Introduction
Adjacent vertebrae articulate through zygapophyseal joints formed by the respective superior and inferior facets of the vertebral articular processes, as well as through interbody symphyses connecting the vertebral bodies. Zygapophyseal joints guide and limit the spine’s range of motion, whereas interbody symphyses facilitate mobility and provide the majority of the spine’s weight-bearing capacity. The inferior surface of a superior vertebral body articulates with the superior surface of the adjacent inferior vertebral body via intervertebral discs (IVDs).
The adult spine contains 23 IVDs: 6 cervical, 12 thoracic, and 5 lumbar. No disc exists between the atlas (C1) and the axis (C2), and the most caudal disc resides at the lumbosacral junction (L5-S1). Collectively, these discs constitute approximately 25% to 33% of the spinal length. IVDs facilitate spinal flexibility while preserving structural integrity, dissipate axial compressive loads, and prevent direct osseous contact between adjacent vertebral bodies. Each disc consists of 3 principal components: the inner nucleus pulposus, the outer annulus fibrosus, and cartilaginous endplates (CEPs) anchoring the disc to adjacent vertebrae (see Image. Intervertebral Disc Anatomy).
The nucleus pulposus is a gelatinous core eccentrically positioned slightly posterior to the geometric center of the IVD. This structure constitutes a critical component of spinal biomechanics by resisting compressive forces and facilitating segmental flexibility. Water comprises 66% to 86% of the nucleus pulposus, with the remainder composed primarily of type II collagen, accompanied by smaller amounts of type VI, IX, and XI collagen, and proteoglycans. The types of proteoglycans present include the larger aggrecan and versican, which bind to hyaluronic acid, as well as several small leucine-rich proteoglycans. Aggrecan is primarily responsible for water retention within the nucleus pulposus. Cellular density within this structure is low. Sparse cells produce extracellular matrix (ECM) products and maintain the structural integrity of the nucleus pulposus.
The annulus fibrosus is a ring-shaped disc of fibrous connective tissue encircling the nucleus pulposus. This structure exhibits a highly organized architecture, consisting of 15 to 25 stacked sheets, or lamellae, composed predominantly of collagen, with interspersed proteoglycans, glycoproteins, elastic fibers, and connective tissue cells responsible for secreting these ECM products.
Each lamella contains collagen fibers oriented uniformly within a plane that differs in alignment from the adjacent lamella by approximately 60°. This arrangement results in the parallel orientation of alternate lamellae. The resulting radial-ply formation confers exceptional tensile strength compared to an entirely longitudinal arrangement and has inspired analogous designs in engineered materials, such as car tires.
Lamellae are interconnected through translamellar bridges. The density of translamellar bridges per unit area is optimized to balance mechanical strength and flexibility. A higher number of bridges enhances resistance to compressive forces but reduces flexibility, whereas fewer bridges increase flexibility at the expense of strength.
The annulus fibrosus contains an inner and an outer portion, differing primarily in collagen composition. Both regions are composed predominantly of collagen, but the outer annulus consists mostly of type I collagen, whereas the inner annulus contains predominantly type II collagen. Proteoglycan content is greater in the inner annulus than in the outer. The ratio of type I to type II collagen transitions gradually with increasing distance from the nucleus pulposus—type II collagen decreases while type I collagen increases. A further distinction between the 2 segments lies in the morphology of the connective tissue cells responsible for secreting ECM. Cells within the inner annulus are round and chondrocyte-like, whereas those of the outer annulus exhibit a more oblong, fibroblast-like appearance.[1]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The IVD functions as a heterogeneous composite structure that enables spinal flexibility while transmitting substantial compressive, tensile, and shear loads. Biomechanically, the disc behaves as a viscoelastic solid, exhibiting time-dependent responses.[2] Mechanical competence depends on the synergistic interaction of 3 distinct substructures: the hydrated nucleus pulposus, the laminar annulus fibrosus, and the CEPs.
The nucleus pulposus serves as the primary load-distributing component of the disc. This structure's ECM is rich in proteoglycans, particularly aggrecan, which contain highly anionic glycosaminoglycan side chains. The negative charge of these chains generates a high fixed charge density, drawing water into the tissue via osmotic pressure to counterbalance external compressive stress.[3] In a healthy disc, the nucleus pulposus functions hydrostatically. When axial load is applied, the high water content (approximately 70%–80%) allows uniform pressurization, converting vertical compressive force into radially directed outward stress.
The annulus fibrosus confines the pressurized nucleus pulposus and maintains the structural integrity of the IVD. The annulus fibrosus is organized into 15 to 25 concentric lamellae reinforced by type I collagen fibers. These fibers are oriented at alternating angles (approximately 30° to 60° relative to the spinal axis) in successive layers, forming an angle-ply laminate structure.[4] This architecture converts radial stress generated by the nucleus pulposus into circumferential tensile stress, a mechanism termed "hoop stress."[5] Alternating fiber orientation provides resistance against multidirectional loads, with specific fiber populations recruiting tension during spinal flexion, extension, and torsion.
