 Anatomy, Bony Pelvis and Lower Limb: Calf
Anatomy, Bony Pelvis and Lower Limb: Calf
Introduction
The calf (Latin: sura) denotes the posterior compartment of the lower leg. This region is characterized by a prominent muscular contour that tapers inferiorly toward the ankle. The calf overlies the posterior aspects of the tibia and fibula and lies in proximity to major neural and vascular structures, including the tibial and sural nerves, popliteal artery, and posterior tibial vein. The calf plays a central role in posture, locomotion, and forceful plantarflexion during gait.
Dysfunction in the calf, whether from trauma, vascular compromise, or neuropathic injury, can result in impaired gait, muscle weakness, or chronic pain. Clinically, this region is significant for the assessment of compartment syndrome, evaluation of vascular status, and planning of surgical approaches. Detailed understanding of calf anatomy and function allows clinicians to diagnose conditions, such as deep vein thrombosis, muscle tears, and peripheral neuropathies, guide interventions like fasciotomy, tendon repair, or vascular access, and reduce the risk of iatrogenic injury to nerves and vessels.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Structure
The 2 largest muscles in the calf are the gastrocnemius and the soleus. The gastrocnemius is the most superficial muscle and has 2 heads, medial and lateral (see Image. Superficial Muscles of the Posterior Leg). The 2 heads converge to form a confluent muscle belly. The lateral head originates from the lateral surface of the lateral femoral condyle and the medial head from the posterior, nonarticular aspect of the medial femoral condyle. The muscle belly of the gastrocnemius joins the soleus distally to form the calcaneal tendon, also known as the Achilles tendon, which inserts onto the posterior calcaneus.[1][2][3][4] The gastrocnemius and soleus form the triceps surae muscle.[5]
The soleus is a large, flat muscle located deep to the gastrocnemius. The plantaris is a small muscle with a long tendinous portion, which can be mistaken for a nerve. The plantaris arises from the lateral supracondylar line of the femur and is absent in up to 10% of the population. The muscle descends medially, forming a tendon that runs between the gastrocnemius and soleus and blends with the calcaneal tendon.
Function
The calf muscles are responsible for plantarflexion of the foot and ankle. The muscles are engaged during running and jumping. The gastrocnemius is primarily active during explosive movements, whereas the soleus predominates during sustained activities such as standing or walking uphill.[6]
Embryology
In most cases, the upper limbs develop before the lower limbs. Lower limb formation begins at week 4 of gestation, with full differentiation of the limb by weeks 8 to 10. Limb buds emerge following activation of mesenchymal cells in the lateral plate mesoderm.
Blood Supply and Lymphatics
The blood supply of the calf muscles is derived from the popliteal artery, which bifurcates into the anterior and posterior tibial arteries (see Image. Arteries of the Lower Limb, Anterior and Posterior Views). The fibular (peroneal) artery arises from the posterior tibial artery. The posterior tibial artery courses alongside the tibial nerve and enters the plantar aspect of the foot via the tarsal tunnel. The anterior tibial artery passes anteriorly between the tibia and fibula through a gap in the interosseous membrane, extending the full length of the leg into the foot, where it continues as the dorsalis pedis artery.
The venous supply of the calf is divided into superficial and deep veins. The superficial veins include the greater and small saphenous veins (see Image. Venous Anatomy of the Lower Limb). The deep veins comprise the popliteal vein, anterior tibial vein, posterior tibial vein, and fibular vein.
The greater saphenous vein is the longest in the body and extends along the entire lower extremity. Cardiothoracic surgeons often harvest this vein for use in coronary artery bypass grafting. The small saphenous vein is a relatively large vein that runs along the posterior calf, passes between the heads of the gastrocnemius muscle, and typically drains into the popliteal vein (see Image. Venous Drainage, Right Leg).
