 Anatomy, Bony Pelvis and Lower Limb: Lateral Femoral Cutaneous Nerve
Anatomy, Bony Pelvis and Lower Limb: Lateral Femoral Cutaneous Nerve
Introduction
The lateral femoral cutaneous nerve (LFCN) is a purely sensory nerve that typically arises from the dorsal divisions of the L2 and L3 ventral rami. The nerve courses through the pelvis and usually exits beneath the inguinal ligament near the anterior superior iliac spine (ASIS) before supplying cutaneous sensation to the anterolateral and lateral thigh (see Image. Superficial Vessels and Nerves of the Upper Thigh).
The principal clinical condition associated with LFCN pathology is meralgia paresthetica, a compressive mononeuropathy characterized by dysesthesia or sensory loss within the LFCN distribution. Common risk factors include obesity, diabetes mellitus, pregnancy, tight clothing, and iatrogenic injury during pelvic or hip surgery.[1] Surgical significance arises from the nerve’s highly variable anatomy and proximity to the ASIS and inguinal ligament, which place it at risk during anterior hip approaches, pelvic and abdominal procedures, iliac crest bone grafting, and regional anesthesia. Detailed knowledge of the nerve’s origin, course, branching patterns, and functional characteristics improves diagnostic accuracy, guides safe surgical dissection and nerve block techniques, and reduces the risk of iatrogenic injury.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The LFCN is a purely sensory nerve that carries afferent fibers without motor or reflex function. The nerve most commonly arises from the L2 and L3 nerve roots of the lumbar plexus. The LFCN emerges from the lateral border of the psoas major muscle and courses obliquely across the iliacus muscle within the fascia iliaca. The nerve then travels in a retroperitoneal plane toward the ASIS, remaining medial to the iliac crest. Near the ASIS, the LFCN approaches the inguinal ligament, which attaches to the ASIS and the sartorius muscle. The nerve typically passes beneath the inguinal ligament approximately 10 mm medial to the ASIS, although considerable anatomic variation exists. Less commonly, the LFCN may pass through or above the inguinal ligament or course anterior or posterior to the sartorius muscle.
Distal to the inguinal ligament, the LFCN usually divides into anterior and posterior branches. Meralgia paresthetica more commonly affects the anterior division, although both divisions may be involved.[2][3] The anterior division supplies the anterolateral thigh, extends distally toward the knee, and contributes to the peripatellar plexus through branches communicating with the femoral and saphenous nerves. The posterior division supplies the lateral thigh from the region of the greater trochanter to the midthigh.
Physiologic Variants
Variations in Origin
Anatomic variability of the LFCN is common and clinically significant. The most common origin is L2 to L3, with a reported prevalence of 27% to 68%, although the nerve may also arise from L1 to L2 or L3 to L4.[4][5] Rarely, the LFCN originates as a branch of the femoral nerve or may be absent, with sensory innervation to the anterolateral thigh supplied by the ilioinguinal, genitofemoral, or anterior femoral cutaneous nerves.
Variations Around the Inguinal Ligament and Anterior Superior Iliac Spine
Known variations in the anatomy of the LFCN include its relationship to the inguinal ligament, the ASIS, and the sartorius muscle, as well as the level of nerve division. The LFCN may exit the pelvis medial to the ASIS and pass over rather than beneath the inguinal ligament, or it may traverse through an aponeurotic opening in the ligament. Bifurcation most commonly occurs distal to the inguinal ligament, but division may also be observed at the level of the ligament or proximal to it within the pelvis. Trifurcation or quadrifurcation is less common.
Proximal division may result in individual branches passing on opposite sides of the ASIS. A branch may cross the iliac crest before reaching the ASIS, while the medial branch may pass through the inguinal ligament aponeurosis rather than crossing over the ligament.
The LFCN may course laterally to the ASIS and perforate the origin of the sartorius muscle, or it may bypass the sartorius entirely, passing through a small bony canal in the ilium just proximal to the muscle origin. The nerve may also course dorsal and caudal to the ASIS, traveling over or above the sartorius muscle, or run over the iliac crest posterior to the ASIS.