The CEPs serve dual roles as mechanical barriers and primary gateways for nutrient transport. Positioned at the cranial and caudal interfaces of the vertebral bodies, the CEPs prevent the pressurized nucleus pulposus from herniating into trabecular bone. The CEPs function as semipermeable membranes that facilitate the diffusion of glucose and oxygen from vertebral capillary beds into the avascular disc center. Calcification or sclerosis of the CEPs impedes solute transport, initiating a metabolic cascade that often precipitates disc degeneration.[6]
Functionally, the IVD exhibits significant diurnal variation due to fluid flux. Under prolonged axial loading, such as standing during the day, hydrostatic pressure within the disc exceeds osmotic swelling pressure, causing water to be expressed from disc tissue. This phenomenon, termed "creep," produces a measurable loss of disc height (10% to 20%) and increases tissue stiffness by evening.[7] The osmotic gradient is restored during unloading, such as recumbent sleep, and the disc reimbibes fluid to recover height and mechanical compliance.[8]
IVDs also protect vertebrae by absorbing shock and distributing forces throughout the spinal column. This function reduces load on individual vertebrae, potentially decreasing the risk of fractures and degenerative changes.
Embryology
The IVD arises from the precise interaction of 2 distinct embryonic lineages: the notochord, which forms the nucleus pulposus, and the sclerotome, paired condensed regions of mesenchymal cells in the paraxial mesoderm, which give rise to the annulus fibrosus and CEPs.[9]
Beginning in the 3rd week of gestation, the notochord functions as a signaling center, secreting Sonic Hedgehog (Shh) to induce sclerotomal cell survival and patterning.[10] The notochord is an embryonic midline structure common to all vertebrates that orients axial development. Vertebrae develop around the notochord from the sclerotome, whereas the IVDs form, in part, from the notochord itself. Interactions with sclerotomal condensations regulated by Pax1 and Pax9 result in regression of the notochord in regions destined to become vertebral bodies. The notochord expands in the transverse plane to form the nucleus pulposus in the remaining regions.
The annulus fibrosus develops from surrounding mesenchyme. Mesenchymal cells form ring-shaped, or annular, condensations around the notochord between the cartilage-like tissue of the primordial vertebral bodies. As the notochord dilates, mesenchymal cells between preformed vertebral bodies differentiate into the annulus fibrosus. The inner annulus is initially cartilaginous, with rapid accumulation of type II collagen, whereas the outer annulus begins as oriented fibroblastic lamellae that accumulate type I collagen. This initial lamellar arrangement establishes the basis for subsequent collagen orientation during later development.
During differentiation of the sclerotomal mesenchyme into the annulus fibrosus, constituent fibroblasts and chondrocyte-like cells synthesize proteoglycans and glycosaminoglycans. The inner annulus, being more cartilaginous, produces greater quantities of proteoglycans, whereas the outer annulus produces a predominantly collagenous matrix.[11]
Blood Supply and Lymphatics
The IVD constitutes the largest avascular structure in the human body. Metabolic homeostasis depends entirely on passive diffusion of glucose and oxygen from capillary beds in the vertebral CEPs and the outer annulus fibrosus. Nutrients must traverse considerable diffusion distances, resulting in the nucleus pulposus center experiencing the lowest oxygen and glucose concentrations and the highest lactic acid levels.[12]
Historically classified as alymphatic, spatial transcriptomic analyses in 2025 confirm the presence of functional lymphatic vessels in the healthy outer annulus fibrosus.[13] These vessels maintain fluid homeostasis and facilitate immune surveillance. In degenerative states, lymphatic vessel density decreases, whereas pathologic microvascular ingrowth increases. This imbalance impairs clearance of inflammatory catabolites and accelerates the degenerative cascade.
Nerves
The IVD receives innervation from multiple sources. Posterior aspects of the discs and the posterior longitudinal ligament (PLL) are supplied by sinuvertebral nerves, recurrent meningeal branches of spinal nerves that reenter the intervertebral foramina.[14] Each sinuvertebral nerve contains somatic fibers from ventral rami and autonomic fibers from grey rami communicantes, forming mixed polysegmental networks.[15] Posterolateral disc surfaces receive branches from adjacent ventral primary rami and grey rami communicantes, whereas lateral surfaces receive additional branches from grey rami communicantes.