The popliteal vein forms from the convergence of the anterior and posterior tibial veins. This blood vessel continues as the femoral vein upon entering the femoral region. The anterior tibial veins drain the knee, ankle, and tibiofibular joints, as well as portions of the anterior leg. The posterior tibial vein receives blood from the lateral and medial plantar veins and drains the posterior muscles of the lower leg and the plantar surface of the foot. The fibular (peroneal) veins carry blood from the lateral compartment of the leg and empty into the posterior tibial vein.[7]
Superficial lymphatics from the medial calf follow the great saphenous vein to the superficial inguinal lymph nodes.[8] Superficial lymphatics from the lateral calf follow the small (short) saphenous vein to the popliteal nodes.[9][10] Efferents from popliteal nodes proceed to deep (internal) inguinal or external iliac nodes. Deep lymphatic vessels accompany the deep veins of the calf and drain into the popliteal nodes and then the deep inguinal-external iliac chain. From the external iliac nodes, lymph ascends to the common iliac and lumbar (para-aortic) nodes, then to the cisterna chyli and the thoracic duct for return to the venous system.[11]
Nerves
The tibial nerve (S1, S2) supplies motor input to the majority of the calf muscles. The tibial nerve passes through the popliteal fossa and provides branches to the gastrocnemius, popliteus, soleus, and plantaris muscles. A cutaneous branch contributes to the formation of the sural nerve. Nerve roots L2 through L4 and L4 through S3 provide all motor and part of the sensory innervation for the lower limbs.[12]
Muscles
The lower leg comprises 4 compartments: anterior, lateral, superficial posterior, and deep posterior. The anterior compartment contains the tibialis anterior, extensor hallucis longus, extensor digitorum longus, peroneus tertius, and the deep peroneal nerve. The lateral compartment houses the peroneus longus and peroneus brevis, along with the superficial peroneal nerve.
The deep posterior compartment includes the tibialis posterior, flexor hallucis longus, flexor digitorum longus, popliteus, and the tibial nerve. The popliteus muscle, positioned behind the knee and forming the base of the popliteal fossa, acts exclusively at the knee by internally rotating the tibia relative to the femur, thus initiating flexion. The tibialis posterior, the deepest muscle of the compartment, originates from the interosseous membrane between the tibia and fibula, inverts and plantarflexes the foot, and maintains the medial arch. The flexor digitorum longus is located medially in the posterior leg and flexes the lateral 4 toes. The flexor hallucis longus is located laterally and flexes the great toe.
The superficial posterior compartment contains the gastrocnemius, soleus, plantaris, and the sural nerve. The tibial nerve provides innervation to all superficial and deep calf muscles.
Physiologic Variants
The soleus muscle demonstrates substantial morphological variability in fiber architecture, shape, length, and tendon characteristics across individuals. Differences in these features may affect biomechanical force generation, susceptibility to injury, and surgical planning.[13] A cadaveric study classified soleus morphology into distinct patterns based on pennation (bipennate, unipennate, multipennate, nonpennate), illustrating interindividual architectural diversity.[14]
The plantaris muscle shows high morphological variability in origin, course, and insertion. Multiple tendon insertion types exist, with some inserting to the calcaneus and others to adjacent fascia. Variability may impact force transmission and clinical interpretation on imaging. The plantaris muscle may be absent in a significant proportion of limbs, and classification schemas describe at least 8 distinct insertion morphologies in fetal studies, indicating developmental variation.[15]
Rare accessory muscle slips or accessory heads of the gastrocnemius have been documented. A case report described an accessory slip of the lateral head receiving innervation from a branch of the common peroneal nerve, rather than the tibial nerve, highlighting clinically relevant neural and structural variants. (Source: Kasat et al, 2025)
The calcaneal (Achilles) tendon, formed by gastrocnemius and soleus insertions, exhibits layer variability and nonuniform aponeurotic arrangements. Accessory muscular structures, including accessory soleus or extra gastrocnemius heads, may be present and influence tendon morphology and pathology.[16]
Surgical Considerations
Peripheral arterial disease of the lower extremity results from atherosclerotic plaque formation. Progressive plaque enlargement leads to claudication, or pain during ambulation. Treatment options include angioplasty, stenting, and lower extremity bypass grafting.[17]
Compartment syndrome arises from severe injuries, fractures, or surgical complications. Elevated pressure within a muscle compartment reduces blood flow and can cause tissue damage. The definitive treatment is fasciotomy.[18]
Reconstructive surgery involving calf muscles often addresses soft tissue defects around the knee and proximal lower leg resulting from trauma, infection, or prosthetic joint complications. The pedicled gastrocnemius muscle flap provides reliable vascularized coverage due to its robust pedicle and proximity to the defect, demonstrating high flap survival even in complex cases.[19][20] The soleus flap serves for more distal defects.[21] Poor technique may cause infection, wound dehiscence, and reduced range of motion. Preservation of vascular anatomy and meticulous flap inset can minimize these risks.[22]
Calf augmentation using silicone implants or autologous fat grafting is indicated for congenital or posttraumatic hypoplasia, muscular asymmetry, or cosmetic enhancement. Advantages include immediate contour improvement and long-term structural support with implants or a natural feel with fat grafting. Potential complications include implant malposition, infection, and fat resorption. Careful pocket creation, sterile technique, and meticulous fat processing reduce risks.
