Introduction
The heart's electrical conduction system is mediated by structures composed of specialized pacemaker cells. The primary pacemaker, the sinoatrial node, is located subepicardially in the right atrial wall near the junction with the superior vena cava. The atrioventricular node lies subendocardially within the triangle of Koch, bordered posteriorly by the coronary sinus ostium, superiorly by the tendon of Todaro, and anteriorly by the septal leaflet of the tricuspid valve. The atrioventricular node tapers into the bundle of His, which bifurcates into right and left bundle branches coursing along the interventricular septum and giving rise to Purkinje fibers in the subendocardial regions of the ventricles.
The sinoatrial node receives blood supply from the sinoatrial nodal artery, a branch of the right coronary artery in approximately 60% of individuals and the left circumflex coronary artery in the remaining 40%. The atrioventricular node is supplied by the atrioventricular nodal branch, most commonly from the right coronary artery (90%) or, less frequently, from the left circumflex artery (10%), depending on coronary dominance. Under normal conditions, electrical impulses originate in the sinoatrial node, initiating atrial contraction. The impulse then travels to the atrioventricular node, where conduction slows briefly before continuing through the bundle of His and Purkinje fibers to trigger ventricular contraction.
Each region containing specialized pacemaker cells can independently sustain the heart rate. Under physiologic conditions, secondary pacemaker sites remain suppressed by overdrive inhibition from the faster depolarization rate of the sinoatrial node, maintaining normal sinus rhythm. If the sinoatrial node slows below the intrinsic rate of another pacemaking structure, the faster region assumes control as the dominant pacemaker. Each region possesses a distinct intrinsic depolarization rate. Therefore, the resulting heart rate and rhythm depend on the predominant site. This mechanism underlies the various forms of junctional rhythm (see Image. Junctional Rhythm).[1][2][3][4][5][6]
The terminology used to classify junctional rhythms is based on ventricular rate and includes the following categories:
- Junctional bradycardia: Heart rate below 40 bpm
- Junctional escape rhythm: Heart rate between 40 and 60 bpm
- Accelerated junctional rhythm: Heart rate between 60 and 100 bpm
- Junctional tachycardia: Heart rate exceeding 100 bpm
Classification of junctional rhythms by rate allows precise identification of underlying electrophysiologic disturbances. Accurate categorization is essential for guiding appropriate management and optimizing patient outcomes.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
A junctional rhythm develops when electrical impulses from the sinoatrial node are blocked or fall below the intrinsic automaticity of the atrioventricular node or bundle of His. Multiple conditions and medications can impair sinoatrial node function and precipitate a junctional rhythm.[7][8][9][10][11][12][13][14] The most commonly reported triggers fall into the following categories:
- Structural and inflammatory causes: Chest trauma, myocarditis, pericarditis, radiation therapy, repair of congenital heart disease, rheumatic fever, ischemic heart disease, acute myocardial infarction, acute and chronic coronary artery disease, amyloidosis, Lyme disease
- Conduction system disorders: Sick sinus syndrome, familial conduction disorders, inherited channelopathy, high-grade second-degree heart block, third-degree heart block
- Neuromuscular conditions: Neuromuscular disorders, X-linked muscular dystrophy
- Systemic conditions: Collagen vascular disease, hypothyroidism, sleep apnea, hypoxia
- Neurologic conditions: Intracranial hypertension, anorexia nervosa
- Autonomic and reflex causes: Vasovagal stimulation (eg, endotracheal suctioning), carotid sinus hypersensitivity
- Electrolyte and metabolic disturbances: Hyperkalemia
- Medications: Clonidine, reserpine, adenosine, cimetidine, antiarrhythmics (classes I–IV), lithium, amitriptyline, β-blockers, calcium channel blockers, digoxin, ivabradine, opioids, cannabinoids, isoproterenol infusion
A wide spectrum of pathologies and pharmacologic agents can precipitate junctional rhythms by disrupting sinoatrial node automaticity. Identification of underlying causes enables targeted management strategies.
Epidemiology
A junctional rhythm may occur in any patient population and affects female and male individuals equally. Morbidity and mortality associated with this rhythm depend directly on the underlying etiology. Consequently, junctional rhythm can represent a benign, intermittent finding in healthy children, athletes, or individuals with increased vagal tone during sleep. This rhythm is also frequently reported as a complication following cardiac procedures, including transcatheter aortic valve replacement and surgeries for congenital cardiac disorders.[15][16]
Pathophysiology
The intrinsic depolarization rate decreases at each successive pacemaker site as the electrical impulse travels through the heart’s conduction system. Junctional rhythms commonly result from sinoatrial node dysfunction, which slows or ceases the node's intrinsic rate. In rare cases, increased automaticity of the atrioventricular node may allow it to override a normally functioning sinoatrial node. Consequently, junctional rhythms may present with rates slower than, equal to, or faster than the typical heart rate.