Healthy IVDs exhibit innervation restricted to the outer and middle 1/3 of the annulus fibrosus, consisting mainly of small-diameter nociceptive sensory fibers and postganglionic sympathetic fibers with vasomotor function.[16] In degenerated or painful discs, nerve ingrowth extends into the inner annulus fibrosus and nucleus pulposus. Substance P–expressing nerve fibers, indicative of nociceptive function, are identified deep within diseased discs at pain-generating levels in 57% of samples, compared to 25% at nonpain levels.[17]
Distinct from annular innervation, the basivertebral nerve (BVN) enters the vertebral body posteriorly through the basivertebral foramen to innervate the superior and inferior vertebral endplates. Sensitization of the BVN correlates with endplate damage, known as Modic changes, and constitutes a specific etiology of vertebrogenic low back pain.[18]
Muscles
No muscles insert into the IVD itself. Consequently, disc stress reflects the summation of body weight transmission and muscle-generated forces, as contraction amplifies axial compression. Dynamic changes in posture and multiplanar loading alter intradiscal pressure and intersegmental load sharing, explaining fluctuations in symptoms during physical activity in disc disease, with pressure tracking external moment.[19]
Segmental stabilizers, such as the multifidus, a deep paraspinal muscle controlling segmental lumbar motion, modulate intersegmental shear and compressive distribution, influencing annular strain during movement. Stability provided by these muscles reduces micromotion. Modeling studies demonstrate that exclusion of multifidus activity increases estimated lumbar compressive loading during flexion tasks, supporting its role as a fine-tuner of lumbar biomechanics relevant to disc loading, with loss of stabilization shifting load to passive tissues.[20]
Nutrient transport and mechanobiology are inseparable from muscle function because cyclical loading alters disc fluid exchange and matrix maintenance demands. Convective transport occurs as a result of this motion.[21]
IVD degeneration strongly correlates with morphofunctional changes in adjacent paraspinal muscles. Fatty infiltration of the multifidus demonstrates a positive correlation with disc degeneration severity as assessed by Pfirrmann grading.[22] This relationship appears bidirectional—disc herniation induces rapid multifidus atrophy through denervation and reflex inhibition secondary to compressed nerve roots, whereas paraspinal muscle degeneration compromises spinal stability and may accelerate disc pathology.
Physiologic Variants
Lumbosacral transitional vertebrae are congenital anomalies of the lumbosacral junction, with a prevalence of 35% in the general population.[23] This variant involves either sacralization of the L5 vertebra, in which the L5 body fuses to the sacrum, or lumbarization of the S1 segment, in which the S1 body separates from the sacrum. The Castellvi classification categorizes these variants based on the morphology of the dysplastic transverse process, an enlarged bony projection.[24] Type I exhibits a dysplastic transverse process greater than 19 mm without articulation. Type II demonstrates a pseudoarticulation, or false joint, between the transverse process and the sacral ala. Type III involves complete osseous fusion. Type IV represents a mixed pattern, with Type II on one side and Type III on the contralateral side.
The presence of lumbosacral transitional vertebrae is clinically significant because these deviations alter spinal biomechanics. The disc at the transitional level is typically hypoplastic and protected from motion, which prevents degeneration.[25] However, the rigid lever arm created by the transitional vertebra transfers increased torque and shear stress to the suprajacent mobile segment, the level immediately above. This mechanical alteration results in accelerated degeneration and a higher incidence of disc herniation at the level cranial to the transitional vertebra. Accurate enumeration of vertebral levels using whole-spine imaging is critical to prevent wrong-level surgery.
A limbus vertebra appears as a triangular corticated osseous fragment, most commonly at the anterosuperior margin of midlumbar vertebral bodies.[26] This variant arises from intrabody herniation of nucleus pulposus material beneath the ring apophysis, or growth plate rim, prior to skeletal maturity. Herniated disc material prevents fusion of the apophyseal ossification center with the vertebral body. Distinction from an acute teardrop fracture is essential. The limbus fragment displays sclerotic margins, and the adjacent vertebral defect possesses a matching corticated rim, indicative of a chronic developmental process. Posterior limbus variants can displace the PLL and cause symptomatic central canal or foraminal stenosis, although most are incidental findings.[27]
Schmorl nodes represent vertical herniations of the nucleus pulposus through the CEP into the vertebral body spongiosa. These nodes are highly prevalent, affecting up to 75% of the population, and appear radiographically as radiolucent defects with sclerotic margins.[28][29] Pathogenesis involves a developmental weakness of the endplate or failure of regression of notochordal vascular channels. The majority are asymptomatic. However, acute Schmorl nodes can present with localized inflammation and bone marrow edema on magnetic resonance imaging, mimicking infection or malignancy.
Congenital block vertebrae result from failure of segmentation during embryogenesis, producing fusion of adjacent vertebral bodies. The IVD at the fused level is rudimentary or absent.[30] This fusion alters spinal kinematics, with the primary clinical consequence being adjacent segment disease.
