 Anatomy, Shoulder and Upper Limb, Median Nerve
Anatomy, Shoulder and Upper Limb, Median Nerve
Introduction
The nerves supplying the upper limb originate from the brachial plexus, which is formed by the anterior rami of spinal nerves C5 to T1. The roots combine to form the superior (C5-C6), middle (C7), and inferior (C8-T1) trunks. Each trunk divides into anterior and posterior divisions that reorganize into the lateral, medial, and posterior cords.
The median nerve, 1 of the 5 terminal branches of the brachial plexus, is formed by the union of the lateral and medial cords. The combined fibers from C5 to T1 contribute to the entire cervical enlargement, resulting in a mixed nerve with a broad segmental origin. The median nerve innervates most forearm flexors and several intrinsic hand muscles.[1][2][3][4]
Knowledge of median nerve anatomy and physiology is essential for diagnosing neuropathies such as carpal tunnel syndrome (CTS), localizing lesions after trauma, and interpreting electrodiagnostic studies. Surgical planning for nerve repair, tendon transfers, or decompression procedures relies on the precise understanding of the nerve's course, branches, and motor distribution. Awareness of anatomic variations prevents iatrogenic injury during procedures involving the axilla, arm, or wrist and guides rehabilitation strategies that restore function and preserve fine motor control.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The median nerve descends in the median bicipital groove within the neurovascular bundle alongside the brachial artery after the convergence of the lateral and medial cords within the axilla. In the arm, the nerve crosses anterior to the brachial artery and passes deep to the bicipital aponeurosis, which inserts the biceps brachii into the proximal forearm and forms the roof of the cubital fossa (see Image. Nerve Distribution in the Arm, Forearm, and Hand). No muscular or cutaneous branches arise in the arm, although the nerve contributes sympathetic fibers to the brachial artery and its distal branches, including the radial and ulnar arteries.[5][6]
At the elbow, the median nerve courses deep to the bicipital aponeurosis and supplies the pronator teres, flexor carpi radialis (FCR), flexor digitorum superficialis (FDS), and palmaris longus. After passing under the aponeurosis, the nerve traverses the interval between the superficial and deep heads of the pronator teres. Compression at this site can produce pronator syndrome.
The nerve then passes beneath the sublime ridge, a fibrous arch formed by the 2 heads of the FDS, before dividing into the anterior interosseous nerve (AIN) and the continuation of the median nerve proper. The median nerve proper descends deep to the FDS but superficial to the flexor digitorum profundus (FDP), whereas the AIN travels deeper, anterior to the interosseous membrane.
In the forearm, the median nerve proper innervates the pronator teres, palmaris longus, and FDS. The AIN supplies the radial 1/2 of the FDP, the flexor pollicis longus (FPL), and the pronator quadratus. Collectively, the median nerve and its branches innervate all forearm flexors except the ulnar 1/2 of the FDP and the flexor carpi ulnaris (see Image. Course of the Median Nerve in the Forearm).
The FDS muscle belly terminates as a tendinous sheath approximately 5 cm proximal to the flexor retinaculum. At this level, the median nerve lies between the tendon of the FDS and that of the FCR before entering the carpal tunnel.[7]
The median nerve gives rise to the palmar cutaneous branch proximal to the wrist. This branch courses superficial to the flexor retinaculum and provides sensory innervation to the palm and the base of the thenar eminence.
At the carpal tunnel, the median nerve passes beneath the flexor retinaculum alongside 9 flexor tendons. The tunnel’s narrowest cross-sectional area measures less than 2 cm², creating a site susceptible to compressive neuropathy. CTS, described below, is the most common entrapment neuropathy.
Distal to the carpal tunnel, the median nerve passes deep to the palmar aponeurosis and gives off the recurrent motor branch, which supplies the thenar muscles: abductor pollicis brevis (APB), flexor pollicis brevis (FPB), and opponens pollicis. The FPL receives motor supply from the AIN, which courses outside the tunnel.