In rare cases, the LFCN may be absent, with sensory innervation to the anterolateral thigh supplied by the ilioinguinal nerve or a branch arising directly from the femoral nerve beneath the inguinal ligament. The distance between the LFCN and the ASIS is highly variable, creating a surgical “risk zone” that has been reported to range from approximately 10 mm (most common) to 46 mm medially.[6]
Variations in the Thigh
The LFCN most commonly bifurcates distal to the inguinal ligament after entering the thigh, although division may also occur at or proximal to the ligament. The nerve typically enters the thigh superficial to the sartorius muscle, with branches coursing parallel to the muscle's lateral border within the intermuscular plane between the sartorius and tensor fasciae latae muscles. Branches may also course superficial to or through these muscles. After passing the inguinal ligament, 83.4% of LFCN branches run over the surface of the sartorius, and approximately 60% traverse the middle portion of its origin. Terminal branching occurs within the intermuscular space between the sartorius and iliopsoas muscles in 91.7% of cases. Less commonly, branches course deep to the fascia of the tensor fasciae latae and perforate the iliotibial tract to supply the lateral thigh.[7][8]
Three major distal branching patterns of the LFCN have been described. Each pattern exhibits distinct sensory distributions and carries specific implications for surgical risk during anterior hip and pelvic procedures.
The sartorius type, the most common configuration, features a dominant anterior branch along the lateral border of the sartorius muscle. Sensory symptoms typically localize to the anterolateral thigh and may extend toward the knee. This branch is particularly vulnerable during anterior hip approaches that utilize the intermuscular plane between the sartorius and tensor fasciae latae.
The posterior type has a prominent posterior branch that crosses laterally toward or over the tensor fasciae latae, producing sensory symptoms that are more lateral, often over the greater trochanter. This configuration increases susceptibility to injury during lateral dissection, acetabular exposure, or retraction of the tensor fasciae latae.
The fan type consists of multiple branches spreading widely across the anterolateral thigh and carries the highest risk of iatrogenic injury. Patients often report diffuse or patchy sensory disturbances, and partial nerve injury with persistent postoperative dysesthesia is more common due to the presence of multiple vulnerable branches.[9]
Surgical Considerations
Many surgical procedures can result in iatrogenic injury of the LFCN, particularly in the presence of anatomic variants such as early bifurcation, which increase the number of nerve branches at risk. The nerve is also susceptible to injury during procedures involving the iliac crest, acetabulum, proximal femur, nerve-block anesthesia, skin transplantation, and anterolateral free flap grafting of the upper leg. Awareness of LFCN variability is critical during pelvic, abdominal, and hip procedures. Ultrasound-guided identification of the nerve can reduce the risk of iatrogenic injury during surgical interventions or regional anesthesia.[10]
A variety of surgical interventions carry specific risks for the LFCN, depending on technique and anatomy. Laparoscopic inguinal hernia repair carries a nerve injury risk of approximately 2%, particularly with variant courses. Iliac crest bone grafting carries a reduced risk when grafts are less than 3 cm in length, and incisions are greater than or equal to 3 cm from the ASIS. Abdominoplasty requires careful dissection within 4 cm of the ASIS to minimize nerve injury.
Direct anterior approach (DAA) total hip arthroplasty is associated with high rates of transient LFCN neurapraxia, reported in up to 80% of patients. Most cases resolve spontaneously, although persistent symptoms may occur.
Clinical Significance
Meralgia Paresthetica
Meralgia paresthetica is a painful compressive mononeuropathy resulting from focal entrapment of the LFCN, most commonly as it passes beneath the inguinal ligament. The condition is characterized by sensory disturbance or neuralgia affecting the anterolateral thigh, with a reported incidence of approximately 4.3 per 10,000 person-years.[11] The syndrome was first described by Bernhardt in 1878, and Roth later coined the term "meralgia paresthetica" in 1895, resulting in the eponym "Bernhardt–Roth syndrome."
Clinical presentation includes burning, tingling, itching, or aching pain, often accompanied by paresthesia or hypoesthesia over the anterolateral or lateral thigh. Symptoms are commonly exacerbated by compression near the inguinal ligament, with focal tenderness at the nerve’s point of exit. Chronic skin irritation or repeated rubbing of the affected area may result in localized hair loss.
