Introduction
Lymph nodes are anatomical structures distributed throughout the lymphatic vascular system. This system mediates the drainage of excess interstitial fluid generated at the interface between blood capillaries and tissues. Interstitial fluid enters lymphatic vessels and is subsequently termed "lymph." Lymph returns to the systemic circulation at the jugulovenous angles after passage through at least 1 lymph node.
Lymph nodes function in lymph filtration and immunologic surveillance. Particulate matter is removed from lymph and degraded by macrophages. Malignant cells, antigens, and microorganisms are captured and processed by antigen-presenting cells. Antigen presentation facilitates interaction with naive B and T lymphocytes that enter the node via the blood supply, enabling activation of an adaptive immune response.
This activity provides an overview of lymph node microanatomy in relation to function. The gross anatomical organization of lymph nodes within the lymphatic vascular system is also reviewed.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Lymph Nodes as Part of the Lymphatic Vascular System
The Starling law of the capillaries dictates that fluid is filtered into the interstitium from capillary blood vessels near arterioles and resorbed into capillary blood vessels near venules. [Preston & Wilson. Lippincott Illustrated Reviews: Physiology, 3rd ed. Blood and the Vasculature. 2025] Depending on the tissue, an excess of approximately 10% of filtration over resorption occurs, with excess interstitial fluid drained by the lymphatic vascular system.
The interstitial fluid passes into lymphatic capillaries, from which point it is termed "lymph." [Pawlina. Histology: A Text and Atlas: With Correlated Cell and Molecular Biology, 9th ed. Cardiovascular System. 2024] Lymphatic capillaries convey lymph into collecting lymphatic vessels, which converge to form larger lymphatic trunks.[1] Along this course, lymph flows through regional and collecting lymph nodes (the latter receiving lymph from multiple regional nodes), where filtration and immune surveillance are performed.
Lymph is eventually deposited into 1 of 2 large ducts. Lymph from the upper right quadrant of the body flows into the right lymphatic duct, which returns it to the blood circulation at the right jugulovenous angle near the confluence of the right internal jugular vein and the right subclavian vein. Lymph from the upper left quadrant and both lower quadrants flows into the thoracic duct, which delivers the fluid to the left jugulovenous angle. [Paulsen & Waschke, eds. Sobotta Atlas of Anatomy, 16th ed. Musculoskeletal System. 2018]
Structure
The lymph node is a bean-shaped structure (see Image. Structure and Histology of a Lymph Node). The convex surface receives afferent lymphatic vessels. The concave surface serves as the exit point for efferent lymphatic vessels and the entry point for blood vessels supplying the node. Physiological lymph node size varies by location, typically ranging from 1 to 20 mm. Parts of the lymph node are explained below.
The capsule is the outermost layer, composed of connective tissue, and provides structural support while separating the node from surrounding tissues. Trabeculae extend from the capsule into the interior of the lymph node. These structures are likewise composed of connective tissue and contribute to internal support.
The following structures are characterized by the presence of reticular cells within their architecture, which synthesize type III collagen, forming a supportive framework for immune cells:
- Superficial cortex: Composed of B lymphocytes associated with follicular dendritic cells and organized into primary follicles. Germinal centers form following B lymphocyte activation, and cellular proliferation occurs. Follicles in this state are designated secondary follicles.
- Deep cortex: Composed of T lymphocytes associated with dendritic cells and organized into structures known as deep cortical units. Activated T lymphocytes undergo proliferation but do not form germinal centers.
- Medulla: Organized into medullary cords containing plasma cells derived from B lymphocytes originating in the superficial cortex.
Sinuses are vessel-like spaces within the lymph node through which lymph flows. The lumen contains a meshwork formed by processes of antigen-presenting cells and type III collagen. The subcapsular sinus is located between the capsule and cortex and represents the most superficial compartment of the lymph node, where lymph initially enters. Trabecular sinuses extend from the subcapsular sinus and permit the passage of lymph toward medullary sinuses located in the deep cortex. From the medullary sinuses, lymph flows into efferent lymphatic vessels and exits the node.
Blood vessels are also present, with high endothelial venules playing a key role in lymphocyte trafficking into the node. High endothelial venules supply most lymphocytes, which enter via diapedesis facilitated by endothelial adhesion molecules.
