Introduction
Hepatic angiosarcoma is a rare, high-grade malignant neoplasm arising from the liver's vascular endothelium. Hepatic angiosarcoma is the most common primary malignant mesenchymal neoplasm of the liver in adults, accounting for approximately 2% of all primary hepatic malignant neoplasms.[1] The disease predominantly affects men in their sixth to seventh decade of life and carries an extremely poor prognosis, with median survival typically measured in months without treatment. Known risk factors include occupational exposure to vinyl chloride, thorotrast, and arsenic, though most cases are idiopathic. Patients often present with nonspecific symptoms, including abdominal pain, hepatomegaly, and constitutional symptoms, making early diagnosis challenging. Diagnostic evaluation relies on cross-sectional imaging with CT or MRI, which demonstrates characteristic, heterogeneous hepatic masses with progressive enhancement, though a definitive diagnosis requires histopathological confirmation. Treatment options are limited, with surgical resection or liver transplant offering the only potential for cure in highly selected patients, though most patients present with advanced, unresectable disease.[2][3][4]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Around 75% of tumors have no known etiology, but the most common known etiologic factors are exposure to vinyl chloride monomer and other industrial materials, iatrogenic exposure to colloidal thorium dioxide (Thorotrast), androgenic corticosteroid use, chronic arsenic ingestion, and exposure to radium. Results from studies have also shown an association between liver cancer and exposure to diethylstilbestrol, urethane, cyclophosphamide, and oral contraceptives. Hepatic angiosarcoma due to environmental exposure has a prolonged latency period of 10 to 40 years.
Vinyl chloride was formerly used to produce polyvinyl chloride. In 1949, it was recognized that the highly reactive epoxide chloroethylene oxide produced during the reaction caused hepatorenal damage. The latency period is about 20 years. Results from large database studies have shown that 12.8% of patients with liver angiosarcoma had a history of vinyl chloride exposure.[5] Cancer associated with vinyl chloride monomer exposure is associated with TP53 mutations.
Thorotrast was used as a radiocontrast material, but its use was stopped shortly thereafter following several reports of organ damage and fatalities. In the liver, the substance is taken up and stored by Kupffer cells, and after cellular destruction, it is stored in the periportal area. This results in periportal, periacinar, and Glisson capsule fibrosis. Kirsten rat sarcoma viral oncogene homolog (KRAS2) mutations have been found in cancer cells from individuals exposed to Thorotrast. Chronic arsenic intoxication initially results in hepatomegaly followed by the development of steatosis, cell necrosis, fibrosis, and cirrhosis.[2][6][7][8]
Epidemiology
Hepatic angiosarcoma accounts for 0.1% to 2% of all primary hepatic malignant neoplasms, but it is still considered the third most common primary hepatic malignant neoplasm. The condition usually occurs in older men, with a peak incidence in the sixth or seventh decade of life. Men are more frequently affected than women, with a ratio of 3:1 to 4:1. However, in childhood, incidence is higher in girls than in boys. Results from studies have shown an increase in the incidence of all angiosarcomas, including hepatic angiosarcoma, in the last 2 decades.[2][5][9][10][11]
Pathophysiology
Hepatic angiosarcoma is primarily composed of vascular or lymphatic endothelial cells and abundant vasculature. Spindle or pleomorphic cells line or grow into the lumina of preexisting vascular spaces, including sinusoids and terminal hepatic venules, causing hepatocyte atrophy and forming vascular channels. Hepatic angiosarcoma can sometimes form solid tumor masses. Hepatic angiosarcoma should be considered when a hepatic bleeding mass is encountered. Metastatic spread usually occurs to the lungs and hilar lymph nodes, but can also spread to the spleen and bones.[2][3][12]
Histopathology
