Indications
Cannabis is commonly sought by patients for symptom management across a range of conditions, including pain, nausea, appetite stimulation, and spasticity, with its therapeutic use directed toward palliation rather than disease modification. However, clinician adoption remains limited due to a paucity of high-quality randomized controlled trials, variability in product composition and dosing, ongoing federal regulatory constraints, and limited formal education regarding cannabinoid pharmacology. Cannabis refers to plants of the Cannabis genus. Marijuana is a nontechnical term describing cannabis cultivated for psychoactive effects and typically characterized by higher concentrations of delta-9-tetrahydrocannabinol (Δ-9 THC). Hemp refers to cannabis plants legally defined in the United States as containing no more than 0.3% Δ-9 THC on a dry-weight basis and is primarily used for industrial or commercial applications per the Agriculture Improvement Act of 2018. Distinguishing among these terms is essential, as they are frequently conflated in both public discourse and clinical practice. Importantly, whole-plant cannabis has not received approval from the US Food and Drug Administration (FDA) for the treatment of any medical condition. However, select purified or synthetic cannabinoid products, such as dronabinol, nabilone, and cannabidiol (CBD), are FDA-approved for specific indications.
FDA-Approved Indications
The FDA-approved analogs of marijuana include CBD, dronabinol, and nabilone.[1]
Cannabidiol: The FDA has approved a CBD oral solution for the treatment of seizures associated with severe forms of epilepsy in patients aged 1 and older, specifically for Lennox-Gastaut syndrome, Dravet syndrome, and tuberous sclerosis complex.[2][3][4]
Dronabinol: Dronabinol is approved by the FDA for the treatment of anorexia associated with weight loss in patients diagnosed with adult immunodeficiency syndrome and for nausea and vomiting associated with cancer chemotherapy.[5]
Nabilone: Nabilone is indicated for the management of refractory chemotherapy-induced nausea and vomiting.[6]
According to the American Society for Clinical Oncology guidelines, for refractory chemotherapy-induced nausea and vomiting due to moderate or highly emetogenic chemotherapy, synthetic cannabinoids such as dronabinol and nabilone may be used as salvage antiemetics.
Off-Label Uses
The off-label uses of marijuana include the following:
- THC, the primary cannabinoid, can reduce intraocular pressure. However, no major ophthalmology organizations currently endorse the use of medical cannabis for glaucoma.[7]
- Improvement of muscle spasms and pain associated with multiple sclerosis and spinal cord injuries has been observed with the use of marijuana. Although the use of cannabis and cannabinoids for chronic pain remains a subject of controversy, it is widely used for this purpose.[8][9]
- Marijuana is used to treat neuropathic pain, spasticity related to Parkinson disease, nausea and vomiting resulting from chemotherapy, anxiety disorders, sleep disorders, Tourette syndrome, and Crohn disease.[10][11]
- Cannabis is also used to stimulate appetite in patients with AIDS-related wasting and in certain psychiatric conditions, such as posttraumatic stress disorder (see Image. Overview of Key Cannabinoids).[12]
Mechanism of Action
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Mechanism of Action
Marijuana comprises over 400 compounds, such as flavonoids, terpenoids, and cannabinoids. Among these, cannabinoids are the active ingredients that exhibit clinical effects. Cannabinoids are a class of biological compounds that bind to cannabinoid receptors. These compounds are most frequently sourced from plants in the genus Cannabis, including Cannabis sativa, Cannabis indica, and Cannabis ruderalis. The earliest known use of cannabinoids was 5000 years ago in modern Romania, whereas the documentation of the earliest medical use dates back to around 400 AD.[13][14] However, the formal extraction, isolation, and structural elucidation of cannabinoids occurred relatively recently, in the late 19th and early 20th centuries.[13] Since then, numerous advancements have been made in further isolating naturally occurring cannabinoids, synthesizing artificial equivalents, and discovering the endogenous endocannabinoid system in mammals, reptiles, fish, and birds.[15][16] Cannabinoids have 3 forms, including:
- Phytocannabinoids: Derived naturally from flora
- Endocannabinoids: Produced endogenously
- Synthetic cannabinoids: Created artificially
Of all known cannabinoids that have been isolated and identified, the most notable are the phytocannabinoids THC and CBD, the former being responsible for psychoactive effects sought by recreational users and the therapeutic effects of the drug. Throughout their storied history, cannabinoids have been renowned for their psychotropic and physiological effects. Cannabinoids are frequently the targets of pharmaceutical innovation, with most being either structurally related to or mimicking the ligand-receptor activity of THC and CBD.
Cytochrome P450 enzymes metabolize cannabinoids in the liver. Although ongoing research continues to elucidate the mechanism of action, it is established that the brain and peripheral tissues harbor widespread cannabinoid receptors forming the endocannabinoid system. This system regulates various bodily functions, including metabolism, appetite, blood pressure, glycemic control, immune response, and sense of reward. Although cannabinoid receptors are located throughout the body, the most prominent effects arise from the interactions in the central nervous system (CNS). Due to their high lipid solubility, cannabinoid receptors are widely distributed throughout the body, producing diverse effects depending on receptor activation and dose.[17]
The primary action of cannabinoids occurs through G-protein–coupled receptors, specifically CB1 and CB2. CB1 receptors located in the CNS modulate the release of several neurotransmitters, including norepinephrine, dopamine, serotonin, and gamma-aminobutyric acid. Conversely, CB2 receptors are located in the immune system and modulate immune and inflammatory responses. Notably, CB2 expression becomes highly inducible in the microglia in the CNS following inflammation.[18][19]
Pharmacokinetics
Absorption: Inhaling marijuana rapidly elevates THC concentration in the bloodstream, reaching its peak within 3 to 10 minutes. Conversely, oral ingestion leads to peak levels within 1 to 2 hours.
Distribution: The lipophilic THC disseminates to adipose tissue, liver, lungs, and spleen. Metabolism results in the generation of psychoactive 11-hydroxy-9-tetrahydrocannabinol and the formation of inactive tetrahydrocannabinol (THC-COOH). After absorption into the bloodstream, THC rapidly penetrates fatty and highly vascularized tissues, including the brain and muscles. This initial distribution is followed by a slower redistribution of the compound from deep fat deposits back into the bloodstream.[20][21]
Metabolism: The cytochrome P450 enzymes, found in liver cells, facilitate microsomal hydroxylation and oxidation, which metabolize THC. Plasma clearance rates vary depending on factors such as gender and usage history. Liver metabolism significantly reduces the oral bioavailability of THC.[22]
Elimination: Most of the metabolized cannabis is excreted through feces (65%) and urine (20%). Glucuronic acid conjugation enhances the solubility of metabolites. THC-COOH is commonly found in urine, whereas 11-hydroxy-9-tetrahydrocannabinol is usually dominant in feces. The detection times of THC vary among users.[23]
Administration
Federally, marijuana (cannabis) remains Schedule I under the Controlled Substances Act. Although many states allow medical or adult-use sales, many consumer CBD products are not FDA-approved, and the FDA has taken the position that CBD and THC are generally not lawful as dietary supplements. However, enforcement and state rules vary. Marijuana is being administered in various ways, including orally, sublingually, or topically. Consumer cannabis products are sold in state-regulated dispensaries (where legal) and via unregulated markets. Formulations include flower for smoking or vaping, edibles, tinctures, and beverages.
Typically, cannabis is smoked, offering the advantage of rapid onset and easy titration as it swiftly reaches the brain and circulatory system. However, the approval of smoked cannabis for medical use has faced challenges for various reasons, with a significant concern being the variable mixture of THC, other cannabinoids, carcinogens, and other toxic substances introduced into the lungs. Topical cannabinoid preparations, particularly creams and ointments, have been evaluated for localized pain conditions such as arthritis, but current evidence is limited and mixed, precluding definitive conclusions regarding efficacy. Variability in product composition and study methodology further complicates the interpretation of available data.