Surgical Considerations
Surgical decision-making for disc herniation requires clinicoradiographic concordance, in which symptoms correspond to the level and laterality of pathology identified on imaging. This principle is critical, as degenerative disc changes are prevalent in asymptomatic adults, and imaging abnormalities alone do not constitute surgical indications.[31] Standardized morphological terminology—bulge, protrusion, extrusion, sequestration—facilitates precise communication between radiologists and surgeons regarding herniation configuration and containment status.[32]
Indications for surgery include failure of adequate conservative management, cauda equina syndrome, and progressive motor deficit. The anatomical location of the herniated fragment and the neural structure compressed determine the surgical approach. Posterolateral lumbar herniations impinging on the traversing nerve root are typically accessible via standard interlaminar discectomy. Far lateral herniations, defined as extraforaminal fragments extending lateral to the neural foramen, compress the exiting nerve root and dorsal root ganglion at that level. These lesions frequently require a paramedian muscle-splitting approach, as the standard midline interlaminar exposure provides inadequate visualization of the extraforaminal compartment (see Image. Lumbar Disc Herniation Zones and Surgical Approaches).[33]
Clinical Significance
Standardized terminology is essential for accurate diagnosis. The North American Spine Society defines IVD herniation as the displacement of disc material involving less than 25% of the disc circumference. Herniations are subclassified by geometry. A protrusion has a base wider than its dome. An extrusion has a dome wider than its base. A sequestration consists of a free fragment that has lost continuity with the parent IVD.
Radicular pain results from a synergistic mechanism of mechanical compression and chemical irritation. The nucleus pulposus releases inflammatory cytokines that sensitize nerve roots and lower firing thresholds.[34] This chemical radiculitis explains why severe pain may occur despite minor radiographic compression. Cauda equina syndrome constitutes a surgical emergency caused by massive compression of lumbosacral nerve roots, most often from a sizeable IVD herniation (see Image. Clinical and Radiological Presentation of Cauda Equina Syndrome). Red flags include saddle anesthesia and bilateral sciatica.
IVD degeneration, defined as structural and biochemical deterioration with age, begins with proteoglycan loss and dehydration of the nucleus pulposus. This process reduces hydrostatic behavior and shifts mechanical stress to the annulus fibrosus.[35] Degenerative changes are graded using the Pfirrmann Classification on T2-weighted magnetic resonance imaging. Grade I represents a hyperintense and homogeneous nucleus with normal disc height, whereas Grade V indicates a collapsed and hypointense, or “black,” IVD.[36]
Vertebral endplate signal abnormalities, known as Modic changes, correlate with histopathology. Type I Modic changes, representing edema, appear hypointense on T1-weighted images and hyperintense on T2, correlating with active inflammation and low back pain. Type II Modic changes, representing fatty replacement, appear hyperintense on T1 and isointense to hyperintense on T2.[37]
Extensive research has focused on methods to replace or regenerate IVDs. Approaches include implantation of synthetic disc implants and stem cell or gene therapy.
Other Issues
No IVD exists between C1 and C2. This absence represents a unique feature within the spine.
Two major ligaments provide support to the IVDs. The anterior longitudinal ligament is a broad band covering the anterolateral surface of the spine from the foramen magnum to the sacrum. This ligament prevents hyperextension and limits anterolateral IVD herniation. The PLL covers the posterior aspect of the vertebral bodies within the vertebral canal. The PLL primarily prevents posterior IVD herniation and contributes to the predominance of posterolateral herniations.
Media
(Click Image to Enlarge)
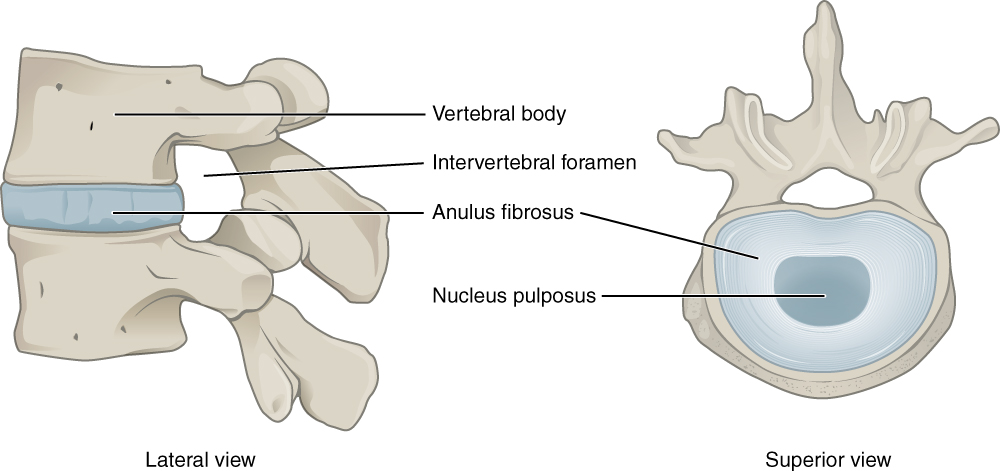
Intervertebral Disc Anatomy. Lateral (left) and superior (right) views depict the vertebral body, intervertebral foramen, annulus fibrosus, and nucleus pulposus of a lumbar vertebra.
Illustration from Anatomy & Physiology, Connexions Web site. http://cnx.org/content/col11496/1.6/, Jun 19, 2013. This file is licensed under the Creative Commons Attribution 3.0 Unported license.
