Introduction
Lateral medullary syndrome (LMS), also known as Wallenberg syndrome, is a neurological disorder affecting the dorsolateral medulla oblongata, most commonly caused by ischemic infarction of the posterior inferior cerebellar artery (PICA) or the vertebral artery (see Image. Lateral Medullary Syndrome). Lateral medullary syndrome was named after Adolf Wallenberg (1862–1949), a German neurologist and neuroanatomist who reported the first case of LMS. LMS and the resulting ischemic injury affect multiple neural structures in the posterolateral medulla, located posterior to the inferior olivary nucleus.
Affected structures include the inferior cerebellar peduncle, spinocerebellar tract, spinothalamic tract, descending sympathetic fibers, spinal trigeminal nucleus and tract, vestibular nuclei, and the nuclei and fibers of cranial nerves IX and X. Involvement of these structures results in a classic constellation of symptoms, including ipsilateral facial sensory loss, contralateral loss of pain and temperature sensation in the body, vertigo, ataxia, dysphagia, hoarseness, and Horner syndrome.[1][2][3][4] Results from recent systematic reviews continue to underscore the clinical heterogeneity of LMS and emphasize the importance of early multimodal neuroimaging for diagnosis.[5]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
LMS is most commonly caused by an acute ischemic stroke affecting the dorsolateral medulla due to a thrombus or embolism of the vertebral artery or PICA. Less common causes include injury to the vertebral artery in the neck, dissection, arteriovenous malformation, or arteritis. The most important risk factors for LMS are hypertension, diabetes mellitus, and cigarette smoking. The common etiologies of LMS are as follows:
- Atherosclerotic disease: Atherosclerotic disease is typically due to thromboembolism or, less commonly, hemodynamic insufficiency.
- Cardiogenic embolism: Cardiogenic embolism is associated with atrial fibrillation,[6] mechanical heart valves, intracardiac thrombi, dilated cardiomyopathy, myocardial infarction, and infective endocarditis. Cocaine use, neck manipulation, medullary tumors, radiation necrosis, and hematomas may also lead to embolism.
- Vertebral artery dissection: Vertebral artery dissection is particularly seen in younger individuals presenting with headache and neurological symptoms consistent with LMS.[7]
- Hypoplastic vertebral artery: Hypoplastic vertebral artery is a rare cause, especially in younger patients with additional risk factors.[8]
- Surgical trauma: PICA is often exposed and injured during surgical procedures, especially telovelar approaches.[9]
- Arteriovenous malformation and aneurysms: Arteriovenous malformations and aneurysms are common causes of LMS, especially when involving the PICA.
- Vertebrobasilar dolichoectasia and ectatic PICA: These malformations compress the medulla and cranial nerves, causing neurovascular compression syndromes.[9]
- Connective tissue diseases: Ehlers-Danlos syndrome, Marfan syndrome, and fibromuscular dysplasia can weaken the walls of blood vessels.
Less common causes include subclavian steal syndrome, rotational vertebral artery compression syndrome, Fabry disease, mitochondrial encephalopathy, lactic acidosis, and migraine headache.[10][11]
Epidemiology
Posterior circulation strokes represent about 20% of all ischemic strokes. Results from a 2024 registry of more than 2900 strokes showed that posterior circulation strokes accounted for 28.8%, with LMS representing 12%.[12] Notably, lateral medullary infarcts occur more frequently in those who consume alcohol.[13] Angiography showing vertebral artery involvement is more common (67%) than isolated PICA involvement (10%). PICA-related infarcts are often due to cardiogenic embolism.[8] Between 51% and 94% of patients with lateral medullary syndrome experience some degree of dysphagia.[1][3]
Pathophysiology
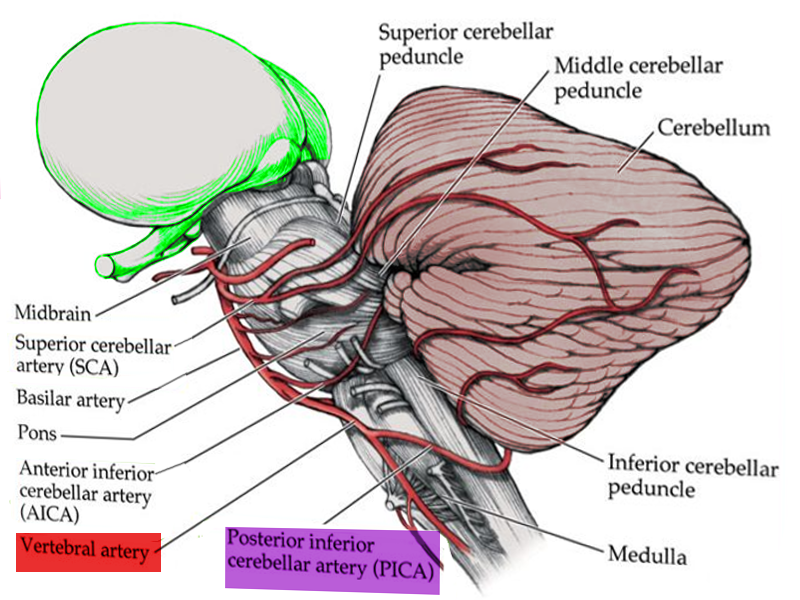
Large artery atherothrombosis accounts for nearly 75% of LMS cases, followed by cardioembolism in 17% and vertebral artery dissection in 8%.[4] Pathophysiologically, the clinical features of LMS correlate with the affected structures in the dorsolateral medulla, an area supplied by the PICA, a branch of the vertebral artery (see Image. Anatomy of Brain Vascular Territories). Therefore, LMS is commonly caused by vertebral artery occlusion. Clinical features of LMS are correlated with dysfunction of neuroanatomical structures as outlined below:
- Vestibular nuclei: Dizziness, vertigo, nystagmus, skew deviation, nausea, and vomiting
- Spinocerebellar tracts and the inferior cerebellar peduncle: Ipsilateral ataxia and lateral pulsion [1][3][8]
- Caudal trigeminal nucleus and tract: Ipsilateral facial sensation abnormalities, primarily involving pain and temperature
- Spinothalamic tract: Contralateral pain and temperature loss affecting the arm, body, and leg
- Descending sympathetic fibers: Ipsilateral Horner syndrome
- Nucleus ambiguus: Ipsilateral dysphagia, dysarthria, and dysphonia [8][14]
- The cough reflex may also be impaired [3]
- Nucleus and tractus solitarius: Ipsilateral taste impairment
Results from a 2025 prospective study using flexible endoscopic evaluation of swallowing and high-resolution pharyngeal manometry demonstrated severe pharyngeal sensory loss and delayed swallow initiation in medullary strokes compared with cerebellar strokes.[15] Additionally, hyponatremia after a brain injury occurs due to the syndrome of inappropriate antidiuretic hormone secretion and cerebral salt wasting syndrome. Syndrome of inappropriate antidiuretic hormone secretion has been reported in patients with lateral medullary infarction. The proposed pathophysiology involves failure of nonosmotic stimuli to propagate from the carotid sinus to the nucleus tractus solitarius via the vagus nerve due to a lesion in the nucleus tractus solitarius of the medulla. This lesion causes disinhibition of pituitary antidiuretic hormone secretion, leading to the syndrome of inappropriate antidiuretic hormone secretion.[16]
Other clinical findings are rarer but have corresponding anatomical variations. Ipsilateral hemiparesis, known as the Opalski variant, has been attributed to LMS affecting the lateral medulla, caudal to the corticospinal decussation, as discussed in a 2024 case report.[17] Life-threatening bradycardia precipitated by vertebral dissection–related LMS has also been reported.[18] Moreover, persistent hiccups are believed to result from the involvement of the nucleus ambiguus or adjacent respiratory regulatory centers.
History and Physical
Many patients with LMS are older adults with multiple vascular risk factors. Typical symptoms include acute onset of vertigo, dizziness, nystagmus, ataxia, nausea, vomiting, dysphagia, hiccups, dysphonia, facial pain, visual disturbances, and headaches. Sensory signs and symptoms are the most frequent manifestations (96%). Ipsilateral extremity ataxia, Horner syndrome, and sensory impairments are also common. Less common clinical presentations include dysarthria, skew deviation, oscillopsia due to nystagmus, and ipsilateral lateral pulsion.