Nonoral delivery methods, including suppositories, lozenges, sublingual tablets, and transdermal formulations, have been explored in clinical and experimental settings. However, their use has been limited by significant variability in cannabinoid content, insufficient pharmacokinetic and pharmacodynamic data, and the absence of standardized dosing, leading to unpredictable clinical effects.[24] When ingested orally, the pharmacokinetics of marijuana vary greatly. The onset is delayed (approximately 30 to 90 minutes), with peak effects commonly occurring around 2 to 3 hours (sometimes longer, depending on the product or food), and elimination is prolonged and highly variable due to redistribution into fat stores.[25]
Retail CBD products often provide 10 to 50 mg per serving, but dosing is not standardized, and the labeled content and quality may vary. Clinically studied prescription CBD uses weight-based dosing. In jurisdictions where cannabis products are regulated, oral THC formulations are typically standardized in unit doses of 5 to 10 mg per serving. Lower initial doses (2.5-5 mg) are commonly advised for individuals without prior THC exposure to minimize adverse psychoactive effects. Doses exceeding 10 to 15 mg per serving are generally reserved for individuals with established tolerance and are associated with a higher likelihood of dose-dependent adverse effects.[26]
Available FDA-Approved Dosage Forms
Depending on the cannabinoid, the route of administration varies. Medical cannabinoids are generally administered orally as a capsule or liquid suspension:
- CBD (Epidiolex): Available as an oral solution at 100 mg/mL, taken twice daily, starting at 2.5 mg/kg/d and titrated based on clinical response and tolerability.
- Dronabinol (Marinol, Syndros): Available as a capsule in 2.5, 5, and 10 mg strengths, as well as an oral solution in a 5 mg/mL formulation. The medication is generally taken twice daily, 1 hour before meals, with titration from the initial dose performed gradually based on tolerability and response.
- Nabilone (Cesamet): Available as a 1 mg capsule and may be taken 2 to 3 times daily, depending on the clinician and patient preference.
Adult Dose
The recommended doses for FDA-approved marijuana analogs (CBD, dronabinol, and nabilone) are as follows:
Cannabidiol:
- Lennox-Gastaut syndrome or Dravet syndrome
- Starting dose: 2.5 mg/kg orally twice daily (5 mg/kg/d)
- Maintenance dose: 5 mg/kg twice daily (10 mg/kg/d)
- Maximum dose: 10 mg/kg twice daily (20 mg/kg/d)
- Tuberous sclerosis complex
- Starting dose: 2.5 mg/kg orally twice daily (5 mg/kg/d)
- Maintenance dose: 12.5 mg/kg twice daily (25 mg/kg/d)
Dronabinol:
- Anorexia is associated with weight loss in patients diagnosed with AIDS
- Starting dose: 2.5 mg dronabinol capsules orally twice daily, 1 hour before lunch and dinner
- Maintenance dose: Increased gradually to 2.5 mg before lunch and 5 mg before dinner, as tolerated
- Maximum dose: 10 mg twice daily
- Nausea and vomiting associated with cancer chemotherapy
- Starting dose: 5 mg/m2 dronabinol orally, 1 to 3 hours before chemotherapy, continued every 2 to 4 hours after chemotherapy daily for 4 to 6 doses
- Maintenance dose: Modified according to the response, increasing or decreasing in 2.5 mg/m2 increments
- Maximum dose: Up to 15 mg/m2 per dose, 4 to 6 times daily
Nabilone:
- Refractory chemotherapy-induced nausea and vomiting
- Starting dose: 1 mg or 2 mg, twice daily, or 1 to 3 hours before chemotherapy. Doses should be low initially and adjusted as required to minimize adverse effects.
- Maintenance dose: Administered 2 or 3 times daily throughout each chemotherapy cycle.
- Maximum daily dose: 6 mg, which should be divided into 3 equal doses taken throughout the day
Specific Patient Populations
Hepatic impairment: No dose adjustments are necessary for CBD in patients with mild hepatic impairment. However, reduction is required for individuals with moderate-to-severe hepatic impairment.[27] CBD should be discontinued if symptoms of jaundice occur alongside alanine aminotransferase elevations or if alanine aminotransferase levels are 5 times the upper limit of normal.[28] Nabilone product labeling does not specify any dosage adjustments; this medication should be administered cautiously to patients with hepatic impairment. Similarly, the manufacturer's labeling does not indicate that any dosage adjustments are necessary for dronabinol.
Renal impairment: The manufacturer's labeling for nabilone, CBD, or dronabinol does not specify any dosage adjustments for patients with renal impairment.
Pregnancy considerations: The use of CBD and dronabinol is not recommended during pregnancy as they can cause fetal harm. Cannabinoid use during pregnancy is unsafe and associated with adverse effects on the fetus, including small-for-gestational-age infants, preterm birth, and possible neurodevelopmental consequences.[29] The American College of Obstetricians and Gynecologists states that cannabinoids primarily affect the CNS through CB1. These receptors are formed in the fetal brain by 14 weeks of gestation and increase with age, indicating a neurodevelopmental role. Animal studies have demonstrated that exposure to external cannabinoids during pregnancy can disrupt fetal brain development, leading to potential cognitive impairment. Human studies have linked prenatal marijuana exposure to attention, behavior, and visual-motor coordination deficits and a higher likelihood of adolescent marijuana use.
Although structural congenital disabilities are not consistently associated with marijuana exposure, some studies have reported a possible increased risk of anencephaly with first-trimester use, potentially confounded by folic acid deficiency. Evidence regarding perinatal mortality is mixed; some studies show no significant differences, whereas others indicate a slight stillbirth risk, often complicated by tobacco use. Frequent marijuana use in the first and second trimesters has been associated with lower birth weight, shorter crown-heel length, and smaller head circumference. Additionally, weekly or more frequent use may also increase the risk of preterm birth, especially with tobacco. Due to potential fetal neurodevelopment and perinatal outcome risks, the American College of Obstetricians and Gynecologists advises against marijuana use during pregnancy and recommends routine, nonjudgmental screening and cessation counseling.[30] Pregnant women should be advised to avoid the use of CBD, dronabinol, and nabilone.
Breastfeeding considerations: CBD, a component of cannabis, has been detected in breastmilk. However, data on its use as an antiepileptic during lactation are lacking. Due to the absence of safety data, an alternate drug is preferred, particularly for newborns or preterm infants. Dronabinol, a synthetic form of Δ9-THC, has also been found in breastmilk. Although its presence does not necessitate stopping breastfeeding, an alternate antiemetic is recommended due to limited safety data during lactation. The Lactation and Cannabis Study showed that Δ-9-THC peaks in milk a few hours after use and accumulates with repeated exposure. Cannabinoid concentrations in milk vary among individuals and correlate with the frequency of use. These findings highlight the need for cautious counseling about cannabis use during breastfeeding.[31][32]
The psychoactive element of cannabis, THC, is present in breast milk in insignificant amounts. Research indicates that THC can be detected in milk for periods ranging from 6 days to over 6 weeks. Concerns arise regarding potential impacts on neurological development, neurotransmitters, and endocannabinoid-related functions. The research observed reduced levels of secretory immunoglobulin A in the breast milk of mothers who use cannabis. A study suggested that regular cannabis use may affect infants' motor development but not their intellectual progress. Guidelines suggest avoiding cannabis while nursing due to potential developmental effects from breast milk exposure. Paternal cannabis use might raise the risk of sudden infant death syndrome.[33]
Pediatric patients: The use of nabilone and dronabinol should be avoided.[34] The American Academy of Pediatrics opposes the use of medical marijuana outside the regulatory framework of the FDA. However, the American Academy of Pediatrics recognizes that cannabinoid-based therapies may be considered for children with severe or life-limiting conditions when standard treatments have failed.[35] Notably, the prevalence of cannabis use disorder was 10.7% among adolescents and 6.4% among young adults within 1 year. Moreover, this discrepancy persisted, with rates of 20.1% for adolescents and 10.9% for young adults when considering a period extending beyond 36 months. This phenomenon aligns harmoniously with the established trajectory, indicating a swifter transition to substance use disorders (SUDs) when drug initiation occurs at an earlier age. Although the American Academy of Pediatrics advocates SUD screening for adolescents, the US Preventive Services Task Force emphasizes screening for SUDs exclusively in adults.[36]
Older patients: Research findings indicate a significant increase in the frequency of emergency department visits associated with cannabis use among individuals aged 65 or older. The comprehensive rate surged from 20.7 per 100,000 emergency department visits in 2005 to 395.0 per 100,000 in 2019. Incorporating discussions about cannabis use and providing valuable advice on its safe use should become a standard component of health care for older adults.[37] Older adults may be more sensitive to adverse effects such as postural hypotension and neuropsychiatric symptoms. These patients should initially take a lower dose of nabilone, dronabinol, and CBD.