Calf reduction or liposuction treats excess adiposity or hypertrophic calves. Benefits include improved leg proportions and symmetry. Potential complications are contour irregularities, hematoma, or nerve injury. Precise technique, controlled aspiration, and avoidance of aggressive superficial liposuction mitigate these issues.[23][24]
Clinical Significance
Thrombosis can occur when the leg veins clot, creating a potential risk for pulmonary embolus. Stenosis or occlusion of the lower leg arteries can result in a cold ischemic leg, necessitating immediate intervention to salvage the limb. Nerve injuries can lead to various neurological deficits.
Compartment syndrome constitutes a surgical emergency requiring prompt fasciotomy. Increased pressure within the compartment causes tissue hypoperfusion. The fascia surrounding the compartment is inelastic, so swelling of muscles or bleeding within the compartment increases internal pressure.[25][26][27]
Foot drop is characterized by the inability to dorsiflex the forefoot due to weakness in the dorsiflexor muscles. Potential causes include neurologic, autoimmune, muscular, spinal, and musculoskeletal disorders. Foot drop can result in an unsteady gait, increasing the risk of falls. Treatment is directed at the underlying etiology.[28]
Other Issues
Achilles Tendon Pathology
Achilles tendon pathology, encompassing Achilles tendinopathy and Achilles tendon rupture, is a prevalent cause of posterior calf morbidity. Achilles tendinopathy is a degenerative, overuse condition marked by pain and functional impairment localized to the tendon, often related to repetitive mechanical loading and microtrauma. Risk factors include older age, high training volume, prior tendinopathy, elevated body mass index, and certain medications, including fluoroquinolones and corticosteroids.
Achilles tendon rupture typically occurs 2 to 6 cm proximal to calcaneal insertion and results from sudden tensile overload on a degenerated tendon. Acute rupture may be treated nonoperatively with functional rehabilitation or surgically, depending on the patient's activity level. Complications include rerupture, tendon elongation, and chronic functional deficits. Management begins with activity modification, progressive loading exercises, shockwave therapy, and adjunctive injections. Refractory cases may require surgical intervention.[29]
