Definition/Introduction
First described by Thomas B. Fitzpatrick in 1972, the Fitzpatrick skin phototypes were developed based on an individual's skin color and their tendency to burn or tan when exposed to sunlight. More specifically, classification was based on a patient's responses to the following questions regarding their skin's reaction to a 45-60 minute, early summer, noon sun exposure in northern latitudes (20-45°): "How painful is your sunburn?" and "How much tan do you develop in a week?" Initially enumerated as skin types I through IV to classify patients with white skin, the Fitzpatrick phototype classification scale was later modified to include types V and VI for persons with darker skin.[1] Generally, a lower Fitzpatrick skin type classification indicates skin that burns more easily than it tans, while a higher Fitzpatrick skin type indicates the opposite (Table 1). The most common skin type in the United States is type III (48%), with types I and II comprising the second largest group (35% in total).[2] See Table. Fitzpatrick Skin Type Descriptions I to VI.
By their nature, Fitzpatrick's skin type classifications are subjective; however, the use of the scale has proven valuable as a diagnostic and therapeutic evaluation tool in many situations. Specifically, these classifications are commonly employed to estimate doses of ultraviolet B (UVB) radiation, psoralen with ultraviolet A (PUVA) therapy, and laser treatments, as well as to predict skin cancer risk and to guide sun protection advice.[3] Though widely used throughout dermatology, plastic surgery, surgical oncology, and other specialties, the Fitzpatrick skin types are not without controversy. Current questions regarding objective determination, self-report accuracy, and effectiveness in ethnic skin are major concerns in Fitzpatrick skin types. See Images. Fitzpatrick Skin Type Quiz, Questionnaire Pages 1 and 2.
Issues of Concern
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Issues of Concern
Objective Determination of Fitzpatrick Skin Types
Given the relative ease of implementation of Fitzpatrick skin typing, it is understandable why this classification system has been so widely applied. However, numerous studies have criticized this system on scientific grounds, and validated objective alternatives have been sought to achieve a comparable prediction of ultraviolet (UV) sensitivity.[4] Methods, including the Wood’s lamp for quantification of cutaneous eumelanin and pheomelanin, have been implemented; however, both have been unsuccessful in differentiating Fitzpatrick skin types higher than level II.[4]
Currently, spectrophotometers are the primary tool for estimating melanin density in the epidermis and for evaluating the accuracy of self-reported skin types.[4] Spectrophotometers are able to distinguish darkening caused by increased melanin from erythema as a result of inflammation or increased hemoglobin, allowing for a more reliable estimation of the true Fitzpatrick skin type.[5] Spectrophotometers have also been used to distinguish constitutive skin color (baseline skin color in body areas not exposed to light) from facultative skin color (skin color in body areas where light-induced pigmentation changes are seen).[4] Specifically, all 6 Fitzpatrick skin types can be discerned using a reflectance spectrophotometer across the 450-615 nm wavelength range.[4] Unfortunately, this tool is not perfect, and the high costs of personnel and equipment may prevent widespread adoption.
