Introduction
Laryngeal mask airways (LMAs) are single-use or reusable supraglottic airway devices that may be placed temporarily to maintain an open airway during anesthesia administration or used as an immediate lifesaving measure in a difficult airway situation, typically in an unconscious patient who cannot be ventilated easily with a mask and for whom immediate endotracheal intubation would be challenging or delayed. Archibald Brain introduced LMAs into clinical practice in 1983, and LMAs were initially implemented primarily in the operating room but have since become widely used in the intensive care unit, emergency department, and prehospital settings.[1] LMAs are easier to place and more effective than bag-valve-mask devices when used by basic life support personnel and may still constitute an effective alternative to intubation for advanced life support clinicians. In addition to their ease of placement, LMAs produce less throat pain and fewer voice changes than endotracheal tubes; however, this benefit comes with a less secure airway and less effective protection against aspiration of gastric contents.[2] Some LMA models may also be used as a conduit to facilitate endotracheal intubation or even percutaneous tracheostomy.[3]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Supraglottic devices, such as the LMA, are designed to be inserted blindly through the mouth into the hypopharynx to seal around the glottic opening and facilitate positive-pressure ventilation. The proximal, rounded portion of the LMA should be seated on the base of the tongue, superior to the epiglottis, while the sides rest in the piriform sinuses. The distal tip of the device lies in the postcricoid region, ideally occluding the esophageal inlet to prevent inflation of the stomach and exclude refluxed gastric contents, although some LMAs have gastric channels for gastric suctioning (see Image. Laryngeal Mask Airway Positioning).[4] However, effective LMA positioning is variable, with both proximal and distal positions acceptable, provided oxygenation and ventilation remain adequate.[5]
The mnemonic restriction, obstruction, or obesity; disrupted or distorted anatomy; and short thyromental distance (RODS) can be used to predict difficulty in either placing an extraglottic airway device or providing adequate gas exchange through it. The RODS mnemonic includes restriction, obstruction or obesity, disrupted or distorted anatomy, and short thyromental distance. Restriction refers to both increased airway resistance, because extraglottic devices have lower leak pressures than endotracheal tubes, and restricted mouth opening insufficient to permit passage of the device. With restrictive airway disease or low pulmonary compliance, an LMA may leak more than an endotracheal tube because of the higher ventilation pressures required. An LMA typically maintains a seal only up to 15 to 20 cm H2O because it rests on the larynx, whereas an endotracheal tube can support much higher airway pressures without leaking.[5] Patients with obesity may have redundant oral and pharyngeal tissue, making it more difficult to position the device correctly, and the increased ventilatory pressures required for these patients increase the likelihood of a leak. Upper aerodigestive tract obstruction due to a tumor, foreign body, or aberrant anatomy may also make device placement difficult or impossible, although some authors have successfully used LMAs to ventilate patients with tracheal obstruction.[6][7] Additionally, small submandibular spaces, assessed by shortened thyromental distance (less than 3 fingerbreadths), are associated with difficult use of extraglottic devices due to the position of the tongue.
Indications
Laryngeal mask airways (LMAs) may be used as primary airway management devices in the operating room for preselected patients who have fasted. Although LMAs have been employed successfully in pediatric patients, adults, and patients with obesity, the ideal cases for LMA use in the operating room are typically short procedures that will not require head movement, which can cause malposition of the device. LMA placement is also considered the method of choice for airway management when general anesthesia has been induced, but mask ventilation is inadequate, and the patient cannot be intubated.[8] Additionally, when a patient cannot be mask-ventilated and prolonged intubation is not anticipated, placement of an LMA is an effective and expedient means of securing the airway (see Image. American Society of Anesthesiologists Difficult Airway Algorithm: Adult Patients).[5] Even in routine airway management situations, the LMA is an excellent alternative to bag-valve-mask devices to reduce the risk of gastric inflation and aspiration, although LMAs are less protective against aspiration than endotracheal tubes.