Intrinsic pacemaker sites and their depolarization rates are as follows:
- Sinoatrial node: 60 to 100 bpm
- Atria: less than 60 bpm
- Atrioventricular node: 40 to 60 bpm
- Ventricles: 20 to 40 bpm
Junctional rhythms reflect shifts in the dominant pacemaker driven by alterations in intrinsic depolarization rates. Recognition of these rate patterns supports accurate diagnosis and guides management strategies for this arrhythmia.
Histopathology
Histopathological findings vary according to the underlying cause of the junctional rhythm. Conditions contributing to sinoatrial node remodeling include myocardial fibrosis, atrophy, hypoplasia, and amyloid deposition. These structural alterations can disrupt normal pacemaker function and predispose to arrhythmia. However, histological abnormalities may be absent despite documented sinoatrial node dysfunction.[17][18]
History and Physical
Patients with junctional rhythm may present with various symptoms or remain asymptomatic. Key history elements include underlying heart disease, recent cardiac procedures, medications, substance use, and a comprehensive review of systems to identify potential triggers. A history of congenital heart disease or a lack of standard newborn screening warrants particular attention in pediatrics.
Symptom presentation largely depends on the underlying etiology of the junctional rhythm. For example, patients with heart failure exacerbation may experience dyspnea and lower extremity edema. Individuals with rheumatic fever may present with a heart murmur secondary to valvular damage, fever, arthralgia, and rash. Other patients may report nonspecific complaints such as dizziness, fatigue, syncope or near-syncope, and palpitations. Physical examination may reveal nonspecific findings, including distended neck veins and a regular heart rate of 20 to 100 bpm.[19][20][21]
Evaluation
History and physical examination are critical components in assessing a patient presenting with signs and symptoms potentially attributable to a junctional rhythm. Hemodynamic stability should be evaluated, and the examination must include vital signs such as respiratory rate, blood pressure, temperature, and heart rate. The history should encompass a review of the patient’s medication list. Diagnostic workup must include an electrocardiogram (ECG). Assessment should also evaluate for underlying ischemic heart disease or heart failure. Consideration may be given to thyroid function testing, routine blood tests, and echocardiography as part of the initial investigation.
Normal P waves measure less than 0.12 seconds (3 small boxes) and appear upright in leads I and II, and inverted in aVR. Inverted P waves in the inferior leads (II, III, aVF) indicate a nonsinoatrial origin. In junctional rhythms, the electrical impulse often arises at or near the atrioventricular node, frequently rendering the P wave invisible. When visible, the P wave may occur just before or after the QRS complex, or be embedded within it. The morphology of visible P waves is often inverted (retrograde) rather than upright. Other specific ECG findings depend on the precise classification of the junctional rhythm. (Source: Bhattad and Jain, 2020)
Treatment / Management
Treatment of a junctional rhythm primarily depends on its underlying cause. Termination should be avoided when the rhythm results from sinus node dysfunction, causing asystole or bradycardia, as the junctional rhythm maintains the heart rate. Identifying the underlying etiology is essential before establishing a management plan. Otherwise healthy individuals with a junctional rhythm who are asymptomatic typically require no medical intervention. This rhythm usually reflects increased vagal tone, which suppresses the intrinsic automaticity of the sinoatrial node.
In cases of digoxin toxicity, treatment includes atropine and digoxin-specific antibodies. If pharmacologic therapy fails and junctional tachycardia develops, intravenous phenytoin may be administered in a monitored setting due to the risk of hypotension. In the pediatric population, persistent symptomatic junctional tachycardia warrants consideration of percutaneous radiofrequency ablation. Permanent pacemaker implantation is indicated in patients with sick sinus syndrome or complete or high-grade atrioventricular block.[22][23][24][25][26](B2)
Differential Diagnosis
The differential diagnosis includes the following:
- Digoxin toxicity
- Atrioventricular nodal reentrant tachycardia
- Atrioventricular reentrant tachycardia
- Sinus node dysfunction
- High-grade second-degree heart block
- Third-degree heart block
Given the overlap in presentation, a detailed assessment is required to differentiate junctional rhythm from other supraventricular arrhythmias and conduction blocks. Proper identification ensures timely and precise intervention.