Symptom severity is influenced by hip position, with prolonged standing or sitting in hip extension increasing discomfort due to greater tension on the LFCN. Hip flexion often provides symptomatic relief.[12] Key clinical features include purely sensory symptoms without motor weakness or muscle atrophy; preservation of the patellar reflex, which helps distinguish the condition from lumbar radiculopathy; and a peak incidence between 40 and 60 years of age.[13]
Risk factors for meralgia paresthetica include obesity, pregnancy, diabetes mellitus, and external compression from tight clothing. In patients with diabetes mellitus, the incidence is approximately 247 per 100,000 individuals, representing a 5-fold increase compared with the general population. Less commonly, proximal compression arises from a retroperitoneal hematoma or tumor. The condition has also been reported following iliac crest bone graft harvesting, femoral artery catheterization, laparoscopic appendectomy, pelvic surgery using an ilioinguinal approach, and hip or lumbar spine surgery, particularly when procedures are performed in the prone position. Perioperative positioning, including lithotomy, beach-chair, and prone positions, constitutes a recognized risk factor.[14][15]
The most common mechanism of LFCN injury is external compression or trauma near the ASIS, the nerve’s most vulnerable point. Contributing factors include tight clothing, belts, or seatbelts; carrying objects such as wallets, phones, or holsters at the waist; obesity-related pannus formation and pregnancy; repetitive hip positioning, such as external rotation in dancers; and scar formation following surgery or trauma.[16]
Direct Anterior Approach Total Hip Arthroplasty
The DAA to total hip arthroplasty is a muscle-sparing technique that utilizes true internervous planes to access the hip joint. The superficial interval lies between the sartorius muscle, innervated by the femoral nerve, and the tensor fasciae latae muscle, innervated by the superior gluteal nerve. Deeper dissection proceeds through the interval between the rectus femoris, also innervated by the femoral nerve, and the gluteus medius and minimus muscles, which are supplied by the superior gluteal nerve. This internervous design allows exposure of the hip without detachment of major muscles.
Despite its advantages, the DAA places the LFCN at risk because the nerve frequently courses near or within the superficial interval, typically medial to the tensor fasciae latae and adjacent to the ASIS. The LFCN is susceptible to traction or transection during skin incision, fascial dissection, and retractor placement. Injury most commonly presents as postoperative dysesthesia, paresthesia, or hypoesthesia over the anterolateral thigh and is usually transient, although persistent symptoms may occur.
To reduce the risk of LFCN injury, many surgeons have modified the classic approach by shifting the superficial interval laterally through the belly of the tensor fasciae latae rather than strictly between the sartorius and tensor fasciae latae. This lateralization moves the surgical corridor away from the most common course of the LFCN and has been associated with lower rates of postoperative sensory neuropathy while preserving the muscle-sparing benefits of the DAA.
Lateral Femoral Cutaneous Nerve Angiomyoma
Angiomyomas are rare, benign tumors derived from smooth muscle cells of vascular origin that may involve peripheral cutaneous nerves, including the LFCN. These tumors can present with localized pain or paresthesia and are often difficult to diagnose preoperatively due to nonspecific imaging features, placing them within a broad differential diagnosis for painful extremity nodules. Surgical excision constitutes the treatment of choice and is typically curative. Complete resection results in the resolution of symptoms, and recurrence is uncommon. Although rare, angiomyomas should be considered when evaluating unexplained painful lesions of the anterolateral thigh.[17][18]
Other Issues
Key clinical and practical considerations regarding the LFCN emphasize its purely sensory function, anatomic variability, and implications for diagnosis and procedural safety. The LFCN is purely sensory, so the presence of motor deficits suggests an alternative diagnosis. Anatomic variability is the rule rather than the exception, and persistent anterolateral thigh pain after anterior hip surgery is commonly attributable to LFCN neurapraxia. Ultrasound is increasingly valuable for both diagnosis and ensuring procedural safety.