Function
Several processes demonstrate the role of lymph nodes in lymph filtration and immune surveillance. High endothelial venules allow entry of naive B and T lymphocytes, defined as mature immune cells that have not yet encountered their specific antigen. Chemokine signaling determines segregation of these lymphocytes into the superficial and deep cortex, respectively. Lymphocytes may be activated by antigen exposure and undergo proliferation following localization within the lymph node. In the absence of an antigen, lymphocytes eventually exit via efferent lymphatic vessels.
Lymph may contain antigens and bacteria that have breached primary immune defenses and entered the interstitial fluid. The mesh-like structure within the sinuses facilitates antigen filtration and endocytosis, resulting in activation of B and T lymphocytes. Activated B lymphocytes differentiate into plasma cells, plasmablasts, and memory B cells. Plasma cells migrate to medullary cords and produce antigen-specific antibodies, which are released into lymph within the medullary sinuses.
Lymph may also contain cellular debris, erythrocytes, or carbon particles. This material is removed via macrophage-mediated phagocytosis within the sinuses.[2]
Embryology
Lymph nodes begin development in utero as mesenchymal condensations, which later bulge to form lymph sacs. At 13 weeks of gestation, the T-cell region begins development. By 17 weeks of gestation, interdigitating reticulum cells (a subtype of T cells) are present in the paracortical region of the lymph node, surrounded by lymphoid cells. B-cell regions within lymph nodes begin development at 14 weeks of gestation at the marginal sinus, with populations including dendritic reticulum cell precursors, lymphoblasts, immunoblasts, and plasmablasts. By 20 weeks of gestation, incipient primary follicles are present in the outer cortex and contain lymphocytes. Lymph nodes undergo granulopoiesis and erythropoiesis between 12 and 14 weeks of gestation, producing undifferentiated blast cells, monocytes, and macrophages transiently.[3][4]
Blood Supply and Lymphatics
Overview
As previously described, lymph from the upper right quadrant of the body is directed into the right lymphatic duct, whereas lymph from the remainder of the body is directed into the thoracic duct. This asymmetry reflects differences in the lymphatic trunks that drain into each duct (see Image. Lymphatic System). The right lymphatic duct receives lymph from the right subclavian trunk. The right subclavian trunk collects lymph from the right upper extremity and the right side of the body wall down to the level of the umbilicus. The right lymphatic duct receives lymph from the right bronchomediastinal trunk. The right bronchomediastinal trunk collects lymph from the thoracic cavity. The right lymphatic duct receives lymph from the right jugular trunk, which collects lymph from the right side of the head. The thoracic duct receives lymph from corresponding left-sided lymphatic trunks and, additionally, from the cisterna chyli, thereby draining lymph from the abdominal viscera below the diaphragm, the abdominal wall below the umbilicus, and both lower extremities.
Lymph Nodes of the Lower Extremity
Popliteal lymph nodes are located in the popliteal fossa, a space bounded by the semimembranosus, semitendinosus, and gastrocnemius muscles, posterior to the distal femur. [Nichols & Ashford. Orthopaedics and Trauma. Surgical anatomy & pathology of the popliteal fossa. 2013] Efferent vessels from these nodes drain into the inguinal lymph nodes. Inguinal lymph nodes are arranged into a vertical chain that runs along the great saphenous vein and a horizontal group located inferior to the inguinal ligament. In addition to afferent lymphatic vessels from the lower extremity, the inguinal lymph nodes receive lymph from the lower abdominal wall and lower back, up to the level of the umbilicus.
Visceral Lymph Nodes Below the Diaphragm
Efferent lymphatics from the inguinal nodes are directed into the external iliac lymph nodes. External iliac lymph nodes are divided into lateral, intermediate, and medial groups. The lateral group lies lateral to the external iliac artery. The intermediate group lies medial to the external iliac artery. The medial group lies medial to the external iliac vein. Efferent lymphatics from the external iliac nodes are directed to the common iliac nodes.
Common iliac nodes are likewise divided into lateral, intermediate, and medial groups. The lateral group is located lateral to the common iliac artery. The intermediate group lies alongside the common iliac artery. The medial group is situated medial to the common iliac artery.[5] Internal iliac nodes, which receive lymph from pelvic viscera, also direct efferent lymphatics into the common iliac nodes. Common iliac nodes drain into the retroperitoneal region, where lymph is received by the lumbar lymph nodes, which are divided into 3 groups. Left lumbar lymph nodes are located near the aorta. Intermediate lumbar lymph nodes are located between the aorta and the inferior vena cava. The right lumbar lymph nodes are located near the inferior vena cava. Common iliac nodes also receive efferent lymphatics from the kidneys and adrenal glands.
