubMed PMID: 30982410]
Level 3 (low-level) evidenceFranca E, Shaydakov ME, Kosove J. Mesenteric Artery Thrombosis. StatPearls. 2026 Jan:(): [PubMed PMID: 30969585]
Mizumoto M, Ochi F, Jogamoto T, Okamoto K, Fukuda M, Yamauchi T, Miyata T, Tashiro R, Eguchi M, Kitazawa R, Ishii E. Nonocclusive Mesenteric Ischemia Rescued by Immediate Surgical Exploration in a Boy with Severe Neurodevelopmental Disability. Case reports in pediatrics. 2019:2019():5354074. doi: 10.1155/2019/5354074. Epub 2019 Feb 19 [PubMed PMID: 30915251]
Level 3 (low-level) evidenceStahl K, Busch M, Maschke SK, Schneider A, Manns MP, Fuge J, Wiesner O, Meyer BC, Hoeper MM, Hinrichs JB, David S. A Retrospective Analysis of Nonocclusive Mesenteric Ischemia in Medical and Surgical ICU Patients: Clinical Data on Demography, Clinical Signs, and Survival. Journal of intensive care medicine. 2020 Nov:35(11):1162-1172. doi: 10.1177/0885066619837911. Epub 2019 Mar 25 [PubMed PMID: 30909787]
Level 2 (mid-level) evidenceKaradeniz E, Bayramoğlu A, Atamanalp SS. Sensitivity and Specificity of the Platelet-Lymphocyte Ratio and the Neutrophil-Lymphocyte Ratio in Diagnosing Acute Mesenteric Ischemia in Patients Operated on for the Diagnosis of Mesenteric Ischemia: A Retrospective Case-Control Study. Journal of investigative surgery : the official journal of the Academy of Surgical Research. 2020 Sep:33(8):774-781. doi: 10.1080/08941939.2019.1566418. Epub 2019 Mar 19 [PubMed PMID: 30885018]
Level 2 (mid-level) evidenceKurita D, Fujita T, Horikiri Y, Sato T, Fujiwara H, Daiko H. Non-occlusive mesenteric ischemia associated with enteral feeding after esophagectomy for esophageal cancer: report of two cases and review of the literature. Surgical case reports. 2019 Feb 20:5(1):36. doi: 10.1186/s40792-019-0580-2. Epub 2019 Feb 20 [PubMed PMID: 30788678]
Level 3 (low-level) evidenceSomarajan S, Muszynski ND, Olson JD, Bradshaw LA, Richards WO. Magnetoenterography for the Detection of Partial Mesenteric Ischemia. The Journal of surgical research. 2019 Jul:239():31-37. doi: 10.1016/j.jss.2019.01.034. Epub 2019 Feb 20 [PubMed PMID: 30782544]
Yu H, Kirkpatrick IDC. An Update on Acute Mesenteric Ischemia. Canadian Association of Radiologists journal = Journal l'Association canadienne des radiologistes. 2023 Feb:74(1):160-171. doi: 10.1177/08465371221094280. Epub 2022 May 11 [PubMed PMID: 35544414]
Expert Panels on Vascular Imaging and Gastrointestinal Imaging:, Ginsburg M, Obara P, Lambert DL, Hanley M, Steigner ML, Camacho MA, Chandra A, Chang KJ, Gage KL, Peterson CM, Ptak T, Verma N, Kim DH, Carucci LR, Dill KE. ACR Appropriateness Criteria(®) Imaging of Mesenteric Ischemia. Journal of the American College of Radiology : JACR. 2018 Nov:15(11S):S332-S340. doi: 10.1016/j.jacr.2018.09.018. Epub [PubMed PMID: 30392602]
Daoud H, Abugroun A, Subahi A, Khalaf H. Isolated Superior Mesenteric Artery Dissection: A Case Report and Literature Review. Gastroenterology research. 2018 Oct:11(5):374-378. doi: 10.14740/gr1056w. Epub 2018 Oct 1 [PubMed PMID: 30344810]
Level 3 (low-level) evidenceLuther B, Mamopoulos A, Lehmann C, Klar E. The Ongoing Challenge of Acute Mesenteric Ischemia. Visceral medicine. 2018 Jul:34(3):217-223. doi: 10.1159/000490318. Epub 2018 Jun 18 [PubMed PMID: 30140688]