In the emergency setting, LMAs are also used as bridges to intubation by prehospital healthcare professionals, in cardiac arrest situations, and as rescue options in difficult airway situations either to secure the airway in preparation for intubation through the device or as temporizing measures before tracheostomy or cricothyrotomy.[9] A properly positioned LMA is particularly effective for facilitating endotracheal intubation over a fiberoptic bronchoscope, because the LMA guides the endoscope straight to the glottic inlet. With sufficient topical and local anesthesia, an LMA can even be used for this purpose in an awake patient who requires endotracheal intubation but whose anatomy is anticipated to be challenging; intubation while the patient is conscious, even with anxiolysis, preserves the airway protective reflexes that potentially prevent an urgent respiratory situation from rapidly progressing to an acute emergency.[5] However, only an endotracheal tube or surgical airway should be considered definitive treatment in an emergency situation, because an LMA will not adequately protect against aspiration of gastric contents in a patient who has not fasted.
Contraindications
Contraindications to LMA use include poor pulmonary compliance, high airway resistance, obesity, retrognathia, increased aspiration risk, and abnormal upper airway anatomy. In particular, patients who require continuous external cricoid pressure to prevent aspiration of gastric contents, such as patients in obstetric settings, are poor candidates for LMA placement because cricoid pressure must be released to permit proper LMA positioning.
Equipment
Laryngeal mask airway devices are available in various forms, depending on the device's primary purpose. The basic design consists of a large-diameter airway tube attached to an inflatable, ovoid cuff that covers the supraglottic area (see Image. Laryngeal Mask Airway). The device permits either spontaneous or positive-pressure ventilation via a conduit with lower resistance than the endotracheal tube that would otherwise be used for the same patient. While the original LMA was reusable, cleaning requirements and high per-unit costs have steered institutions toward less costly single-use LMAs. The original LMA design had crossbars over the aperture to prevent herniation of the epiglottis into the opening; however, that design makes endotracheal intubation through the device impossible. However, those first-generation LMAs are still commonly used for routine cases due to their low cost and low complication rates. Newer, second-generation LMAs are now available and permit higher cuff pressures, lack aperture bars, allow easier intubation with standard endotracheal tubes, and provide a gastric access port for venting or aspirating stomach contents. Some devices even incorporate a bite block.
The LMA Fastrach (Teleflex Inc, Morrisville, NC), also called the intubating laryngeal mask airway (ILMA), is specifically designed to facilitate intubation without the need for visualization. The device is available in both reusable and disposable variants. A handle similar to that of a laryngoscope promotes optimal positioning, and a bar elevates the epiglottis to clear the airway for intubation. The ILMA is designed for use with proprietary endotracheal tubes made and packaged with the device.
The i-gel LMAs (Intersurgical Ltd, Wokingham, UK) are unique in that they have noninflatable collars rather than conventional cuffs. The collars are made of a gel-like substance that will not curl or ripple during placement. I-gel LMAs are designed to allow passage of standard endotracheal tubes and may be used in patients of all ages, from infants to adults. Many other manufacturers produce LMAs with different features, and the selection of a particular device for an individual patient is determined by the clinical situation, the clinician's experience and preference, and equipment availability.
Personnel
Although anesthesia clinicians initially developed and used LMAs, studies have demonstrated successful LMA placement by novice intubators, prehospital healthcare professionals, nurses, advanced practice clinicians, and clinicians from multiple specialties.