At the level of the palmar aponeurosis, the median nerve divides into radial and ulnar branches that form the common palmar digital nerves. These branches innervate the 1st and 2nd lumbricals and provide cutaneous sensation to the palmar aspect of the thumb, index and middle fingers, and the radial 1/2 of the ring finger. Sensory supply also extends to the dorsal surface of the index and middle fingers, and the radial 1/2 of the ring finger distal to the proximal interphalangeal (PIP) joints, including the nail beds.[8]
Blood Supply and Lymphatics
The median nerve receives its vascular supply from numerous small vasa nervorum derived from adjacent arteries along its course. In the arm, the brachial artery and its muscular branches provide the principal contribution. Around the elbow, additional supply is derived from the inferior ulnar collateral artery, radial recurrent artery, and branches of the cubital anastomosis.
In the forearm, the nerve is supplied by branches of the ulnar and radial arteries, with a major contribution from the anterior interosseous artery, a branch of the common interosseous artery from the ulnar artery. A persistent median artery, when present, may accompany the nerve and augment its perfusion. At the wrist and in the hand, branches of the radial and ulnar arteries, together with the superficial palmar arch, supply the terminal segment of the nerve and its digital branches.[9][10]
Muscles
The muscles innervated by the median nerve in the forearm are organized into 3 layers within the anterior compartment. The superficial layer originates from the medial epicondyle and includes the pronator teres, FCR, and palmaris longus. The intermediate layer consists of the FDS. Both layers receive motor supply from the median nerve proper.
The deep layer contains the FDP, FPL, and pronator quadratus. These muscles are supplied by the AIN, a purely motor branch of the median nerve. The FDP demonstrates dual innervation. The AIN supplies the muscle's radial (lateral) portion, while the ulnar nerve supplies its ulnar (medial) segment.
In the hand, the median nerve innervates the thenar muscles—APB, FPB, and opponens pollicis—through the recurrent motor branch, and supplies the 1st and 2nd lumbricals. All remaining intrinsic hand muscles receive innervation from the deep branch of the ulnar nerve (see Image. Intrinsic Muscles and Ligaments of the Palm).
Sensory innervation of the forearm terminates proximally, with no sensory branches crossing the wrist except for the palmar cutaneous branch of the median nerve. In the hand, the median nerve supplies the palmar surfaces of the thumb, index and middle fingers, and the radial 1/2 of the ring finger. The ulnar nerve provides sensation to the medial hand, including the ulnar 1/2 of the ring finger and the entire little finger, and contributes dorsal sensation via its dorsal cutaneous branch. The superficial branch of the radial nerve completes dorsal innervation by supplying the radial aspect of the dorsum of the hand, including the dorsal thumb and proximal phalanges of the index and middle fingers.[11]
Surgical Considerations
A Monteggia fracture, defined as a proximal ulnar fracture with associated radial head dislocation, places the AIN at risk near the fracture site. Traction or compression at this level can result in neuropathy. Posterior interosseous nerve palsy may also occur due to entrapment, stretching, scarring, displacement, or direct trauma. Open reduction and internal fixation of the ulna restores alignment, relieves tension on the affected nerve, and is frequently associated with recovery of baseline function.[12][13]
CTS is the most common entrapment neuropathy of the median nerve and occurs as the nerve passes beneath the flexor retinaculum of the wrist. Repetitive tendon loading can produce synovial inflammation, resulting in increased compartmental pressure and median nerve compression. Clinical manifestations include numbness and pain in the palmar aspect of the thumb, index and middle fingers, and the radial 1/2 of the ring finger. Symptoms typically worsen at night. Severe cases produce weakness and atrophy of the thenar musculature.