Histologically, the malignant neoplasm is composed of spindle-shaped and polyhedral cells, exhibiting various vascular channel patterns. Solid areas that resemble fibrosarcoma and polynuclear giant cells may also be seen. Tumor invasion of the portal and hepatic vein branches is common. Areas of infarct, atrophy, and fibrosis are also commonly seen because parenchymal loss causes scarring and occlusion of preexisting vessels. Immunohistochemical markers, including CD31, CD34, ETS-related gene (ERG), Ulex europaeus agglutinin I, and factor VIII–related antigen, can aid diagnosis. Because of the highly vascular nature of the tumor, liver biopsy has a high risk of morbidity and mortality.[2][12][13][14][15]
History and Physical
Hepatic angiosarcoma usually presents with nonspecific symptoms, including right upper quadrant abdominal pain, weight loss, abdominal distention, jaundice, and fatigue.[2] The physical examination can reveal jaundice, ascites, and hepatomegaly.[14] However, most patients are asymptomatic early in the disease course, and the lesions are found incidentally on imaging. Hepatic angiosarcoma is often diagnosed at an advanced stage, with distant metastasis present in over 60% of patients at presentation. The most common sites of metastases are the lung and hilar lymph nodes, followed by the spleen and bones.[15]
Evaluation
Diagnosing hepatic angiosarcoma is challenging because of nonspecific symptoms. Most liver tumors are detected incidentally on abdominal imaging. Differentiating hepatic angiosarcoma from other hepatic tumors is difficult because of its hypervascularity. Ultrasonography may reveal multiple nodules or a solitary mass with variable echogenicity resulting from necrosis or hemorrhage. Computed tomography and MRI are commonly used for detection. On unenhanced CT, lesions typically appear hypodense, with occasional hyperdense areas due to hemorrhage. (see Image. Hepatic Angiosarcoma). MRI highlights the hemorrhagic, heterogeneous, and hypervascular features of these lesions. Multiphasic contrast-enhanced CT and MRI are the preferred imaging modalities for hepatic angiosarcoma because they best demonstrate tumor vascularity. During contrast administration, these tumors show progressive, heterogeneous enhancement in the delayed phase, with a centripetal or diffuse flash-fill pattern, without rapid contrast washout, which helps distinguish them from hepatocellular carcinoma or hypervascular metastases.[16]
Laboratory studies often reveal elevated alanine aminotransferase and aspartate aminotransferase levels, indicating hepatocellular injury and tumor replacement of normal liver tissue. Anemia and thrombocytopenia are also common due to the consumption of clotting factors. Tumor markers such as α-fetoprotein, carcinoembryonic antigen, carbohydrate antigen 19-9, and cancer antigen 125 are typically normal or only slightly elevated. Definitive diagnosis requires correlation of radiological findings with histological interpretation. Despite an accurate diagnosis, the tumor often progresses rapidly and is associated with a poor prognosis.[2][3][4][8][12][17]
Treatment / Management
Primary hepatic angiosarcoma has an aggressive clinical course with an extremely poor prognosis, with results from studies showing a 1-year survival rate of 12.8%.[5] Complete hepatic resection is the only potentially curative treatment. Results from studies have shown improved survival, particularly when the lesion is limited to a single lobe and distant metastases are absent. However, surgical procedures are associated with high rates of postoperative complications, mortality, and recurrence. Liver transplant is generally not recommended because of rapid disease progression and high recurrence rates, with posttransplant survival less than 7 months.[17][18]
Most cases are diagnosed at an advanced, unresectable stage, although results from some case reports have shown benefits from chemotherapy. Although no standardized regimen exists, agents such as paclitaxel, gemcitabine, docetaxel, doxorubicin, and cyclophosphamide have been used sparingly. Evidence suggests increased survival with chemotherapy, and adjuvant chemotherapy after resection may also provide benefit.[1][15]
Transarterial chemoembolization and other local therapies are used for unresectable liver-dominant disease and for controlling bleeding in cases of tumor rupture. Transarterial chemoembolization may be used alone or in combination with other modalities and may improve survival in select cases.[15][19] Because hepatic angiosarcoma is rare, most available data are limited to small case series and retrospective studies, and no established guidelines for optimal treatment exist. Treatment should be individualized and coordinated through an interdisciplinary team, and referral to a sarcoma specialty center is recommended by the American College of Gastroenterology.[1][18][16][20][21](B2)