Gradual onset occurs in approximately 25% of cases, progressing over several hours to days, with symptoms of headache, dizziness, vertigo, or gait ataxia, followed by sensory deficits, hiccups, hoarseness, and dysphagia. Weakness is a relatively uncommon feature of LMS, often resulting in a missed diagnosis. Partial syndromes are also more common than complete syndromes.[1][2][8][10][16]
Classic signs of LMS include:
- Impaired pain and thermal sensation over the contralateral side of the trunk and limbs
- Impaired pain and thermal sensation over the ipsilateral face
- Ipsilateral Horner syndrome, including partial ptosis, miosis, and facial anhidrosis
- Ipsilateral extremity ataxia
- Ipsilateral taste impairment
- Dysphagia
- Nystagmus, either horizontal or rotational, beating opposite to the side of the lesion, or directionally changing gaze-evoked, and is sometimes accompanied by skew deviation
- Intractable hiccups, which may lead to diagnostic delay
The clinical presentation varies depending on the size and location of the infarct.[4]
Evaluation
Evaluating patients with LMS should include a detailed clinical history, physical examination, and appropriate testing, including:
- Screening for stroke risk factors such as hypertension, diabetes mellitus, smoking history, and heart disease. A history of neck pain, trauma, or headache, particularly in younger patients, may suggest vertebral artery dissection (see Image. Vertebral Artery Anatomy in the Neck Region).[8][11]
- A complete neurological examination is critical because LMS is a clinical diagnosis based on a characteristic history and constellation of physical findings.
- Routine blood testing, including blood glucose levels and serum electrolyte levels, is appropriate.
- An electrocardiogram is necessary to screen for atrial fibrillation.
- Transthoracic echocardiography with Doppler carotid ultrasonography, CT, or magnetic resonance angiography may be indicated.
- Clinical and instrumental swallowing evaluations assess swallowing function and are performed using videofluoroscopy or fiberendoscopy.[3]
Diagnostic Imaging Tests
A brain CT scan is typically the initial imaging test for patients with lateral medullary syndrome, similar to any emergent evaluation for a patient with acute ischemic stroke symptoms. However, CT provides suboptimal visualization of posterior fossa structures due to bony obscuration. Early ischemic changes are often not visible.[11] Magnetic resonance imaging of the brain provides better visualization of soft tissue structures. For example, an imaging protocol that includes fluid-attenuated inversion recovery sequences improves the visualization of medullary infarction.[8][10] Additionally, diffusion-weighted MRI can detect an infarct earlier.
Neurovascular Studies
CT angiography and MR angiography examinations are advanced imaging studies that may be clinically indicated, often in consultation with a neurologist.
Treatment / Management
Similar to the treatment of any acute ischemic stroke, the principle of time is brain underscores the need for rapid evaluation. An algorithmic approach should be developed within each hospital.[19] Results from studies showed that treatment in certified stroke centers improves overall patient outcomes.[20] Treatment aims to reduce the infarct size and prevent medical complications, thereby improving patient outcomes and prognosis.[4] Standard acute ischemic stroke algorithms apply, including intravenous thrombolysis, endovascular thrombectomy, blood pressure control, and antiplatelet or anticoagulant therapy (see Image. Blood Supply to Medulla). Endovascular thrombectomy (EVT) for large-vessel occlusion in the anterior circulation can be efficacious up to 24 hours after onset (see Image. Diagram of Brain Circulation). The outcomes of endovascular thrombectomy for posterior circulation large-vessel occlusion, including the vertebral artery and basilar arteries, remain largely uncertain.[21] Patients with posterior circulation large-vessel occlusion should be treated at certified stroke centers with interventional neuroradiologists and receive individualized treatment plans to achieve the best outcomes.[22]
Intravenous Alteplase and Intravenous Tenecteplase
Tenecteplase offers advantages over alteplase, including a longer half-life (20-24 minutes versus 5 minutes), 15-fold higher fibrin specificity with less systemic lytic effect, and the ability to be administered as a single intravenous bolus. Tenecteplase is also more cost-effective. Furthermore, results from recent studies indicated that tenecteplase has a comparable efficacy and safety profile to alteplase.[23][24][25] According to the 2023 American Heart Association guidelines, it may be reasonable to choose tenecteplase over alteplase in patients without contraindications to intravenous fibrinolytics and who are eligible for mechanical thrombectomy.[19] Tenecteplase is typically given with an intravenous bolus of 0.25 mg/kg over 5 seconds and has become the fibrinolytic agent of choice at most stroke centers in the US.[26] The new treatment guidelines recommend either alteplase or tenecteplase within the 4.5-hour treatment window, regardless of National Institutes of Health Stroke Scale (NIHSS) score, and without advanced imaging. The new guidelines also provide support for select patients with stroke of unknown onset, including wake-up strokes or 4.5 to 9 hours from onset, using advanced imaging criteria such as fluid-attenuated inversion recovery–diffusion mismatch or diffusion-perfusion mismatch.[27][28](A1)
Magnetic Resonance Imaging–Guided Thrombolysis for Stroke With Unknown Time of Onset
Many patients wake up with symptoms of an acute stroke, rendering them ineligible for intravenous thrombolytic therapy because their last known normal state was at bedtime. The Efficacy and Safety of Magnetic Resonance Imaging–Based Thrombolysis in Wake-Up Stroke (WAKE-UP) Stroke Trial used the mismatch between a positive diffusion-weighted imaging (DWI) MRI sequence, indicating an acute ischemic infarction, and a negative fluid-attenuated inversion recovery (FLAIR) MRI sequence, suggesting that the infarct occurred within 4.5 hours of the MRI. Diffusion-weighted imaging becomes positive within 30 minutes of an acute infarct, whereas the fluid-attenuated inversion recovery sequence typically remains negative until about 4.5 hours after onset. This mismatch suggests the stroke occurred within the 4.5-hour window, making the patient eligible for intravenous thrombolytic therapy.[28][29] Patients with mild nondisabling acute ischemic stroke deficits, such as isolated sensory symptoms within 4.5 hours, should not receive intravascular thrombolysis, and dual antiplatelet therapy is reasonable.[30][31][32][33][31](A1)
Endovascular Therapy
The 2026 guidelines recommend EVT for acute ischemic stroke caused by basilar artery occlusion with a baseline modified Rankin Scale score of 0 to 1, NIHSS score 10 or greater, and posterior circulation Alberta Stroke Program Early CT Score of 6 or greater, indicating mild ischemic damage on CT, within 24 hours of symptom onset. However, the effectiveness of EVT for NIHSS scores less than 10 has not been established. Results from a recent review and meta-analysis (VERITAS) of acute ischemic stroke due to vertebral artery occlusion reached conclusions similar to those for basilar artery occlusion. Patients with moderate to severe stroke symptoms with NIHSS scores of 10 or greater have better functional outcomes after EVT within 12 hours of symptom onset. The benefits for milder strokes are uncertain.[34] For cases of basilar artery occlusion, EVT is often considered beyond the typical 6-hour time window, and even delayed reperfusion therapy is deemed feasible for these infarcts. Brain imaging revealing a substantial mismatch between the brain infarct volume and the area of decreased perfusion or a high degree of collateral circulation might prompt a more urgent thrombectomy.(A1)
The Trial of Endovascular Treatment of Acute Basilar-Artery Occlusion (ATTENTION) and the Basilar Artery Occlusion Chinese Endovascular Trial (BAOCHE) trials, published in 2022, showed better functional outcomes with EVT within 12 to 24 hours after strokes caused by basilar artery occlusion.[35][36] The improved functional outcomes of EVT are also sustained at 3-year follow-up.[37] Notably, intravenous tenecteplase followed by endovascular thrombectomy did not improve functional outcomes in patients with basilar artery occlusion compared with EVT alone, according to the phase 3 ATTENTION-LATE study. Conversely, strokes caused by medium and small vessel occlusions, such as occlusion of the P2 (anterior medullary), P3 (lateral medullary), posterior inferior cerebellar artery, and superior cerebellar artery, are not improved by EVT within 12 hours, as shown in the results from the Endovascular Treatment to Improve Outcomes for Medium Vessel Occlusions (ESCAPE-MeVO) trial.[38] When reperfusion is not possible, aspirin therapy, with or without another antiplatelet agent such as clopidogrel, is indicated. Anticoagulation therapy may also be considered in patients with embolic events.(A1)
Factor XI Inhibitors
Factor XI inhibitors are a new class of medications with promising future use as antithrombotic agents. Factor XI plays only a minor role in hemostasis, yet it limits thrombus extension. Factor XI inhibition reduces thrombotic events and complications without significant bleeding risk. Results from recent studies showed that factor XI inhibition is also safe.[39] Factor XI inhibitors may be most useful for patients with acute ischemic stroke due to embolic stroke of unknown source and patients without any obvious cardioembolic source.