Lumbar trunks arise from the common iliac nodes and drain into the cisterna chyli. The cisterna chyli is a saccular lymphatic structure of variable size and morphology, typically located near the aorta at the level of the L1–L2 vertebral bodies. Formation of the cisterna chyli occurs through the confluence of the bilateral lumbar trunks with the intestinal trunk, which collects lymph from the mesentery and abdominal viscera.[6] The cisterna chyli gives rise to the thoracic duct, which ascends through the diaphragm and drains into the left jugulovenous angle.
Visceral Lymph Nodes of the Thorax
In the thorax, the lungs contain 2 parallel lymphatic drainage systems: the peribronchial system, which follows the bronchi, and the subpleural system, which lies more superficially. Both systems converge at the tracheobronchial lymph nodes.
Tracheobronchial lymph nodes, together with the brachiocephalic lymph nodes—which drain the thymus, thyroid gland, and pericardium—provide afferent drainage to the bronchomediastinal trunks. The right and left bronchomediastinal trunks drain into the right lymphatic duct and thoracic duct, respectively.[7] [Paulsen & Waschke, eds. Sobotta Atlas of Anatomy, 16th ed. Internal Organs. 2018]
Lymph Nodes of the Upper Extremity
The upper extremity contains cubital lymph nodes located within the cubital fossa, which is bounded by the pronator teres and brachioradialis muscles and lies anterior to the distal humerus. Afferent lymphatics from the upper extremity are directed into the axillary lymph nodes, which additionally receive afferent lymphatics from the trunk wall up to the level of the umbilicus (see Image. Anatomy of Axillary Lymph Nodes). Axillary lymph nodes are frequently discussed in the context of breast cancer metastasis, with a clinical division into 3 levels and sequential spread from levels I to III.[8] [Ciesla, et al. Nowotwory Journal of Oncology. The surgical anatomy of the mammary gland. Vascularisation, innervation, lymphatic drainage, the structure of the axillary fossa (part 2). 2021]
Level I contains nodes lateral and inferior to the pectoralis minor muscle. This group includes pectoral nodes near the lateral thoracic artery and vein, subscapular nodes near the subscapular artery and vein, and lateral axillary nodes near the axillary artery and vein. Level II nodes lie on the pectoralis minor (interpectoral nodes) or posterior to this muscle (central axillary nodes). Level III nodes are located medial to the pectoralis minor and include apical axillary nodes. Efferent vessels from apical axillary nodes drain into the subclavian trunks and subsequently into the major lymphatic ducts. A clinically less significant lymphatic pathway drains lymph from the medial portions of the breast into the parasternal lymph nodes.[9]
Recent years have seen the development of revised lymph node classification systems intended to better reflect patterns of lymphatic drainage from the breast in the context of cancer metastasis.[10] The Clough classification replaces levels I and II with 4 zones labeled A to D. A lateral reference line is formed by the 2nd intercostobrachial nerve, and a vertical reference line is formed by the lateral thoracic vein, dividing the region into 4 quadrants. Zone A is located in the medial inferior quadrant, medial to the lateral thoracic vein and inferior to the 2nd intercostobrachial nerve. Zone B occupies the medial superior quadrant. Zone C corresponds to the lateral inferior quadrant. Zone D comprises the lateral superior quadrant.
Lymph Nodes of the Head and Neck
Regional lymph nodes of the head include occipital nodes located at the lateral border of the trapezius muscles and mastoid nodes located at the insertion of the SCM on the mastoid process of the temporal bone. Parotid nodes are divided into superficial and deep groups. Facial nodes include malar nodes located in the infraorbital region, as well as buccinator nodes and mandibular nodes. Regional lymph nodes of the head give rise to efferent lymphatics that direct lymph toward the neck. Lymphatic drainage in the neck is described in 2 contexts: lymphatic cervical chains and anatomical levels of dissection. Lymphatic cervical chains consist of large lymphatic vessels containing interspersed lymph nodes. Anatomically, the neck is divided into 6 levels of dissection.