Differential Diagnosis
Differential diagnoses of hepatic angiosarcoma include the following:
- Inflammatory disorders of the liver
- Benign vascular diseases of the liver
- Kaposi sarcoma
- Liver metastasis from angiosarcoma arising in other organs
- Epithelioid hemangioendothelioma
- Hepatocellular carcinoma
- Fibrosarcoma [2]
Staging
Clinical staging of angiosarcoma is based on the American Joint Committee on Cancer staging system for soft tissue sarcoma, which considers tumor size, depth, regional lymph node involvement, distant metastases, and histological grade. All hepatic angiosarcomas are considered deep tumors because they are located beneath the superficial fascia. Stage II and III hepatic angiosarcomas are rare, making outcomes more difficult to predict. Results from studies have shown that the majority of cases are stage I or IV.[21]
Prognosis
Hepatic angiosarcoma is a rapidly progressive malignant neoplasm, and most patients die within 6 months, with only 5% to 11% of patients surviving 5 years. Tumor rupture is a particularly poor prognostic event, often resulting in death within 1 month. Factors associated with poor prognosis include male sex, older age, and advanced stage at diagnosis. Surgical procedures and chemotherapy have been shown to increase survival from 1 month with no treatment to 6 months.[2][3][5][22][5][3]
Complications
Hepatic angiosarcoma is a rapidly fatal tumor, with mortality within 6 months from liver failure or hemorrhage. Tumor rupture may occur, resulting in hemoperitoneum, which is seen in 17% to 27% of cases. Once tumor rupture occurs, transarterial embolization is usually the first intervention performed to stabilize the patient and stop the bleeding. However, no definitive recommendation exists for treating acute bleeding from liver angiosarcoma because of the rarity of the tumor.[2][4][13] Other rare complications include Kasabach-Merritt syndrome, characterized by thrombocytopenia and hyperconsumption of coagulation factors within a vascular tumor, and disseminated intravascular coagulation.[15]
Deterrence and Patient Education
The diagnosis of hepatic angiosarcoma remains difficult during the early stages because of nonspecific symptoms. Prognosis is poor because of rapid progression, high recurrence rate, and resistance to traditional chemotherapy and radiotherapy. Surgical resection remains the most definitive curative therapy. However, no therapeutic guidelines have been established to date because of the rarity of this cancer. As previously mentioned, exposure to environmental and chemical substances remains the most common known etiology of the disease.[2][4]
Enhancing Healthcare Team Outcomes
Unfortunately, because of the small number of cases of this rare malignant neoplasm, therapeutic guidelines have not been definitively established. Diagnosing hepatic angiosarcoma remains a challenge because of the nonspecificity of presenting symptoms, such as weight loss and abdominal pain. Laboratory cancer markers are also nonspecific to the diagnosis, and diagnosing the tumor on radiological imaging is difficult. Biopsy of the lesion carries risks of bleeding because of the highly vascular nature of the tumor. Diagnosis and treatment of hepatic angiosarcoma should involve an interdisciplinary approach among an interprofessional team of primary care clinicians, hepatologists, radiologists, pathologists, oncologists, and palliative care clinicians. Surgical resection offers a chance for prolonged survival, but most patients present with unresectable or advanced disease. Systemic therapies, including chemotherapy, radiation, and immunotherapy, as well as transarterial therapies, may be considered for palliation, but evidence of efficacy is limited. Liver transplant is contraindicated because of high recurrence rates. Early goals-of-care discussions and involvement of palliative care are essential, given the rapid progression and poor outcomes. Oncology and hospice nurses play a key role in patient education, symptom treatment, and communication with the care team.
Media
(Click Image to Enlarge)
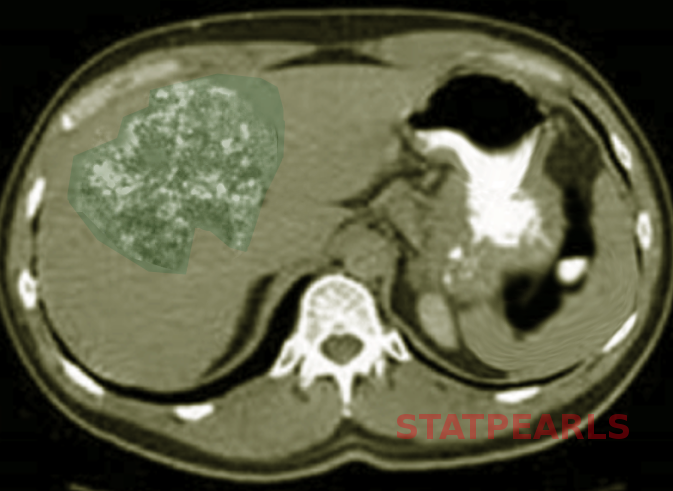
Hepatic Angiosarcoma. An axial computed tomography scan reveals a large, heterogeneous, hypoattenuating mass within the right hepatic lobe, which is consistent with a diagnosis of hepatic angiosarcoma.
