 Anatomy, Thorax, Heart Left Anterior Descending (LAD) Artery
Anatomy, Thorax, Heart Left Anterior Descending (LAD) Artery
Introduction
The continuously pumping myocardium requires oxygen and nutrients for normal function, supplied by blood from the coronary arteries. Occlusion of the coronary arteries can result in ischemic death of cardiomyocytes, leading to myocardial infarction. The intrinsic neovascular response of the heart to ischemic injury is typically insufficient to fully reestablish perfusion within the infarcted myocardium, which is subsequently replaced by nonfunctional scar tissue.
The coronary arteries originate from the aortic sinuses of the ascending aorta, just superior to the aortic valve at the sinotubular junction. Two main coronary arteries are present—the right and the left—both arising perpendicularly from the aorta.
The right coronary artery (RCA) arises from the right anterior aortic sinus. The left coronary artery (LCA), also referred to as the "left main coronary artery" (LMCA), arises from the left anterior aortic sinus. The LMCA bifurcates into the left anterior descending (LAD) artery, which courses over the interventricular septum within the anterior interventricular sulcus toward the cardiac apex and supplies the anteroseptal wall of the heart, and the left circumflex (LCx) coronary artery, which courses within the left atrioventricular groove and supplies the posterior and lateral portions (see Image. Gross Anatomy and Coronary Vasculature of the Heart).[1]
The LAD, also known as the anterior interventricular branch of the LCA, serves as the principal arterial supply to the anterior left ventricular wall and the majority of the interventricular septum. Owing to its extensive perfusion territory, occlusion of the LAD frequently results in a large myocardial infarction with marked impairment of left ventricular function and an adverse prognosis, leading to the clinical designation “widow-maker.” The LAD is a common target for both diagnostic imaging and coronary revascularization.[2][3]
Recognition of anatomical variants, including a “wrap-around” LAD and dual LAD anatomy, has become increasingly important for contemporary imaging, interventional planning, and surgical strategy. A comprehensive understanding of LAD anatomy, function, embryology, physiologic variants, procedural considerations, and clinical significance remains essential for practitioners involved in cardiac imaging, intervention, and education in coronary anatomy.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The LAD is the most critical coronary artery, supplying the largest myocardial territory, approximately 50% to 60% of the left ventricle. Owing to this extensive perfusion territory, even mild LAD lesions can have significant clinical consequences. LAD lesions account for more than half of all clinically significant coronary events. Several features distinguish the LAD from other coronary arteries. The vessel is typically longer, follows a more tortuous course, and is more frequently affected by atherosclerotic disease.
Like other epicardial coronary arteries, the LAD consists of 3 layers: the tunica intima, tunica media, and tunica adventitia. The tunica intima comprises a layer of endothelial cells supported by a thin subendothelial connective tissue layer and an internal elastic lamina. The tunica media is composed primarily of concentric layers of vascular smooth muscle cells, which regulate vessel diameter and contribute to the control of coronary blood flow. The outermost layer, the tunica adventitia, contains connective tissue, autonomic nerve fibers, and small vessels known as the vasa vasorum, which supply the arterial wall.[4][5]
The LAD carries approximately 50% of the total coronary blood flow. During systole, myocardial contraction compresses the perforating arteriolar branches, resulting in a marked reduction or transient cessation of blood flow. Therefore, coronary perfusion occurs predominantly during diastole, when pressure generated by cardiac contraction no longer impedes flow. Consequently, coronary blood flow depends primarily on diastolic blood pressure. As in other capillary beds, the coronary circulation is regulated by local autoregulatory mechanisms mediated by demand-dependent arteriolar dilation.[6][7]
The coronary arteries course along the epicardial surface of the heart, a location that limits significant compression during myocardial contraction. The LAD is the largest coronary artery and courses anterior to the interventricular septum within the anterior interventricular groove, extending from the base of the heart to the apex.