Head Positioning
Overall, in patients with acute ischemic stroke, 0° head positioning provides no benefit more than 30°. Even in patients with large-artery occlusion who are not candidates for reperfusion therapy, Trendelenburg positioning (-20°) does not improve functional outcomes compared with 0° to 30°. However, in patients with large-vessel occlusion stroke before thrombectomy, a 0° head position improves functional outcome compared with 30° while awaiting definitive reperfusion therapy.[40](A1)
Blood Pressure Management
Guidelines recommend maintaining blood pressure below 180/105 mm Hg for the first 24 hours following intravenous alteplase administration.[19] In patients with blood pressure 220/120 mm Hg or greater who did not receive intravascular thrombolysis or EVT, the benefit of hypertension treatment within the first 48 to 72 hours is uncertain. In patients with blood pressure less than 220/120 mm Hg who did not receive intravascular thrombolysis or EVT, treatment of hypertension within the first 48 to 72 hours does not improve outcomes.[41] The 2023 American Heart Association guidelines recommend maintaining blood pressure at or below 185/110 mm Hg before the procedure in patients scheduled for mechanical thrombectomy who have not received intravascular thrombolysis.[19] Findings from several new trials assessed the efficacy and safety of blood pressure lowering after intravascular thrombolysis or EVT. More intensive blood pressure lowering does not improve functional outcomes after thrombolysis and may result in harm after EVT. Therefore, intensive blood pressure lowering to a systolic blood pressure of less than 140 mm Hg is not recommended.[42][43](A1)
Acute treatment of LMS also includes the following:
- Intensive care unit monitoring should be used for patients with respiratory failure and increased intracranial pressure.[13] Signs of increased intracranial pressure may include disorientation, lethargy, headache, and vomiting. Late signs include bradycardia, hypertension with widened pulse pressure, or an irregular respiratory pattern (Cushing triad). Treatment includes head elevation to 30°, blood pressure treatment to maintain cerebral perfusion, targeted hyperventilation, neurosurgical consultation, and occasionally osmotic agents, such as 3% saline or mannitol.[44]
- Extracranial vertebral artery stenting may be beneficial during endovascular therapy for tandem posterior circulation lesions. Results from a 2025 registry analysis demonstrated improved 1-year functional outcomes with this intervention.[45]
- Secondary stroke prevention can be achieved with antiplatelets, antihypertensives, and statins.[11]
- An enteral nutrition evaluation with nasogastric or gastrostomy feeding is useful if severe dysphagia persists.
- Dysphagia management can be achieved with postural and dietary modifications, swallowing exercises, or botulinum toxin for trismus.[1][3] Persistent dysphagia mandates early swallow assessment, enteral support, and goal-directed therapy with long-term rehabilitation.[46]
- Low-molecular-weight heparin prophylaxis is useful for preventing deep vein thrombosis.
- Speech-language therapy can be effective for dysphagia.
- Gabapentin is useful for persistent hiccups or chronic facial pain.[2]
- Managing autonomic complications is essential; cardiac pacing can help with acute heart failure due to bradycardia.[47]
- An ophthalmology evaluation can be useful for neurotrophic keratopathy.[14]
- Regular evaluation of speech and motor function is essential.[10] (B2)
Differential Diagnosis
Depending on the predominant symptoms, the differential diagnosis of LMS varies. The most common presentation is dizziness and vertigo with nausea and vomiting. The most important differential diagnosis is acute peripheral vestibulopathy (acute vestibular neuritis). A careful evaluation should differentiate the 2 using the Head Impulse, Nystagmus, Test of Skew (HINTS) test. The head impulse test results are negative in LMS but positive in cases of peripheral vestibulopathy. Nystagmus is unilateral and beats away from the side of the lesion with vestibulopathy, but is bilateral or vertical in LMS. Skew deviation is present in LMS but absent in peripheral vestibulopathy. The HINTS test may identify patients at risk of stroke who require MRI and hospitalization.[48] Additionally, hemorrhagic stroke is a much less common differential diagnosis, and headache is a prominent symptom. Acute demyelination, as in multiple sclerosis, may present with medullary symptoms, but the patients are generally younger women with a history of a demyelinating disease.[4]
Other differential diagnoses include:
- Headache, including migraine or cluster
- Intracerebral hemorrhage
- Brainstem or cerebellar tumor, including primary and secondary malignant neoplasms
- Psychiatric conversion disorders
- Reversible cerebral vasoconstriction syndrome [11]
- Vasculitis of the large and medium vessels, such as giant cell arteritis
- Vertebral artery dissection
Prognosis
LMS has a generally favorable prognosis. Significant functional recovery is common, including improvement of dysphagia.[1][8]
Complications
Complications of LMS can include the following:
- Respiratory complications may include aspiration pneumonia, respiratory failure, and central hypoventilation syndrome (eg, Ondine curse). Respiratory failure due to autonomic dysfunction can be observed rarely and causes apnea and death.
- Syndrome of inappropriate antidiuretic hormone secretion can be a complication, although this condition is rare in LMS compared with other types of stroke.
- Neurotrophic keratopathy, including corneal damage and infection, is a potential complication.[14][49]
- Severe dysphagia may occur in lateral medullary syndrome due to involvement of the nucleus ambiguus, which innervates muscles responsible for swallowing.
- Trigeminal neuralgia can result from disruption of the spinal trigeminal nucleus and tract, leading to facial pain and sensory disturbances.
- Cardiac complications are rare and may occur when the nucleus tractus solitarius, which is involved in cardiovascular regulation, is affected.[47]
- Obstructive hydrocephalus may develop as a rare complication of lateral medullary syndrome due to brainstem edema or infarct-related compression of cerebrospinal fluid pathways, such as the fourth ventricle.
Deterrence and Patient Education
Patients with lateral medullary syndrome require early initiation of physical and occupational therapy to support recovery of strength, mobility, and functional independence. Secondary stroke prevention strategies, including risk factor modification and antithrombotic therapy, should be discussed to optimize long-term outcomes. Patients with dysphagia should undergo formal swallowing rehabilitation. In cases of severe dysphagia, placement of a gastrostomy tube may be necessary to maintain adequate nutrition. Regular follow-up with a speech-language pathologist is recommended to monitor progress and adjust therapeutic interventions accordingly.
Pearls and Other Issues
Pearls regarding LMS include:
- A physical examination, including the HINTS test, is the most crucial clinical examination to differentiate between vestibular neuritis and stroke in patients with an acute onset of vertigo.
- Loss of pain and temperature sensation on the ipsilateral face and the contralateral side of the body, arm, and leg is most diagnostic of an acute LMS.
- Weakness is uncommon in LMS.
- The prognosis for patients with LMS depends on the size of the infarct; however, most patients generally have a better outcome than patients with other ischemic stroke syndromes, except for some lacunar syndromes.
- Gait instability or ataxia is the most typical sequela.
- Intractable hiccups may occur.[4]
Enhancing Healthcare Team Outcomes
Optimal outcomes in managing LMS require a collaborative, interprofessional approach. Emergency clinicians and hospitalists play a crucial role in the early recognition and stabilization of patients presenting with symptoms suggestive of brainstem infarction. Neurologists confirm the diagnoses, guide acute management, and coordinate appropriate imaging and interventions. Nurses provide continuous monitoring and patient education, while physical and occupational therapists help address balance, coordination, and activities of daily living to maximize functional recovery.