(Click Image to Enlarge)
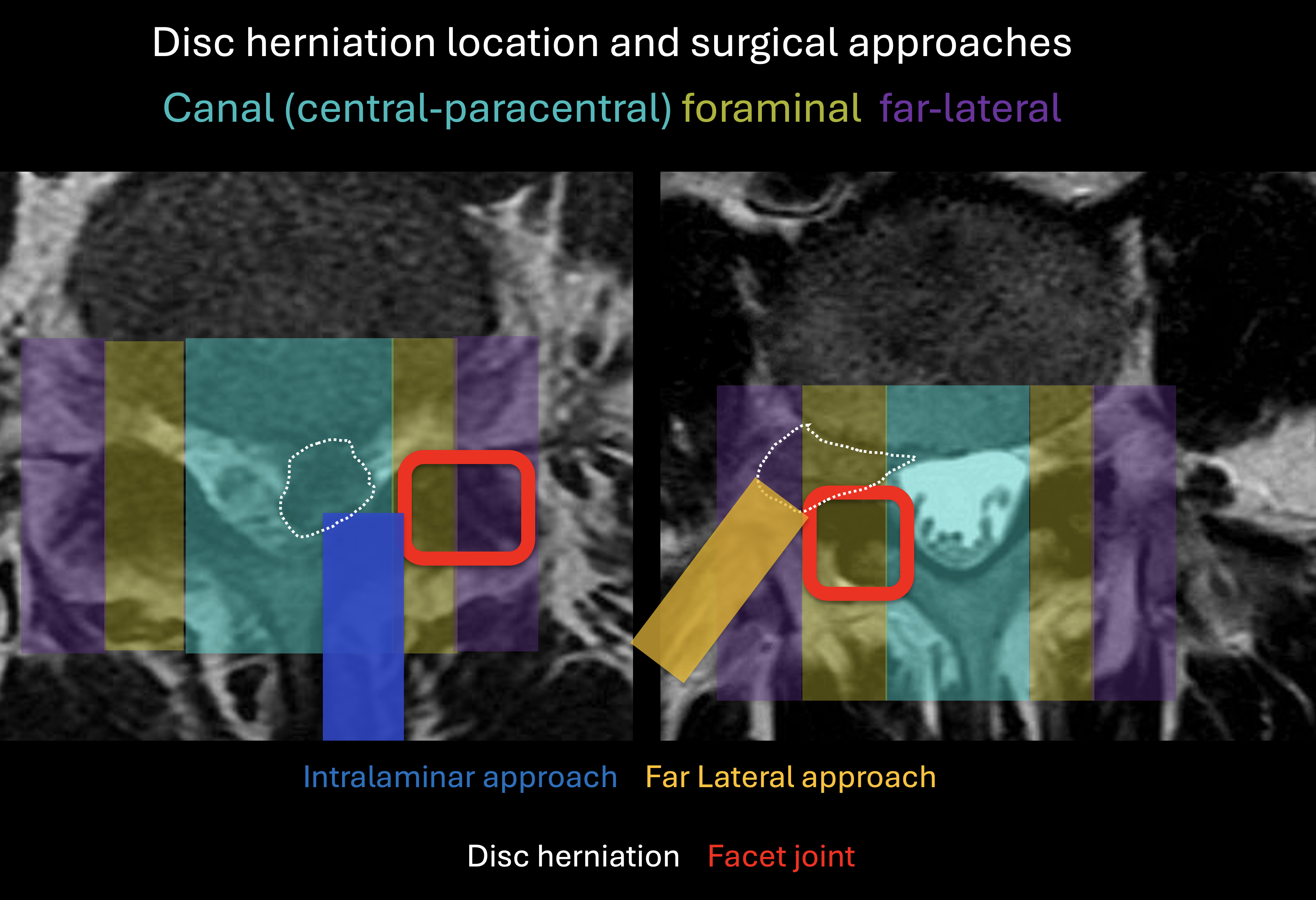
Lumbar Disc Herniation Zones and Surgical Approaches. The axial lumbar spine is divided into central–paracentral (cyan), foraminal (yellow), and far-lateral (purple) zones based on their relationship to the pedicle and facet joint (red). Central and paracentral herniations, which typically compress the traversing nerve root, are accessed via an intralaminar approach (blue). Foraminal and far-lateral herniations, which affect the exiting nerve root, are approached through a far-lateral intermuscular corridor (orange) to minimise facet joint violation.