The LAD gives rise to septal and diagonal branches. Septal branches perforate the interventricular septum and supply the anterior 2/3 of the septum. These branches are designated S1, S2, and so forth, numbered sequentially from the base toward the apex. The diagonal branches course over the anterior surface of the left ventricle. These branches are designated D1, D2, and so forth, numbered from proximal to distal.
Near the apex, the LAD forms anastomoses with terminal branches of the posterior descending artery (PDA), most commonly a branch of the RCA in a right-dominant circulation pattern. A small left conus branch typically arises from the proximal LAD and anastomoses with a corresponding branch from the RCA around the aortic conus, as well as with the vasa vasorum of the aorta and pulmonary artery. Small right ventricular branches may also arise from the LAD and supply limited portions of the anterior right ventricle.
Multiple anastomoses exist between the coronary arteries. The terminal LAD anastomoses with the terminal branches of the PDA within the posterior interventricular groove in approximately 90% of cases, but no such anastomoses are present in approximately 10% of cases. Within the interventricular septum, septal branches of the LAD freely anastomose with septal branches of the PDA. However, flow through these anastomoses remains limited and is insufficient in the setting of sudden occlusion of a parent vessel. Gradual occlusion of a parent vessel may allow progressive enlargement of these anastomoses, enabling the development of clinically meaningful collateral flow. The LAD and its branches are epicardial vessels that give rise to end arteries, which perforate the myocardium to supply the underlying tissue.
Embryology
Research into the embryological origin and development of the coronary arteries is still ongoing. Both coronary arteries and veins are believed to derive from epicardial cells, indicating an extracardiac origin.[8] Development of the coronary arteries begins with the formation of a subepicardial vascular plexus, which subsequently invades the myocardium and gives rise to small vessels and capillaries. The primitive myocardium is thin and lined by endocardium. Nutrient and oxygen delivery occur directly from blood within the ventricular cavities through intertrabecular spaces lined by endocardium via passive diffusion.
Myocardial compaction and thickening occur with cardiac development. Passive diffusion from the ventricular cavities becomes insufficient to meet increasing metabolic demands. This transition is associated with the replacement of intramyocardial vasculature by vessels with subepicardial endothelium. Multiple progenitor sources are proposed for these endothelial cells, including the proepicardium or epicardium, the sinus venosus, and the endocardium.
A ring of subepicardial vascular plexus cells, termed the "peritruncal ring," forms around the base of the aorta and establishes connections with the aortic sinuses. Vascular endothelial growth factor (VEGF) family signaling molecules, particularly VEGF-A, expressed around the developing outflow tract, play a critical role in directing coronary artery development toward the aortic sinuses. The CXCL12/CXCR4 signaling pathway also contributes to coronary vascularization and endothelial cell migration. VEGF promotes arterialization, whereas the CXCL12/CXCR4 cascade promotes vascularization.
Coronary artery endothelial cells ultimately grow into the aortic wall via the aortic peritruncal ring, forming the coronary ostia. This developmental sequence supports the ingrowth hypothesis, which proposes that coronary vessels arise from subepicardial and peritruncal vascular plexuses that extend into the aortic wall to establish the coronary ostia. The earlier outgrowth hypothesis, which proposed endothelial sprouting from the aorta toward the myocardium, has largely been discounted by modern lineage tracing and molecular studies. Defective migration of coronary endothelial cells or downregulation of VEGF may result in congenital coronary artery anomalies.[9][10]
Blood Supply and Lymphatics
The vasa vasorum are small blood vessels that supply the walls of the coronary arteries and other large cardiac vessels. These blood vessels provide oxygen and nutrients to the outer layers of the vascular wall, particularly the tunica adventitia and the outer portion of the tunica media, which lie too far from the luminal blood supply to be nourished by diffusion alone.