The most significant lymphatic drainage pathway of the neck is the deep lateral cervical chain, which occupies levels II, III, and IV. These levels are arranged vertically, with a common lateral border formed by the medial surface of the SCM and a medial border formed by the internal carotid artery in level II or the common carotid artery in levels III and IV. Level II extends from the base of the skull to the hyoid bone and is bounded anteriorly by the submandibular gland. Level II contains the superior deep lateral cervical nodes. Level III extends from the hyoid bone to the cricoid cartilage, is bounded anteriorly by the anterior border of the SCM, and contains the middle deep lateral cervical nodes. Level IV extends from the cricoid cartilage to the clavicle, is also bounded anteriorly by the anterior border of the SCM, and contains the inferior deep lateral cervical nodes. Efferents from the deep lateral cervical chain drain into the jugular trunks, which direct lymph into 1 of the 2 major lymphatic ducts.
Another major lymphatic drainage pathway of the neck is the deep posterior cervical chain, which occupies level V. This level corresponds to the region bounded anteriorly by the posterior border of the SCM and posteriorly by the anterior border of the trapezius. Vertically, the region is bounded by the hyoid bone superiorly and the transverse cervical vessels inferiorly. Unlike the lateral cervical region, the posterior cervical region is not subdivided into multiple levels. Nodes within this region are classified as superior, middle, and inferior deep posterior cervical lymph nodes. Additional lymphatic pathways include the superficial lateral jugular chain, the superficial anterior jugular chain, and the deep anterior cervical chain.
Level I is located in the floor of the mouth and is subdivided into levels Ia and Ib. Level Ia is located anterior to level Ib and contains submental nodes (see Image. Lymphatics of the Tongue). Level Ib contains submandibular nodes.
Levels II, III, IV, and V have been described above. Level VI corresponds to the anterior cervical compartment, located between the anterior borders of the SCMs. This compartment is vertically bounded by the hyoid bone superiorly and the manubrium of the sternum inferiorly. Level VI contains anterior jugular nodes as well as nodes associated with the trachea and thyroid gland.[11][12] In addition to conventional lymphatic drainage, a brain-specific fluid-clearance network called the "glymphatic system" directs waste-laden cerebrospinal and interstitial fluid from the parenchyma toward cervical lymph nodes.[13]
Clinical Significance
The lymphatic system is involved in infectious, inflammatory, and malignant disease processes. Therefore, lymph node enlargement may result from multiple etiologies. Endoscopic ultrasound with or without fine-needle aspiration may aid diagnosis in cases of lymphadenopathy of unclear origin.[14] This diagnostic approach demonstrates high accuracy, with reported sensitivity of up to 85% and specificity of 100%, and plays a key role in malignancy detection and staging.[15] Elastography has an increasingly important diagnostic role when lymph nodes are not accessible for fine-needle sampling, functioning in a manner analogous to a virtual biopsy.[16]
Functional and anatomical information may also be obtained through conventional imaging modalities such as positron emission tomography combined with computed tomography. However, this approach is typically performed as whole-body imaging and is associated with relatively high exposure to ionizing radiation. Despite advances in imaging techniques, diagnosis continues to rely heavily on clinical correlation with patient symptoms.
Other Issues
Subcapsular Proliferative Foci
Subcapsular proliferative foci (SPFs) are transient, flattened aggregates of activated B lymphocytes beneath the subcapsular sinus that arise during antigen re-exposure, specifically to particulate antigens delivered via afferent lymphatics. These inducible niches contain activated B cells, subcapsular sinus macrophages, and T-helper cell interactions at the cortex–paracortex interface, and their proliferation precedes classical germinal center formation, driving rapid plasmablast differentiation and early antibody production.
SPFs represent a distinct anatomical compartment, spatially segregated from follicle–paracortex–medulla zoning, and contribute to layered humoral-recall responses within the node. Expansion of these foci is common in acute infection and inflammation and supports early antibody generation while limiting antigen spread. No direct role in neoplasia is established, although reactive patterns may occur in oncologic settings.