Tolonen M, Vikatmaa P. Diagnosis and management of acute mesenteric ischemia: What you need to know. The journal of trauma and acute care surgery. 2025 Aug 1:99(2):151-161. doi: 10.1097/TA.0000000000004585. Epub 2025 Mar 20 [PubMed PMID: 40107963]
Lendzion RJ, Frahm-Jensen G, Keck J. Acute Mesenteric Ischemia. Clinics in colon and rectal surgery. 2022 May:35(3):227-236. doi: 10.1055/s-0042-1743283. Epub 2022 Aug 12 [PubMed PMID: 35966379]
Bala M, Kashuk J, Moore EE, Kluger Y, Biffl W, Gomes CA, Ben-Ishay O, Rubinstein C, Balogh ZJ, Civil I, Coccolini F, Leppaniemi A, Peitzman A, Ansaloni L, Sugrue M, Sartelli M, Di Saverio S, Fraga GP, Catena F. Acute mesenteric ischemia: guidelines of the World Society of Emergency Surgery. World journal of emergency surgery : WJES. 2017:12():38. doi: 10.1186/s13017-017-0150-5. Epub 2017 Aug 7 [PubMed PMID: 28794797]
Salsano A, Salsano G, Spinella G, Palombo D, Santini F. Acute Mesenteric Ischemia: Have the Guidelines of the World Society of Emergency Surgery Analyzed All the Available Evidence? Cardiovascular and interventional radiology. 2018 Feb:41(2):358-359. doi: 10.1007/s00270-017-1817-8. Epub 2017 Oct 30 [PubMed PMID: 29086055]
Bala M, Catena F, Kashuk J, De Simone B, Gomes CA, Weber D, Sartelli M, Coccolini F, Kluger Y, Abu-Zidan FM, Picetti E, Ansaloni L, Augustin G, Biffl WL, Ceresoli M, Chiara O, Chiarugi M, Coimbra R, Cui Y, Damaskos D, Di Saverio S, Galante JM, Khokha V, Kirkpatrick AW, Inaba K, Leppäniemi A, Litvin A, Peitzman AB, Shelat VG, Sugrue M, Tolonen M, Rizoli S, Sall I, Beka SG, Di Carlo I, Ten Broek R, Mircea C, Tebala G, Pisano M, van Goor H, Maier RV, Jeekel H, Civil I, Hecker A, Tan E, Soreide K, Lee MJ, Wani I, Bonavina L, Malangoni MA, Koike K, Velmahos GC, Fraga GP, Fette A, de'Angelis N, Balogh ZJ, Scalea TM, Sganga G, Kelly MD, Khan J, Stahel PF, Moore EE. Acute mesenteric ischemia: updated guidelines of the World Society of Emergency Surgery. World journal of emergency surgery : WJES. 2022 Oct 19:17(1):54. doi: 10.1186/s13017-022-00443-x. Epub 2022 Oct 19 [PubMed PMID: 36261857]
Kärkkäinen JM. Acute Mesenteric Ischemia: A Challenge for the Acute Care Surgeon. Scandinavian journal of surgery : SJS : official organ for the Finnish Surgical Society and the Scandinavian Surgical Society. 2021 Jun:110(2):150-158. doi: 10.1177/14574969211007590. Epub 2021 Apr 19 [PubMed PMID: 33866891]
Scali ST, Ayo D, Giles KA, Gray S, Kubilis P, Back M, Fatima J, Arnaoutakis D, Berceli SA, Beck AW, Upchurch GJ, Feezor RJ, Huber TS. Outcomes of antegrade and retrograde open mesenteric bypass for acute mesenteric ischemia. Journal of vascular surgery. 2019 Jan:69(1):129-140. doi: 10.1016/j.jvs.2018.04.063. Epub 2018 Jun 29 [PubMed PMID: 30580778]
Yang S, Zhao Y, Chen J, Ni Q, Guo X, Huang X, Xue G, Zhang L. Clinical Features and Outcomes of Patients With Acute Mesenteric Ischemia and Concomitant Colon Ischemia: A Retrospective Cohort Study. The Journal of surgical research. 2019 Jan:233():231-239. doi: 10.1016/j.jss.2018.08.010. Epub 2018 Aug 31 [PubMed PMID: 30502253]
Level 2 (mid-level) evidence