Cardiac lymphatic vessels accompany the coronary arteries and veins along the epicardial surface of the heart. Lymphatic channels drain interstitial fluid from the myocardium and converge into larger collecting vessels that course along the coronary arteries toward the base of the heart. From the base, these vessels pass through the fibrous pericardium alongside the ascending aorta and pulmonary trunk. Cardiac lymphatic drainage ultimately empties into the tracheobronchial lymph nodes and then into the mediastinal lymph trunks, which subsequently drain into the thoracic duct or right lymphatic duct before returning lymph to the systemic venous circulation.[11]
Nerves
The LAD and its perfusion territory receive autonomic innervation from the cardiac plexus, which contains both sympathetic and parasympathetic fibers. The left coronary plexus, derived primarily from the left portion of the deep cardiac plexus, accompanies the branches of the LCA and contributes to the autonomic innervation of the left atrium and ventricle.
Sympathetic fibers arise from the cervical and upper thoracic sympathetic ganglia and reach the heart via the cardiac nerves. These fibers increase heart rate, myocardial contractility, and conduction velocity, and may also influence coronary vascular tone. Parasympathetic fibers originate from the vagus nerve (cranial nerve X) and modulate cardiac function primarily by decreasing heart rate and atrioventricular conduction.
Changes in myocardial metabolic demand produced by autonomic activity indirectly influence coronary blood flow. The balance between sympathetic and parasympathetic inputs plays an important role in regulating coronary vascular tone and myocardial perfusion, particularly during physiological stress or myocardial ischemia.[12]
Muscles
Like other epicardial coronary arteries, the LAD possesses a well-developed tunica media composed predominantly of concentric layers of vascular smooth muscle cells. These smooth muscle cells regulate coronary vascular tone by contracting or relaxing in response to neural, metabolic, and endothelial signals. Contraction of smooth muscle within the tunica media produces vasoconstriction, whereas relaxation results in vasodilation, thereby modulating coronary blood flow to match myocardial metabolic demand.
Epicardial coronary arteries, such as the LAD, function primarily as conductance vessels, delivering blood to the myocardium with relatively low resistance. The majority of coronary vascular resistance occurs in the smaller intramyocardial arterioles, where smooth muscle tone plays a dominant role in controlling regional myocardial perfusion.
Endothelial-derived factors, including nitric oxide, prostacyclin, and endothelin, as well as metabolic mediators released by the myocardium, influence the contractile activity of vascular smooth muscle and contribute to autoregulation of coronary blood flow. Pathological alterations in coronary smooth muscle function are implicated in several clinical conditions. Excessive smooth muscle contraction may contribute to coronary vasospasm, while proliferation and migration of smooth muscle cells into the intima play a key role in atherosclerotic plaque formation within the coronary arteries.[13]
Physiologic Variants
Myocardial Bridging
Coronary arteries course along the epicardial surface in the normal heart. In some individuals, a segment of a coronary artery runs intramyocardially beneath a band of myocardium, termed a "myocardial bridge." Myocardial bridging is identified in approximately 0.5% to 40% of individuals on clinical imaging and in 15% to 85% of cases in autopsy studies.[14] The condition may occur in any coronary artery, but the LAD is most commonly affected. Myocardial bridging is generally considered a physiologic variant when the LAD is only superficially covered by myocardial fibers. A deeper and longer intramyocardial course may be associated with myocardial ischemia, particularly when systolic compression of the bridged segment occurs due to surrounding myocardial fibers.[15]
Absent Left Main Coronary Artery
In some cases, the LMCA is absent, and the LAD and LCx arise directly from the aorta through a common ostium. In other cases, the LAD and LCx originate separately from 2 distinct ostia within the left aortic sinus.
Coronary Fistulae
Coronary fistulae are rare in adults but account for a significant proportion of congenital coronary anomalies in children. A fistulous communication between a coronary artery and a cardiac chamber is referred to as a "coronary–cameral fistula." A communication between a coronary artery and a venous structure is called a "coronary arteriovenous fistula." Most coronary fistulae are congenital, although acquired cases may occur secondary to iatrogenic procedures or trauma.