Adverse Effects
The most commonly reported adverse effects of cannabis, particularly THC-containing products, include dizziness, dry mouth, impaired attention and coordination, euphoria or dysphoria, anxiety, confusion, disorientation, sedation, and tachycardia. Respiratory symptoms, such as cough or wheeze, are more strongly associated with inhalational exposure.[38][39][40][41] Acute anxiety reactions, including panic symptoms, are a common reason for emergency evaluation after cannabis exposure, particularly with high-THC products.[42] Marijuana use has been associated with cases of acute reversible psychotic reactions in adolescents. Furthermore, cannabis elevates the risk of psychotic disorders and worsens or causes relapses of symptoms in individuals with preexisting psychotic disorders.[43] Results from certain studies suggest an elevated risk of lung cancer is associated with the inhalation of marijuana, along with a connection between inhalational marijuana use and spontaneous pneumothorax. In addition, inhaled marijuana is linked to bullous emphysema and complications related to chronic obstructive pulmonary disease, including increased wheezing, cough, and phlegm production.[44]
Prenatal cannabis use has been associated with increased odds of adverse neonatal outcomes, including preterm birth and small-for-gestational-age infants. Marijuana use is also associated with impaired spermatogenesis.[45] Long-term marijuana use has also been associated with periodontal disease and more frequent pain crises in sickle cell patients, but data remain limited and heterogeneous.[46] Epidemiologic studies estimate that approximately 22% to 30% of individuals who use cannabis meet criteria for cannabis use disorder, with a higher risk among those who initiate use in adolescence and those who use frequently.[47] Furthermore, adolescents who used marijuana were significantly less likely than their peers to complete high school or attain a degree. However, these associations are subject to confounding factors, including socioeconomic status, co-occurring substance use, and mental health conditions. Marijuana may also worsen verbal memory, depression, and anxiety disorders.[48] Chronic use has been well-documented as a cause of cannabinoid hyperemesis syndrome, initially described in Australia by Allen et al in 2004. This syndrome is characterized by recurrent episodes of nausea and vomiting that are alleviated by hot showers.[49]
Withdrawal
Complications have been associated with the abrupt cessation of marijuana following chronic use. Cannabis withdrawal typically necessitates supportive care, and symptoms may include irritability, poor sleep, poor appetite, and restlessness.[50][51] As a combination of CBD with alcohol increases the potential for sedation, lethargy, and CNS depression, the combination should be avoided.[52]
Drug-Drug Interactions
Potent inducers of CYP3A4 and CYP2C19 enzymes, such as rifampin, can reduce CBD and its metabolite 7-OH-CBD levels by approximately 32% and 63%, respectively, potentially affecting CBD's effectiveness.[53] CBD inhibits CYP1A2, affecting the metabolism of substances such as caffeine, theophylline, and tizanidine.[54] CBD shows potential interactions with substrates of CYP2B6, such as bupropion and efavirenz; UGT1A9, such as diflunisal, propofol, and fenofibrate; UGT2B7, such as gemfibrozil, lamotrigine, morphine, and lorazepam; CYP2C8; and CYP2C9. Plasma concentrations of CYP2C19 substrates, such as diazepam, can increase when coadministered with CBD, necessitating a dosage reduction. The concurrent administration of CBD and valproate increases the risk of hepatocellular enzyme elevation, which may require treatment discontinuation. Clobazam's active metabolite levels elevate 3-fold in the presence of CBD, impacting dosing considerations. Because CBD increases stiripentol levels, careful monitoring for associated adverse effects is recommended.[55][56] CBD increases the concentration of P-glycoprotein substrates, such as everolimus, necessitating careful dose adjustments.[57]
When dronabinol is taken concomitantly with drugs that have comparable cardiovascular effects, such as hypotension, hypertension, and tachycardia, the potential for additive cardiac effects exists, including syncope. Dronabinol's metabolism is primarily mediated by CYP2C9 and CYP3A4. Inhibitors of these enzymes can increase dronabinol levels, whereas inducers may decrease them. These interactions can lead to increased adverse reactions or reduced dronabinol efficacy. Monitoring is advised when combining dronabinol with CYP2C9 inhibitors, such as amiodarone and fluconazole, and CYP3A4 inhibitors, such as ketoconazole, itraconazole, clarithromycin, ritonavir, erythromycin, or grapefruit juice, to detect potential adverse reactions related to dronabinol. Dronabinol strongly binds to plasma proteins, potentially impacting the free fraction of coadministered protein-bound drugs. Although not confirmed in vivo, cautious monitoring is recommended when initiating or increasing the dose of dronabinol or when using highly protein-bound drugs such as cyclosporine and amphotericin B.
Concurrent use of amphetamines, cocaine, and other sympathomimetic drugs may lead to additive hypertension, tachycardia, and potential cardiotoxicity. The concurrent usage of amitriptyline, amoxapine, desipramine, and other tricyclic antidepressants with cannabis may induce additive tachycardia, hypertension, and drowsiness. Concurrent use of barbiturates, benzodiazepines, lithium, buspirone, antihistamines, muscle relaxants, and other CNS depressants may result in significant CNS depression. Marijuana use in combination with disulfiram has been associated with a reversible hypomanic reaction. In addition, hypomania has been reported following the simultaneous use of marijuana with fluoxetine.[58] As the simultaneous use of opioids and marijuana can lead to potentiation, clinicians should be cautious when prescribing opioids to individuals who are using medical cannabis.[59]
Contraindications
Contraindications
Limited standardized information exists regarding contraindications for non–FDA-approved medical cannabis products because composition and dosing vary widely. In contrast, contraindications for FDA-approved cannabinoid pharmaceuticals are clearly defined in product labeling. Dronabinol is contraindicated in patients with a prior hypersensitivity reaction to the active ingredient. Dronabinol capsules (Marinol) are contraindicated in individuals with hypersensitivity to sesame oil, whereas dronabinol oral solution (Syndros) is contraindicated in those with hypersensitivity to alcohol, which is present as an excipient. CBD (Epidiolex) and nabilone (Cesamet) are contraindicated in patients with prior hypersensitivity to the drug or, in the case of nabilone, to cannabinoids.[60]
Warnings and Precautions
Cardiovascular and psychiatric risk: Cannabis and cannabinoid products should be used cautiously in patients with clinically significant cardiovascular disease, such as coronary disease, arrhythmias, or unstable hemodynamics, and in those with a history of psychotic disorders or severe psychiatric illness, as THC-containing products may exacerbate psychiatric symptoms and can alter heart rate and blood pressure. Acute marijuana smoking has been associated with a transient increase in the risk of myocardial infarction during the first hour after use, based on findings from observational trigger studies.[61][62]
Allergy and contamination: Cannabis allergy has been documented, including cross-reactivity with certain plant foods in sensitized individuals; both direct and passive exposure have been reported as triggers in findings from case reports.[63] Patients who are immunocompromised may be at risk from contaminated inhaled cannabis. Invasive fungal infections, including aspergillosis, have been reported in association with cannabis use, and contamination has been documented.[64][65]
Hepatic effects (cannabidiol): Prescription CBD can cause dose-related elevations in transaminases. Concomitant use of valproate along with elevated baseline liver enzymes increases this risk, necessitating monitoring and possible dose adjustment or discontinuation as per the labeling.
Seizure risk (dronabinol): Seizures and seizure-like activity have been reported with dronabinol. Patients should discontinue the medication and seek medical attention if a seizure occurs, and caution is advised in those with a prior seizure history. Individuals with a history of substance use disorder may be at increased risk of misuse.[66]
Cannabidiol
- Hepatic injury: CBD can increase liver transaminases, especially at higher doses or when used with valproate. Regular monitoring of liver enzymes and bilirubin is advised.