Preparation
Before inserting an LMA, the patient should ideally have fasted and be assessed for contraindications. However, this evaluation may not be possible in emergency situations. The LMA is available in various sizes, and recommendations are generally weight-based and printed on the package and device. For adults, the following is a simple size guide: size 3 for those weighing 30 to 50 kg, size 4 for those weighing 50 to 70 kg, and size 5 for those weighing more than 70 kg. In general, the larger size should be chosen for patients between sizes because it will seal more effectively.[10] Regarding medications before LMA placement, neuromuscular blockade may be administered as in endotracheal intubation, but it is not necessarily required because stimulation from tracheal cannulation is absent.[1]
Technique or Treatment
If present, the cuff should be inflated and then completely deflated to ensure the cuff is not folded, with the device pressed firmly against a flat surface before insertion. Both sides of the cuff should be coated with a water-soluble lubricant. When no cervical spine injury risk is present, the neck is extended in a sniffing position. Otherwise, a jaw thrust may be performed to facilitate passage of the device through the mouth. The LMA is introduced behind the tongue with backward pressure using the index finger, pressing the device against the hard palate until it is completely inserted. The other hand then pushes the LMA until resistance is felt and the device cannot advance farther. Alternatively, the LMA may be passed into the mouth with the cuff facing the posterior pharynx and the device rotated 180° as it is advanced into the supraglottis. Importantly, no cricoid pressure should be applied during insertion, because this prevents the distal tip of the LMA from advancing sufficiently into the hypopharynx.[11] The cuff is then inflated with approximately 20 mL of air for a size 3 device, 30 mL for a size 4 device, and 40 mL for a size 5 device, which should result in a cuff pressure of less than 60 cm H2O. Once the cuff is inflated, a subtle fullness of the anterior neck at the level of the larynx is typically visible. This volume may need to be adjusted to optimize the seal and minimize the air leak. An air leak may also occur if placement is not quite correct, but a slight shift in the LMA's position typically remedies the leak quickly. Once the cuff is inflated with the appropriate amount of air and a good seal is obtained, correct placement is verified by attaching a bag-mask device, delivering breaths, assessing breath sounds, and using continuous waveform capnography or, at a minimum, a CO2 detector device.
Endotracheal intubation can be achieved by inserting the endotracheal tube (ETT) through most second-generation LMAs. The Fastrach LMA has a higher rate of successful intubation than first-generation LMAs and is designed for blind intubation using the company’s proprietary endotracheal tube. Blind intubation success rates are higher with the Fastrach than with other supraglottic devices, such as the i-gel and Air-Q (DeRoyal Industries Inc). The i-gel appears to outperform the AuraGain (Ambu Inc, Ballerup, Denmark), which is not recommended for blind intubation.[12] Since failure rates can be as high as 40%, endotracheal intubation through an LMA is best performed under indirect visualization using a flexible bronchoscope. Standard endotracheal tubes are usually not long enough to go past the vocal cords when inserted through an LMA. Using either a tube exchanger that slides over a flexible bronchoscope or a nasal Adair-Elwyn tube, which is longer, can overcome that problem. Newer, third-generation LMAs incorporate vision guidance systems and may also serve as intubation aids, offering a good alternative to endoscopic intubation.[13][14] Additionally, LMAs are being developed to incorporate automatic recording, which may be valuable for teaching and medicolegal documentation.[15]
Complications
The distal tip of the cuff on the LMA may occasionally roll upward during insertion, hindering optimal placement. Some experts encourage partial inflation of the cuff before insertion or inserting the LMA turned around and rotating it into position to prevent this complication, but evidence is insufficient to recommend this practice. Forceful insertion may cause abrasion of the pharyngeal mucosa or bleeding, and anterior malposition of the tip may occlude the laryngeal opening. Additionally, gastric insufflation may occur with high-pressure ventilation. The degree to which LMAs of different varieties prevent aspiration of gastric contents is unknown, and LMA use should be considered a temporary or rescue measure in patients at risk for vomiting and aspiration, rather than a replacement for endotracheal intubation. Maintaining an effective seal around the cuff may be difficult in patients who require high positive airway pressures due to restrictive pulmonary conditions, such as obesity. In addition, having patients with morbid obesity breathe spontaneously through an LMA during anesthesia may lead to hypoventilation due to the patient's position and the weight of the abdomen.[16] However, LMAs are frequently used successfully as rescue devices in patients with obesity and difficult mask ventilation or difficult airways.[17] Clinicians should remember that the device may also easily become malpositioned during cardiopulmonary resuscitation or if the patient's head is moved away from the midline.[18]
The complication rates with LMAs are lower than those associated with both endotracheal intubation and bag-valve-mask devices; however, despite their ease of use and safety profile, significant complications may occur with LMA use, including nausea, vomiting, aspiration, and coughing. LMAs may stimulate the gag reflex and, therefore, should not be used in conscious patients. Laryngospasm may also occur, particularly when a patient's head is moved or the airway is manipulated while the LMA is in place.