Risk factors include occupational or repetitive activities involving sustained wrist flexion or extension, such as typing, computer work, and manual labor. Pregnancy, weight gain, hypothyroidism, diabetes, inflammatory arthritis, and prior wrist trauma also increase risk. Initial management consists of conservative measures, including night splinting, activity modification, occupational therapy, and nonsteroidal anti-inflammatory medications. Persistent or severe cases may require surgical decompression via carpal tunnel release.[14]
Pronator syndrome is a proximal median nerve compression neuropathy that mimics CTS but produces pain localized to the anterior proximal forearm. Compression typically occurs between the 2 heads of the pronator teres muscle. Paresthesia is present in the sensory distribution of the median nerve and includes numbness of the palm, a finding that differentiates pronator syndrome from CTS. Risk factors resemble those of CTS and include repetitive forearm pronation and supination. Evidence supporting surgical decompression is limited, and approximately 50% to 70% of patients improve with conservative therapy. Management includes rest, ice application, immobilization, nonsteroidal anti-inflammatory drug intake, and occupational therapy.[15]
Clinical Significance
High Median Neuropathy
On physical examination, the thenar eminence should be inspected for atrophy. Light-touch sensation should be assessed over the lateral 3-1/2 digits. The pronator teres, FCR, palmaris longus, and FDS are innervated by the median nerve proper. Lesions affecting these muscles result in weakness of pronation (pronator teres) and marked weakness of forearm flexion at the elbow (FCR and FDS). Finger flexion strength should be evaluated by stabilizing the patient’s hand and testing individual digits. The FDS tendons insert on the sides of the middle phalanges. Thus, weakness of PIP joint flexion is characteristic of a high median neuropathy.[16][17]
The AIN should be tested by asking the patient to form an “OK” sign with the thumb and index finger. An inability to make an "O" shape with the thumb and index finger, producing a flattened pinch, is characteristic of AIN palsy. Distal motor function of the median nerve may also be evaluated by asking the patient to place the hand flat on a surface and raise the thumb. Failure to perform this motion indicates impaired opposition and abduction of the thumb, a finding associated with high median neuropathy.[18][19][20][21]
When median nerve pathology is suspected proximal to the elbow, the patient should be instructed to make a fist. Lesions at this level impair FDS function, producing weakness of flexion of all 4 fingers at the PIP joints. Loss of AIN function abolishes flexion at the distal interphalangeal joints of the index and middle fingers. When attempting to make a fist, the index and middle fingers remain extended, creating the so-called “hand of benediction” or “preacher’s hand.” Anatomic variation of the ulnar nerve often preserves flexion of the middle finger at the PIP joint. Consequently, the resulting posture more closely resembles a pointing index finger, a finding characteristic of high median neuropathy. Supracondylar fractures of the humerus may injure the entire median nerve and produce high median neuropathy.
Median nerve injury at the elbow or forearm can result in a single-palmar-crease appearance. This finding reflects the combined inability to flex the index finger and distal phalanx of the thumb, weak flexion of the middle finger, and defective opposition of the thumb, all consistent with high median neuropathy.
Low Median Neuropathy
Low median neuropathies include CTS, discussed above, and median recurrent neuropathy. Injury to the recurrent branch of the median nerve denervates the FPB, opponens pollicis, and APB. The recurrent branch lies superficially near the midpoint of the thenar muscle mass and is vulnerable to laceration from sharp objects, such as knives or broken glass. Injury may be overlooked in the acute setting if sensory examination reveals no deficit, as this branch carries no sensory fibers. In such cases, the wound may be closed without further evaluation. Failure to recognize the motor deficit may result in progressive loss of thumb opposition and severe thenar muscle atrophy, which may constitute medical negligence.
During the physical examination, thumb opposition should be assessed by instructing the patient to touch the pad of the thumb to the pad of the little finger. Inability to perform this movement is diagnostic of median recurrent neuropathy.
Loss of thenar muscle innervation results in marked atrophy of the thumb musculature. The resulting flattening of the thenar eminence is sometimes referred to as “ape hand,” despite true apes possessing opposable thumbs.
At the elbow, the median nerve lies medial to the brachial artery. During arterial blood gas sampling, the radial artery is commonly selected due to its accessibility. Historically, the Allen test was performed to determine whether the anastomosis between the radial and ulnar arteries could provide sufficient blood flow to the thumb and index finger, since radial artery puncture may cause thrombosis. If the test demonstrated inadequate perfusion through the radial artery, the brachial artery was used as an alternative site.
The modified Allen test has been reported to have low sensitivity for detecting collateral circulation patency.[22] Ultrasound and color Doppler evaluation of the radial artery are now recommended before radial artery catheterization. Accurate localization of the radial artery by palpation or sonography is required. Puncture medial to the brachial artery must be avoided to prevent median nerve injury.
Injection nerve palsy is an iatrogenic condition caused by intramuscular injection placed near or directly into a nerve, resulting in axonal and myelin degeneration. The injected agent can penetrate the endoneurium, causing perineural edema that ultimately leads to nerve injury and, in severe cases, nerve necrosis. The condition is typically extremely painful, with motor deficits generally more pronounced than sensory loss. The most neurotoxic agents include penicillin, chlorpromazine, meperidine, dimenhydrinate, tetanus toxoid, procaine, and hydrocortisone.[23]
Diagnostics
Nerve conduction studies and electromyography are the gold standard for diagnosing median neuropathies such as CTS. Sensitivity may be limited in early or mild disease. A systematic review reported that the sensitivity of nerve conduction studies for CTS ranges from 56% to 85%, with specificity from 94% to 97%.[24] These findings indicate that a threshold degree of nerve impairment is often required before abnormalities become detectable. Clinical findings must be interpreted alongside electrodiagnostic results when evaluating suspected median neuropathies.