Microscopically, SPFs appear as thin, flattened, capsule-conforming sheets of lymphocytes rather than rounded follicles, reflecting their surface-oriented, inducible architecture.[17] Their organization as a rapid-response B-cell memory niche suggests that SPFs may be strategically targeted to enhance secondary antibody responses and improve vaccine efficacy.[18]
Intranodal Lympho-Venous Shunts
High-resolution imaging in mammalian models has demonstrated intranodal lympho-venous shunts that connect lymphatic sinuses directly to intranodal venous channels. This finding challenges the traditional model of strictly unidirectional lymph flow through efferent lymphatics. Evidence suggests potential intranodal bypass pathways for fluid and cellular transit into the bloodstream. Functional implications include modulation of intranodal fluid clearance and redistribution, with possible effects on edema resolution and metastatic cell trafficking within the lymph node microarchitecture.[19]
Updates on Nodal-Based Cancer Staging
Recent updates to the TNM (tumor, node, metastasis) classification have moved beyond the traditional binary designation of “node-positive versus node-negative,” which has limited prognostic value. Current staging frameworks require more granular reporting, including the absolute number of metastatic lymph nodes, involvement of specific nodal stations, and lymph node ratio metrics. These parameters provide a more accurate representation of metastatic burden and are now routinely incorporated into pathology reporting. Adoption across various malignancies enables more precise risk stratification and treatment planning. Integration of detailed nodal data improves prognostic discrimination by capturing both patterns of tumor spread and host immune interaction within the nodal basin.[20][21][22]
A clear example can be drawn from breast cancer staging within the American Joint Committee on Cancer framework. Pathologic staging distinguishes categories such as pN1 (1–3 axillary lymph nodes involved), pN2 (4–9 nodes contain metastasis), and pN3 (≥10 nodes affected, or infraclavicular, supraclavicular, or internal mammary nodes harbor metastasis). This gradation directly influences stage grouping, prognosis, and adjuvant treatment decisions, including indications for regional radiotherapy and systemic therapy.[23]
Media
(Click Image to Enlarge)
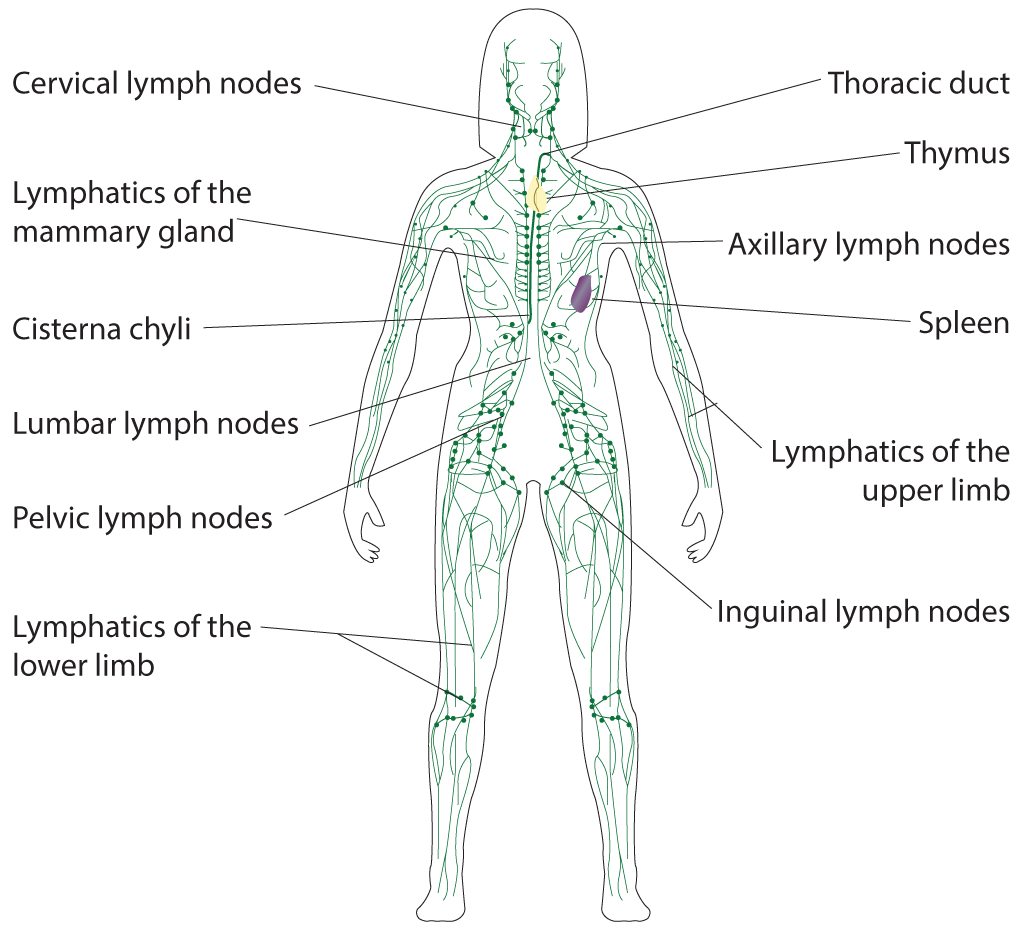
Lymphatic System. Illustrated anatomy includes the cervical lymph nodes, lymphatics of the mammary gland, cisterna chyli, lumbar lymph nodes, pelvic lymph nodes, lymphatics of the lower limb, thoracic duct, thymus, axillary lymph nodes, spleen, lymphatics of the upper limb, and inguinal lymph nodes.