Speech-language pathologists play an integral role in assessing and treating dysphagia and communication difficulties, which are common in patients with lateral medullary syndrome. Registered dietitians ensure nutritional needs are safely met, especially when swallowing is impaired. Social workers support patients and families by addressing psychosocial needs, arranging resources, and facilitating discharge planning. Stroke prevention, supportive care, and caregiver education are crucial in reducing the risk of recurrent events and optimizing long-term outcomes. Ongoing follow-up and rehabilitation are vital to promote patient safety, independence, and quality of life.
Media
(Click Image to Enlarge)
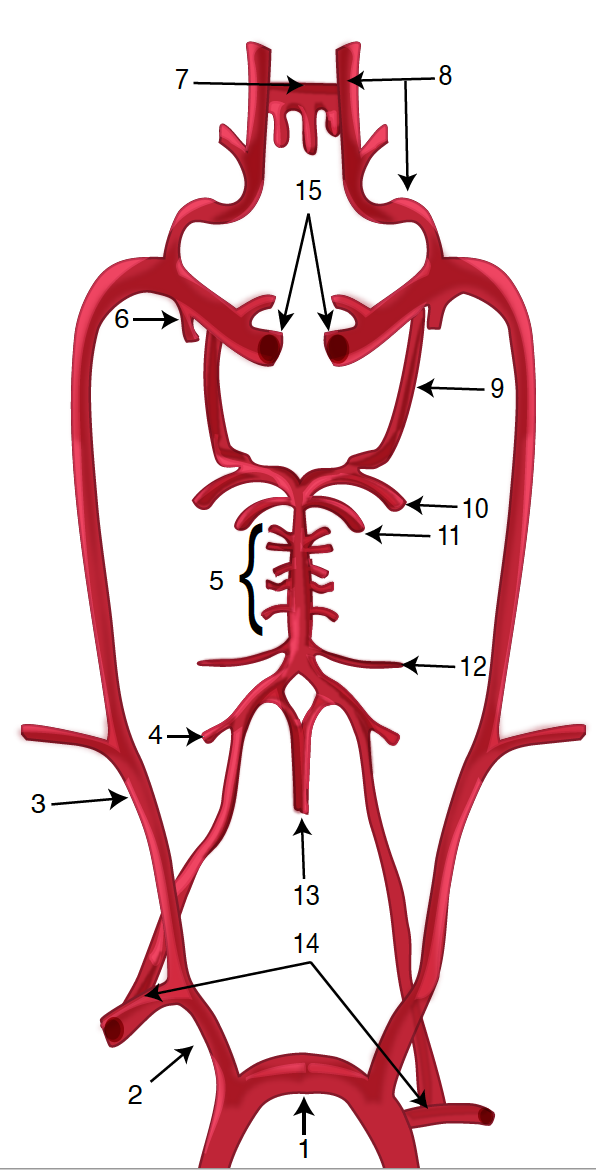
Diagram of the Brain Blood Circulation. Each number corresponds to the following neuroanatomy: 1) aortic arch; 2) brachiocephalic artery; 3) common carotid artery; 4) posterior inferior cerebellar artery; 5) pontine arteries; 6) anterior choroidal artery; 7) anterior communicating artery; 8) anterior cerebral artery; 9) posterior communicating artery; 10) posterior cerebral artery; 11) superior cerebellar artery; 12) anterior inferior cerebellar artery; 13) anterior spinal artery; 14) arches of vertebral arteries; and 15) internal carotid arteries.
Contributed by O Kuybu, MD
(Click Image to Enlarge)
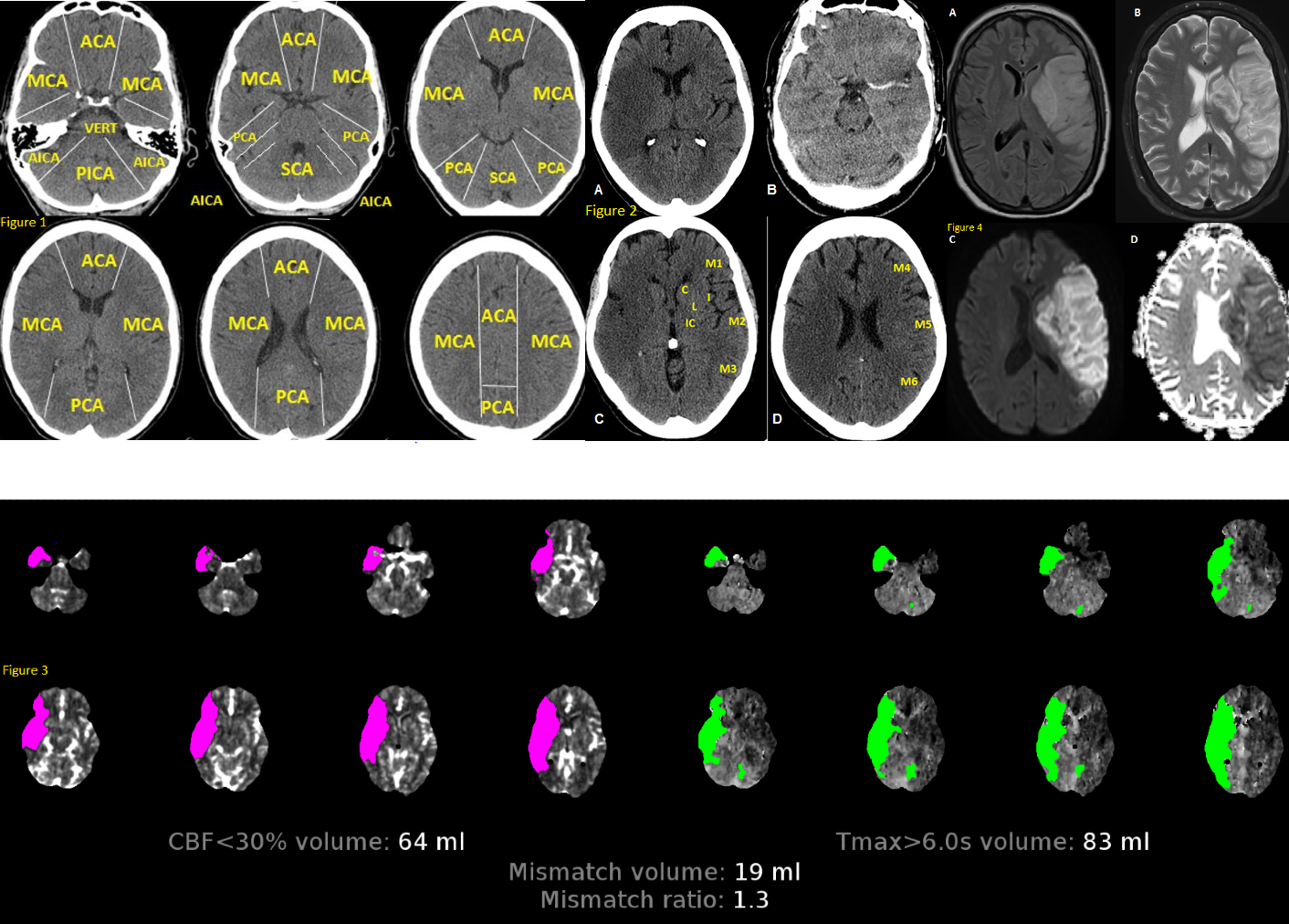
Anatomy of Brain Vascular Territories. Figure 1: ACA (anterior cerebral artery), MCA (middle cerebral artery), PCA (posterior cerebral artery), AICA (anterior inferior cerebellar artery), PICA (posterior inferior cerebellar artery), and SCA (superior cerebellar artery). Figure 2: Noncontrast CT shows loss of gray-white matter differentiation in the right MCA territory, consistent with acute large right MCA infarction. Figure 3: CT perfusion imaging reveals stroke; areas with increased mean transit time and time-to-peak/time-to-maximum, along with decreased cerebral blood volume and cerebral blood flow, indicate infarct core. Figure 4: MRI shows large left MCA infarction. It appears hyperintense on FLAIR (A) and T2 (B), with mass effect suggesting subacute infarction. Diffusion restriction is confirmed by hyperintensity on DWI (C) and hypointensity on ADC map (D).