Contributed by S Bhimji, MD
References
Frenette C, Mendiratta-Lala M, Salgia R, Wong RJ, Sauer BG, Pillai A. ACG Clinical Guideline: Focal Liver Lesions. The American journal of gastroenterology. 2024 Jul 1:119(7):1235-1271. doi: 10.14309/ajg.0000000000002857. Epub 2024 Jan 26 [PubMed PMID: 38958301]
Chaudhary P, Bhadana U, Singh RA, Ahuja A. Primary hepatic angiosarcoma. European journal of surgical oncology : the journal of the European Society of Surgical Oncology and the British Association of Surgical Oncology. 2015 Sep:41(9):1137-43. doi: 10.1016/j.ejso.2015.04.022. Epub 2015 May 14 [PubMed PMID: 26008857]
Yi LL, Zhang JX, Zhou SG, Wang J, Huang YQ, Li J, Yu X, Wang RN. CT and MRI studies of hepatic angiosarcoma. Clinical radiology. 2019 May:74(5):406.e1-406.e8. doi: 10.1016/j.crad.2018.12.013. Epub 2019 Jan 25 [PubMed PMID: 30686504]
Chien CY, Hwang CC, Yeh CN, Chen HY, Wu JT, Cheung CS, Lin CL, Yen CL, Wang WY, Chiang KC. Liver angiosarcoma, a rare liver malignancy, presented with intraabdominal bleeding due to rupture--a case report. World journal of surgical oncology. 2012 Jan 26:10():23. doi: 10.1186/1477-7819-10-23. Epub 2012 Jan 26 [PubMed PMID: 22280556]
Level 3 (low-level) evidenceZeng D, Zeng X, Duan J, Chen D, Zhu B. Clinical characteristics of primary hepatic angiosarcoma outcomes: a SEER database analysis. Translational cancer research. 2021 Jan:10(1):110-125. doi: 10.21037/tcr-20-2780. Epub [PubMed PMID: 35116244]
Tripke V, Heinrich S, Huber T, Mittler J, Hoppe-Lotichius M, Straub BK, Lang H. Surgical therapy of primary hepatic angiosarcoma. BMC surgery. 2019 Jan 10:19(1):5. doi: 10.1186/s12893-018-0465-5. Epub 2019 Jan 10 [PubMed PMID: 30630447]
Elliott P, Kleinschmidt I. Angiosarcoma of the liver in Great Britain in proximity to vinyl chloride sites. Occupational and environmental medicine. 1997 Jan:54(1):14-8 [PubMed PMID: 9072028]
Level 3 (low-level) evidenceTran Minh M, Mazzola A, Perdigao F, Charlotte F, Rousseau G, Conti F. Primary hepatic angiosarcoma and liver transplantation: Radiological, surgical, histological findings and clinical outcome. Clinics and research in hepatology and gastroenterology. 2018 Feb:42(1):17-23. doi: 10.1016/j.clinre.2017.02.006. Epub 2017 Apr 14 [PubMed PMID: 28416360]
Level 2 (mid-level) evidenceWagner MJ, Ravi V, Schaub SK, Kim EY, Sharib J, Mogal H, Park M, Tsai M, Duarte-Bateman D, Tufaro A, Loggers ET, Cranmer LD, Chau B, Hassett MJ, Grilley-Olson J, Paulson KG. Incidence and Presenting Characteristics of Angiosarcoma in the US, 2001-2020. JAMA network open. 2024 Apr 1:7(4):e246235. doi: 10.1001/jamanetworkopen.2024.6235. Epub 2024 Apr 1 [PubMed PMID: 38607625]
Averbukh LD, Mavilia MG, Einstein MM. Hepatic Angiosarcoma: A Challenging Diagnosis. Cureus. 2018 Sep 11:10(9):e3283. doi: 10.7759/cureus.3283. Epub 2018 Sep 11 [PubMed PMID: 30443453]
Millan M, Delgado A, Caicedo LA, Arrunategui AM, Meneses CA, Villegas JI, Serrano O, Caicedo L, Duque M, Echeverri GJ. Liver Angiosarcoma: Rare tumour associated with a poor prognosis, literature review and case report. International journal of surgery case reports. 2016:28():165-168. doi: 10.1016/j.ijscr.2016.09.044. Epub 2016 Sep 29 [PubMed PMID: 27718433]