Illustrated by B Parker
(Click Image to Enlarge)
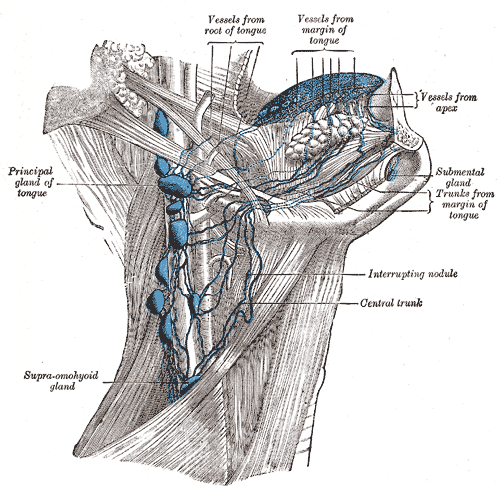
Lymphatics of the Tongue. The illustration displays the primary lymphatic trunks and interrupting nodules located within the neck and submental regions. Labels identify key structures such as the principal gland of the tongue and the supra-omohyoid gland.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
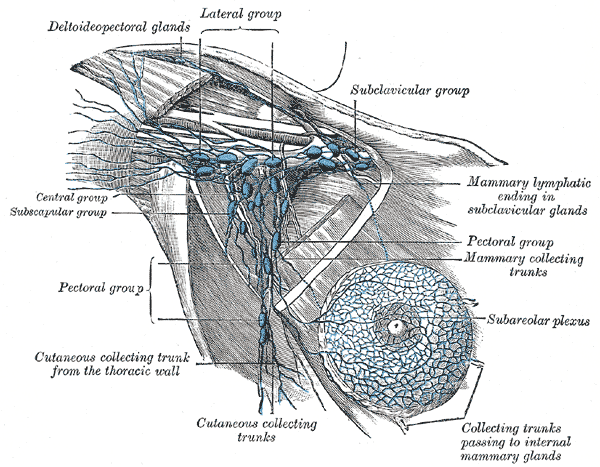
Anatomy of Axillary Lymph Nodes. Illustration of axillary lymph node anatomy, depicting the deltopectoral glands; lateral, subclavicular, central, subscapular, and pectoral groups; cutaneous and mammary collecting trunks; subareolar plexus; and mammary lymphatic ending in the subclavicular glands.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
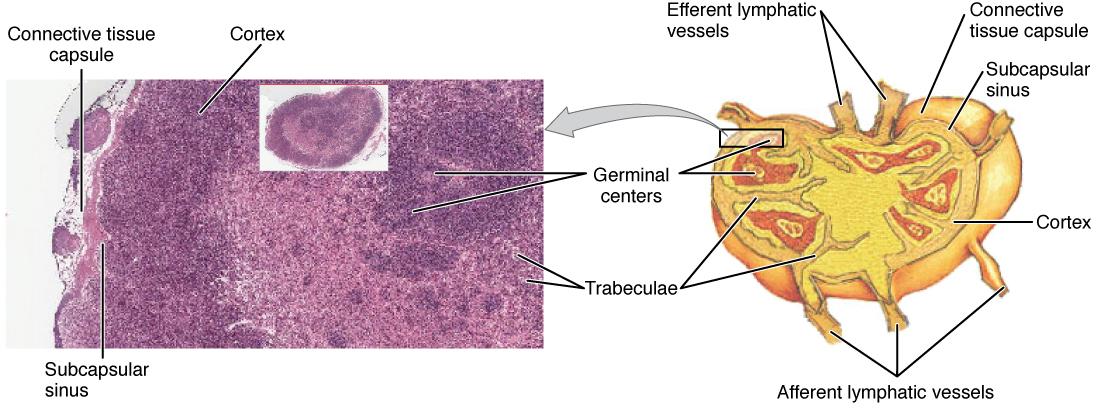
Structure and Histology of a Lymph Node. Illustration of lymph node organization showing capsule, cortex, paracortex, medulla, and associated lymphatic and vascular channels.