Contributed by O Shafaat, MD
(Click Image to Enlarge)
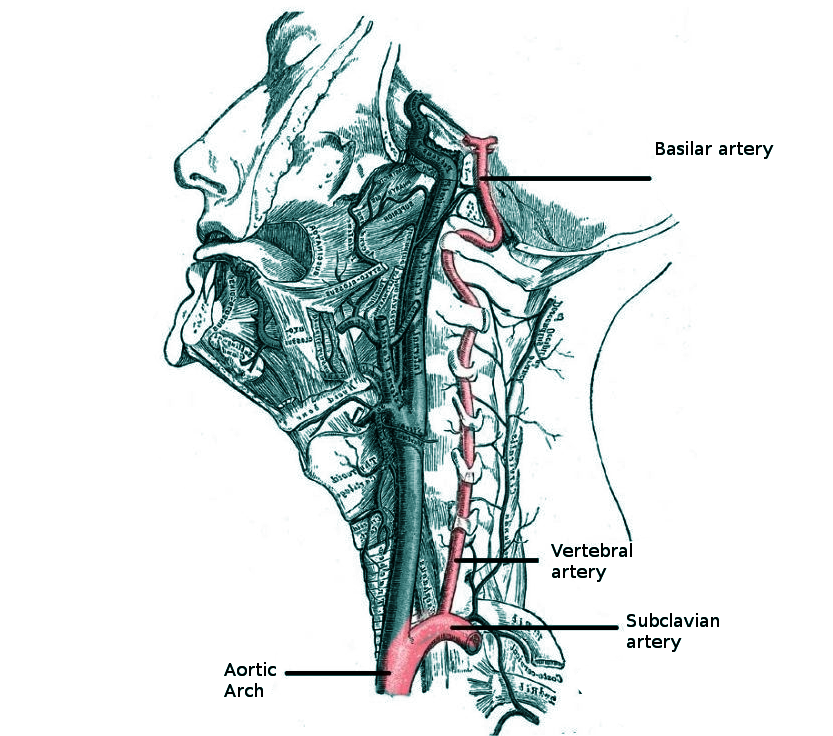
Vertebral Artery Anatomy in the Neck Region. This illustration shows the vertebral artery's course in the neck and relationships to the subclavian artery, aortic arch, cervical vertebrae, and basilar artery.
Contributed by O Chaigasame, MD
(Click Image to Enlarge)
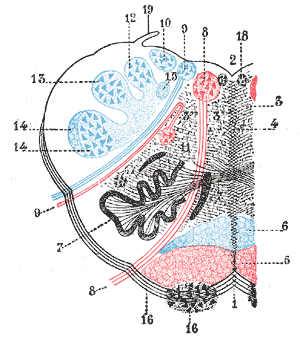
Lateral Medullary Syndrome. This syndrome, also known as Wallenberg syndrome, is a neurological disorder affecting the dorsolateral medulla oblongata, most commonly caused by ischemic infarction of the posterior inferior cerebellar artery or the vertebral artery.
1. Anterior median fissure. 2. Fourth ventricle. 3. Formatio reticularis. 4. Raphe. 5. Pyramid. 6. Lemniscus. 7. Inferior olivary nucleus with the two accessory olivary nuclei. 8. Hypoglossal nerve. 10. Lateral dorsal acoustic nucleus. 11. Nucleus ambiguus. 12. Gracile nucleus. 13. Cuneate nucleus. 14. Head of posterior column. 15. Fasciculus solitarius. 16. Anterior external arcuate fibers. 17. Nucleus lateralis 18. Nucleus of fasciculus teres. 19. Ligula.
Henry Van Dyke Carter, Public Domain, via Wikimedia Commons
{kind=link}
(Click Image to Enlarge)
Blood Supply to Medulla. The medulla oblongata receives blood from several key arteries, primarily branches of the vertebral and basilar arteries, part of the posterior circulation.
Contributed by S Bhimji, MD
References
Kim H, Lee HJ, Park JW. Clinical course and outcome in patients with severe dysphagia after lateral medullary syndrome. Therapeutic advances in neurological disorders. 2018:11():1756286418759864. doi: 10.1177/1756286418759864. Epub 2018 Feb 28 [PubMed PMID: 29511384]
Level 3 (low-level) evidenceSampath V, Gowda MR, Vinay HR, Preethi S. Persistent hiccups (singultus) as the presenting symptom of lateral medullary syndrome. Indian journal of psychological medicine. 2014 Jul:36(3):341-3. doi: 10.4103/0253-7176.135397. Epub [PubMed PMID: 25035568]
Level 3 (low-level) evidenceBattel I, Koch I, Biddau F, Carollo C, Piccione F, Meneghello F, Merico A, Palmer K, Marchese Ragona R. Efficacy of botulinum toxin type-A and swallowing treatment for oropharyngeal dysphagia recovery in a patient with lateral medullary syndrome. European journal of physical and rehabilitation medicine. 2017 Oct:53(5):798-801. doi: 10.23736/S1973-9087.17.04499-9. Epub 2017 Mar 6 [PubMed PMID: 28264544]
Lui F, Tadi P, Anilkumar AC. Wallenberg Syndrome(Archived). StatPearls. 2026 Jan:(): [PubMed PMID: 29262144]
Thapliyal K, Garg A, Singh VP. Lateral medullary syndrome: Case report and review of literature. Journal of family medicine and primary care. 2022 Nov:11(11):7438-7441. doi: 10.4103/jfmpc.jfmpc_667_22. Epub 2022 Dec 16 [PubMed PMID: 36993088]
Level 3 (low-level) evidenceShrestha S, Maharjan S, Ghimire B, Mainali N, Gurung K, Yadav HR, Bhandari K, Shrestha S, Halder A, Rajak K, Jaiswal V. Lateral medullary syndrome resulting from atrial fibrillation due to rheumatic heart disease: A case report and literature review. Clinical case reports. 2024 Jul:12(7):e9124. doi: 10.1002/ccr3.9124. Epub 2024 Jun 28 [PubMed PMID: 38947544]
Level 3 (low-level) evidenceGiannopoulos S, Markoula S, Kosmidou M, Pelidou SH, Kyritsis AP. Lateral medullary ischaemic events in young adults with hypoplastic vertebral artery. Journal of neurology, neurosurgery, and psychiatry. 2007 Sep:78(9):987-9 [PubMed PMID: 17702781]
Level 3 (low-level) evidenceKim JS. Pure lateral medullary infarction: clinical-radiological correlation of 130 acute, consecutive patients. Brain : a journal of neurology. 2003 Aug:126(Pt 8):1864-72 [PubMed PMID: 12805095]
Level 2 (mid-level) evidenceMiao HL, Zhang DY, Wang T, Jiao XT, Jiao LQ. Clinical Importance of the Posterior Inferior Cerebellar Artery: A Review of the Literature. International journal of medical sciences. 2020:17(18):3005-3019. doi: 10.7150/ijms.49137. Epub 2020 Oct 18 [PubMed PMID: 33173421]
Shetty SR, Anusha R, Thomas PS, Babu SG. Wallenberg's syndrome. Journal of neurosciences in rural practice. 2012 Jan:3(1):100-2. doi: 10.4103/0976-3147.91980. Epub [PubMed PMID: 22346215]
Nouh A, Remke J, Ruland S. Ischemic posterior circulation stroke: a review of anatomy, clinical presentations, diagnosis, and current management. Frontiers in neurology. 2014:5():30. doi: 10.3389/fneur.2014.00030. Epub 2014 Apr 7 [PubMed PMID: 24778625]
Imam YZ, Chandra P, Singh R, Hakeem I, Al Sirhan S, Kotob M, Akhtar N, Kamran S, Al Jerdi S, Muhammad A, Haroon KH, Hussain S, Perkins JD, Elalamy O, Alhatou M, Ali L, Abdelmoneim MS, Joseph S, Morgan D, Uy RT, Bhutta Z, Azad A, Ayyad A, Elsotouhy A, Own A, Deleu D. Incidence, clinical features, and outcomes of posterior circulation ischemic stroke: insights from a large multiethnic stroke database. Frontiers in neurology. 2024:15():1302298. doi: 10.3389/fneur.2024.1302298. Epub 2024 Feb 7 [PubMed PMID: 38385041]
Aynaci O, Gok F, Yosunkaya A. Management of a patient with Opalski's syndrome in intensive care unit. Clinical case reports. 2017 Sep:5(9):1518-1522. doi: 10.1002/ccr3.1111. Epub 2017 Jul 30 [PubMed PMID: 28878917]
Level 3 (low-level) evidenceCidad P, Boto A, Del Hierro A, Capote M, Noval S, Garcia A, Santiago S. Unilateral punctate keratitis secondary to Wallenberg Syndrome. Korean journal of ophthalmology : KJO. 2014 Jun:28(3):278-83. doi: 10.3341/kjo.2014.28.3.278. Epub 2014 May 19 [PubMed PMID: 24882965]