Contributed by Konstantinos Margetis MD
(Click Image to Enlarge)
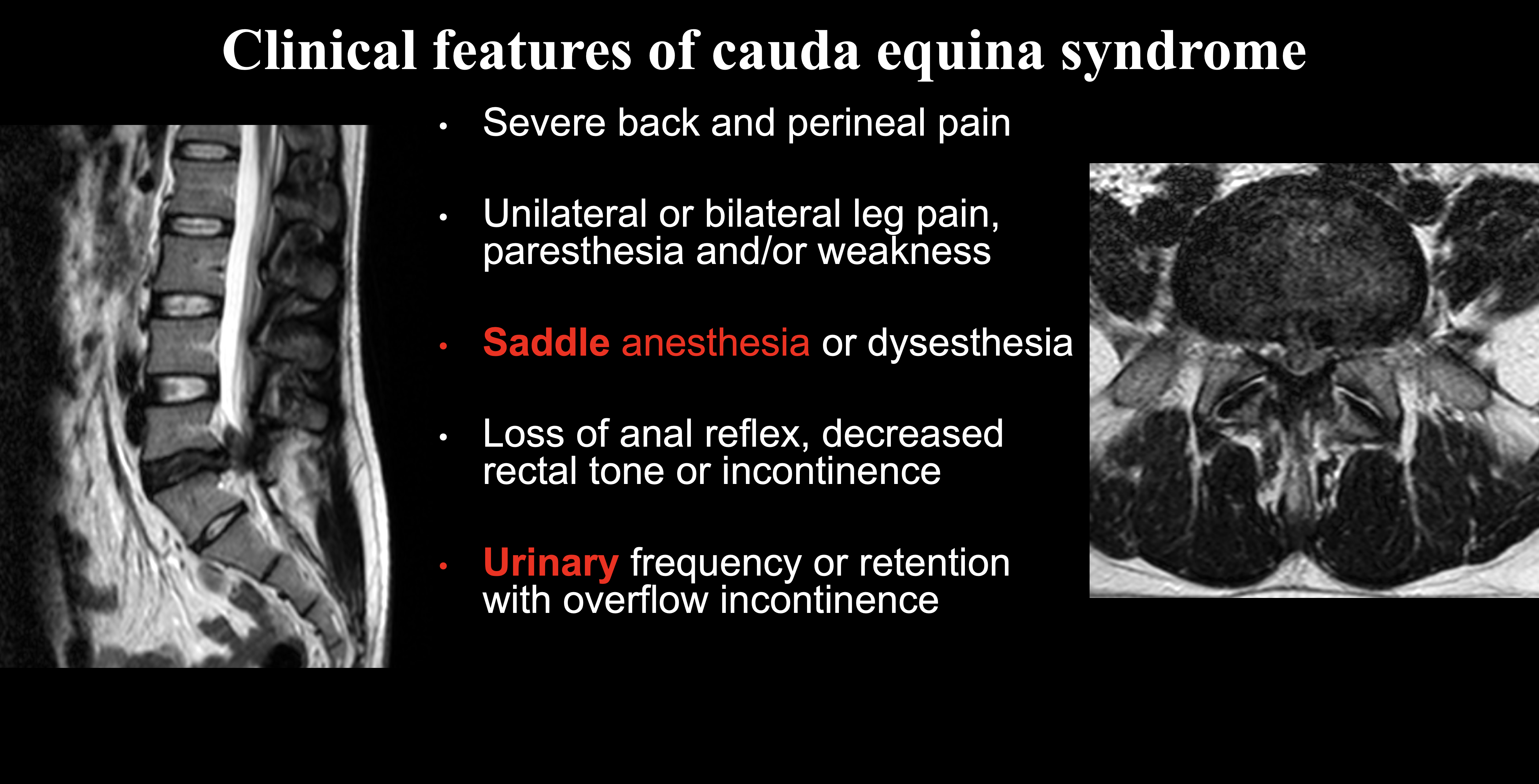
Clinical and Radiological Presentation of Cauda Equina Syndrome. The figure illustrates the cardinal features of cauda equina syndrome (CES), a neurosurgical emergency typically resulting from massive central disc herniation. Sagittal T2-weighted magnetic resonance imaging (MRI) demonstrates a large extruded disc fragment compromising the spinal canal (left). Axial T2-weighted MRI shows severe canal stenosis and compression of the cauda equina nerve roots (right). The listed clinical findings (text) emphasize "red flag" symptoms for CES, specifically saddle anesthesia and urinary retention/overflow incontinence, which are highlighted in red.