Inconsistencies with Self-Reporting and Ethnic Skin
It is important to highlight that the Fitzpatrick skin type is a classification intended to reflect sun sensitivity and not a proxy for racial or phenotypic features. The description of the skin by color – white, brown, black – was meant to denote complexion rather than a self-identification of ethnic origin.[6] For example, a cross-sectional survey of an ethnically diverse population showed self-reported pigmentary phenotypes and race were significant but incomplete predictors of Fitzpatrick skin types.[7]
The difficulty in assessing ethnic skin with the current Fitzpatrick skin type system can be traced to the origin of skin types V and VI. When these additional types were created in 1988, the initial intention was to place all Black individuals in the Type VI category. However, people with mixed heritage or races who identify as black often self-report in a variety of categories, ranging from type IV to type VI.[8] Though the reasons for this are multifaceted, the concept of labeling one’s skin reaction to the sun as tanning or burning lacks reliability, as these words have different meanings to different people. Specifically, participants with skin of color have been shown to report fewer painful burns or tanning episodes, or to have a limited understanding of tanning.[8][9] The functionality of Fitzpatrick skin typing in ethnic skin is also under question. In a population-based study of 2691 participants, this classification system correlated with sun sensitivity among non-Hispanic white and Hispanic participants but not among black participants.[2] In response, multiple scales limited to single ethnic groups have been developed, including a Japanese Skin Type scale by Kawada and a scale for individuals of African descent by Willis and Earles, to more accurately classify the nuances of ethnic skin.[10]
Laser Therapy in Ethnic Skin
Structural and functional differences between darkly pigmented and lightly pigmented skin are important considerations when performing laser or light-based procedures. In general, darker skin types possess increased epidermal melanin, larger and more widely distributed melanosomes, and reactive fibroblasts.[11] Higher Fitzpatrick skin types are therefore associated with these biological characteristics, leading to increased melanin content and epidermal distribution. Increased melanin concentration provides greater protection against ultraviolet radiation, resulting in less pronounced and delayed signs of photoaging.[12]
There are several factors to consider when treating individuals with Fitzpatrick skin types IV through VI. Melanin in the epidermis acts as a chromophore, absorbing more laser energy and increasing the risk of adverse events from epidermal injury in those with darkly pigmented skin. To circumvent this risk, longer-wavelength lasers are recommended. Deeper penetration of the laser allows for an increased ratio of the temperature of the hair bulb to the temperature of the epidermis, leading to follicular destruction with little epidermal damage.[13] Similarly, lower fluences and longer pulse durations (laser hair removal) or lower treatment densities (laser resurfacing) are suggested for darker-skinned individuals to decrease the risk of thermal injury to the epidermis.[13] Pre- and post-treatment with bleaching agents (eg, hydroquinone cream) has been shown to reduce the risk of post-inflammatory hyperpigmentation, particularly after laser resurfacing.[14] Cooling of the epidermis at pre- or post-treatment times can also prevent pigmentary abnormalities, with the most common modalities involving contact or cryogen spray cooling.
With regard to laser or light-based procedures, the risk of postprocedural hyperpigmentation or hypopigmentation is higher in patients with Fitzpatrick skin types IV through VI. In general, dyschromia is among the most common reasons that individuals with skin of color consult dermatologists, as injury or inflammation can alter pigment production.[15] In addition to the aforementioned recommendations, classification systems, such as the Laser Ethnicity Scale, have been developed to better predict healing efficacy and time in patients undergoing laser procedures.[16]
Clinical Significance
Fitzpatrick skin types have long been the favored method of classifying an individual’s skin color based on their specific reactions to sun exposure. Clinically, these designations have been employed to estimate dosages, assess cancer risk, or guide counseling (Figures 1 & 2). However, this system has been recognized as ineffectual in certain populations, especially those with darker, non-Caucasian ethnic skin. These individuals are at greater risk of post-procedural pigmentary and scarring-related adverse effects. Thus, the accurate determination of Fitzpatrick skin types has important therapeutic consequences. Numerous attempts have been made to develop objective methods for determining an individual’s skin type; although none are yet considered a gold standard, reflectance spectrophotometers constitute an efficient, noninvasive alternative with a proven record of success.
Nursing, Allied Health, and Interprofessional Team Interventions
While the determination of Fitzpatrick skin types is typically performed by a physician, the administration of laser treatments may involve multiple healthcare workers. Physicians, physician assistants, nurse practitioners, nurses, and medical assistants are involved in laser treatments, and an interprofessional team approach is essential to prevent and mitigate pre-, intra-, and post-treatment complications. Detailed education on side effects, careful management of expectations, and thorough counseling on results are essential interprofessional team interventions that improve outcomes for patients across all Fitzpatrick skin types.