Media
(Click Image to Enlarge)
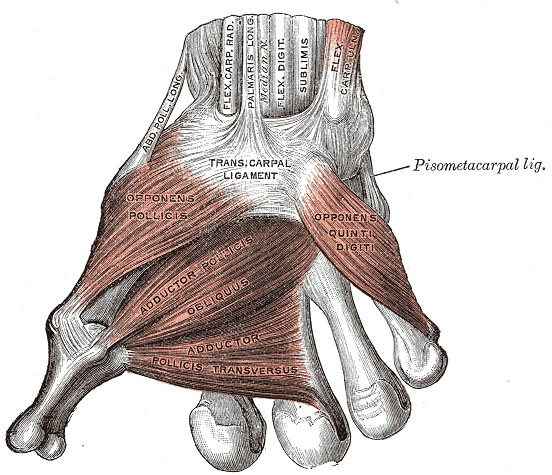
Intrinsic Muscles and Ligaments of the Palm. Illustrated are the opponens pollicis, opponens digiti quinti, adductor pollicis (including oblique and transverse heads), and the transcarpal and pisometacarpal ligaments. Also labeled are the tendons of abductor longus, flexor carpi radialis, palmaris longus, palmaris profundus, flexor digitorum sublimis, and flexor carpi ulnaris.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
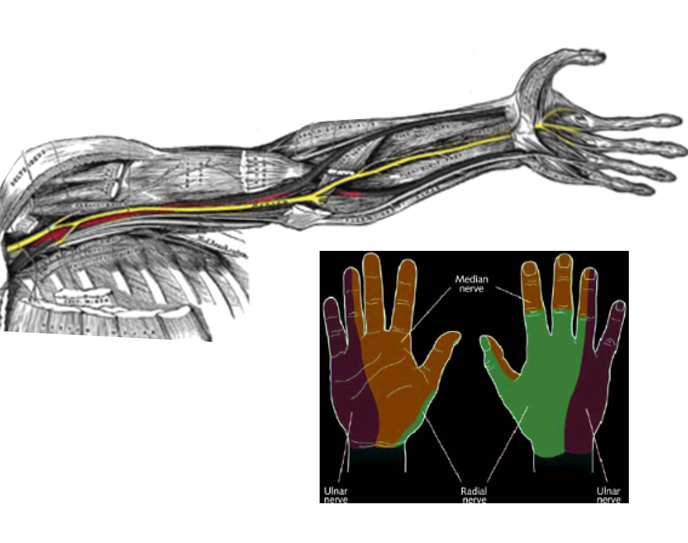
Nerve Distribution in the Arm, Forearm, and Hand. The diagram shows the median nerve's path in the arm and forearm. The inset illustrates sensory regions of the hand innervated by the median, ulnar, and radial nerves.
Contributed by S Bhimji, MD
(Click Image to Enlarge)
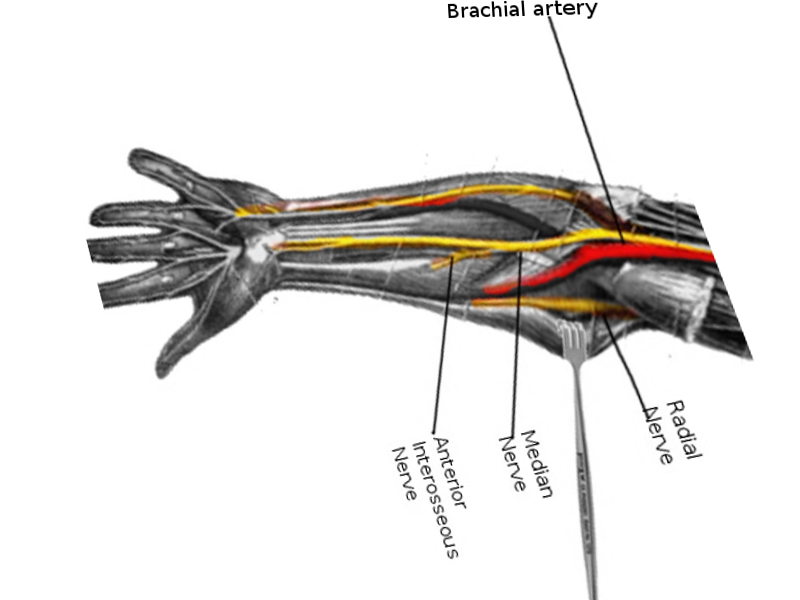
Course of the Median Nerve in the Forearm. The image depicts the course of the median nerve and its branch, the anterior interosseous nerve, in the forearm. The radial nerve and brachial artery are also shown for anatomical reference.