Genetic Myopathies Affecting the Calf Musculature
Duchenne muscular dystrophy (DMD) and its less severe variant, Becker muscular dystrophy (BMD), are X-linked recessive dystrophinopathies arising from mutations in the DMD gene (absent dystrophin in DMD, reduced or abnormal dystrophin in BMD). Dystrophin deficiency destabilizes the sarcolemma, causing repeated muscle fiber damage and progressive weakness. Boys are predominantly affected. Early in DMD, calf muscles demonstrate pseudohypertrophy due to fatty infiltration and fibrosis, whereas BMD shows milder or later-onset calf involvement.
Complications of these conditions stem from progressive muscle weakness and dystrophin deficiency. Calf pseudohypertrophy, contractures, and gait disturbances are common. Respiratory muscle involvement can lead to restrictive lung disease and infections. Cardiomyopathy and arrhythmias frequently develop. DMD generally presents in early childhood with delayed motor milestones and rapid functional decline. BMD onset is more variable. Management includes corticosteroids to slow progression and emerging gene-targeted therapies. Supportive care addresses respiratory, cardiac, and orthopedic complications, including gait impairment and risk of contractures.[30]
Media
(Click Image to Enlarge)
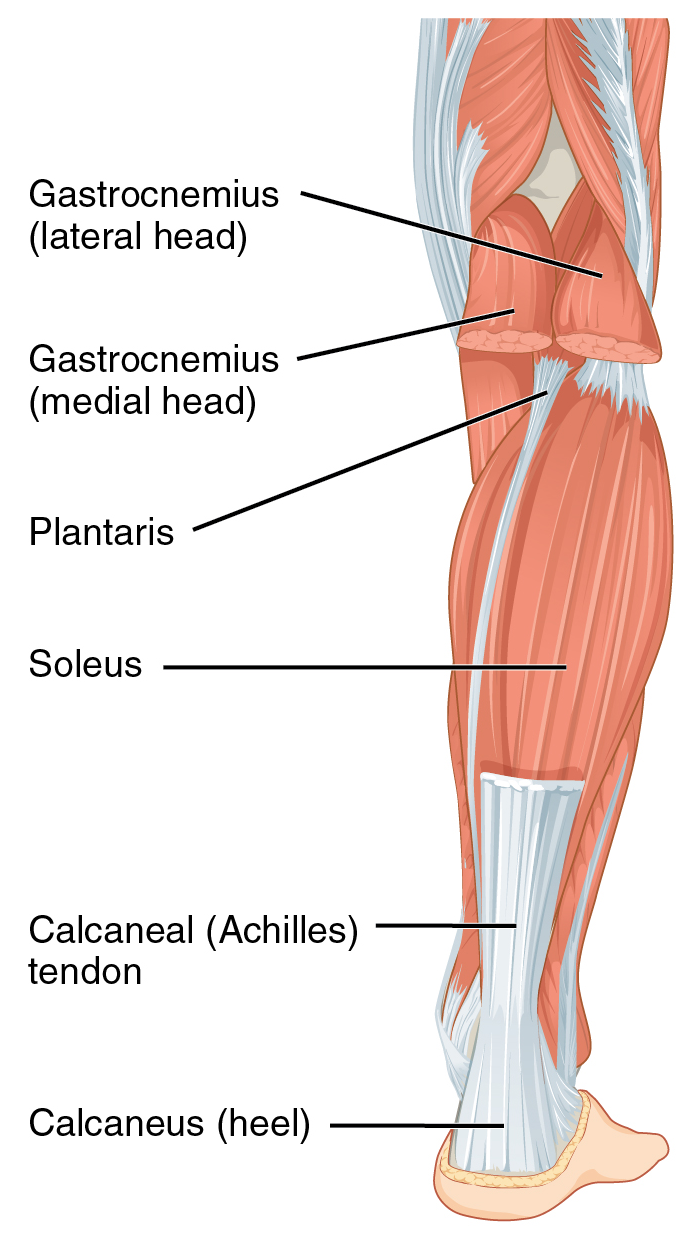
Superficial Muscles of the Posterior Leg. Labeled structures include the gastrocnemius, soleus, and plantaris muscles and their convergence into the calcaneal tendon inserting on the calcaneus.
JG Betts, KA Young, JA Wise, E Johnson, B Poe, DH Kruse, O Korol, JE Johnson, M Womble, P DeSaix, Public Domain, via Wikimedia Commons
{kind=link}
(Click Image to Enlarge)
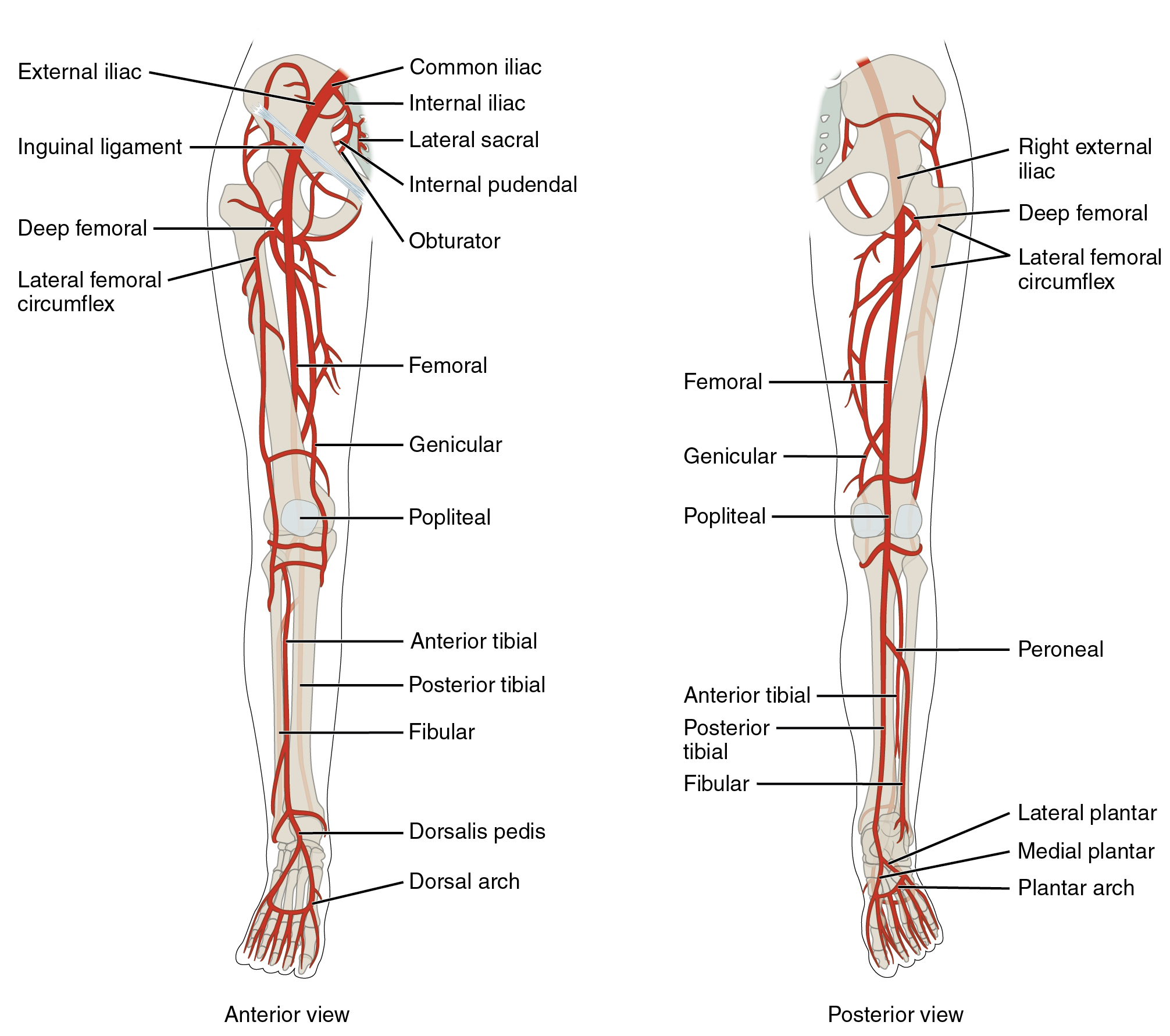