- Sedation: Patients should be monitored for signs of drowsiness. Caution is advised when engaging in activities that require alertness, such as driving or operating machinery.
- Suicidal behavior and ideation: Patients should be evaluated for new or worsening suicidal thoughts or behaviors.
- Withdrawal of antiepileptic drugs: CBD dosage should be reduced gradually to lower the risk of increased seizure activity and status epilepticus.
Dronabinol
- Neuropsychiatric adverse reactions: Dronabinol may cause psychiatric and cognitive effects, impairing mental or physical abilities. Therefore, its use should be avoided in patients with a history of psychiatric disorders.
- Hemodynamic instability: Patients with cardiac conditions may experience hypotension, hypertension, syncope, or tachycardia. Clinicians should avoid using drugs with similar effects and monitor patients for changes in blood pressure and heart rate after initiating dronabinol or increasing the dosage.
- Strong CYP3A4 and CYP2C9 inhibitors: Certain azole antifungals and protease inhibitors, such as ritonavir, may increase dronabinol levels. Caution and monitoring are recommended for these interactions.[53]
- Paradoxical nausea, vomiting, or abdominal pain: If these symptoms worsen during treatment, dose reduction or discontinuation of dronabinol should be considered.
Nabilone
- Psychiatric adverse effects: The effects of nabilone are unpredictable after oral administration, with psychiatric reactions potentially lasting 48 to 72 hours after treatment is discontinued.
- Central nervous system effects: Nabilone may affect the CNS, causing dizziness, drowsiness, euphoria, ataxia, anxiety, disorientation, depression, hallucinations, and psychosis.
- Cardiovascular effects: Nabilone can cause tachycardia and orthostatic hypotension.
- Precautions for hazardous activities: Patients taking nabilone should be cautioned against driving, operating machinery, or engaging in other hazardous activities.
Monitoring
Monitoring of patients receiving cannabinoids should be guided by clinical presentation. Clinical monitoring should include assessment for tachycardia, orthostatic hypotension, and behavioral changes.[67] Patients with a history of cannabis use disorder warrant close observation due to the high risk of relapse.[68] Coadministration with CYP inhibitors may lead to toxicity, and concurrent administration with CYP inducers may reduce efficacy, as discussed above. Clinicians should use the prescription drug monitoring program when substance use disorder is suspected.[69] Evaluating alanine transaminase, aspartate transaminase, and total bilirubin levels before initiating treatment, during dose changes, or when changing hepatotoxic medications is crucial.[28]
Clinicians can typically detect marijuana use for approximately 1 to 3 days after exposure in infrequent users, though detection may extend up to 5 days in some cases. In chronic or heavy users, detection may persist for 10 to 30 days or longer, reflecting accumulation of THC in adipose tissue and slow redistribution. Detection times vary based on multiple factors, including frequency and route of use, dose, individual metabolism, body fat composition, and volume of distribution. Detection also depends on the specific analyte measured, as most routine tests identify the inactive metabolite 11-nor-9-carboxy-Δ9-tetrahydrocannabinol (THC-COOH) rather than parent THC. Although immunoassay screening tests may yield presumptive positives, confirmatory testing with more specific methods, such as gas or liquid chromatography-mass spectrometry, can distinguish true positives from rare false positives.
Toxicity
Clinical Features
Data on cannabinoid toxicities remain limited in the literature. The lethal dose has not been established, and studies on dog and monkey models have shown that doses up to 3000 mg/kg do not lead to fatality.[70] Findings from a recent study suggest that electroencephalography can detect acute cannabis consumption. Electroencephalography displays alterations in θ-band oscillatory activity (4-7 Hz); it is not a validated clinical tool for diagnosing cannabis intoxication.[71] Cannabinoid overdose has no known antidote; only supportive therapy is available to help manage the symptoms. Chronic, prolonged, high-volume use of cannabinoids can lead to neuropsychiatric effects, with intelligence quotient and cognition being most impacted.[72] The estimated toxic dose for dronabinol is 30 mg/kg. Illicit synthetic cannabinoids are known to lead to toxicity at much lower doses.
Overdose with dronabinol or nabilone can lead to a range of symptoms affecting the CNS, cardiovascular system, gastrointestinal tract, and autonomic functions. These symptoms may include drowsiness, euphoria, heightened sensory perception, altered time awareness, memory impairment, mood alteration, depersonalization, lethargy, slurred speech, and impaired motor coordination. Autonomic features include dry mouth, reddened conjunctiva, urinary retention, and reduced bowel motility. Tachycardia and postural hypotension are also observed. Individuals with a history of anxiety or nervousness may experience panic reactions, and seizures can occur in patients with known seizure disorders. Psychotic features such as hallucinations, delusions, or paranoia are observed at very high doses. Marijuana toxicity may manifest with clinical features such as tachycardia, postural hypotension, tachypnea, nystagmus, ataxia, euphoria or dysphoria, conjunctival injection, hypotonia, seizures associated with the coingestion of cocaine, impaired cognition, respiratory depression, and coma.[73]
Diagnosis
Following guidance from the Substance Abuse and Mental Health Services Administration, the recommended detection threshold is 50 ng/mL.[23][74]
Management
An anecdote for overdose is not available; only supportive therapy to help manage the symptoms. Discontinuation of the drug is essential. The management of conditions related to marijuana toxicity involves the following actions:
- Maintain airway, breathing, and circulation. In patients with respiratory depression or significantly altered mental status, airway protection and ventilatory support are essential. Hypotension should be managed with intravenous fluids and, if necessary, vasopressors or inotropes. Activated charcoal is preferred for gastrointestinal tract decontamination and may be administered in repeated doses to enhance elimination. Gastric emptying should only be considered if the airway is protected.
- Administer benzodiazepines, such as lorazepam or midazolam, for seizures.
- Treat cannabis hyperemesis syndrome with intravenous fluids and antiemetics, such as ondansetron, and consider haloperidol in refractory cases.[75]
- Consult a psychiatrist following stabilization for patients with cannabis use disorder. Reassurance and verbal support may be sufficient for managing mild-to-moderate psychiatric symptoms. In more severe cases, antipsychotic medications may be used with caution.[76]
Enhancing Healthcare Team Outcomes
A substantial body of literature exists on marijuana and its potential health benefits. However, this evidence consists of observational studies, small trials, or anecdotal reports, depending on the indication. Due to the absence of clinical trials and a lack of a universal formula for marijuana, significant controversies persist regarding the clinical benefits of marijuana. All clinicians, including nurse practitioners and pharmacists, should educate patients that marijuana may not be a panacea for all medical disorders. Marijuana has demonstrated appetite-stimulating and antiemetic effects in specific clinical settings. Until data from randomized clinical trials are available, the recommendation of marijuana use should be approached cautiously, as more evidence seems to indicate that this product may not be entirely safe for long-term consumption.[77][78][79]
Opinions and values regarding the use of cannabinoids in medicine vary widely. Some individuals see cannabinoids as having significant potential to reduce pain, whereas others believe cannabis-derived compounds have no place in modern clinical practice. Regardless of personal values, clinicians should recognize the existence and use of cannabinoids among their patient population when deciding treatment options. Patients should feel comfortable discussing their cannabinoid use, including the type, dose, and CBD-to-THC ratio.[80]
Dronabinol and nabilone are both legal and are available by prescription throughout all 50 states of the United States.[81] The legal status of formulas containing only CBD is more variable. Laws concerning the restriction of products containing THC vary widely across states.[82] If a patient informs the medical staff about using a cannabinoid, this information should be communicated to the primary clinician overseeing their care.