Contributed by O Chaigasame, MD
References
Wertheimer A, Kiel J. Anatomy, Shoulder and Upper Limb, Forearm Anterior Interosseous Nerve. StatPearls. 2025 Jan:(): [PubMed PMID: 30335313]
Bains KNS, Lappin SL. Anatomy, Shoulder and Upper Limb, Elbow Cubital Fossa. StatPearls. 2025 Jan:(): [PubMed PMID: 29083694]
Seiler JG 3rd, Daruwalla JH, Payne SH, Faucher GK. Normal Palmar Anatomy and Variations That Impact Median Nerve Decompression. The Journal of the American Academy of Orthopaedic Surgeons. 2017 Sep:25(9):e194-e203. doi: 10.5435/JAAOS-D-16-00038. Epub [PubMed PMID: 28837460]
Raza K, Singh S, Rani N, Mishra R, Mehta K, Kaler S. Anomalous Innervation of the Median Nerve in the Arm in the Absence of the Musculocutaneous Nerve. Sultan Qaboos University medical journal. 2017 Feb:17(1):e106-e108. doi: 10.18295/squmj.2016.17.01.019. Epub 2017 Mar 30 [PubMed PMID: 28417038]
Doughty CT, Bowley MP. Entrapment Neuropathies of the Upper Extremity. The Medical clinics of North America. 2019 Mar:103(2):357-370. doi: 10.1016/j.mcna.2018.10.012. Epub [PubMed PMID: 30704687]
Ram S. "Carpal tunnel syndrome:" A bibliometric study of 35 years of research. Neurology India. 2019 Jan-Feb:67(Supplement):S55-S61. doi: 10.4103/0028-3886.250698. Epub [PubMed PMID: 30688235]
Caetano EB, Toledo JPN, Amaral SAD, Vieira LA, Pigossi BD, Andrade RA. INNERVATION OF THE MEDIAN NERVE MOTOR BRANCHES IN THE FOREARM AND ITS CLINICAL SIGNIFICANCE. Acta ortopedica brasileira. 2020 Sep-Oct:28(5):251-255. doi: 10.1590/1413-785220202805235028. Epub [PubMed PMID: 33144842]
Bertelli JA, Patel N, Soldado F, Duarte ECW. Patterns of median nerve branching in the cubital fossa: implications for nerve transfers to restore motor function in a paralyzed upper limb. Journal of neurosurgery. 2021 Nov 1:135(5):1524-1533. doi: 10.3171/2020.9.JNS202742. Epub 2021 Mar 19 [PubMed PMID: 33740763]
Giesen T, Acland RD, Thirkannad S, Elliot D. The vascularization of the median nerve in the distal forearm and its potential clinical importance. The Journal of hand surgery. 2012 Jun:37(6):1200-7. doi: 10.1016/j.jhsa.2012.03.028. Epub [PubMed PMID: 22624784]
BLUNT MJ. The vascular anatomy of the median nerve in the forearm and hand. Journal of anatomy. 1959 Jan:93(1):15-22 [PubMed PMID: 13620612]
Bertelli JA, Seltser A, Gasparelo KR, Hill EJR. The Cutaneous Branches of the Median and Ulnar Nerves in the Palm. The Journal of hand surgery. 2023 Nov:48(11):1166.e1-1166.e6. doi: 10.1016/j.jhsa.2022.03.021. Epub 2022 May 28 [PubMed PMID: 35641387]
Zaremski JL, Wright TW, Herman DC. Humeral Stress Fracture With Median Nerve Injury in a Baseball Player: A Case Report and Discussion. Current sports medicine reports. 2018 Jun:17(6):183-186. doi: 10.1249/JSR.0000000000000489. Epub [PubMed PMID: 29889146]