Arteries of the Lower Limb, Anterior and Posterior Views. This detailed illustration shows the arterial anatomy of the lower limb from both anterior and posterior perspectives. Labeled vessels include the common, external, and internal iliac arteries, femoral artery, profunda femoris (deep femoral) artery with its lateral and medial circumflex branches, genicular artery, popliteal artery, anterior and posterior tibial arteries, fibular (peroneal) artery, dorsalis pedis artery, medial and lateral plantar arteries, and the dorsal and plantar arches.
OpenStax College, Public Domain, via Wikimedia Commons
{kind=link}
(Click Image to Enlarge)
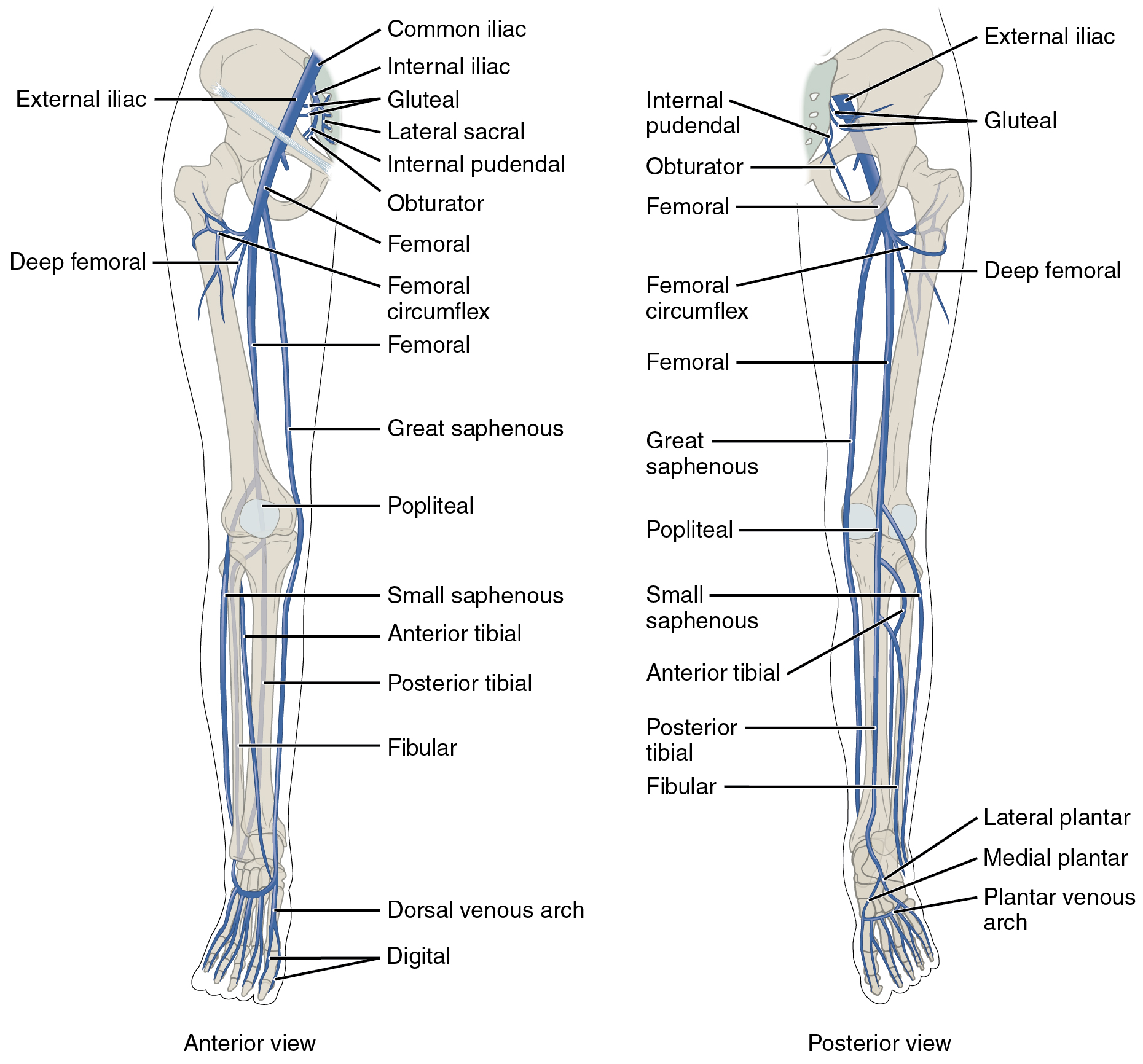
Venous Anatomy of the Lower Limb. This illustration presents a comparative view of the anterior and posterior venous systems of the leg. Key superficial structures identified include the great saphenous vein on the medial aspect and the small saphenous vein posteriorly. The diagram also details deep venous pathways such as the femoral, popliteal, and tibial veins, demonstrating the drainage pattern from the foot toward the femoral triangle. Additional labeled vessels include the common and external iliac veins, the deep femoral vein, and the fibular veins, as well as the dorsal and plantar venous arches and their associated metatarsal and plantar veins.
OpenStax College, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
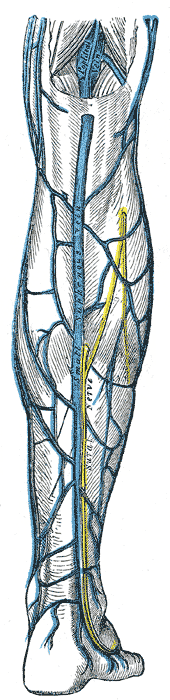
Venous Drainage, Right Leg. The diagram illustrates the drainage of the small saphenous vein into the deeper popliteal vein within the posterior compartment of the leg. The image also identifies the sural nerve, which provides sensory innervation to the posterolateral calf and follows the longitudinal path of the saphenous vasculature.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Mostafa E, Graefe SB, Varacallo MA. Anatomy, Bony Pelvis and Lower Limb: Leg Posterior Compartment. StatPearls. 2025 Jan:(): [PubMed PMID: 30726025]
Hardin JM, Devendra S. Anatomy, Bony Pelvis and Lower Limb: Calf Common Peroneal Nerve (Common Fibular Nerve). StatPearls. 2025 Jan:(): [PubMed PMID: 30422563]
Palmisano L, Launico MV. Anatomy, Bony Pelvis and Lower Limb: Calf Deep Peroneal Nerve (Deep Fibular Nerve). StatPearls. 2025 Jan:(): [PubMed PMID: 30252289]
Wong M, Jardaly AH, Kiel J. Anatomy, Bony Pelvis and Lower Limb: Achilles Tendon. StatPearls. 2025 Jan:(): [PubMed PMID: 29763092]