Anomalous Origin
Anomalous origin of the LCA from the pulmonary artery is a rare malformation (incidence of 0.25%–0.50%) in children with abnormal cardiac development, associated with a mortality rate of 90% in unoperated infants.[16] In some instances, the LAD may arise from the proximal RCA. The LAD and LCx may also originate separately, representing the most common form of congenital anomalous coronary artery malformation.[17]
Wrap-Around Left Anterior Descending Artery
Depending on length, the LAD is classified into 4 types. Type 1 does not supply the left ventricular apex. Type 2 supplies part of the apex, with the remainder supplied by the RCA. Type 3 supplies the entire apex. Type 4 supplies the apex and more than 25% of the inferior wall, referred to as a “wrap-around” LAD.
A wrap-around LAD has important clinical implications. In patients with anterior ST-elevation myocardial infarction (STEMI) caused by proximal LAD occlusion, a wrap-around LAD may result in a larger infarct territory, involving both the anterior wall and the apical or inferior regions of the left ventricle. This pattern has been associated with adverse long-term outcomes, including increased rates of left ventricular remodeling, heart failure, and stroke.[18][19]
Dual Left Anterior Descending Artery
This variant is rare, in which 2 separate LADs with variable origins supply the LAD territory. A short LAD and a long LAD are typically present. The majority of cases are asymptomatic.[20]
Surgical Considerations
The LAD is the most critical target in coronary artery bypass grafting. The left internal mammary artery (LIMA), mobilized from the chest wall while preserving its origin, is commonly anastomosed end-to-side to the LAD. LIMA–LAD grafts demonstrate excellent long-term patency and confer prognostic benefit.
Due to its anterior epicardial course, the LAD is susceptible to incidental radiation exposure during left-sided breast cancer radiotherapy. Even relatively modest radiation doses may induce endothelial injury and accelerate atherosclerotic changes, particularly in the proximal and middle segments of the artery. Modern radiotherapy techniques, including deep inspiration breath-hold and advanced planning methods such as intensity-modulated radiotherapy and volumetric modulated arc therapy, treat the LAD and left ventricle as distinct organs at risk, thereby substantially reducing radiation exposure and the risk of radiation-induced coronary artery disease.[21]
Clinical Significance
Compared with other coronary arteries, occlusion of the LAD, resulting in anterior STEMI, is associated with the highest risk of poor clinical outcomes.[22] The LAD is typically the largest branch of the LCA and supplies a substantial portion of the myocardium. Atherosclerotic or thrombotic occlusion of this vessel causes myocardial infarction involving large regions of the anterior, septal, and apical myocardium, leading to significant impairment of cardiac function. Consequently, restoration of LAD flow during revascularization, whether percutaneous or surgical, is a critical therapeutic goal.[23][24]
Infarctions associated with LAD occlusion frequently involve the apex. Apical involvement may be accompanied by mural thrombus formation within the left ventricle. These thrombi may embolize and result in stroke or systemic embolic events.
The LAD’s extensive perfusion territory and unique flow dynamics expose the vessel to higher shear stress and turbulent flow, promoting early and aggressive atherosclerosis. LAD plaques demonstrate relatively consistent progression and increased vulnerability compared with plaques in the LCx or RCA, particularly within the proximal LAD, due to anatomical configuration and high myocardial demand. LAD involvement correlates strongly with major adverse cardiac events and carries significant prognostic weight in coronary artery disease.[25] LAD infarctions are associated with higher short-term mortality, increased incidence of heart failure and stroke, and poorer outcomes, particularly among women and patients with multivessel disease.
Fractional flow reserve (FFR) is an invasive physiologic index defined as the ratio of maximal achievable blood flow distal to a coronary stenosis to the theoretical normal flow in that vessel, typically measured during adenosine-induced hyperemia. An FFR value less than or equal to 0.80 generally indicates hemodynamically significant stenosis warranting revascularization.