Level 3 (low-level) evidenceVaquero-Picado A, González-Morán G, Moraleda L. Management of supracondylar fractures of the humerus in children. EFORT open reviews. 2018 Oct:3(10):526-540. doi: 10.1302/2058-5241.3.170049. Epub 2018 Oct 1 [PubMed PMID: 30662761]
Kortlever JTP, Becker SJE, Zhao M, Ring D. Borderline Nerve Conduction Velocities for Median Neuropathy at the Carpal Tunnel. The Journal of hand surgery. 2020 May:45(5):379-388.e1. doi: 10.1016/j.jhsa.2019.11.020. Epub 2020 Feb 20 [PubMed PMID: 32089378]
Dididze M, Tafti D, Sherman AL. Pronator Teres Syndrome. StatPearls. 2025 Jan:(): [PubMed PMID: 30252346]
Isaacs J, Ugwu-Oju O. High Median Nerve Injuries. Hand clinics. 2016 Aug:32(3):339-48. doi: 10.1016/j.hcl.2016.03.004. Epub 2016 May 2 [PubMed PMID: 27387077]
Morimoto D, Isu T, Kim K, Sugawara A, Isobe M, Morita A. Proximal Entrapment Neuropathy of the Median Nerve above the Elbow-Case Report. Journal of Nippon Medical School = Nippon Ika Daigaku zasshi. 2015:82(6):287-9. doi: 10.1272/jnms.82.287. Epub [PubMed PMID: 26823032]
Level 3 (low-level) evidenceKowalska B, Sudoł-Szopińska I. Ultrasound assessment on selected peripheral nerve pathologies. Part I: Entrapment neuropathies of the upper limb - excluding carpal tunnel syndrome. Journal of ultrasonography. 2012 Sep:12(50):307-18. doi: 10.15557/JoU.2012.0016. Epub 2012 Sep 30 [PubMed PMID: 26674101]
Keiner D, Tschabitscher M, Welschehold S, Oertel J. Anterior interosseous nerve compression syndrome: is there a role for endoscopy? Acta neurochirurgica. 2011 Nov:153(11):2225-9. doi: 10.1007/s00701-011-1091-5. Epub 2011 Jul 23 [PubMed PMID: 21786008]
Level 3 (low-level) evidenceLeclère FM, Bignion D, Franz T, Mathys L, Vögelin E. Endoscopically assisted nerve decompression of rare nerve compression syndromes at the upper extremity. Archives of orthopaedic and trauma surgery. 2013 Apr:133(4):575-82. doi: 10.1007/s00402-012-1668-3. Epub 2013 Feb 17 [PubMed PMID: 23417113]
Level 2 (mid-level) evidenceStrohl AB, Zelouf DS. Ulnar Tunnel Syndrome, Radial Tunnel Syndrome, Anterior Interosseous Nerve Syndrome, and Pronator Syndrome. The Journal of the American Academy of Orthopaedic Surgeons. 2017 Jan:25(1):e1-e10. doi: 10.5435/JAAOS-D-16-00010. Epub [PubMed PMID: 27902538]
Cho SA, Jang YE, Ji SH, Kim EH, Lee JH, Kim HS, Kim JT. Ultrasound-guided arterial catheterization. Anesthesia and pain medicine. 2021 Apr:16(2):119-132. doi: 10.17085/apm.21012. Epub 2021 Apr 15 [PubMed PMID: 33866769]
Sriwong PT, Sirasaporn P, Foochareon C, Srichompoo K. Median neuropathy at the wrist in patients with systemic sclerosis: two-year follow-up study. Reumatologia. 2018:56(5):294-300. doi: 10.5114/reum.2018.79500. Epub 2018 Oct 31 [PubMed PMID: 30505011]
Demino C, Fowler JR. The Sensitivity and Specificity of Nerve Conduction Studies for Diagnosis of Carpal Tunnel Syndrome: A Systematic Review. Hand (New York, N.Y.). 2021 Mar:16(2):174-178. doi: 10.1177/1558944719855442. Epub 2019 Jun 17 [PubMed PMID: 31203646]
Level 1 (high-level) evidence