Lezak B, Varacallo MA. Anatomy, Bony Pelvis and Lower Limb: Calf Peroneus Longus Muscle. StatPearls. 2025 Jan:(): [PubMed PMID: 31536256]
Harðarson GR, Huseth KR, Aagaard P, Zügner R, Karlsson J, Brorsson A, Helander KN, Tranberg R. Differential contributions of lower leg muscle activation to plantar flexor function during single-leg hopping one year after Achilles tendon rupture: A shift from monoarticular to biarticular muscle work. Journal of biomechanics. 2026 Jan:195():113082. doi: 10.1016/j.jbiomech.2025.113082. Epub 2025 Nov 21 [PubMed PMID: 41308404]
Bordoni B, Varacallo MA. Anatomy, Bony Pelvis and Lower Limb, Gastrocnemius Muscle. StatPearls. 2025 Jan:(): [PubMed PMID: 30422541]
Shinaoka A, Koshimune S, Suami H, Yamada K, Kumagishi K, Boyages J, Kimata Y, Ohtsuka A. Lower-Limb Lymphatic Drainage Pathways and Lymph Nodes: A CT Lymphangiography Cadaver Study. Radiology. 2020 Jan:294(1):223-229. doi: 10.1148/radiol.2019191169. Epub 2019 Nov 19 [PubMed PMID: 31746690]
Elshikh M, Moawad AW, Salem U, Klimkowski SP, Hassan T, Rao Korivi B, Jensen CT, Javadi S, Elsayes KM. Oncologic Imaging of the Lymphatic System: Current Perspective with Multi-Modality Imaging and New Horizon. Cancers. 2021 Sep 10:13(18):. doi: 10.3390/cancers13184554. Epub 2021 Sep 10 [PubMed PMID: 34572781]
Level 3 (low-level) evidenceChauhan HM, Taqi M. Anatomy, Bony Pelvis and Lower Limb: Arches of the Foot. StatPearls. 2025 Jan:(): [PubMed PMID: 36508535]
Level 2 (mid-level) evidencePlutecki D, Bonczar M, Wilk J, Necka S, Joniec M, Elsaftawy A, Matuszyk A, Walocha J, Koziej M, Ostrowski P. The Anatomy of the Thoracic Duct and Cisterna Chyli: A Meta-Analysis with Surgical Implications. Journal of clinical medicine. 2024 Jul 23:13(15):. doi: 10.3390/jcm13154285. Epub 2024 Jul 23 [PubMed PMID: 39124550]
Level 1 (high-level) evidenceSpence KT, Forro SD. Anatomy, Bony Pelvis and Lower Limb: Nerves. StatPearls. 2025 Jan:(): [PubMed PMID: 30335337]
Olewnik Ł, Landfald IC, Ruzik K, Gołek Ł, Gonera B. The forgotten powerhouse: Variations of the soleus muscle and their clinical relevance. Annals of anatomy = Anatomischer Anzeiger : official organ of the Anatomische Gesellschaft. 2025 Aug:261():152696. doi: 10.1016/j.aanat.2025.152696. Epub 2025 Jul 8 [PubMed PMID: 40639549]