The LAD exhibits distinct physiological behavior during FFR assessment, often yielding lower values for comparable angiographic stenosis. These differences reflect the extensive perfusion territory, higher hyperemic flow demand, and flow dynamics rather than ischemic burden alone. Therefore, vessel-specific FFR considerations are relevant for LAD lesions, as reliance on the conventional 0.80 cutoff may overestimate the need for revascularization in this artery.
Media
(Click Image to Enlarge)
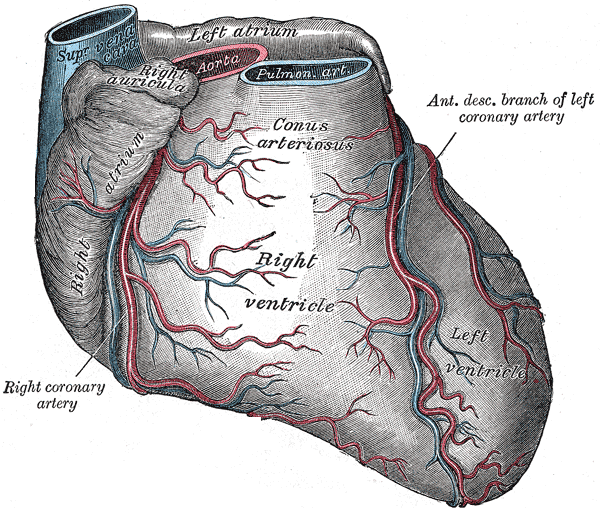
Gross Anatomy and Coronary Vasculature of the Heart. This illustration depicts the anterior surface of the heart, highlighting the major chambers and great vessels, including the superior vena cava, aorta, and pulmonary artery. The branching patterns of the right coronary artery and the anterior descending branch of the left coronary artery are traced across the ventricular epicardium. Labels identify the conus arteriosus and the relationship between the right auricle and the underlying atrium.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Thiene G, Frescura C, Padalino M, Basso C, Rizzo S. Coronary Arteries: Normal Anatomy With Historical Notes and Embryology of Main Stems. Frontiers in cardiovascular medicine. 2021:8():649855. doi: 10.3389/fcvm.2021.649855. Epub 2021 May 31 [PubMed PMID: 34136540]
Bauke F, Schmitz T, Harmel E, Raake P, Heier M, Linseisen J, Peters A, Meisinger C. Anterior-wall and non-anterior-wall STEMIs do not differ in long-term mortality: results from the augsburg myocardial infarction registry. Frontiers in cardiovascular medicine. 2023:10():1306272. doi: 10.3389/fcvm.2023.1306272. Epub 2024 Jan 8 [PubMed PMID: 38259315]
Karwowski J, Gierlotka M, Gąsior M, Poloński L, Ciszewski J, Bęćkowski M, Kowalik I, Szwed H. Relationship between infarct artery location, acute total coronary occlusion, and mortality in STEMI and NSTEMI patients. Polish archives of internal medicine. 2017 Jun 30:127(6):401-411. doi: 10.20452/pamw.4018. Epub 2017 May 5 [PubMed PMID: 28475171]
Entezarjou A, Mohammad MA, Andell P, Koul S. Culprit vessel: impact on short-term and long-term prognosis in patients with ST-elevation myocardial infarction. Open heart. 2018:5(2):e000852. doi: 10.1136/openhrt-2018-000852. Epub 2018 Sep 5 [PubMed PMID: 30228908]
Seo CO, Kim H, Koh JS. Fractional Flow Reserve in the Left Anterior Descending Artery. Journal of clinical medicine. 2025 Aug 1:14(15):. doi: 10.3390/jcm14155429. Epub 2025 Aug 1 [PubMed PMID: 40807049]
Bozbeyoğlu E, Aslanger E, Yıldırımtürk Ö, Şimşek B, Karabay CY, Türer A, Kozan Ö, Değertekin M. An algorithm for the differentiation of the infarct territory in difficult to discern electrocardiograms. Journal of electrocardiology. 2018 Nov-Dec:51(6):1055-1060. doi: 10.1016/j.jelectrocard.2018.09.006. Epub 2018 Sep 11 [PubMed PMID: 30497730]