Media
(Click Image to Enlarge)
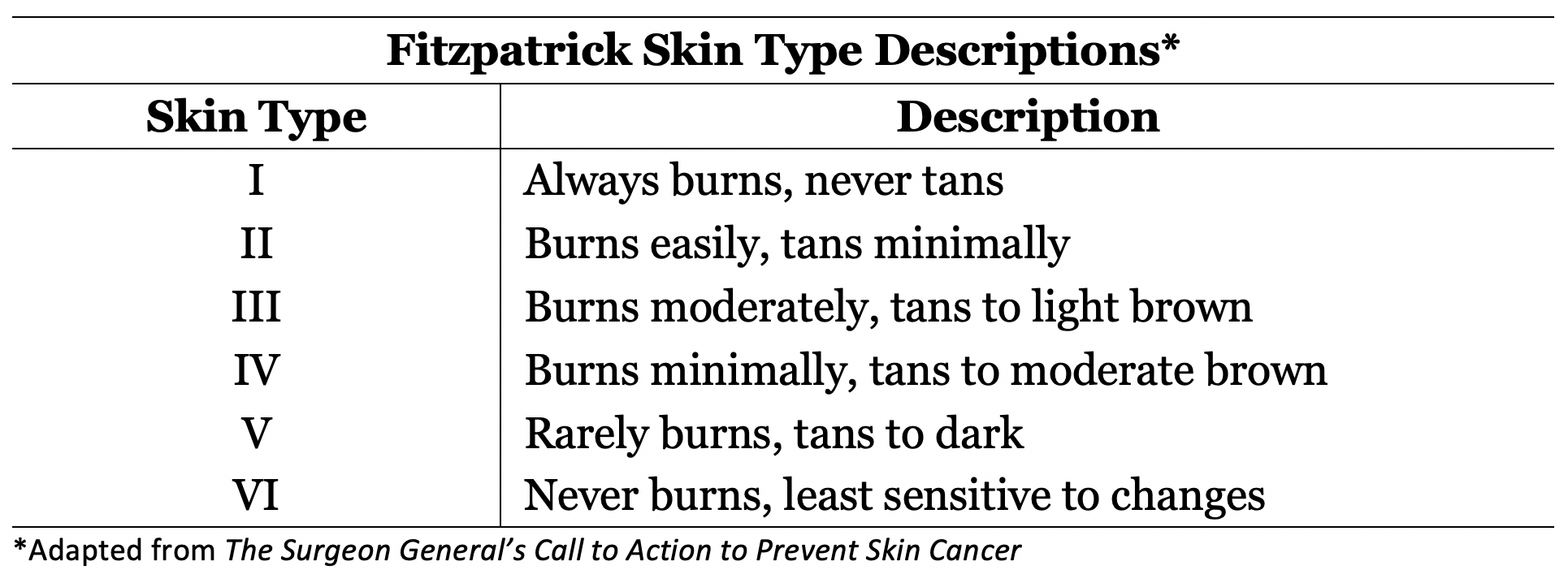
Fitzpatrick Skin Type Descriptions I to VI. The table shows the burning and tanning descriptions for skin types I to VI.
Adapted from the US Department of Health and Human Services. The Surgeon General’s Call to Action to Prevent Skin Cancer. Washington, DC: US Department of Health and Human Services, Office of the Surgeon General; 2014.
(Click Image to Enlarge)
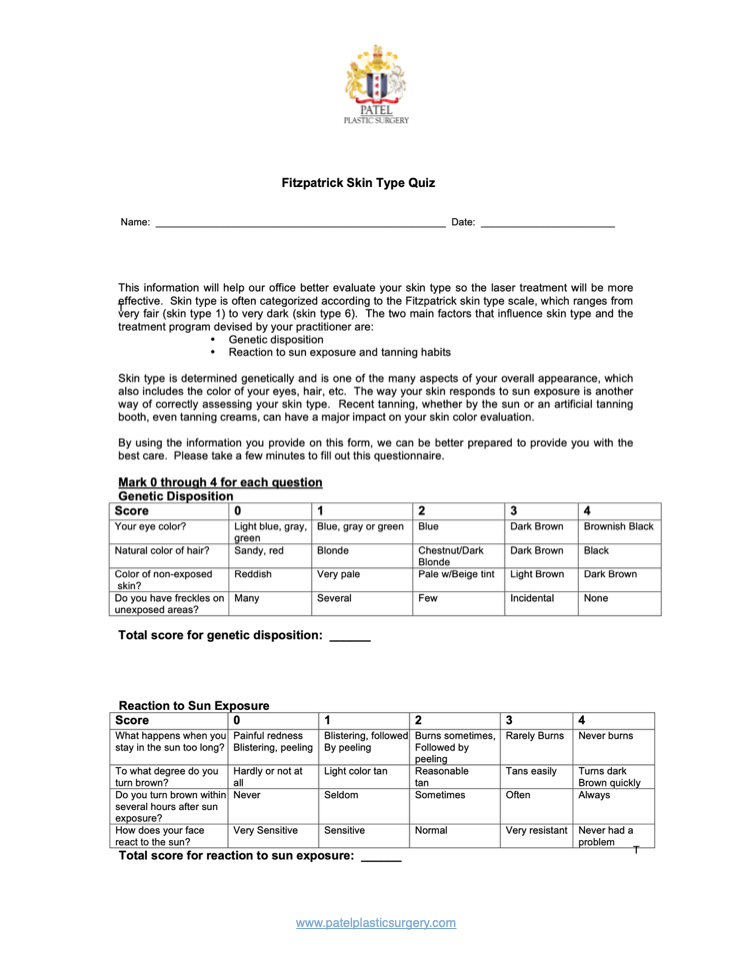
Fitzpatrick Skin Type Quiz, Questionnaire Page 1
Contributed by BCK Patel, MD, FRCS
(Click Image to Enlarge)
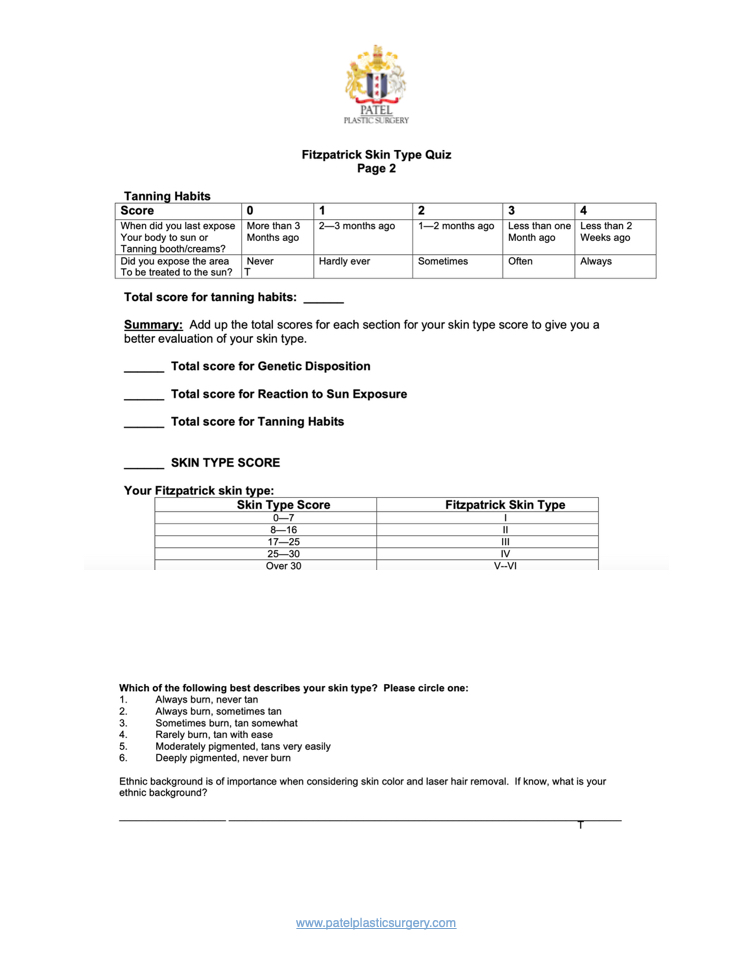
Fitzpatrick Skin Type Quiz, Questionnaire Page 2
Contributed by BCK Patel, MD, FRCS
References
Fitzpatrick TB. The validity and practicality of sun-reactive skin types I through VI. Archives of dermatology. 1988 Jun:124(6):869-71 [PubMed PMID: 3377516]
Keiser E, Linos E, Kanzler M, Lee W, Sainani KL, Tang JY. Reliability and prevalence of digital image skin types in the United States: results from National Health and Nutrition Examination Survey 2003-2004. Journal of the American Academy of Dermatology. 2012 Jan:66(1):163-5. doi: 10.1016/j.jaad.2011.02.044. Epub [PubMed PMID: 22177642]
Level 3 (low-level) evidenceSachdeva S. Fitzpatrick skin typing: applications in dermatology. Indian journal of dermatology, venereology and leprology. 2009 Jan-Feb:75(1):93-6 [PubMed PMID: 19172048]