Prognosis
As with management, outcomes depend largely on the underlying etiology and the specific type of junctional rhythm. Congenital junctional ectopic tachycardia in pediatrics carries higher morbidity and mortality compared to the postoperative form of the same arrhythmia. Prompt identification and treatment of the rhythm and its underlying cause are essential for optimizing outcomes. For additional information, see StatPearls’ companion reference on junctional ectopic tachycardia.[27]
Complications
Symptoms such as syncope, fatigue, or dizziness may arise when junctional rhythms are not promptly identified. Certain forms may result in cardiac dilation, leading to congestive heart failure or progression to more serious arrhythmias, including ventricular fibrillation or complete heart block. Others may cause severe hypotension, particularly in patients with underlying autonomic dysfunction.[28]
Deterrence and Patient Education
Patient education should be provided using accessible and familiar resources, such as pamphlets or trusted online platforms. Symptom tracking, including palpitations or dizziness, should be encouraged, with prompt reporting of any changes. Emphasis on medication adherence and regular follow-up visits supports early detection and management of recurrent or worsening junctional rhythms.
Pearls and Other Issues
Integrating clinical history with focused diagnostic testing can expedite management and improve outcomes. In patients with a junctional rhythm receiving digoxin, a serum digoxin level should always be obtained to evaluate possible toxicity. In patients with a history of tick exposure, empirical antibiotic therapy should be initiated while awaiting Lyme disease serologic results, as early treatment may prevent progression of underlying infectious causes.
Enhancing Healthcare Team Outcomes
Junctional rhythms encompass multiple subtypes with varied presentations, prognoses, and potential complications. These rhythms can arise from a wide range of conditions, diseases, and pharmacologic agents. Awareness and role-specific competence among all members of the healthcare team are essential when a junctional rhythm is identified.
Effective management is best achieved through an interprofessional approach. Nurses often serve as the first to recognize junctional rhythms on telemetry monitoring. Initial evaluation is typically performed by primary care or emergency medicine clinicians, with cardiology referral warranted for most new diagnoses. Cardiologists provide ongoing care in both inpatient and outpatient settings.
Cardiology and emergency nurses play a critical role in administering treatments, monitoring responses, and collaborating with physicians or advanced practice providers to detect complications. Pharmacists review medications, identify potential drug interactions, and counsel patients regarding appropriate use and side effects. Patient education and ensuring closed-loop communication between patients and the healthcare team further optimize management of junctional rhythms.
Media
(Click Image to Enlarge)
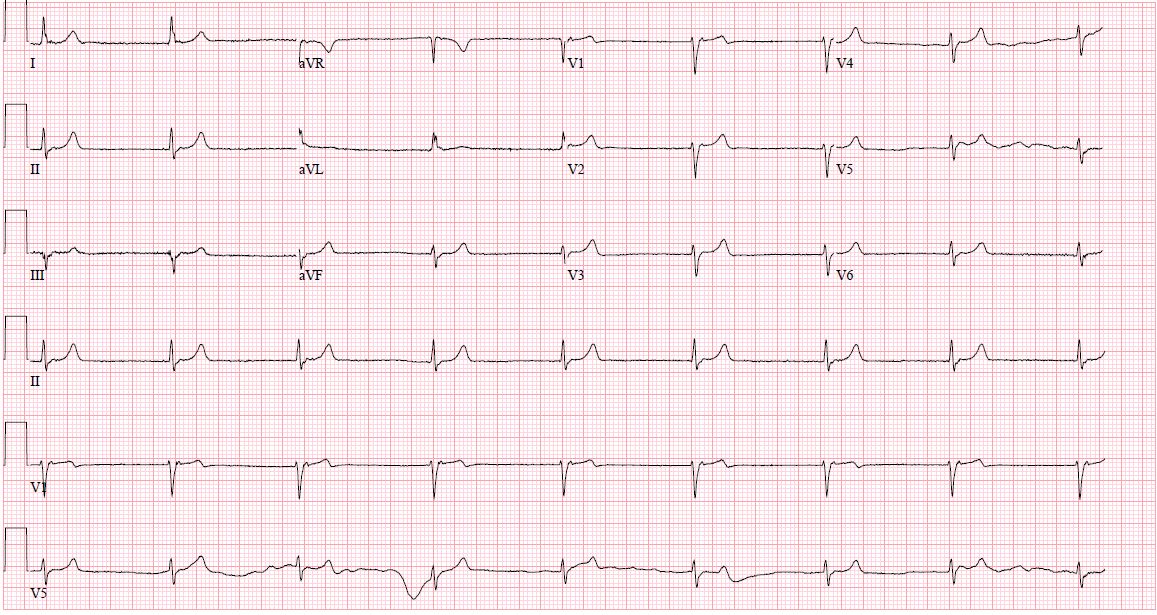
Junctional Rhythm. This electrocardiogram shows a regular rhythm with absent or inverted P waves and a narrow QRS complex, consistent with an electrical impulse originating near the atrioventricular node.