Clinical Significance
Laryngeal mask airways are essential tools in modern airway management, combining the advantages of external mask ventilation and endotracheal intubation. Results from studies demonstrated their safety and efficacy across patients of all ages, often with fewer complications than endotracheal intubation.[19][20] Results from studies also showed that LMAs were as effective as other airway management strategies in patients receiving cardiopulmonary resuscitation and potentially more effective than mask ventilation for healthcare personnel without significant airway management experience.[21]
Failure rates for blind intubation with an LMA range from 10% to 70%, depending on the device and the operator's skill.[22][23] Blind intubation success rates are highest for the Fastrach LMA (intubating laryngeal mask airway) compared with other supraglottic devices, but are best achieved with flexible fiberoptic guidance or a vision-incorporated third-generation LMA whenever possible. Ultimately, however, an LMA should not be the final secured airway solution in a failed airway rescue, because LMAs can be dislodged relatively easily and are better suited as a conduit to a secure airway with an endotracheal tube.
Enhancing Healthcare Team Outcomes
Laryngeal mask airways have an important role in the treatment of patients with respiratory distress. While most healthcare professionals are familiar with the endotracheal tube, LMA use requires experience. Healthcare professionals, including those who have never used an LMA, should first consult with an anesthesiologist before attempting placement. The LMA is only a temporary airway solution and can be easily dislodged by patient movement; therefore, it is generally used in the operating room.
Media
(Click Image to Enlarge)
Laryngeal Mask Airway. This illustration shows a laryngeal mask airway.
Contributed by S Dulebohn, MD
(Click Image to Enlarge)
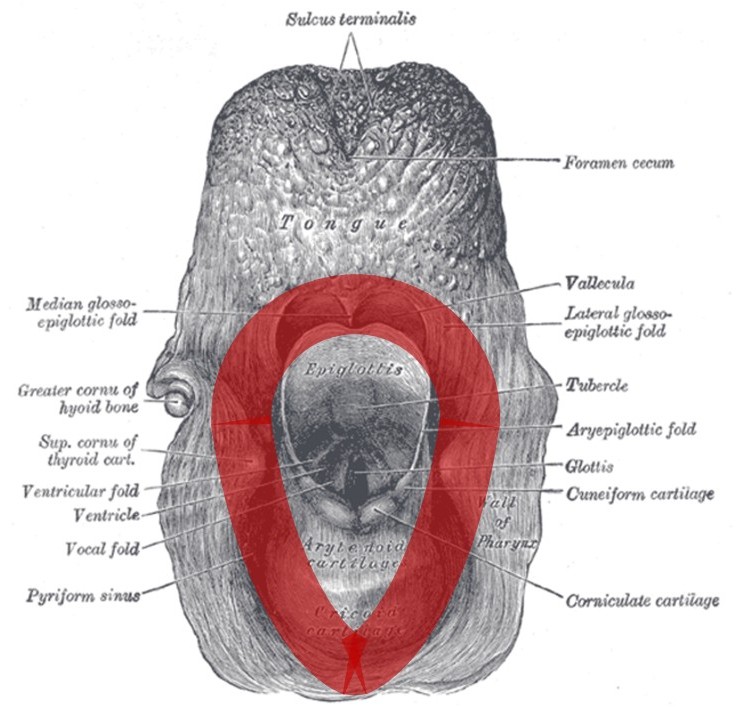
Laryngeal mask airway positioning. The cuff of the device (red) surrounds the laryngeal inlet, resting superiorly on the base of the tongue above the epiglottis, laterally sealing against the piriform sinuses, and inferiorly lying on the posterior aspect of the cricoid cartilage, with the tip of the device occluding the esophageal inlet so as to prevent gastric insufflation.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
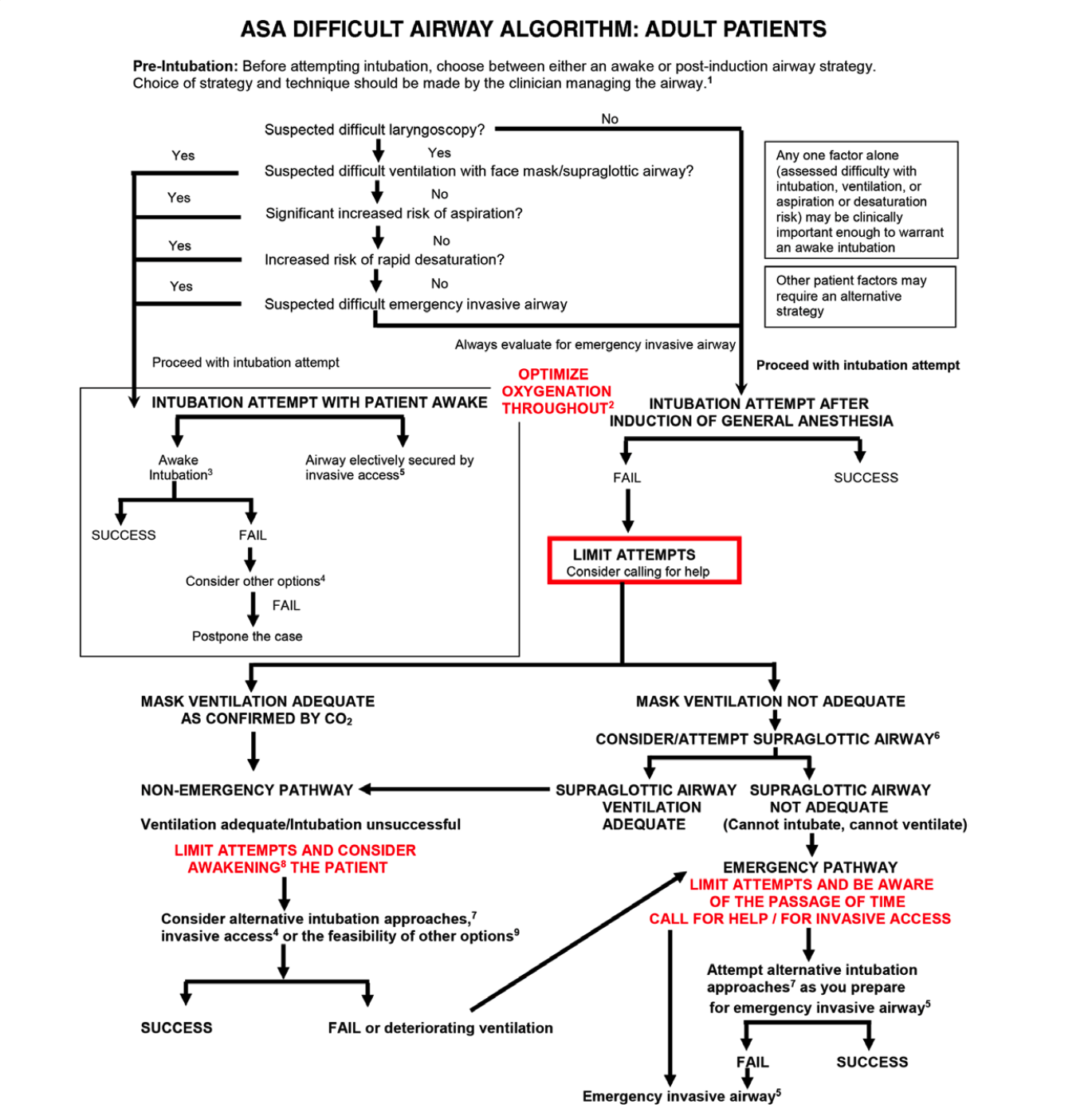
ASA Difficult Airway Algorithm: Adult Patients
Apfelbaum JL, Hagberg CA, Connis RT, Abdelmalak BB, Agarkar M, Dutton RP, Fiadjoe JE, Greif R, Klock PA, Mercier D, Myatra SN, O'Sullivan EP, Rosenblatt WH, Sorbello M, Tung A. 2022 American Society of Anesthesiologists Practice Guidelines for Management of the Difficult Airway. Anesthesiology. 2022 Jan 1;136(1):31-81. doi: 10.1097/ALN.0000000000004002. PMID: 34762729.