Shaikh SSA, Munde K, Patil V, Phutane M, Singla R, Khan Z, Bansal NO. "Superdominant" Left Anterior Descending Artery Continuing as Posterior Descending Artery: Extremely Rare Coronary Artery Anomaly. Cardiology research. 2018 Aug:9(4):253-257. doi: 10.14740/cr738w. Epub 2018 Aug 10 [PubMed PMID: 30116455]
Winter EM, Gittenberger-de Groot AC. Epicardium-derived cells in cardiogenesis and cardiac regeneration. Cellular and molecular life sciences : CMLS. 2007 Mar:64(6):692-703 [PubMed PMID: 17380310]
Tian X, Zhou B. Coronary vessel formation in development and regeneration: origins and mechanisms. Journal of molecular and cellular cardiology. 2022 Jun:167():67-82. doi: 10.1016/j.yjmcc.2022.03.009. Epub 2022 Mar 27 [PubMed PMID: 35354073]
Ramai D, Lai J, Monzidelis C, Reddy S. Coronary Artery Development: Origin, Malformations, and Translational Vascular Reparative Therapy. Journal of cardiovascular pharmacology and therapeutics. 2018 Jul:23(4):292-300. doi: 10.1177/1074248418769633. Epub 2018 Apr 11 [PubMed PMID: 29642708]
Brakenhielm E, Alitalo K. Cardiac lymphatics in health and disease. Nature reviews. Cardiology. 2019 Jan:16(1):56-68. doi: 10.1038/s41569-018-0087-8. Epub [PubMed PMID: 30333526]
Wink J, van Delft R, Notenboom RGE, Wouters PF, DeRuiter MC, Plevier JWM, Jongbloed MRM. Human adult cardiac autonomic innervation: Controversies in anatomical knowledge and relevance for cardiac neuromodulation. Autonomic neuroscience : basic & clinical. 2020 Sep:227():102674. doi: 10.1016/j.autneu.2020.102674. Epub 2020 May 16 [PubMed PMID: 32497872]
Goodwill AG, Dick GM, Kiel AM, Tune JD. Regulation of Coronary Blood Flow. Comprehensive Physiology. 2017 Mar 16:7(2):321-382. doi: 10.1002/cphy.c160016. Epub 2017 Mar 16 [PubMed PMID: 28333376]
Kastellanos S, Aznaouridis K, Vlachopoulos C, Tsiamis E, Oikonomou E, Tousoulis D. Overview of coronary artery variants, aberrations and anomalies. World journal of cardiology. 2018 Oct 26:10(10):127-140. doi: 10.4330/wjc.v10.i10.127. Epub [PubMed PMID: 30386490]
Level 3 (low-level) evidenceSternheim D, Power DA, Samtani R, Kini A, Fuster V, Sharma S. Myocardial Bridging: Diagnosis, Functional Assessment, and Management: JACC State-of-the-Art Review. Journal of the American College of Cardiology. 2021 Nov 30:78(22):2196-2212. doi: 10.1016/j.jacc.2021.09.859. Epub [PubMed PMID: 34823663]
Tahir H, Ahmad S, Awan MU, Omar B, Glass J, Cole J. Anomalous Origin of Left Anterior Descending Artery and Left Circumflex Artery from Right Coronary Sinus with Malignant Left Anterior Descending Artery Course: Role of Coronary CT Angiography Derived Fractional Flow Reserve in Decision Making. Cureus. 2018 Aug 28:10(8):e3220. doi: 10.7759/cureus.3220. Epub 2018 Aug 28 [PubMed PMID: 30405995]
Masoumi S, Separham A, Parizad R, Jafarisis S, Assefi M. Dual Left Anterior Descending Artery: Clinical Overview and Interventional Management. The journal of Tehran Heart Center. 2023 Apr:18(2):146-150. doi: 10.18502/jthc.v18i2.13326. Epub [PubMed PMID: 37637287]