Contributed by D Desai, MD, MPH
References
Spodick DH. Normal sinus heart rate: sinus tachycardia and sinus bradycardia redefined. American heart journal. 1992 Oct:124(4):1119-21 [PubMed PMID: 1529897]
Thery C, Gosselin B, Lekieffre J, Warembourg H. Pathology of sinoatrial node. Correlations with electrocardiographic findings in 111 patients. American heart journal. 1977 Jun:93(6):735-40 [PubMed PMID: 871100]
Dobrzynski H, Anderson RH, Atkinson A, Borbas Z, D'Souza A, Fraser JF, Inada S, Logantha SJ, Monfredi O, Morris GM, Moorman AF, Nikolaidou T, Schneider H, Szuts V, Temple IP, Yanni J, Boyett MR. Structure, function and clinical relevance of the cardiac conduction system, including the atrioventricular ring and outflow tract tissues. Pharmacology & therapeutics. 2013 Aug:139(2):260-88. doi: 10.1016/j.pharmthera.2013.04.010. Epub 2013 Apr 20 [PubMed PMID: 23612425]
Level 3 (low-level) evidenceVan der Hauwaert LG, Stroobandt R, Verhaeghe L. Arterial blood supply of the atrioventricular node and main bundle. British heart journal. 1972 Oct:34(10):1045-51 [PubMed PMID: 5086972]
Pejković B, Krajnc I, Anderhuber F, Kosutić D. Anatomical aspects of the arterial blood supply to the sinoatrial and atrioventricular nodes of the human heart. The Journal of international medical research. 2008 Jul-Aug:36(4):691-8 [PubMed PMID: 18652764]
Chua K, Upadhyay GA, Lee E, Aziz Z, Beaser AD, Ozcan C, Broman M, Nayak HM, Tung R. High-resolution mapping of the triangle of Koch: Spatial heterogeneity of fast pathway atrionodal connections. Heart rhythm. 2018 Mar:15(3):421-429. doi: 10.1016/j.hrthm.2017.10.030. Epub 2017 Nov 26 [PubMed PMID: 29081398]
Semelka M, Gera J, Usman S. Sick sinus syndrome: a review. American family physician. 2013 May 15:87(10):691-6 [PubMed PMID: 23939447]
Trappe HJ. Tachyarrhythmias, bradyarrhythmias and acute coronary syndromes. Journal of emergencies, trauma, and shock. 2010 Apr:3(2):137-42. doi: 10.4103/0974-2700.62112. Epub [PubMed PMID: 20606790]
Silvestri NJ, Ismail H, Zimetbaum P, Raynor EM. Cardiac involvement in the muscular dystrophies. Muscle & nerve. 2018 May:57(5):707-715. doi: 10.1002/mus.26014. Epub 2017 Nov 28 [PubMed PMID: 29130502]
Patel P, Kelschenbach K. Case of Junctional Rhythm in the Setting of Acute Adrenal Insufficiency. Cureus. 2022 Aug:14(8):e27605. doi: 10.7759/cureus.27605. Epub 2022 Aug 2 [PubMed PMID: 36059370]
Level 3 (low-level) evidenceEid MM. COVID-19 patient with symptomatic bradycardia. Visual journal of emergency medicine. 2021 Jan:22():100920. doi: 10.1016/j.visj.2020.100920. Epub 2020 Nov 11 [PubMed PMID: 33200102]
Frustaci A, Verardo R, Galea N, Lavalle C, Bagnato G, Scialla R, Chimenti C. Hypersensitivity Myocarditis after COVID-19 mRNA Vaccination. Journal of clinical medicine. 2022 Mar 16:11(6):. doi: 10.3390/jcm11061660. Epub 2022 Mar 16 [PubMed PMID: 35329986]
Vishnu VK, Jamshed N, Amrithanand VT, Thandar S. BRASH Syndrome: A Case Report. The Journal of emergency medicine. 2021 Jun:60(6):818-822. doi: 10.1016/j.jemermed.2021.01.033. Epub 2021 Feb 24 [PubMed PMID: 33640217]
Level 3 (low-level) evidenceDrumheller BC, Tuffy E, Gibney F, Stallard S, Siewers C, Korvek S. Severe bradycardia from severe hyperkalemia: Patient characteristics, outcomes and factors associated with hemodynamic support. The American journal of emergency medicine. 2022 May:55():117-125. doi: 10.1016/j.ajem.2022.03.007. Epub 2022 Mar 10 [PubMed PMID: 35306438]