The effective use of cannabinoids for emetic control is best achieved through an interprofessional healthcare team approach. Dronabinol and nabilone are most commonly prescribed by oncologists, palliative care specialists, and infectious disease specialists. Oncologists frequently prescribe cannabinoids alongside chemotherapy regimens.[83] Palliative care and infectious disease specialists often prescribe cannabinoids to provide comfort in the setting of nausea or to benefit from their orexigenic components. In states where medical marijuana is legal, a team of healthcare professionals, including clinicians, nurse practitioners, and physician assistants, can authorize the use of CBD- and THC-containing formulations for patients with various conditions, including nausea and vomiting. Pharmacists play a crucial role in verifying dosing, checking for potential drug interactions, and providing additional counseling to patients as needed.[84]
Findings from a 2019 survey of 178 community-based pharmacists and medical marijuana dispensing pharmacists revealed that both pharmacist groups highly valued opioid use information within the Connecticut Prescription Monitoring and Reporting System. Although approximately 90% of healthcare professionals in both groups checked opioid use, 81.2% of medical marijuana dispensing pharmacists and 38.4% of community-based pharmacists monitored medical marijuana use. Medical marijuana dispensing pharmacists highlighted the need for marijuana-related data for effective counseling. The study underscores the potential benefits of integrating marijuana data into prescription drug monitoring programs, enhancing pharmacist recommendations by addressing drug interactions and workflow issues.[85] The entire clinical picture must be considered when deciding whether to initiate cannabinoid therapy. Triage nurses and clinicians in the emergency department should assess and maintain airway, breathing, and circulation in acute intoxication. Psychiatrists should evaluate for signs of psychosis and administer proper treatment. Critical care clinicians should care for the patient in the intensive care unit. Additionally, clinicians should refer patients with cannabis dependency to social workers. Clinicians, pharmacists, specialists, nurses, and other healthcare professionals are involved in patient care, and an interprofessional approach helps minimize the risk associated with the use of marijuana and its analogs.
Media
(Click Image to Enlarge)
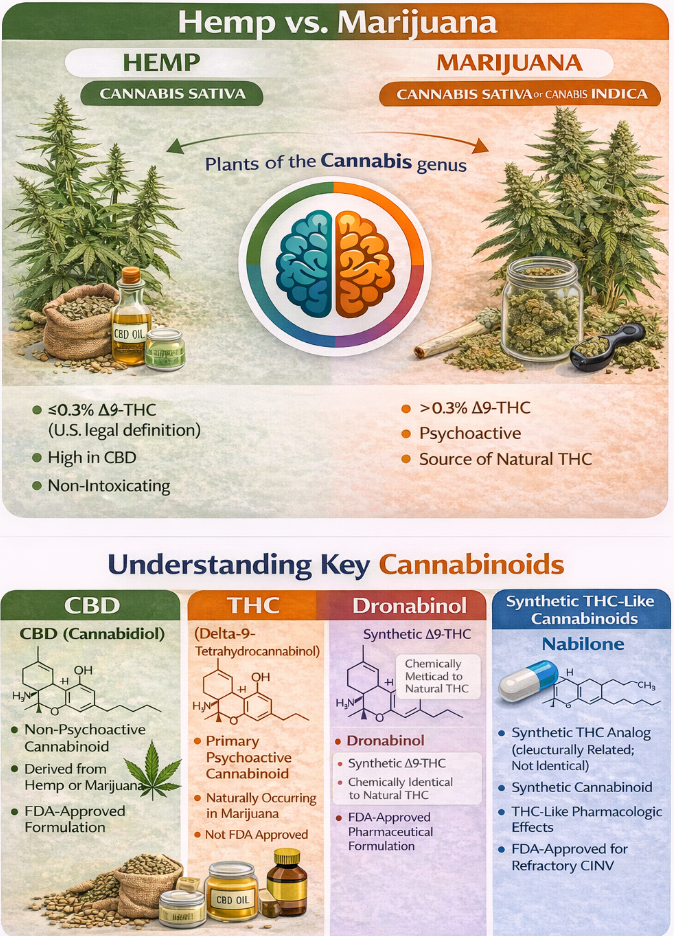
Overview of Key Cannabinoids. A comparison of hemp and marijuana based on their delta-9-tetrahydrocannabinol concentrations as well as various natural and synthetic cannabinoids according to their chemical properties, psychoactive effects, and pharmaceutical status. CINV, chemotherapy-induced nausea and vomiting.
Contributed by P Patel, PharmD
References
Eichhorn Bilodeau S, Wu BS, Rufyikiri AS, MacPherson S, Lefsrud M. An Update on Plant Photobiology and Implications for Cannabis Production. Frontiers in plant science. 2019:10():296. doi: 10.3389/fpls.2019.00296. Epub 2019 Mar 29 [PubMed PMID: 31001288]
Schubert-Bast S, Strzelczyk A. Review of the treatment options for epilepsy in tuberous sclerosis complex: towards precision medicine. Therapeutic advances in neurological disorders. 2021:14():17562864211031100. doi: 10.1177/17562864211031100. Epub 2021 Jul 17 [PubMed PMID: 34349839]
Level 3 (low-level) evidenceAuvin S, Damera V, Martin M, Holland R, Simontacchi K, Saich A. The impact of seizure frequency on quality of life in patients with Lennox-Gastaut syndrome or Dravet syndrome. Epilepsy & behavior : E&B. 2021 Oct:123():108239. doi: 10.1016/j.yebeh.2021.108239. Epub 2021 Aug 7 [PubMed PMID: 34375802]
Level 2 (mid-level) evidenceStrickland JC, Jackson H, Schlienz NJ, Salpekar JA, Martin EL, Munson J, Bonn-Miller MO, Vandrey R. Cross-sectional and longitudinal evaluation of cannabidiol (CBD) product use and health among people with epilepsy. Epilepsy & behavior : E&B. 2021 Sep:122():108205. doi: 10.1016/j.yebeh.2021.108205. Epub 2021 Jul 27 [PubMed PMID: 34311183]
Level 2 (mid-level) evidenceBadowski ME, Yanful PK. Dronabinol oral solution in the management of anorexia and weight loss in AIDS and cancer. Therapeutics and clinical risk management. 2018:14():643-651. doi: 10.2147/TCRM.S126849. Epub 2018 Apr 6 [PubMed PMID: 29670357]
Hesketh PJ, Kris MG, Basch E, Bohlke K, Barbour SY, Clark-Snow RA, Danso MA, Dennis K, Dupuis LL, Dusetzina SB, Eng C, Feyer PC, Jordan K, Noonan K, Sparacio D, Lyman GH. Antiemetics: ASCO Guideline Update. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2020 Aug 20:38(24):2782-2797. doi: 10.1200/JCO.20.01296. Epub 2020 Jul 13 [PubMed PMID: 32658626]
Tomida I, Pertwee RG, Azuara-Blanco A. Cannabinoids and glaucoma. The British journal of ophthalmology. 2004 May:88(5):708-13 [PubMed PMID: 15090428]
Rice J, Hildebrand A, Spain R, Senders A, Silbermann E, Wooliscroft L, Yadav V, Bourdette D, Cameron M. A cross-sectional survey of cannabis use by people with MS in Oregon and Southwest Washington. Multiple sclerosis and related disorders. 2021 Oct:55():103172. doi: 10.1016/j.msard.2021.103172. Epub 2021 Jul 25 [PubMed PMID: 34332457]
Level 2 (mid-level) evidencePantoja-Ruiz C, Restrepo-Jimenez P, Castañeda-Cardona C, Ferreirós A, Rosselli D. Cannabis and pain: a scoping review. Brazilian journal of anesthesiology (Elsevier). 2022 Jan-Feb:72(1):142-151. doi: 10.1016/j.bjane.2021.06.018. Epub 2021 Jul 16 [PubMed PMID: 34280454]
Level 2 (mid-level) evidenceAbi-Jaoude E, Chen L, Cheung P, Bhikram T, Sandor P. Preliminary Evidence on Cannabis Effectiveness and Tolerability for Adults With Tourette Syndrome. The Journal of neuropsychiatry and clinical neurosciences. 2017 Fall:29(4):391-400. doi: 10.1176/appi.neuropsych.16110310. Epub 2017 May 3 [PubMed PMID: 28464701]
May MB, Glode AE. Dronabinol for chemotherapy-induced nausea and vomiting unresponsive to antiemetics. Cancer management and research. 2016:8():49-55. doi: 10.2147/CMAR.S81425. Epub 2016 May 12 [PubMed PMID: 27274310]
Spanagel R, Bilbao A. Approved cannabinoids for medical purposes - Comparative systematic review and meta-analysis for sleep and appetite. Neuropharmacology. 2021 Sep 15:196():108680. doi: 10.1016/j.neuropharm.2021.108680. Epub 2021 Jun 26 [PubMed PMID: 34181977]