References
Brain AI. The laryngeal mask--a new concept in airway management. British journal of anaesthesia. 1983 Aug:55(8):801-5 [PubMed PMID: 6349667]
Singh A, Bhalotra AR, Anand R. A comparative evaluation of ProSeal laryngeal mask airway, I-gel and Supreme laryngeal mask airway in adult patients undergoing elective surgery: A randomised trial. Indian journal of anaesthesia. 2018 Nov:62(11):858-864. doi: 10.4103/ija.IJA_153_18. Epub [PubMed PMID: 30532321]
Level 2 (mid-level) evidenceStrametz R, Bergold MN, Weberschock T. Laryngeal mask airway versus endotracheal tube for percutaneous dilatational tracheostomy in critically ill adults. The Cochrane database of systematic reviews. 2018 Nov 15:11(11):CD009901. doi: 10.1002/14651858.CD009901.pub3. Epub 2018 Nov 15 [PubMed PMID: 30536850]
Level 1 (high-level) evidenceIn CB, Cho SA, Lee SJ, Sung TY, Cho CK. Comparison of the clinical performance of airway management with the i-gel® and laryngeal mask airway SupremeTM in geriatric patients: a prospective and randomized study. Korean journal of anesthesiology. 2019 Feb:72(1):39-46. doi: 10.4097/kja.d.18.00121. Epub 2018 Oct 22 [PubMed PMID: 30343563]
Level 1 (high-level) evidenceBenumof JL. Laryngeal mask airway and the ASA difficult airway algorithm. Anesthesiology. 1996 Mar:84(3):686-99 [PubMed PMID: 8659797]
Schieren M, Egyed E, Hartmann B, Aleksanyan A, Stoelben E, Wappler F, Defosse JM. Airway Management by Laryngeal Mask Airways for Cervical Tracheal Resection and Reconstruction: A Single-Center Retrospective Analysis. Anesthesia and analgesia. 2018 Apr:126(4):1257-1261. doi: 10.1213/ANE.0000000000002753. Epub [PubMed PMID: 29293182]
Level 2 (mid-level) evidenceGadre VN, Ramteke DB, Yadav SR, Mundrawala EG. Anaesthesia for tracheal reconstruction - Neither a dilemma nor a catastrophe. Indian journal of anaesthesia. 2019 Feb:63(2):152-153. doi: 10.4103/ija.IJA_629_18. Epub [PubMed PMID: 30814758]
Apfelbaum JL, Hagberg CA, Caplan RA, Blitt CD, Connis RT, Nickinovich DG, Hagberg CA, Caplan RA, Benumof JL, Berry FA, Blitt CD, Bode RH, Cheney FW, Connis RT, Guidry OF, Nickinovich DG, Ovassapian A, American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Practice guidelines for management of the difficult airway: an updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Anesthesiology. 2013 Feb:118(2):251-70. doi: 10.1097/ALN.0b013e31827773b2. Epub [PubMed PMID: 23364566]
Level 1 (high-level) evidenceWhite L, Melhuish T, Holyoak R, Ryan T, Kempton H, Vlok R. Advanced airway management in out of hospital cardiac arrest: A systematic review and meta-analysis. The American journal of emergency medicine. 2018 Dec:36(12):2298-2306. doi: 10.1016/j.ajem.2018.09.045. Epub 2018 Sep 26 [PubMed PMID: 30293843]
Level 1 (high-level) evidenceDe Rosa S, Messina A, Sorbello M, Rigobello A, Colombo D, Piccolo A, Bonaldi E, Gennaro P, Urukalo V, Pellizzari A, Bonato R, Carboni SC. Laryngeal Mask Airway Supreme vs. the Spritztube tracheal cannula in anaesthetised adult patients: A randomised controlled trial. European journal of anaesthesiology. 2019 Dec:36(12):955-962. doi: 10.1097/EJA.0000000000001106. Epub [PubMed PMID: 31644512]
Level 1 (high-level) evidenceBrimacombe J, Berry A. Cricoid pressure and the LMA: efficacy and interpretation. British journal of anaesthesia. 1994 Dec:73(6):862-5 [PubMed PMID: 7741878]