Level 3 (low-level) evidenceKobayashi N, Maehara A, Brener SJ, Généreux P, Witzenbichler B, Guagliumi G, Peruga JZ, Mehran R, Mintz GS, Stone GW. Usefulness of the Left Anterior Descending Coronary Artery Wrapping Around the Left Ventricular Apex to Predict Adverse Clinical Outcomes in Patients With Anterior Wall ST-Segment Elevation Myocardial Infarction (from the Harmonizing Outcomes With Revascularization and Stents in Acute Myocardial Infarction Trial). The American journal of cardiology. 2015 Dec 1:116(11):1658-65. doi: 10.1016/j.amjcard.2015.09.004. Epub 2015 Sep 11 [PubMed PMID: 26433272]
Level 2 (mid-level) evidenceKobayashi N, Maehara A. Left anterior descending artery wrapping around the left ventricular apex predicts additional risk of future events after anterior myocardial infarction. Anatolian journal of cardiology. 2019 Apr:21(5):259-260. doi: 10.14744/AnatolJCardiol.2019.79803. Epub [PubMed PMID: 31062762]
Kassem J, Yildiz A, Gowda M, Shahab H. Dual left anterior descending artery: A case report. Journal of clinical imaging science. 2024:14():47. doi: 10.25259/JCIS_122_2024. Epub 2024 Dec 3 [PubMed PMID: 39639884]
Level 3 (low-level) evidenceDiremsizoglu U, Topal N, Konuk AO, Suyusal IH, Genc D, Ari O, Cevik HF, Kefeli AU, Aksu MG, Sarper EB. Strategies to Reduce Left Anterior Descending Artery and Left Ventricle Organ Doses in Radiotherapy Planning for Left-Sided Breast Cancer. Reviews in cardiovascular medicine. 2025 Feb:26(2):26366. doi: 10.31083/RCM26366. Epub 2025 Feb 21 [PubMed PMID: 40026509]
Karha J, Murphy SA, Kirtane AJ, de Lemos JA, Aroesty JM, Cannon CP, Antman EM, Braunwald E, Gibson CM, TIMI Study Group. Evaluation of the association of proximal coronary culprit artery lesion location with clinical outcomes in acute myocardial infarction. The American journal of cardiology. 2003 Oct 15:92(8):913-8 [PubMed PMID: 14556865]
Level 2 (mid-level) evidenceCarrington M, Santos AR, Picarra BC, Pais JA. De Winter pattern: a forgotten pattern of acute LAD artery occlusion. BMJ case reports. 2018 Nov 8:2018():. pii: bcr-2018-226413. doi: 10.1136/bcr-2018-226413. Epub 2018 Nov 8 [PubMed PMID: 30413454]
Level 3 (low-level) evidenceAlsamara M, Degheim G, Gholkar G, Hiner E, Zughaib M. Is symptom to balloon time a better predictor of outcomes in acute ST-segment elevation myocardial infarction than door to balloon time? American journal of cardiovascular disease. 2018:8(4):43-47 [PubMed PMID: 30498623]
Bax AM, Lin FY, van Rosendael AR, Ma X, Lu Y, van den Hoogen IJ, Gianni U, Tantawy SW, Andreini D, Budoff MJ, Cademartiri F, Chinnaiyan K, Choi JH, Conte E, de Araújo Gonçalves P, Gottlieb I, Hadamitzky M, Leipsic JA, Maffei E, Pontone G, Stone G, Shin S, Kim YJ, Lee BK, Chun EJ, Sung JM, Lee SE, Berman DS, Narula J, Chang HJ, Shaw LJ. Marked variation in atherosclerotic plaque progression between the major epicardial coronary arteries. European heart journal. Cardiovascular Imaging. 2022 Oct 20:23(11):1482-1491. doi: 10.1093/ehjci/jeac044. Epub [PubMed PMID: 35471406]