Level 2 (mid-level) evidenceBridgeman MB, Abazia DT. Medicinal Cannabis: History, Pharmacology, And Implications for the Acute Care Setting. P & T : a peer-reviewed journal for formulary management. 2017 Mar:42(3):180-188 [PubMed PMID: 28250701]
Zias J, Stark H, Sellgman J, Levy R, Werker E, Breuer A, Mechoulam R. Early medical use of cannabis. Nature. 1993 May 20:363(6426):215 [PubMed PMID: 8387642]
Level 3 (low-level) evidenceMcPartland JM, Agraval J, Gleeson D, Heasman K, Glass M. Cannabinoid receptors in invertebrates. Journal of evolutionary biology. 2006 Mar:19(2):366-73 [PubMed PMID: 16599912]
Level 3 (low-level) evidenceMechoulam R, Fride E, Di Marzo V. Endocannabinoids. European journal of pharmacology. 1998 Oct 16:359(1):1-18 [PubMed PMID: 9831287]
Level 3 (low-level) evidencePremoli M, Aria F, Bonini SA, Maccarinelli G, Gianoncelli A, Pina SD, Tambaro S, Memo M, Mastinu A. Cannabidiol: Recent advances and new insights for neuropsychiatric disorders treatment. Life sciences. 2019 May 1:224():120-127. doi: 10.1016/j.lfs.2019.03.053. Epub 2019 Mar 22 [PubMed PMID: 30910646]
Level 3 (low-level) evidenceBorgelt LM, Franson KL, Nussbaum AM, Wang GS. The pharmacologic and clinical effects of medical cannabis. Pharmacotherapy. 2013 Feb:33(2):195-209. doi: 10.1002/phar.1187. Epub [PubMed PMID: 23386598]
Level 3 (low-level) evidenceBenito C, Núñez E, Tolón RM, Carrier EJ, Rábano A, Hillard CJ, Romero J. Cannabinoid CB2 receptors and fatty acid amide hydrolase are selectively overexpressed in neuritic plaque-associated glia in Alzheimer's disease brains. The Journal of neuroscience : the official journal of the Society for Neuroscience. 2003 Dec 3:23(35):11136-41 [PubMed PMID: 14657172]
Chiarotti M, Costamagna L. Analysis of 11-nor-9-carboxy-delta(9)-tetrahydrocannabinol in biological samples by gas chromatography tandem mass spectrometry (GC/MS-MS). Forensic science international. 2000 Oct 9:114(1):1-6 [PubMed PMID: 10924845]
Musshoff F, Madea B. Review of biologic matrices (urine, blood, hair) as indicators of recent or ongoing cannabis use. Therapeutic drug monitoring. 2006 Apr:28(2):155-63 [PubMed PMID: 16628124]
. Marijuana. LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. 2012:(): [PubMed PMID: 37023245]
Sharma P, Murthy P, Bharath MM. Chemistry, metabolism, and toxicology of cannabis: clinical implications. Iranian journal of psychiatry. 2012 Fall:7(4):149-56 [PubMed PMID: 23408483]
Steigerwald S, Wong PO, Khorasani A, Keyhani S. The Form and Content of Cannabis Products in the United States. Journal of general internal medicine. 2018 Sep:33(9):1426-1428. doi: 10.1007/s11606-018-4480-0. Epub [PubMed PMID: 29770952]
Grotenhermen F. Pharmacokinetics and pharmacodynamics of cannabinoids. Clinical pharmacokinetics. 2003:42(4):327-60 [PubMed PMID: 12648025]
Drug Enforcement Administration, Department of Justice. Schedules of Controlled Substances: Placement in Schedule V of Certain FDA-Approved Drugs Containing Cannabidiol; Corresponding Change to Permit Requirements. Final order. Federal register. 2018 Sep 28:83(189):48950-3 [PubMed PMID: 30272400]
. Dronabinol. LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. 2012:(): [PubMed PMID: 31644137]
. Cannabidiol. LiverTox®: Clinical and Research Information on Drug-Induced Liver Injury. 2012:(): [PubMed PMID: 31644197]
Metz TD, Borgelt LM. Marijuana Use in Pregnancy and While Breastfeeding. Obstetrics and gynecology. 2018 Nov:132(5):1198-1210. doi: 10.1097/AOG.0000000000002878. Epub [PubMed PMID: 30234728]
. Committee Opinion No. 722: Marijuana Use During Pregnancy and Lactation. Obstetrics and gynecology. 2017 Oct:130(4):e205-e209. doi: 10.1097/AOG.0000000000002354. Epub [PubMed PMID: 28937574]
Level 3 (low-level) evidenceHoldsworth EA, Berim A, Gang DR, Williams JE, Smith CB, Caffé B, Brooks O, Barbosa-Leiker C, McGuire MA, McGuire MK, Meehan CL. Human Milk Cannabinoid Concentrations and Associations with Maternal Factors: The Lactation and Cannabis (LAC) Study. Breastfeeding medicine : the official journal of the Academy of Breastfeeding Medicine. 2024 Jul:19(7):515-524. doi: 10.1089/bfm.2024.0021. Epub 2024 May 2 [PubMed PMID: 38695182]
. Cannabidiol. Drugs and Lactation Database (LactMed®). 2006:(): [PubMed PMID: 30601607]
. Cannabis. Drugs and Lactation Database (LactMed®). 2006:(): [PubMed PMID: 30000647]
Chao YS, McCormack S. Medicinal and Synthetic Cannabinoids for Pediatric Patients: A Review of Clinical Effectiveness and Guidelines. 2019 Oct 11:(): [PubMed PMID: 31873990]
Committee on Substance Abuse, Committee on Adolescence, Committee on Substance Abuse Committee on Adolescence. The impact of marijuana policies on youth: clinical, research, and legal update. Pediatrics. 2015 Mar:135(3):584-7. doi: 10.1542/peds.2014-4146. Epub 2015 Jan 26 [PubMed PMID: 25624383]
Volkow ND, Han B, Einstein EB, Compton WM. Prevalence of Substance Use Disorders by Time Since First Substance Use Among Young People in the US. JAMA pediatrics. 2021 Jun 1:175(6):640-643. doi: 10.1001/jamapediatrics.2020.6981. Epub [PubMed PMID: 33779715]
Han BH, Brennan JJ, Orozco MA, Moore AA, Castillo EM. Trends in emergency department visits associated with cannabis use among older adults in California, 2005-2019. Journal of the American Geriatrics Society. 2023 Apr:71(4):1267-1274. doi: 10.1111/jgs.18180. Epub 2023 Jan 9 [PubMed PMID: 36622838]
Posis A, Bellettiere J, Liles S, Alcaraz J, Nguyen B, Berardi V, Klepeis NE, Hughes SC, Wu T, Hovell MF. Indoor cannabis smoke and children's health. Preventive medicine reports. 2019 Jun:14():100853. doi: 10.1016/j.pmedr.2019.100853. Epub 2019 Mar 16 [PubMed PMID: 30976488]
Freeman TP, Hindocha C, Green SF, Bloomfield MAP. Medicinal use of cannabis based products and cannabinoids. BMJ (Clinical research ed.). 2019 Apr 4:365():l1141. doi: 10.1136/bmj.l1141. Epub 2019 Apr 4 [PubMed PMID: 30948383]
Ugradar S, Manta A, Flanagan D. Unilateral cilioretinal artery occlusion following cannabis use. Therapeutic advances in ophthalmology. 2019 Jan-Dec:11():2515841419838661. doi: 10.1177/2515841419838661. Epub 2019 Mar 27 [PubMed PMID: 30944891]
Level 3 (low-level) evidenceDrummer OH, Gerostamoulos D, Woodford NW. Cannabis as a cause of death: A review. Forensic science international. 2019 May:298():298-306. doi: 10.1016/j.forsciint.2019.03.007. Epub 2019 Mar 14 [PubMed PMID: 30925348]