Olewnik Ł, Zielinska N, Paulsen F, Podgórski M, Haładaj R, Karauda P, Polguj M. A proposal for a new classification of soleus muscle morphology. Annals of anatomy = Anatomischer Anzeiger : official organ of the Anatomische Gesellschaft. 2020 Nov:232():151584. doi: 10.1016/j.aanat.2020.151584. Epub 2020 Aug 15 [PubMed PMID: 32810614]
Waśniewska-Włodarczyk A, Paulsen F, Olewnik Ł, Polguj M. Morphological variability of the plantaris tendon in the human fetus. Scientific reports. 2021 Aug 19:11(1):16871. doi: 10.1038/s41598-021-96391-8. Epub 2021 Aug 19 [PubMed PMID: 34413401]
Zielinska N, LaPrade RF, Olewnik Ł. Morphological variations of the calcaneal tendon: clinical significance. Journal of orthopaedic surgery and research. 2023 Apr 4:18(1):275. doi: 10.1186/s13018-023-03748-y. Epub 2023 Apr 4 [PubMed PMID: 37016428]
Carr JG, Langhoff R, DeRubertis BG, Hood KL, Krishnan P, Puttaswamy V, Zeller T, Secemsky EA. Published Evidence on Peripheral Atherectomy: A Meta-analysis and Systematic Literature Review of More Than 300 Original Investigations. Journal of the Society for Cardiovascular Angiography & Interventions. 2025 Nov:4(11):104009. doi: 10.1016/j.jscai.2025.104009. Epub 2025 Oct 21 [PubMed PMID: 41324060]
Level 1 (high-level) evidenceMarciano ND, Sarpong K, Smart J. A Case Report of Acute Compartment Syndrome. Journal of education & teaching in emergency medicine. 2024 Apr:9(2):V1-V5. doi: 10.21980/J87061. Epub 2024 Apr 30 [PubMed PMID: 38707942]
Level 3 (low-level) evidenceGkiatas I, Korompilia M, Kostas-Agnantis I, Tsirigkakis SE, Stavraki M, Korompilias A. Gastrocnemius pedicled muscle flap for knee and upper tibia soft tissue reconstruction. A useful tool for the orthopaedic surgeon. Injury. 2021 Dec:52(12):3679-3684. doi: 10.1016/j.injury.2021.04.009. Epub 2021 Apr 20 [PubMed PMID: 33892927]
Theil C, Stock ME, Gosheger G, Moellenbeck B, Schwarze J, Schmidt-Braekling T. Gastrocnemius Muscle Flaps for Soft Tissue Coverage in Periprosthetic Knee Joint Infection. The Journal of arthroplasty. 2020 Dec:35(12):3730-3736. doi: 10.1016/j.arth.2020.06.074. Epub 2020 Jun 30 [PubMed PMID: 32694027]