OpenStax College, Public Domain, via Wikimedia Commons
{kind=link}
References
Swartz MA. The physiology of the lymphatic system. Advanced drug delivery reviews. 2001 Aug 23:50(1-2):3-20 [PubMed PMID: 11489331]
Level 3 (low-level) evidenceWillard-Mack CL. Normal structure, function, and histology of lymph nodes. Toxicologic pathology. 2006:34(5):409-24 [PubMed PMID: 17067937]
Level 3 (low-level) evidenceMarkgraf R, von Gaudecker B, Müller-Hermelink HK. The development of the human lymph node. Cell and tissue research. 1982:225(2):387-413 [PubMed PMID: 6980711]
Cupedo T. Human lymph node development: An inflammatory interaction. Immunology letters. 2011 Jul:138(1):4-6. doi: 10.1016/j.imlet.2011.02.008. Epub 2011 Feb 17 [PubMed PMID: 21333686]
Level 3 (low-level) evidenceHsu MC, Itkin M. Lymphatic Anatomy. Techniques in vascular and interventional radiology. 2016 Dec:19(4):247-254. doi: 10.1053/j.tvir.2016.10.003. Epub 2016 Oct 8 [PubMed PMID: 27993319]
Pinto PS, Sirlin CB, Andrade-Barreto OA, Brown MA, Mindelzun RE, Mattrey RF. Cisterna chyli at routine abdominal MR imaging: a normal anatomic structure in the retrocrural space. Radiographics : a review publication of the Radiological Society of North America, Inc. 2004 May-Jun:24(3):809-17 [PubMed PMID: 15143230]
Lengelé B, Nyssen-Behets C, Scalliet P. Anatomical bases for the radiological delineation of lymph node areas. Upper limbs, chest and abdomen. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology. 2007 Sep:84(3):335-47 [PubMed PMID: 17719668]
BERG JW. The significance of axillary node levels in the study of breast carcinoma. Cancer. 1955 Jul-Aug:8(4):776-8 [PubMed PMID: 13240660]
Zhou Y, Hou J, Meng N, Daniel S, Chen J, Xu L. Case Report: Intercostal Lymph Node Metastasis: A Case Report and Review of the Literature. Frontiers in oncology. 2021:11():638948. doi: 10.3389/fonc.2021.638948. Epub 2021 Mar 4 [PubMed PMID: 33747962]
Level 3 (low-level) evidenceCirocchi R, Amabile MI, De Luca A, Frusone F, Tripodi D, Gentile P, Tabola R, Pironi D, Forte F, Monti M, D'Andrea V, Sorrenti S. New classifications of axillary lymph nodes and their anatomical-clinical correlations in breast surgery. World journal of surgical oncology. 2021 Mar 29:19(1):93. doi: 10.1186/s12957-021-02209-2. Epub 2021 Mar 29 [PubMed PMID: 33781279]
Grégoire V, Ang K, Budach W, Grau C, Hamoir M, Langendijk JA, Lee A, Le QT, Maingon P, Nutting C, O'Sullivan B, Porceddu SV, Lengele B. Delineation of the neck node levels for head and neck tumors: a 2013 update. DAHANCA, EORTC, HKNPCSG, NCIC CTG, NCRI, RTOG, TROG consensus guidelines. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology. 2014 Jan:110(1):172-81. doi: 10.1016/j.radonc.2013.10.010. Epub 2013 Oct 31 [PubMed PMID: 24183870]
Level 3 (low-level) evidenceLengelé B, Hamoir M, Scalliet P, Grégoire V. Anatomical bases for the radiological delineation of lymph node areas. Major collecting trunks, head and neck. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology. 2007 Oct:85(1):146-55 [PubMed PMID: 17383038]