Pershing LK, Tirumala VP, Nelson JL, Corlett JL, Lin AG, Meyer LJ, Leachman SA. Reflectance spectrophotometer: the dermatologists' sphygmomanometer for skin phototyping? The Journal of investigative dermatology. 2008 Jul:128(7):1633-40. doi: 10.1038/sj.jid.5701238. Epub 2008 Jan 17 [PubMed PMID: 18200057]
Barsh GS. What controls variation in human skin color? PLoS biology. 2003 Oct:1(1):E27 [PubMed PMID: 14551921]
Amblard P, Beani J, Gautron R, Reymond J, Doyon B. Statistical study of individual variations in sunburn sensitivity in 303 volunteers without photodermatosis. Archives of dermatological research. 1982:274(3-4):195-206 [PubMed PMID: 7165371]
He SY, McCulloch CE, Boscardin WJ, Chren MM, Linos E, Arron ST. Self-reported pigmentary phenotypes and race are significant but incomplete predictors of Fitzpatrick skin phototype in an ethnically diverse population. Journal of the American Academy of Dermatology. 2014 Oct:71(4):731-7. doi: 10.1016/j.jaad.2014.05.023. Epub 2014 Jun 11 [PubMed PMID: 24928709]
Level 2 (mid-level) evidenceEilers S, Bach DQ, Gaber R, Blatt H, Guevara Y, Nitsche K, Kundu RV, Robinson JK. Accuracy of self-report in assessing Fitzpatrick skin phototypes I through VI. JAMA dermatology. 2013 Nov:149(11):1289-94. doi: 10.1001/jamadermatol.2013.6101. Epub [PubMed PMID: 24048361]
Level 2 (mid-level) evidenceRobinson JK, Joshi KM, Ortiz S, Kundu RV. Melanoma knowledge, perception, and awareness in ethnic minorities in Chicago: recommendations regarding education. Psycho-oncology. 2011 Mar:20(3):313-20. doi: 10.1002/pon.1736. Epub [PubMed PMID: 20878831]