Hankiss J, Schmitz C. [The soleus muscle flap]. Operative Orthopadie und Traumatologie. 2013 Apr:25(2):145-51. doi: 10.1007/s00064-012-0197-0. Epub [PubMed PMID: 23519296]
Rovere G, Smakaj A, Calori S, Barbaliscia M, Ziranu A, Pataia E, Maccauro G, De Mauro D, Liuzza F. Use of muscular flaps for the treatment of knee prosthetic joint infection: A systematic review. Orthopedic reviews. 2022:14(2):33943. doi: 10.52965/001c.33943. Epub 2022 Apr 25 [PubMed PMID: 35774925]
Level 1 (high-level) evidenceEscandón JM, Sweitzer K, Amalfi AN, Mohammad A, Ciudad P, Manrique OJ. Calf augmentation and volumetric restoration: A systematic review and meta-analysis. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2022 Sep:75(9):3551-3567. doi: 10.1016/j.bjps.2022.06.051. Epub 2022 Jun 20 [PubMed PMID: 35965213]
Level 1 (high-level) evidenceAcharya P, Alagarasan AR, Khan M, Zuluaga Blanco JP, Cakir A, Abusada F, ALQahtani MF, Siddiqui HF. Shaping the Silhouette: A Comprehensive Review of Surgical Body Contouring Techniques for the Torso and Limbs. Cureus. 2025 Jul:17(7):e88737. doi: 10.7759/cureus.88737. Epub 2025 Jul 25 [PubMed PMID: 40861576]
Hsu D, Chang KV. Gastrocnemius Strain. StatPearls. 2025 Jan:(): [PubMed PMID: 30521187]
Medina Pabón MA, Naqvi U. Achilles Tendinopathy. StatPearls. 2025 Jan:(): [PubMed PMID: 30844176]
Mays RJ, Mays AA, Mizner RL. Efficacy of ankle-foot orthoses on walking ability in peripheral artery disease. Vascular medicine (London, England). 2019 Aug:24(4):324-331. doi: 10.1177/1358863X19831765. Epub 2019 Mar 29 [PubMed PMID: 30924412]
Nori SL, Stretanski MF. Foot Drop. StatPearls. 2025 Jan:(): [PubMed PMID: 32119280]
Knapik JJ, Pope R. Achilles Tendinopathy: Pathophysiology, Epidemiology, Diagnosis, Treatment, Prevention, and Screening. Journal of special operations medicine : a peer reviewed journal for SOF medical professionals. 2020 Spring:20(1):125-140. doi: 10.55460/QXTX-A72P. Epub [PubMed PMID: 32203618]
Duan D, Goemans N, Takeda S, Mercuri E, Aartsma-Rus A. Duchenne muscular dystrophy. Nature reviews. Disease primers. 2021 Feb 18:7(1):13. doi: 10.1038/s41572-021-00248-3. Epub 2021 Feb 18 [PubMed PMID: 33602943]