Tejada-Perdomo JH, Melo-Moreno CE, Tovar-Cardozo JH, Ramos-Castaneda JA. Supraglottic airway devices for blind endotracheal intubation: A systematic review. PloS one. 2024:19(12):e0315301. doi: 10.1371/journal.pone.0315301. Epub 2024 Dec 11 [PubMed PMID: 39661586]
Level 1 (high-level) evidenceCastillo-Monzón CG, Gaszyński T, Marroquín-Valz HA, Orozco-Montes J, Ratajczyk P. Supraglottic Airway Devices with Vision Guided Systems: Third Generation of Supraglottic Airway Devices. Journal of clinical medicine. 2023 Aug 9:12(16):. doi: 10.3390/jcm12165197. Epub 2023 Aug 9 [PubMed PMID: 37629238]
Van Zundert AAJ, Gatt SP, Van Zundert TCRV, Kumar CM, Pandit JJ. Features of new vision-incorporated third-generation video laryngeal mask airways. Journal of clinical monitoring and computing. 2022 Aug:36(4):921-928. doi: 10.1007/s10877-021-00780-3. Epub 2021 Dec 17 [PubMed PMID: 34919170]
van Zundert AAJ, Gatt SP, van Zundert TCRV, Hagberg CA, Pandit JJ. Supraglottic Airway Devices: Present State and Outlook for 2050. Anesthesia and analgesia. 2024 Feb 1:138(2):337-349. doi: 10.1213/ANE.0000000000006673. Epub 2024 Jan 12 [PubMed PMID: 38215712]
Kim HY, Baek SH, Cho YH, Kim JY, Choi YM, Choi EJ, Yoon JP, Park JH. Iatrogenic Intramural Dissection of the Esophagus after Insertion of a Laryngeal Mask Airway. Acute and critical care. 2018 Nov:33(4):276-279. doi: 10.4266/acc.2016.00829. Epub 2017 Jun 30 [PubMed PMID: 31723897]
Sinha A, Jayaraman L, Punhani D. The supraglottic airway device as first line of management in anticipated difficult mask ventilation in the morbidly obese. Journal of anaesthesiology, clinical pharmacology. 2019 Oct-Dec:35(4):540-545. doi: 10.4103/joacp.JOACP_159_19. Epub [PubMed PMID: 31920242]
Sabuncu U, Kusderci HS, Oterkus M, Abdullayev R, Demir A, Uludag O, Ozdas S, Goksu M. AuraGain and i-Gel laryngeal masks in general anesthesia for laparoscopic cholecystectomy. Performance characteristics and effects on hemodynamics. Saudi medical journal. 2018 Nov:39(11):1082-1089. doi: 10.15537/smj.2018.11.22346. Epub [PubMed PMID: 30397706]
Yang LQ, Zhu L, Shi X, Miao CH, Yuan HB, Liu ZQ, Gu WD, Liu F, Hu XX, Shi DP, Duan HW, Wang CY, Weng H, Huang ZL, Li LZ, He ZZ, Li J, Hu YP, Lin L, Pan ST, Xu SH, Tang D, Sessler DI, Liu J, Irwin MG, Yu WF, POLMA-EP investigators. Postoperative pulmonary complications in older patients undergoing elective surgery with a supraglottic airway device or tracheal intubation. Anaesthesia. 2023 Aug:78(8):953-962. doi: 10.1111/anae.16030. Epub 2023 Jun 4 [PubMed PMID: 37270923]
Jamil SN, Alam M, Usmani H, Khan MM. A Study of the Use of Laryngeal Mask Airway (LMA) in Children and its Comparison with Endotracheal Intubation. Indian journal of anaesthesia. 2009 Apr:53(2):174-8 [PubMed PMID: 20640119]
Martin PD, Cyna AM, Hunter WA, Henry J, Ramayya GP. Training nursing staff in airway management for resuscitation. A clinical comparison of the facemask and laryngeal mask. Anaesthesia. 1993 Jan:48(1):33-7 [PubMed PMID: 8434745]
Lim SL, Tay DH, Thomas E. A comparison of three types of tracheal tube for use in laryngeal mask assisted blind orotracheal intubation. Anaesthesia. 1994 Mar:49(3):255-7 [PubMed PMID: 7848398]
Heath ML. Endotracheal intubation through the Laryngeal Mask--helpful when laryngoscopy is difficult or dangerous. European journal of anaesthesiology. Supplement. 1991:4():41-5 [PubMed PMID: 1879412]