Media
(Click Image to Enlarge)
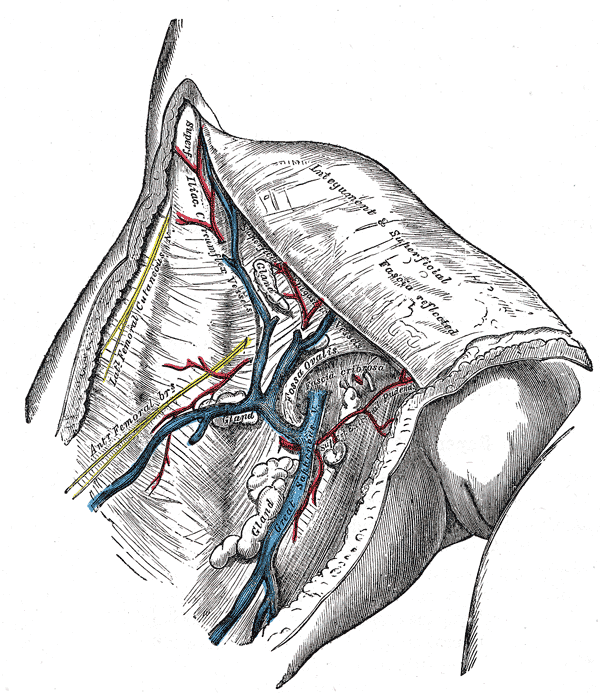
Superficial Vessels and Nerves of the Upper Thigh. This illustration displays the great saphenous vein entering the fossa ovalis through the fascia cribrosa. Labeled vessels include the superficial iliac circumflex, superficial epigastric, and superficial external pudendal arteries and veins. The lateral and anterior femoral cutaneous nerves are visible alongside reflected integument and superficial fascia. Lymphatic glands are shown clustered near the venous junctions.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Tomaszewski KA, Popieluszko P, Henry BM, Roy J, Sanna B, Kijek MR, Walocha JA. The surgical anatomy of the lateral femoral cutaneous nerve in the inguinal region: a meta-analysis. Hernia : the journal of hernias and abdominal wall surgery. 2016 Oct:20(5):649-57. doi: 10.1007/s10029-016-1493-7. Epub 2016 Apr 26 [PubMed PMID: 27115766]
Level 1 (high-level) evidenceCarai A, Fenu G, Sechi E, Crotti FM, Montella A. Anatomical variability of the lateral femoral cutaneous nerve: findings from a surgical series. Clinical anatomy (New York, N.Y.). 2009 Apr:22(3):365-70. doi: 10.1002/ca.20766. Epub [PubMed PMID: 19173255]
Level 2 (mid-level) evidenceDibenedetto LM, Lei Q, Gilroy AM, Hermey DC, Marks SC Jr, Page DW. Variations in the inferior pelvic pathway of the lateral femoral cutaneous nerve: implications for laparoscopic hernia repair. Clinical anatomy (New York, N.Y.). 1996:9(4):232-6 [PubMed PMID: 8793216]
den Brave PS, Vas Nunes SE, Bronkhorst MW. Anatomical Variations of the Lateral Femoral Cutaneous Nerve and Iatrogenic Injury After Autologous Bone Grafting From the Iliac Crest. Journal of orthopaedic trauma. 2015 Dec:29(12):549-53. doi: 10.1097/BOT.0000000000000401. Epub [PubMed PMID: 26595594]
de Ridder VA, de Lange S, Popta JV. Anatomical variations of the lateral femoral cutaneous nerve and the consequences for surgery. Journal of orthopaedic trauma. 1999 Mar-Apr:13(3):207-11 [PubMed PMID: 10206253]
Kosiyatrakul A, Nuansalee N, Luenam S, Koonchornboon T, Prachaporn S. The anatomical variation of the lateral femoral cutaneous nerve in relation to the anterior superior iliac spine and the iliac crest. Musculoskeletal surgery. 2010 May:94(1):17-20. doi: 10.1007/s12306-010-0054-y. Epub 2010 Feb 5 [PubMed PMID: 20135245]
Mangla N, Wadhwa S, Mishra S, Sural S, Vasudeva N. Cadaveric Study of Variations in the Course of Lateral Femoral Cutaneous Nerve: Insight to Prevent Injury. Medeniyet medical journal. 2023 Sep 28:38(3):172-179. doi: 10.4274/MMJ.galenos.2023.23356. Epub [PubMed PMID: 37766598]
Lee SH, Shin KJ, Gil YC, Ha TJ, Koh KS, Song WC. Anatomy of the lateral femoral cutaneous nerve relevant to clinical findings in meralgia paresthetica. Muscle & nerve. 2017 May:55(5):646-650. doi: 10.1002/mus.25382. Epub 2017 Jan 3 [PubMed PMID: 27543938]