Romhilt DW, Doyle M, Sagar KB, Hastillo A, Wolfgang TC, Lower RR, Hess ML. Prevalence and significance of arrhythmias in long-term survivors of cardiac transplantation. Circulation. 1982 Aug:66(2 Pt 2):I219-22 [PubMed PMID: 6177443]
Angsubhakorn N, Anderson M, Akdemir B, Bertog S, Garcia S, Sharma A, Tholakanahalli V, Adabag S. Prevalence and Implications of Junctional Rhythm During Transcatheter Aortic Valve Replacement. Cardiovascular revascularization medicine : including molecular interventions. 2021 May:26():61-62. doi: 10.1016/j.carrev.2020.11.014. Epub 2020 Nov 12 [PubMed PMID: 33203581]
Rodriguez RD, Schocken DD. Update on sick sinus syndrome, a cardiac disorder of aging. Geriatrics. 1990 Jan:45(1):26-30, 33-6 [PubMed PMID: 2403955]
Sanders P, Kistler PM, Morton JB, Spence SJ, Kalman JM. Remodeling of sinus node function in patients with congestive heart failure: reduction in sinus node reserve. Circulation. 2004 Aug 24:110(8):897-903 [PubMed PMID: 15302799]
Kim D, Shinohara T, Joung B, Maruyama M, Choi EK, On YK, Han S, Fishbein MC, Lin SF, Chen PS. Calcium dynamics and the mechanisms of atrioventricular junctional rhythm. Journal of the American College of Cardiology. 2010 Aug 31:56(10):805-12. doi: 10.1016/j.jacc.2010.03.070. Epub [PubMed PMID: 20797495]
Level 3 (low-level) evidenceCools E, Missant C. Junctional ectopic tachycardia after congenital heart surgery. Acta anaesthesiologica Belgica. 2014:65(1):1-8 [PubMed PMID: 24988822]
Di Biase L, Gianni C, Bagliani G, Padeletti L. Arrhythmias Involving the Atrioventricular Junction. Cardiac electrophysiology clinics. 2017 Sep:9(3):435-452. doi: 10.1016/j.ccep.2017.05.004. Epub [PubMed PMID: 28838549]
Tuohy S, Saliba W, Pai M, Tchou P. Catheter ablation as a treatment of atrioventricular block. Heart rhythm. 2018 Jan:15(1):90-96. doi: 10.1016/j.hrthm.2017.08.015. Epub 2017 Aug 18 [PubMed PMID: 28823599]
Antman EM, Wenger TL, Butler VP Jr, Haber E, Smith TW. Treatment of 150 cases of life-threatening digitalis intoxication with digoxin-specific Fab antibody fragments. Final report of a multicenter study. Circulation. 1990 Jun:81(6):1744-52 [PubMed PMID: 2188752]
Level 2 (mid-level) evidenceHauptman PJ, Kelly RA. Digitalis. Circulation. 1999 Mar 9:99(9):1265-70 [PubMed PMID: 10069797]
Kelly RA, Smith TW. Recognition and management of digitalis toxicity. The American journal of cardiology. 1992 Jun 4:69(18):108G-118G; disc. 118G-119G [PubMed PMID: 1626485]
Dobrzynski H, Boyett MR, Anderson RH. New insights into pacemaker activity: promoting understanding of sick sinus syndrome. Circulation. 2007 Apr 10:115(14):1921-32 [PubMed PMID: 17420362]
Level 3 (low-level) evidenceAshraf M, Collier SA. Junctional Ectopic Tachycardia. StatPearls. 2026 Jan:(): [PubMed PMID: 32809686]
Misumi I, Yamakawa M, Harada M, Sato K, Tabira A, Usuku H, Tsujita K. Severe hypotension during junctional rhythm in a patient with multiple cerebral infarcts. Journal of cardiology cases. 2023 Feb:27(2):84-87. doi: 10.1016/j.jccase.2022.10.010. Epub 2022 Oct 29 [PubMed PMID: 36788952]
Level 3 (low-level) evidence