Level 3 (low-level) evidenceHe Z, Xie M, Xie C, An D, Dai M, Wen H, Shan Y. Characteristics of Dysphagia in Medullary and Cerebellar Stroke: An Observational Study Based on HRPM and FEES. Archives of physical medicine and rehabilitation. 2026 Feb:107(2):225-234. doi: 10.1016/j.apmr.2025.05.003. Epub 2025 May 20 [PubMed PMID: 40403865]
Level 2 (mid-level) evidenceKim JM, Park KY, Kim DH, Bae JH, Shin DW, Youn YC, Kwon OS. Symptomatic hyponatremia following lateral medullary infarction: a case report. BMC neurology. 2014 May 22:14():111. doi: 10.1186/1471-2377-14-111. Epub 2014 May 22 [PubMed PMID: 24886592]
Level 3 (low-level) evidenceAgarwal A, Agrawal P, Suri K, Theengh DP, Kaushal H. Ipsilateral Hemiparesis in Lateral Medullary Syndrome: A Case Report on Opalski's Syndrome. Cureus. 2024 Dec:16(12):e76105. doi: 10.7759/cureus.76105. Epub 2024 Dec 20 [PubMed PMID: 39834955]
Level 3 (low-level) evidenceSun B, Jin Y, Ye Z, Xu H, Luo W, Liu S. Vertebral artery dissection induced lateral medullary syndrome characterized with severe bradycardia: a case report and review of the literature. Annals of palliative medicine. 2022 Oct:11(10):3330-3336. doi: 10.21037/apm-22-1098. Epub [PubMed PMID: 36367000]
Level 3 (low-level) evidencePowers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, Biller J, Brown M, Demaerschalk BM, Hoh B, Jauch EC, Kidwell CS, Leslie-Mazwi TM, Ovbiagele B, Scott PA, Sheth KN, Southerland AM, Summers DV, Tirschwell DL. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2019 Dec:50(12):e344-e418. doi: 10.1161/STR.0000000000000211. Epub 2019 Oct 30 [PubMed PMID: 31662037]
Boggs KM, Vogel BT, Zachrison KS, Espinola JA, Faridi MK, Cash RE, Sullivan AF, Camargo CA Jr. An inventory of stroke centers in the United States. Journal of the American College of Emergency Physicians open. 2022 Apr:3(2):e12673. doi: 10.1002/emp2.12673. Epub 2022 Feb 28 [PubMed PMID: 35252972]
Ahmed HK, Mathisen SM, Kurz K, Dalen I, Logallo N, Thomassen L, Kurz M. Thrombolysis in wake-up stroke based on MRI mismatch. Journal of the neurological sciences. 2024 Nov 15:466():123265. doi: 10.1016/j.jns.2024.123265. Epub 2024 Oct 4 [PubMed PMID: 39378794]
Baik SH, Kim JY, Jung C. A Review of Endovascular Treatment for Posterior Circulation Strokes. Neurointervention. 2023 Jun:18(2):90-106. doi: 10.5469/neuroint.2023.00213. Epub 2023 Jun 27 [PubMed PMID: 37365755]
Kvistad CE, Næss H, Helleberg BH, Idicula T, Hagberg G, Nordby LM, Jenssen KN, Tobro H, Rörholt DM, Kaur K, Eltoft A, Evensen K, Haasz J, Singaravel G, Fromm A, Thomassen L. Tenecteplase versus alteplase for the management of acute ischaemic stroke in Norway (NOR-TEST 2, part A): a phase 3, randomised, open-label, blinded endpoint, non-inferiority trial. The Lancet. Neurology. 2022 Jun:21(6):511-519. doi: 10.1016/S1474-4422(22)00124-7. Epub 2022 May 4 [PubMed PMID: 35525250]
Level 1 (high-level) evidenceRehman AU, Mohsin A, Cheema HA, Zahid A, Ebaad Ur Rehman M, Ameer MZ, Ayyan M, Ehsan M, Shahid A, Aemaz Ur Rehman M, Shah J, Khawaja A. Comparative efficacy and safety of tenecteplase and alteplase in acute ischemic stroke: A pairwise and network meta-analysis of randomized controlled trials. Journal of the neurological sciences. 2023 Feb 15:445():120537. doi: 10.1016/j.jns.2022.120537. Epub 2022 Dec 29 [PubMed PMID: 36630803]
Level 1 (high-level) evidenceBala F, Singh N, Buck B, Ademola A, Coutts SB, Deschaintre Y, Khosravani H, Appireddy R, Moreau F, Phillips S, Gubitz G, Tkach A, Catanese L, Dowlatshahi D, Medvedev G, Mandzia J, Pikula A, Shankar JJ, Williams H, Field TS, Manosalva Alzate A, Siddiqui M, Zafar A, Imoukhoude O, Hunter G, Alhabli I, Benali F, Horn M, Hill MD, Shamy M, Sajobi TT, Swartz RH, Menon BK, Almekhlafi M. Safety and Efficacy of Tenecteplase Compared With Alteplase in Patients With Large Vessel Occlusion Stroke: A Prespecified Secondary Analysis of the ACT Randomized Clinical Trial. JAMA neurology. 2023 Aug 1:80(8):824-832. doi: 10.1001/jamaneurol.2023.2094. Epub [PubMed PMID: 37428494]
Level 1 (high-level) evidenceRodriguez M, Sidebottom C, Wells DA, Dhasakeerthi T, Hayes L, Elangovan C, Krishnaiah B. A Systematic Review of the Efficacy and Safety of Tenecteplase Versus Alteplase in Acute Ischemic Stroke: A Time to Pass the Torch. Stroke (Hoboken, N.J.). 2024 Jul:4(4):e001110. doi: 10.1161/SVIN.123.001110. Epub 2024 Apr 26 [PubMed PMID: 41585398]
Level 1 (high-level) evidencePrabhakaran S, Gonzalez NR, Zachrison KS, Adeoye O, Alexandrov AW, Ansari SA, Chapman S, Czap AL, Dumitrascu OM, Ishida K, Jadhav AP, Johnson B, Johnston KC, Khatri P, Kimberly WT, Lee VH, Leslie-Mazwi TM, Mac Grory B, Madsen TE, Menon B, Mistry EA, Park S, Parker S, Pérez de la Ossa N, Reeves M, Saiz T, Scott PA, Schwartzberg D, Sheth SA, Sporns PB, Times S, Tjoumakaris S, Wolfe SQ, Yaghi S, Peer Review Committee. 2026 Guideline for the Early Management of Patients With Acute Ischemic Stroke: A Guideline From the American Heart Association/American Stroke Association. Stroke. 2026 Jan 26:():. doi: 10.1161/STR.0000000000000513. Epub 2026 Jan 26 [PubMed PMID: 41582814]
Thomalla G, Simonsen CZ, Boutitie F, Andersen G, Berthezene Y, Cheng B, Cheripelli B, Cho TH, Fazekas F, Fiehler J, Ford I, Galinovic I, Gellissen S, Golsari A, Gregori J, Günther M, Guibernau J, Häusler KG, Hennerici M, Kemmling A, Marstrand J, Modrau B, Neeb L, Perez de la Ossa N, Puig J, Ringleb P, Roy P, Scheel E, Schonewille W, Serena J, Sunaert S, Villringer K, Wouters A, Thijs V, Ebinger M, Endres M, Fiebach JB, Lemmens R, Muir KW, Nighoghossian N, Pedraza S, Gerloff C, WAKE-UP Investigators. MRI-Guided Thrombolysis for Stroke with Unknown Time of Onset. The New England journal of medicine. 2018 Aug 16:379(7):611-622. doi: 10.1056/NEJMoa1804355. Epub 2018 May 16 [PubMed PMID: 29766770]