Contributed by Konstantinos Margetis MD
References
van Uden S, Silva-Correia J, Oliveira JM, Reis RL. Current strategies for treatment of intervertebral disc degeneration: substitution and regeneration possibilities. Biomaterials research. 2017:21():22. doi: 10.1186/s40824-017-0106-6. Epub 2017 Oct 23 [PubMed PMID: 29085662]
Iatridis JC, Weidenbaum M, Setton LA, Mow VC. Is the nucleus pulposus a solid or a fluid? Mechanical behaviors of the nucleus pulposus of the human intervertebral disc. Spine. 1996 May 15:21(10):1174-84 [PubMed PMID: 8727192]
Urban JP, McMullin JF. Swelling pressure of the lumbar intervertebral discs: influence of age, spinal level, composition, and degeneration. Spine. 1988 Feb:13(2):179-87 [PubMed PMID: 3406838]
Marchand F, Ahmed AM. Investigation of the laminate structure of lumbar disc anulus fibrosus. Spine. 1990 May:15(5):402-10 [PubMed PMID: 2363068]
Adams MA, Dolan P. Recent advances in lumbar spinal mechanics and their clinical significance. Clinical biomechanics (Bristol, Avon). 1995 Jan:10(1):3-19 [PubMed PMID: 11415526]
Level 3 (low-level) evidenceRoberts S, Urban JP, Evans H, Eisenstein SM. Transport properties of the human cartilage endplate in relation to its composition and calcification. Spine. 1996 Feb 15:21(4):415-20 [PubMed PMID: 8658243]
Broberg KB. Slow deformation of intervertebral discs. Journal of biomechanics. 1993 Apr-May:26(4-5):501-12 [PubMed PMID: 8478352]
Keller TS, Nathan M. Height change caused by creep in intervertebral discs: a sagittal plane model. Journal of spinal disorders. 1999 Aug:12(4):313-24 [PubMed PMID: 10451048]
Sivakamasundari V, Lufkin T. Bridging the Gap: Understanding Embryonic Intervertebral Disc Development. Cell & developmental biology. 2012 May:1(2):. pii: 103. Epub [PubMed PMID: 23106046]
Level 3 (low-level) evidenceDahia CL, Mahoney E, Wylie C. Shh signaling from the nucleus pulposus is required for the postnatal growth and differentiation of the mouse intervertebral disc. PloS one. 2012:7(4):e35944. doi: 10.1371/journal.pone.0035944. Epub 2012 Apr 27 [PubMed PMID: 22558278]
Williams S, Alkhatib B, Serra R. Development of the axial skeleton and intervertebral disc. Current topics in developmental biology. 2019:133():49-90. doi: 10.1016/bs.ctdb.2018.11.018. Epub 2019 Jan 3 [PubMed PMID: 30902259]
Urban JP, Smith S, Fairbank JC. Nutrition of the intervertebral disc. Spine. 2004 Dec 1:29(23):2700-9 [PubMed PMID: 15564919]
Zou F, Lu X, Wang S, Lin Z, Xu G, Li D, Gong Z, Wu J, Wang H, Wu J, Guan Y, Yang S, Zhang Y, Sun C, Song J, Wang H, Zhu W, Xia X, Lyu F, Jiang J, Liang K, Chen L, Ma X. Revealing the presence of lymphatic vessels within intervertebral discs: Novel insights into disc degeneration. Innovation (Cambridge (Mass.)). 2025 Jun 2:6(6):100865. doi: 10.1016/j.xinn.2025.100865. Epub 2025 Mar 3 [PubMed PMID: 40528887]
Bogduk N,Tynan W,Wilson AS, The nerve supply to the human lumbar intervertebral discs. Journal of anatomy. 1981 Jan; [PubMed PMID: 7275791]
Bogduk N. The innervation of the lumbar spine. Spine. 1983 Apr:8(3):286-93 [PubMed PMID: 6226119]
García-Cosamalón J, del Valle ME, Calavia MG, García-Suárez O, López-Muñiz A, Otero J, Vega JA. Intervertebral disc, sensory nerves and neurotrophins: who is who in discogenic pain? Journal of anatomy. 2010 Jul:217(1):1-15. doi: 10.1111/j.1469-7580.2010.01227.x. Epub 2010 Apr 26 [PubMed PMID: 20456524]
Freemont AJ, Peacock TE, Goupille P, Hoyland JA, O'Brien J, Jayson MI. Nerve ingrowth into diseased intervertebral disc in chronic back pain. Lancet (London, England). 1997 Jul 19:350(9072):178-81 [PubMed PMID: 9250186]
Schnapp W, Martiatu K, Delcroix GJ. Basivertebral Nerve Ablation for the Treatment of Chronic Low Back Pain: A Scoping Review of the Literature. Pain physician. 2022 Jul:25(4):E551-E562 [PubMed PMID: 35793179]
Level 2 (mid-level) evidenceLiebsch C, Wilke HJ. The effect of multiplanar loading on the intradiscal pressure of the whole human spine: systematic review and meta-analysis. European cells & materials. 2021 Mar 21:41():388-400. doi: 10.22203/eCM.v041a25. Epub 2021 Mar 21 [PubMed PMID: 33745125]
Level 1 (high-level) evidenceWang K, Deng Z, Chen X, Shao J, Qiu L, Jiang C, Niu W. The Role of Multifidus in the Biomechanics of Lumbar Spine: A Musculoskeletal Modeling Study. Bioengineering (Basel, Switzerland). 2023 Jan 4:10(1):. doi: 10.3390/bioengineering10010067. Epub 2023 Jan 4 [PubMed PMID: 36671639]