Degenhardt L, Coffey C, Romaniuk H, Swift W, Carlin JB, Hall WD, Patton GC. The persistence of the association between adolescent cannabis use and common mental disorders into young adulthood. Addiction (Abingdon, England). 2013 Jan:108(1):124-33. doi: 10.1111/j.1360-0443.2012.04015.x. Epub 2012 Oct 18 [PubMed PMID: 22775447]
Mustonen A, Niemelä S, Nordström T, Murray GK, Mäki P, Jääskeläinen E, Miettunen J. Adolescent cannabis use, baseline prodromal symptoms and the risk of psychosis. The British journal of psychiatry : the journal of mental science. 2018 Apr:212(4):227-233. doi: 10.1192/bjp.2017.52. Epub [PubMed PMID: 29557758]
Stefani A, Aramini B, Baraldi C, Pellesi L, Della Casa G, Morandi U, Guerzoni S. Secondary spontaneous pneumothorax and bullous lung disease in cannabis and tobacco smokers: A case-control study. PloS one. 2020:15(3):e0230419. doi: 10.1371/journal.pone.0230419. Epub 2020 Mar 30 [PubMed PMID: 32226050]
Level 2 (mid-level) evidenceGundersen TD, Jørgensen N, Andersson AM, Bang AK, Nordkap L, Skakkebæk NE, Priskorn L, Juul A, Jensen TK. Association Between Use of Marijuana and Male Reproductive Hormones and Semen Quality: A Study Among 1,215 Healthy Young Men. American journal of epidemiology. 2015 Sep 15:182(6):473-81. doi: 10.1093/aje/kwv135. Epub 2015 Aug 16 [PubMed PMID: 26283092]
Level 2 (mid-level) evidenceMeier MH, Caspi A, Cerdá M, Hancox RJ, Harrington H, Houts R, Poulton R, Ramrakha S, Thomson WM, Moffitt TE. Associations Between Cannabis Use and Physical Health Problems in Early Midlife: A Longitudinal Comparison of Persistent Cannabis vs Tobacco Users. JAMA psychiatry. 2016 Jul 1:73(7):731-40. doi: 10.1001/jamapsychiatry.2016.0637. Epub [PubMed PMID: 27249330]
Callaghan RC, Sanches M, Kish SJ. Quantity and frequency of cannabis use in relation to cannabis-use disorder and cannabis-related problems. Drug and alcohol dependence. 2020 Dec 1:217():108271. doi: 10.1016/j.drugalcdep.2020.108271. Epub 2020 Sep 11 [PubMed PMID: 32977043]
Auer R, Vittinghoff E, Yaffe K, Künzi A, Kertesz SG, Levine DA, Albanese E, Whitmer RA, Jacobs DR Jr, Sidney S, Glymour MM, Pletcher MJ. Association Between Lifetime Marijuana Use and Cognitive Function in Middle Age: The Coronary Artery Risk Development in Young Adults (CARDIA) Study. JAMA internal medicine. 2016 Mar:176(3):352-61. doi: 10.1001/jamainternmed.2015.7841. Epub [PubMed PMID: 26831916]
Lapoint J, Meyer S, Yu CK, Koenig KL, Lev R, Thihalolipavan S, Staats K, Kahn CA. Cannabinoid Hyperemesis Syndrome: Public Health Implications and a Novel Model Treatment Guideline. The western journal of emergency medicine. 2018 Mar:19(2):380-386. doi: 10.5811/westjem.2017.11.36368. Epub 2017 Nov 8 [PubMed PMID: 29560069]
Chadi N, Levy S. What Every Pediatric Gynecologist Should Know About Marijuana Use in Adolescents. Journal of pediatric and adolescent gynecology. 2019 Aug:32(4):349-353. doi: 10.1016/j.jpag.2019.03.004. Epub 2019 Mar 26 [PubMed PMID: 30923025]
Giano Z, Hubach RD, Currin JM, Wheeler DL. Adverse childhood experiences and MSM marijuana use. Drug and alcohol dependence. 2019 May 1:198():76-79. doi: 10.1016/j.drugalcdep.2019.01.024. Epub 2019 Feb 27 [PubMed PMID: 30878770]
Ronen A, Chassidim HS, Gershon P, Parmet Y, Rabinovich A, Bar-Hamburger R, Cassuto Y, Shinar D. The effect of alcohol, THC and their combination on perceived effects, willingness to drive and performance of driving and non-driving tasks. Accident; analysis and prevention. 2010 Nov:42(6):1855-65. doi: 10.1016/j.aap.2010.05.006. Epub 2010 Jun 9 [PubMed PMID: 20728636]
Level 1 (high-level) evidenceWatanabe K, Yamaori S, Funahashi T, Kimura T, Yamamoto I. Cytochrome P450 enzymes involved in the metabolism of tetrahydrocannabinols and cannabinol by human hepatic microsomes. Life sciences. 2007 Mar 20:80(15):1415-9 [PubMed PMID: 17303175]
Antoniou T, Bodkin J, Ho JM. Drug interactions with cannabinoids. CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne. 2020 Mar 2:192(9):E206. doi: 10.1503/cmaj.191097. Epub [PubMed PMID: 32122975]
Devinsky O, Patel AD, Thiele EA, Wong MH, Appleton R, Harden CL, Greenwood S, Morrison G, Sommerville K, GWPCARE1 Part A Study Group. Randomized, dose-ranging safety trial of cannabidiol in Dravet syndrome. Neurology. 2018 Apr 3:90(14):e1204-e1211. doi: 10.1212/WNL.0000000000005254. Epub 2018 Mar 14 [PubMed PMID: 29540584]
Level 1 (high-level) evidenceBen-Menachem E, Gunning B, Arenas Cabrera CM, VanLandingham K, Crockett J, Critchley D, Wray L, Tayo B, Morrison G, Toledo M. A Phase II Randomized Trial to Explore the Potential for Pharmacokinetic Drug-Drug Interactions with Stiripentol or Valproate when Combined with Cannabidiol in Patients with Epilepsy. CNS drugs. 2020 Jun:34(6):661-672. doi: 10.1007/s40263-020-00726-4. Epub [PubMed PMID: 32350749]
Level 1 (high-level) evidenceWray L, Berwaerts J, Critchley D, Hyland K, Chen C, Thai C, Tayo B. Pharmacokinetic Drug-Drug Interaction With Coadministration of Cannabidiol and Everolimus in a Phase 1 Healthy Volunteer Trial. Clinical pharmacology in drug development. 2023 Sep:12(9):911-919. doi: 10.1002/cpdd.1262. Epub 2023 May 3 [PubMed PMID: 37132402]
Lucas CJ, Galettis P, Schneider J. The pharmacokinetics and the pharmacodynamics of cannabinoids. British journal of clinical pharmacology. 2018 Nov:84(11):2477-2482. doi: 10.1111/bcp.13710. Epub 2018 Aug 7 [PubMed PMID: 30001569]
Reisfield GM. Medical cannabis and chronic opioid therapy. Journal of pain & palliative care pharmacotherapy. 2010 Dec:24(4):356-61. doi: 10.3109/15360288.2010.519431. Epub [PubMed PMID: 21133743]
Level 3 (low-level) evidenceSkypala IJ, Jeimy S, Brucker H, Nayak AP, Decuyper II, Bernstein JA, Connors L, Kanani A, Klimek L, Lo SCR, Murphy KR, Nanda A, Poole JA, Walusiak-Skorupa J, Sussman G, Zeiger JS, Goodman RE, Ellis AK, Silvers WS, Ebo DG, International Cannabis Allergy Collaboration. Cannabis-related allergies: An international overview and consensus recommendations. Allergy. 2022 Jul:77(7):2038-2052. doi: 10.1111/all.15237. Epub 2022 Feb 14 [PubMed PMID: 35102560]
Level 3 (low-level) evidenceCavazos-Rehg PA, Krauss MJ, Cahn E, Lee KE, Ferguson E, Rajbhandari B, Sowles SJ, Floyd GM, Berg C, Bierut LJ. Marijuana Promotion Online: an Investigation of Dispensary Practices. Prevention science : the official journal of the Society for Prevention Research. 2019 Feb:20(2):280-290. doi: 10.1007/s11121-018-0889-2. Epub [PubMed PMID: 29629505]