Zhang J, Ta N, Fu M, Tian FH, Wang J, Zhang T, Wang B. Use of DWI-FLAIR Mismatch to Estimate the Onset Time in Wake-Up Strokes. Neuropsychiatric disease and treatment. 2022:18():355-361. doi: 10.2147/NDT.S351943. Epub 2022 Feb 21 [PubMed PMID: 35228801]
Ma H, Campbell BCV, Parsons MW, Churilov L, Levi CR, Hsu C, Kleinig TJ, Wijeratne T, Curtze S, Dewey HM, Miteff F, Tsai CH, Lee JT, Phan TG, Mahant N, Sun MC, Krause M, Sturm J, Grimley R, Chen CH, Hu CJ, Wong AA, Field D, Sun Y, Barber PA, Sabet A, Jannes J, Jeng JS, Clissold B, Markus R, Lin CH, Lien LM, Bladin CF, Christensen S, Yassi N, Sharma G, Bivard A, Desmond PM, Yan B, Mitchell PJ, Thijs V, Carey L, Meretoja A, Davis SM, Donnan GA, EXTEND Investigators. Thrombolysis Guided by Perfusion Imaging up to 9 Hours after Onset of Stroke. The New England journal of medicine. 2019 May 9:380(19):1795-1803. doi: 10.1056/NEJMoa1813046. Epub [PubMed PMID: 31067369]
Campbell BCV, Ma H, Ringleb PA, Parsons MW, Churilov L, Bendszus M, Levi CR, Hsu C, Kleinig TJ, Fatar M, Leys D, Molina C, Wijeratne T, Curtze S, Dewey HM, Barber PA, Butcher KS, De Silva DA, Bladin CF, Yassi N, Pfaff JAR, Sharma G, Bivard A, Desmond PM, Schwab S, Schellinger PD, Yan B, Mitchell PJ, Serena J, Toni D, Thijs V, Hacke W, Davis SM, Donnan GA, EXTEND, ECASS-4, and EPITHET Investigators. Extending thrombolysis to 4·5-9 h and wake-up stroke using perfusion imaging: a systematic review and meta-analysis of individual patient data. Lancet (London, England). 2019 Jul 13:394(10193):139-147. doi: 10.1016/S0140-6736(19)31053-0. Epub 2019 May 22 [PubMed PMID: 31128925]
Level 1 (high-level) evidenceChen HS, Cui Y, Zhou ZH, Zhang H, Wang LX, Wang WZ, Shen LY, Guo LY, Wang EQ, Wang RX, Han J, Dong YL, Li J, Lin YZ, Yang QC, Zhang L, Li JY, Wang J, Xia L, Ma GB, Lu J, Jiang CH, Huang SM, Wan LS, Piao XY, Li Z, Li YS, Yang KH, Wang DL, Nguyen TN, ARAMIS Investigators. Dual Antiplatelet Therapy vs Alteplase for Patients With Minor Nondisabling Acute Ischemic Stroke: The ARAMIS Randomized Clinical Trial. JAMA. 2023 Jun 27:329(24):2135-2144. doi: 10.1001/jama.2023.7827. Epub [PubMed PMID: 37367978]
Level 1 (high-level) evidenceCoutts SB, Ankolekar S, Appireddy R, Arenillas JF, Assis Z, Bailey P, Barber PA, Bazan R, Buck BH, Butcher KS, Camden MC, Campbell BCV, Casaubon LK, Catanese L, Chatterjee K, Choi PMC, Clarke B, Dowlatshahi D, Ferrari J, Field TS, Ganesh A, Ghia D, Goyal M, Greisenegger S, Halse O, Horn M, Hunter G, Imoukhuede O, Kelly PJ, Kennedy J, Kenney C, Kleinig TJ, Krishnan K, Lima F, Mandzia JL, Marko M, Martins SO, Medvedev G, Menon BK, Mishra SM, Molina C, Moussaddy A, Muir KW, Parsons MW, Penn AMW, Pille A, Pontes-Neto OM, Roffe C, Serena J, Simister R, Singh N, Spratt N, Strbian D, Tham CH, Wiggam MI, Williams DJ, Willmot MR, Wu T, Yu AYX, Zachariah G, Zafar A, Zerna C, Hill MD, TEMPO-2 investigators. Tenecteplase versus standard of care for minor ischaemic stroke with proven occlusion (TEMPO-2): a randomised, open label, phase 3 superiority trial. Lancet (London, England). 2024 Jun 15:403(10444):2597-2605. doi: 10.1016/S0140-6736(24)00921-8. Epub 2024 May 17 [PubMed PMID: 38768626]
Level 1 (high-level) evidenceNogueira RG, Jovin TG, Liu X, Hu W, Langezaal LCM, Li C, Dai Q, Tao C, Mont'Alverne FJA, Ji X, Liu R, Li R, Dippel DWJ, Wu C, Zhu W, Xu P, van Zwam WH, Wu L, Zhang C, Michel P, Chen J, Wang L, Puetz V, Zhao W, Liu T, Audebert HJ, Chen Z, Pontes-Neto OM, Yi T, Moran TP, Doheim MF, Schonewille WJ, ATTENTION, BASICS, BAOCHE, and BEST Investigators. Endovascular therapy for acute vertebrobasilar occlusion (VERITAS): a systematic review and individual patient data meta-analysis. Lancet (London, England). 2025 Jan 4:405(10472):61-69. doi: 10.1016/S0140-6736(24)01820-8. Epub 2024 Dec 12 [PubMed PMID: 39674187]
Tao C, Nogueira RG, Zhu Y, Sun J, Han H, Yuan G, Wen C, Zhou P, Chen W, Zeng G, Li Y, Ma Z, Yu C, Su J, Zhou Z, Chen Z, Liao G, Sun Y, Ren Y, Zhang H, Chen J, Yue X, Xiao G, Wang L, Liu R, Liu W, Liu Y, Wang L, Zhang C, Liu T, Song J, Li R, Xu P, Yin Y, Wang G, Baxter B, Qureshi AI, Liu X, Hu W, ATTENTION Investigators. Trial of Endovascular Treatment of Acute Basilar-Artery Occlusion. The New England journal of medicine. 2022 Oct 13:387(15):1361-1372. doi: 10.1056/NEJMoa2206317. Epub [PubMed PMID: 36239644]
Jovin TG, Li C, Wu L, Wu C, Chen J, Jiang C, Shi Z, Gao Z, Song C, Chen W, Peng Y, Yao C, Wei M, Li T, Wei L, Xiao G, Yang H, Ren M, Duan J, Liu X, Yang Q, Liu Y, Zhu Q, Shi W, Zhu Q, Li X, Guo Z, Yang Q, Hou C, Zhao W, Ma Q, Zhang Y, Jiao L, Zhang H, Liebeskind DS, Liang H, Jadhav AP, Wen C, Brown S, Zhu L, Ye H, Ribo M, Chang M, Song H, Chen J, Ji X, BAOCHE Investigators. Trial of Thrombectomy 6 to 24 Hours after Stroke Due to Basilar-Artery Occlusion. The New England journal of medicine. 2022 Oct 13:387(15):1373-1384. doi: 10.1056/NEJMoa2207576. Epub [PubMed PMID: 36239645]
Hu W, Tao C, Li R, Chen Z, Chen W, Yi T, Wang H, Zhou P, Cao Z, Zeng G, Cui T, Su J, Chen L, Wang G, Sun J, Zhu Y, Wang L, Zhang C, Liu T, Song J, Jing X, Wang A, Wang J, Xu P, Luo C, Qureshi AI, AbdalKader M, Nguyen TN, Saver JL, Nogueira RG, Liu X. Endovascular vs Medical Treatment of Basilar Artery Occlusion: 3-Year Outcomes of the ATTENTION Randomized Clinical Trial. JAMA neurology. 2026 Feb 1:83(2):107-114. doi: 10.1001/jamaneurol.2025.5077. Epub [PubMed PMID: 41460644]