Rudin D, Manestar M, Ullrich O, Erhardt J, Grob K. The Anatomical Course of the Lateral Femoral Cutaneous Nerve with Special Attention to the Anterior Approach to the Hip Joint. The Journal of bone and joint surgery. American volume. 2016 Apr 6:98(7):561-7. doi: 10.2106/JBJS.15.01022. Epub [PubMed PMID: 27053584]
Ozaki Y, Baba T, Homma Y, Tanabe H, Ochi H, Bannno S, Watari T, Kaneko K. Preoperative ultrasound to identify distribution of the lateral femoral cutaneous nerve in total hip arthroplasty using the direct anterior approach. SICOT-J. 2018:4():42. doi: 10.1051/sicotj/2018037. Epub 2018 Sep 17 [PubMed PMID: 30222102]
Dimitropoulos G, Schaepkens van Riempst J, Schertenleib P. Anatomical variation of the lateral femoral cutaneous nerve: a case report and review of the literature. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2011 Jul:64(7):961-2. doi: 10.1016/j.bjps.2010.11.020. Epub 2011 Jan 3 [PubMed PMID: 21208836]
Level 3 (low-level) evidencePearce JM. Meralgia paraesthetica (Bernhardt-Roth syndrome). Journal of neurology, neurosurgery, and psychiatry. 2006 Jan:77(1):84 [PubMed PMID: 16361600]
Weng WC, Wei YC, Huang WY, Chien YY, Peng TI, Wu CL. Risk factor analysis for meralgia paresthetica: A hospital-based study in Taiwan. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia. 2017 Sep:43():192-195. doi: 10.1016/j.jocn.2017.04.024. Epub 2017 May 13 [PubMed PMID: 28511974]
Scholz C, Hohenhaus M, Pedro MT, Uerschels AK, Dengler NF. Meralgia Paresthetica: Relevance, Diagnosis, and Treatment. Deutsches Arzteblatt international. 2023 Sep 29:120(39):655-661. doi: 10.3238/arztebl.m2023.0170. Epub [PubMed PMID: 37534445]
Brandt L, Albert S, Brandt KL. [Meralgia paraesthetica as complication of patient positioning : A not fully controllable risk]. Die Anaesthesiologie. 2022 Nov:71(11):858-864. doi: 10.1007/s00101-022-01213-9. Epub 2022 Oct 25 [PubMed PMID: 36282281]
Schwaiger K, Panzenbeck P, Purschke M, Russe E, Kaplan R, Heinrich K, Mandal P, Wechselberger G. Surgical decompression of the lateral femoral cutaneous nerve (LFCN) for Meralgia paresthetica treatment: Experimental or state of the art? A single-center outcome analysis. Medicine. 2018 Aug:97(33):e11914. doi: 10.1097/MD.0000000000011914. Epub [PubMed PMID: 30113491]
Mugge L, Dang DD, Chandela S. Lateral Femoral Cutaneous Nerve Angiomyoma. Cureus. 2021 Oct:13(10):e18726. doi: 10.7759/cureus.18726. Epub 2021 Oct 12 [PubMed PMID: 34790481]
Kumar S, Hasan R, Maddukuri SB, Mathew M. Angiomyoma presenting as a painful subcutaneous mass: a diagnostic challenge. BMJ case reports. 2014 Oct 16:2014():. doi: 10.1136/bcr-2014-206606. Epub 2014 Oct 16 [PubMed PMID: 25323285]
Level 3 (low-level) evidence