Level 3 (low-level) evidenceLee SW, Song CY, Gi YH, Kang SB, Kim YS, Nam SW, Lee DS, Kim JO. Hepatic angiosarcoma manifested as recurrent hemoperitoneum. World journal of gastroenterology. 2008 May 14:14(18):2935-8 [PubMed PMID: 18473427]
Level 3 (low-level) evidenceMatsumoto M, Tamura M, Komiya T, Aridome G, Narita R, Hisaoka M, Ohtsuki M, Otsuji Y. Hepatic angiosarcoma: a rare liver tumor in a hemodialysis patient. Clinical nephrology. 2009 May:71(5):590-2 [PubMed PMID: 19473625]
Level 3 (low-level) evidenceForbes A, Portmann B, Johnson P, Williams R. Hepatic sarcomas in adults: a review of 25 cases. Gut. 1987 Jun:28(6):668-74 [PubMed PMID: 3623214]
Level 3 (low-level) evidenceRamakrishnan N, Mokhtari R, Charville GW, Bui N, Ganjoo K. Management Strategies and Outcomes in Primary Liver Angiosarcoma. American journal of clinical oncology. 2023 Oct 1:46(10):439-444. doi: 10.1097/COC.0000000000001032. Epub 2023 Aug 15 [PubMed PMID: 37580871]
Huang NC, Kuo YC, Chiang JC, Hung SY, Wang HM, Hung YM, Chang YT, Wann SR, Chang HT, Wang JS, Ho SY, Guo HR. Hepatic angiosarcoma may have fair survival nowadays. Medicine. 2015 May:94(19):e816. doi: 10.1097/MD.0000000000000816. Epub [PubMed PMID: 25984668]
Katou S, Di Pietro Martinelli C, Silveira C, Schmid F, Becker F, Radunz S, Juratli M, Morgul H, Banz V, Pascher A, Andreou A, Struecker B. Liver Resection for Primary Hepatic Angiosarcoma: Bicentric Analysis of a Challenging Entity. Journal of clinical medicine. 2022 May 25:11(11):. doi: 10.3390/jcm11112990. Epub 2022 May 25 [PubMed PMID: 35683376]
Tsunematsu S, Muto S, Oi H, Naka T, Kitagataya T, Sasaki R, Taya Y, Baba U, Tsukamoto Y, Uemura K, Kimura T, Ohara Y. Surgically Diagnosed Primary Hepatic Angiosarcoma. Internal medicine (Tokyo, Japan). 2018 Mar 1:57(5):687-691. doi: 10.2169/internalmedicine.9318-17. Epub 2017 Nov 20 [PubMed PMID: 29151516]
Zheng YW, Zhang XW, Zhang JL, Hui ZZ, Du WJ, Li RM, Ren XB. Primary hepatic angiosarcoma and potential treatment options. Journal of gastroenterology and hepatology. 2014 May:29(5):906-11. doi: 10.1111/jgh.12506. Epub [PubMed PMID: 24372769]
Kim HR, Rha SY, Cheon SH, Roh JK, Park YN, Yoo NC. Clinical features and treatment outcomes of advanced stage primary hepatic angiosarcoma. Annals of oncology : official journal of the European Society for Medical Oncology. 2009 Apr:20(4):780-7. doi: 10.1093/annonc/mdn702. Epub 2009 Jan 29 [PubMed PMID: 19179547]
Level 2 (mid-level) evidenceHuang IH, Wu YY, Huang TC, Chang WK, Chen JH. Statistics and outlook of primary hepatic angiosarcoma based on clinical stage. Oncology letters. 2016 May:11(5):3218-3222 [PubMed PMID: 27123094]
Level 3 (low-level) evidenceZeng D, Cheng J, Gong Z, Chen J, Long H, Zhu B. A pooled analysis of primary hepatic angiosarcoma. Japanese journal of clinical oncology. 2020 May 5:50(5):556-567. doi: 10.1093/jjco/hyaa017. Epub [PubMed PMID: 32083280]