Level 1 (high-level) evidenceGoyal M, Ospel JM, Ganesh A, Dowlatshahi D, Volders D, Möhlenbruch MA, Jumaa MA, Nimjee SM, Booth TC, Buck BH, Kennedy J, Shankar JJ, Dorn F, Zhang L, Hametner C, Nardai S, Zafar A, Diprose W, Vatanpour S, Stebner A, Bosshart S, Singh N, Sebastian I, Uchida K, Ryckborst KJ, Fahed R, Hu SX, Vollherbst DF, Zaidi SF, Lee VH, Lynch J, Rempel JL, Teal R, Trivedi A, Bode FJ, Ogungbemi A, Pham M, Orosz P, Abdalkader M, Taschner C, Tarpley J, Poli S, Singh RJ, De Leacy R, Lopez G, Sahlas D, Chen M, Burns P, Schaafsma JD, Marigold R, Reich A, Amole A, Field TS, Swartz RH, Settecase F, Lenzsér G, Ortega-Gutierrez S, Asdaghi N, Lobotesis K, Siddiqui AH, Berrouschot J, Mokin M, Ebersole K, Schneider H, Yoo AJ, Mandzia J, Klostranec J, Jadun C, Patankar T, Sauvageau E, Lenthall R, Peeling L, Huynh T, Budzik R, Lee SK, Makalanda L, Levitt MR, Perry RJ, Hlaing T, Jahromi BS, Singh P, Demchuk AM, Hill MD, ESCAPE-MeVO Investigators. Endovascular Treatment of Stroke Due to Medium-Vessel Occlusion. The New England journal of medicine. 2025 Apr 10:392(14):1385-1395. doi: 10.1056/NEJMoa2411668. Epub 2025 Feb 5 [PubMed PMID: 39908448]
Level 3 (low-level) evidenceCapodanno D, Alexander JH, Bahit MC, Eikelboom JW, Gibson CM, Goodman SG, Kunadian V, Lip GYH, Lopes RD, Mehran R, Mehta SR, Patel MR, Piccini JP, Rao SV, Ruff CT, Steg PG, Weitz JI, Angiolillo DJ. Factor XI inhibitors for the prevention and treatment of venous and arterial thromboembolism. Nature reviews. Cardiology. 2025 Nov:22(11):896-912. doi: 10.1038/s41569-025-01144-z. Epub 2025 Mar 31 [PubMed PMID: 40164778]
Alexandrov AW, Shearin AJ, Mandava P, Torrealba-Acosta G, Elangovan C, Krishnaiah B, Nearing K, Robinson E, Guthrie-Chu C, Holzmann M, Fill B, Trivedi DR, Richardson A, Middleton S, Brewer BB, Liebeskind DS, Goyal N, Grotta JC, Alexandrov AV, ZODIAC Investigators. Optimal Head-of-Bed Positioning Before Thrombectomy in Large Vessel Occlusion Stroke: A Randomized Clinical Trial. JAMA neurology. 2025 Sep 1:82(9):905-914. doi: 10.1001/jamaneurol.2025.2253. Epub [PubMed PMID: 40465238]
Level 1 (high-level) evidenceLee M, Ovbiagele B, Hong KS, Wu YL, Lee JE, Rao NM, Feng W, Saver JL. Effect of Blood Pressure Lowering in Early Ischemic Stroke: Meta-Analysis. Stroke. 2015 Jul:46(7):1883-9. doi: 10.1161/STROKEAHA.115.009552. Epub 2015 May 28 [PubMed PMID: 26022636]
Level 1 (high-level) evidenceAnderson CS, Huang Y, Lindley RI, Chen X, Arima H, Chen G, Li Q, Billot L, Delcourt C, Bath PM, Broderick JP, Demchuk AM, Donnan GA, Durham AC, Lavados PM, Lee TH, Levi C, Martins SO, Olavarria VV, Pandian JD, Parsons MW, Pontes-Neto OM, Ricci S, Sato S, Sharma VK, Silva F, Song L, Thang NH, Wardlaw JM, Wang JG, Wang X, Woodward M, Chalmers J, Robinson TG, ENCHANTED Investigators and Coordinators. Intensive blood pressure reduction with intravenous thrombolysis therapy for acute ischaemic stroke (ENCHANTED): an international, randomised, open-label, blinded-endpoint, phase 3 trial. Lancet (London, England). 2019 Mar 2:393(10174):877-888. doi: 10.1016/S0140-6736(19)30038-8. Epub 2019 Feb 7 [PubMed PMID: 30739745]
Level 1 (high-level) evidenceGhozy S, Mortezaei A, Elfil M, Abdelghaffar M, Kobeissi H, Aladawi M, Abbas AS, Nayak SS, Kadirvel R, Rabinstein AA, Kallmes DF. Intensive vs Conventional Blood Pressure Control After Thrombectomy in Acute Ischemic Stroke: A Systematic Review and Meta-Analysis. JAMA network open. 2024 Feb 5:7(2):e240179. doi: 10.1001/jamanetworkopen.2024.0179. Epub 2024 Feb 5 [PubMed PMID: 38386320]
Level 1 (high-level) evidenceZhang Z, Guo Q, Wang E. Hyperventilation in neurological patients: from physiology to outcome evidence. Current opinion in anaesthesiology. 2019 Oct:32(5):568-573. doi: 10.1097/ACO.0000000000000764. Epub [PubMed PMID: 31211719]
Level 3 (low-level) evidenceLi W, Doheim MF, Qiu Z, Wang T, Chen Z, Zi W, Yang Q, Guan H, Qiao H, Liu W, Hu W, Liu X, Huang J, Han Z, Chen Z, Zhao Z, Sun W, Nogueira RG. Endovascular Treatment for Acute Posterior Circulation Tandem Lesions: Insights From the BASILAR and PERSIST Registries. Journal of stroke. 2025 Jan:27(1):75-84. doi: 10.5853/jos.2024.03055. Epub 2025 Jan 31 [PubMed PMID: 39916456]
Level 2 (mid-level) evidenceMagara J, Ita R, Tsutsui Y, Sakai H, Zhang M, Inoue M. A Case of Dysphagia Rehabilitation in a Patient in the Chronic Stage of Lateral Medullary Syndrome. Dysphagia. 2024 Jun:39(3):534-539. doi: 10.1007/s00455-024-10690-6. Epub 2024 Mar 23 [PubMed PMID: 38520512]
Level 3 (low-level) evidencevon Heinemann P, Grauer O, Schuierer G, Ritzka M, Bogdahn U, Kaiser B, Schlachetzki F. Recurrent cardiac arrest caused by lateral medulla oblongata infarction. BMJ case reports. 2009:2009():. pii: bcr02.2009.1625. doi: 10.1136/bcr.02.2009.1625. Epub 2009 Oct 12 [PubMed PMID: 21991295]
Level 3 (low-level) evidenceKrishnan K, Bassilious K, Eriksen E, Bath PM, Sprigg N, Brækken SK, Ihle-Hansen H, Horn MA, Sandset EC. Posterior circulation stroke diagnosis using HINTS in patients presenting with acute vestibular syndrome: A systematic review. European stroke journal. 2019 Sep:4(3):233-239. doi: 10.1177/2396987319843701. Epub 2019 Apr 10 [PubMed PMID: 31984230]
Level 1 (high-level) evidenceWu S, Li N, Xia F, Sidlauskas K, Lin X, Qian Y, Gao W, Zhang Q. Neurotrophic keratopathy due to dorsolateral medullary infarction (Wallenberg syndrome): case report and literature review. BMC neurology. 2014 Dec 4:14():231. doi: 10.1186/s12883-014-0231-y. Epub 2014 Dec 4 [PubMed PMID: 25472780]
Level 3 (low-level) evidence