Kahan M, Srivastava A. New medical marijuana regulations: the coming storm. CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne. 2014 Sep 2:186(12):895-6. doi: 10.1503/cmaj.131821. Epub 2014 Jun 23 [PubMed PMID: 24958833]
Hoffman BC, Kuhl M, Harbeck RJ, Rabinovitch N. Cannabis allergy in a child with asthma chronically exposed to marijuana. The journal of allergy and clinical immunology. In practice. 2020 Jan:8(1):422-423. doi: 10.1016/j.jaip.2019.06.042. Epub 2019 Jul 16 [PubMed PMID: 31323337]
Szyper-Kravitz M, Lang R, Manor Y, Lahav M. Early invasive pulmonary aspergillosis in a leukemia patient linked to aspergillus contaminated marijuana smoking. Leukemia & lymphoma. 2001 Nov-Dec:42(6):1433-7 [PubMed PMID: 11911432]
Level 3 (low-level) evidenceThompson GR 3rd, Tuscano JM, Dennis M, Singapuri A, Libertini S, Gaudino R, Torres A, Delisle JM, Gillece JD, Schupp JM, Engelthaler DM. A microbiome assessment of medical marijuana. Clinical microbiology and infection : the official publication of the European Society of Clinical Microbiology and Infectious Diseases. 2017 Apr:23(4):269-270. doi: 10.1016/j.cmi.2016.12.001. Epub 2016 Dec 9 [PubMed PMID: 27956269]
Degenhardt L, Hall W, Lynskey M. The relationship between cannabis use and other substance use in the general population. Drug and alcohol dependence. 2001 Nov 1:64(3):319-27 [PubMed PMID: 11672946]
Rezkalla S, Kloner RA. Cardiovascular effects of marijuana. Trends in cardiovascular medicine. 2019 Oct:29(7):403-407. doi: 10.1016/j.tcm.2018.11.004. Epub 2018 Nov 10 [PubMed PMID: 30447899]
Lattanzi S, Brigo F, Trinka E, Zaccara G, Cagnetti C, Del Giovane C, Silvestrini M. Efficacy and Safety of Cannabidiol in Epilepsy: A Systematic Review and Meta-Analysis. Drugs. 2018 Nov:78(17):1791-1804. doi: 10.1007/s40265-018-0992-5. Epub [PubMed PMID: 30390221]
Level 1 (high-level) evidenceSteuart SR. The addition of cannabis to prescription drug monitoring programs and medication fills in Medicaid. Health economics. 2025 Feb:34(2):283-296. doi: 10.1002/hec.4911. Epub 2024 Nov 4 [PubMed PMID: 39496576]
Brutlag A, Hommerding H. Toxicology of Marijuana, Synthetic Cannabinoids, and Cannabidiol in Dogs and Cats. The Veterinary clinics of North America. Small animal practice. 2018 Nov:48(6):1087-1102. doi: 10.1016/j.cvsm.2018.07.008. Epub [PubMed PMID: 30342565]
Level 3 (low-level) evidenceSchiemer C, Summers MJ, Stefanidis KB. Identifying EEG markers related to acute cannabis consumption: A systematic review. Neuroscience and biobehavioral reviews. 2025 May:172():106092. doi: 10.1016/j.neubiorev.2025.106092. Epub 2025 Mar 6 [PubMed PMID: 40057256]
Level 1 (high-level) evidenceBraidwood R, Mansell S, Waldron J, Rendell PG, Kamboj SK, Curran HV. Non-Dependent and Dependent Daily Cannabis Users Differ in Mental Health but Not Prospective Memory Ability. Frontiers in psychiatry. 2018:9():97. doi: 10.3389/fpsyt.2018.00097. Epub 2018 Mar 27 [PubMed PMID: 29636705]
Appelboam A, Oades PJ. Coma due to cannabis toxicity in an infant. European journal of emergency medicine : official journal of the European Society for Emergency Medicine. 2006 Jun:13(3):177-9 [PubMed PMID: 16679885]
Level 3 (low-level) evidenceKulig K. Interpretation of Workplace Tests for Cannabinoids. Journal of medical toxicology : official journal of the American College of Medical Toxicology. 2017 Mar:13(1):106-110. doi: 10.1007/s13181-016-0587-z. Epub 2016 Sep 29 [PubMed PMID: 27686239]
Hickey JL, Witsil JC, Mycyk MB. Haloperidol for treatment of cannabinoid hyperemesis syndrome. The American journal of emergency medicine. 2013 Jun:31(6):1003.e5-6. doi: 10.1016/j.ajem.2013.02.021. Epub 2013 Apr 10 [PubMed PMID: 23583118]
Level 3 (low-level) evidenceWilson RP, Bhattacharyya S. Antipsychotic efficacy in psychosis with co-morbid cannabis misuse: A systematic review. Journal of psychopharmacology (Oxford, England). 2016 Feb:30(2):99-111. doi: 10.1177/0269881115612237. Epub 2015 Oct 28 [PubMed PMID: 26510450]
Level 1 (high-level) evidenceWisk LE, Levy S, Weitzman ER. Parental views on state cannabis laws and marijuana use for their medically vulnerable children. Drug and alcohol dependence. 2019 Jun 1:199():59-67. doi: 10.1016/j.drugalcdep.2018.12.027. Epub 2019 Feb 14 [PubMed PMID: 30999251]
Artukoglu BB, Bloch MH. The Potential of Cannabinoid-Based Treatments in Tourette Syndrome. CNS drugs. 2019 May:33(5):417-430. doi: 10.1007/s40263-019-00627-1. Epub [PubMed PMID: 30977108]
Friedman D, French JA, Maccarrone M. Safety, efficacy, and mechanisms of action of cannabinoids in neurological disorders. The Lancet. Neurology. 2019 May:18(5):504-512. doi: 10.1016/S1474-4422(19)30032-8. Epub 2019 Mar 22 [PubMed PMID: 30910443]
Leen NA, Kowal MA, Batalla A, Bossong MG. The effects of standardized cannabis products in healthy volunteers and patients: a systematic literature review. Frontiers in pharmacology. 2024:15():1411631. doi: 10.3389/fphar.2024.1411631. Epub 2024 Oct 17 [PubMed PMID: 39484170]
Level 1 (high-level) evidenceRubin R. The Path to the First FDA-Approved Cannabis-Derived Treatment and What Comes Next. JAMA. 2018 Sep 25:320(12):1227-1229. doi: 10.1001/jama.2018.11914. Epub [PubMed PMID: 30193358]
Corroon J, Kight R. Regulatory Status of Cannabidiol in the United States: A Perspective. Cannabis and cannabinoid research. 2018:3(1):190-194. doi: 10.1089/can.2018.0030. Epub 2018 Sep 27 [PubMed PMID: 30283822]
Level 3 (low-level) evidenceZylla D, Steele G, Eklund J, Mettner J, Arneson T. Oncology Clinicians and the Minnesota Medical Cannabis Program: A Survey on Medical Cannabis Practice Patterns, Barriers to Enrollment, and Educational Needs. Cannabis and cannabinoid research. 2018:3(1):195-202. doi: 10.1089/can.2018.0029. Epub 2018 Oct 1 [PubMed PMID: 30426072]
Level 3 (low-level) evidenceSchmitz N, Richert L. Pharmacists and the future of cannabis medicine. Journal of the American Pharmacists Association : JAPhA. 2020 Jan-Feb:60(1):207-211. doi: 10.1016/j.japh.2019.11.007. Epub 2019 Dec 20 [PubMed PMID: 31870860]
Rickles NM, Wakai S, Karim-Nejad L. The use of an integrated opioid and medical marijuana prescription drug monitoring program. Journal of the American Pharmacists Association : JAPhA. 2021 Jul-Aug:61(4):408-417. doi: 10.1016/j.japh.2021.02.020. Epub 2021 Mar 4 [PubMed PMID: 33903060]