Level 2 (mid-level) evidenceDe Geer CM. Intervertebral Disk Nutrients and Transport Mechanisms in Relation to Disk Degeneration: A Narrative Literature Review. Journal of chiropractic medicine. 2018 Jun:17(2):97-105. doi: 10.1016/j.jcm.2017.11.006. Epub 2018 Jun 14 [PubMed PMID: 30166966]
Shi L, Yan B, Jiao Y, Chen Z, Zheng Y, Lin Y, Cao P. Correlation between the fatty infiltration of paraspinal muscles and disc degeneration and the underlying mechanism. BMC musculoskeletal disorders. 2022 May 30:23(1):509. doi: 10.1186/s12891-022-05466-8. Epub 2022 May 30 [PubMed PMID: 35637476]
Apazidis A, Ricart PA, Diefenbach CM, Spivak JM. The prevalence of transitional vertebrae in the lumbar spine. The spine journal : official journal of the North American Spine Society. 2011 Sep:11(9):858-62. doi: 10.1016/j.spinee.2011.08.005. Epub [PubMed PMID: 21951610]
Castellvi AE, Goldstein LA, Chan DP. Lumbosacral transitional vertebrae and their relationship with lumbar extradural defects. Spine. 1984 Jul-Aug:9(5):493-5 [PubMed PMID: 6495013]
Konin GP, Walz DM. Lumbosacral transitional vertebrae: classification, imaging findings, and clinical relevance. AJNR. American journal of neuroradiology. 2010 Nov:31(10):1778-86. doi: 10.3174/ajnr.A2036. Epub 2010 Mar 4 [PubMed PMID: 20203111]
Ghelman B, Freiberger RH. The limbus vertebra: an anterior disc herniation demonstrated by discography. AJR. American journal of roentgenology. 1976 Nov:127(5):854-5 [PubMed PMID: 973676]
Huang PY, Yeh LR, Tzeng WS, Tsai MY, Shih TT, Pan HB, Chen CK. Imaging features of posterior limbus vertebrae. Clinical imaging. 2012 Nov-Dec:36(6):797-802. doi: 10.1016/j.clinimag.2012.01.031. Epub 2012 Jun 8 [PubMed PMID: 23154012]
Silberstein M, Opeskin K, Fahey V. Spinal Schmorl's nodes: sagittal sectional imaging and pathological examination. Australasian radiology. 1999 Feb:43(1):27-30 [PubMed PMID: 10901866]
Mattei TA, Rehman AA. Schmorl's nodes: current pathophysiological, diagnostic, and therapeutic paradigms. Neurosurgical review. 2014 Jan:37(1):39-46. doi: 10.1007/s10143-013-0488-4. Epub 2013 Aug 18 [PubMed PMID: 23955279]
Leivseth G, Frobin W, Brinckmann P. Congenital cervical block vertebrae are associated with caudally adjacent discs. Clinical biomechanics (Bristol, Avon). 2005 Aug:20(7):669-74 [PubMed PMID: 15964113]
Brinjikji W, Luetmer PH, Comstock B, Bresnahan BW, Chen LE, Deyo RA, Halabi S, Turner JA, Avins AL, James K, Wald JT, Kallmes DF, Jarvik JG. Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. AJNR. American journal of neuroradiology. 2015 Apr:36(4):811-6. doi: 10.3174/ajnr.A4173. Epub 2014 Nov 27 [PubMed PMID: 25430861]
Level 1 (high-level) evidenceFardon DF, Williams AL, Dohring EJ, Murtagh FR, Gabriel Rothman SL, Sze GK. Lumbar disc nomenclature: version 2.0: Recommendations of the combined task forces of the North American Spine Society, the American Society of Spine Radiology and the American Society of Neuroradiology. The spine journal : official journal of the North American Spine Society. 2014 Nov 1:14(11):2525-45. doi: 10.1016/j.spinee.2014.04.022. Epub 2014 Apr 24 [PubMed PMID: 24768732]
Berra LV, Di Rita A, Longhitano F, Mailland E, Reganati P, Frati A, Santoro A. Far lateral lumbar disc herniation part 1: Imaging, neurophysiology and clinical features. World journal of orthopedics. 2021 Dec 18:12(12):961-969. doi: 10.5312/wjo.v12.i12.961. Epub 2021 Dec 18 [PubMed PMID: 35036338]
Takahashi H, Suguro T, Okazima Y, Motegi M, Okada Y, Kakiuchi T. Inflammatory cytokines in the herniated disc of the lumbar spine. Spine. 1996 Jan 15:21(2):218-24 [PubMed PMID: 8720407]
Lyu FJ, Cui H, Pan H, Mc Cheung K, Cao X, Iatridis JC, Zheng Z. Painful intervertebral disc degeneration and inflammation: from laboratory evidence to clinical interventions. Bone research. 2021 Jan 29:9(1):7. doi: 10.1038/s41413-020-00125-x. Epub 2021 Jan 29 [PubMed PMID: 33514693]
Pfirrmann CW, Metzdorf A, Zanetti M, Hodler J, Boos N. Magnetic resonance classification of lumbar intervertebral disc degeneration. Spine. 2001 Sep 1:26(17):1873-8 [PubMed PMID: 11568697]
Modic MT, Steinberg PM, Ross JS, Masaryk TJ, Carter JR. Degenerative disk disease: assessment of changes in vertebral body marrow with MR imaging. Radiology. 1988 Jan:166(1 Pt 1):193-9 [PubMed PMID: 3336678]
Level 2 (mid-level) evidence