Kawada A. UVB-induced erythema, delayed tanning, and UVA-induced immediate tanning in Japanese skin. Photo-dermatology. 1986 Dec:3(6):327-33 [PubMed PMID: 3588352]
Alexis AF. Lasers and light-based therapies in ethnic skin: treatment options and recommendations for Fitzpatrick skin types V and VI. The British journal of dermatology. 2013 Oct:169 Suppl 3():91-7. doi: 10.1111/bjd.12526. Epub [PubMed PMID: 24098905]
Alexis AF, Alam M. Racial and ethnic differences in skin aging: implications for treatment with soft tissue fillers. Journal of drugs in dermatology : JDD. 2012 Aug:11(8):s30-2; discussion s32 [PubMed PMID: 22859226]
Level 3 (low-level) evidenceRoss EV, Cooke LM, Timko AL, Overstreet KA, Graham BS, Barnette DJ. Treatment of pseudofolliculitis barbae in skin types IV, V, and VI with a long-pulsed neodymium:yttrium aluminum garnet laser. Journal of the American Academy of Dermatology. 2002 Aug:47(2):263-70 [PubMed PMID: 12140474]
Alajlan AM, Alsuwaidan SN. Acne scars in ethnic skin treated with both non-ablative fractional 1,550 nm and ablative fractional CO2 lasers: comparative retrospective analysis with recommended guidelines. Lasers in surgery and medicine. 2011 Sep:43(8):787-91. doi: 10.1002/lsm.21092. Epub [PubMed PMID: 21956625]
Level 2 (mid-level) evidenceAlexis AF, Sergay AB, Taylor SC. Common dermatologic disorders in skin of color: a comparative practice survey. Cutis. 2007 Nov:80(5):387-94 [PubMed PMID: 18189024]
Level 2 (mid-level) evidenceLancer HA. Lancer Ethnicity Scale (LES). Lasers in surgery and medicine. 1998:22(1):9 [PubMed PMID: 9443143]
Level 3 (low-level) evidence