Level 3 (low-level) evidenceLicastro E, Pignataro G, Iliff JJ, Xiang Y, Lo EH, Hayakawa K, Esposito E. Glymphatic and lymphatic communication with systemic responses during physiological and pathological conditions in the central nervous system. Communications biology. 2024 Feb 24:7(1):229. doi: 10.1038/s42003-024-05911-5. Epub 2024 Feb 24 [PubMed PMID: 38402351]
Hocke M, Ignee A, Dietrich C. Role of contrast-enhanced endoscopic ultrasound in lymph nodes. Endoscopic ultrasound. 2017 Jan-Feb:6(1):4-11. doi: 10.4103/2303-9027.190929. Epub [PubMed PMID: 28218194]
Eloubeidi MA, Chen VK, Eltoum IA, Jhala D, Chhieng DC, Jhala N, Vickers SM, Wilcox CM. Endoscopic ultrasound-guided fine needle aspiration biopsy of patients with suspected pancreatic cancer: diagnostic accuracy and acute and 30-day complications. The American journal of gastroenterology. 2003 Dec:98(12):2663-8 [PubMed PMID: 14687813]
Popescu A, Săftoiu A. Can elastography replace fine needle aspiration? Endoscopic ultrasound. 2014 Apr:3(2):109-17. doi: 10.4103/2303-9027.123009. Epub [PubMed PMID: 24955340]
Moran I, Nguyen A, Khoo WH, Butt D, Bourne K, Young C, Hermes JR, Biro M, Gracie G, Ma CS, Munier CML, Luciani F, Zaunders J, Parker A, Kelleher AD, Tangye SG, Croucher PI, Brink R, Read MN, Phan TG. Memory B cells are reactivated in subcapsular proliferative foci of lymph nodes. Nature communications. 2018 Aug 22:9(1):3372. doi: 10.1038/s41467-018-05772-7. Epub 2018 Aug 22 [PubMed PMID: 30135429]
Dhenni R, Phan TG. The geography of memory B cell reactivation in vaccine-induced immunity and in autoimmune disease relapses. Immunological reviews. 2020 Jul:296(1):62-86. doi: 10.1111/imr.12862. Epub 2020 May 30 [PubMed PMID: 32472583]
Sukhbaatar A, Mishra R, Nakamura A, Mori S, Sugiura T, Kodama T. Lymphatic topology reveals a novel intranodal lympho-venous shunt. The Journal of pathology. 2026 Apr:268(4):477-492. doi: 10.1002/path.70032. Epub 2026 Feb 4 [PubMed PMID: 41635937]
Li MH, Hu YJ, Shan HM, Gao XL, Huang QY, Zhao WY, Zhang ST, Zhang Y, Chen SW, Song M. The role of lymph node level ratio in predicting prognosis and the benefits of postoperative radiotherapy in patients with pathological N1 stage head and neck squamous cell carcinoma. Oral oncology. 2025 Feb:161():107193. doi: 10.1016/j.oraloncology.2025.107193. Epub 2025 Jan 18 [PubMed PMID: 39827591]
Akkus E, Kayaalp M, Karaoğlan BB, Akyol C, Utkan G. Lymph Node Ratio (LNR) Discriminates Prognostication in pN1a-b and pN2 Stage-III Colon Cancer. Journal of Cancer. 2025:16(4):1032-1039. doi: 10.7150/jca.104336. Epub 2025 Jan 1 [PubMed PMID: 39895795]
Wang J, Liu F, Ma W, Hu H, Li F. Metastatic lymph node ratio as an important prognostic factor in advanced gallbladder carcinoma with at least 6 lymph nodes retrieved. Langenbeck's archives of surgery. 2023 Sep 28:408(1):382. doi: 10.1007/s00423-023-03119-5. Epub 2023 Sep 28 [PubMed PMID: 37770780]
Safavi A, Mohammadzadeh N, Kaviani A, Dadashi A, Dadashi A. Axillary staging in post-neoadjuvant chemotherapy breast cancer patients: prognostic analysis and validation of axillary nodal metrics and comparison of the pathological node staging versus the lymph node ratio systems in a 169-case series. BMC cancer. 2026 Jan 30:26(1):. doi: 10.1186/s12885-026-15564-8. Epub 2026 Jan 30 [PubMed PMID: 41612229]
Level 1 (high-level) evidence