Introduction
Jugular venous pressure assessment is a fundamental component of the cardiovascular physical examination, providing a noninvasive estimate of central venous pressure and right atrial hemodynamics. Despite advances in diagnostic technology, this bedside skill remains clinically valuable, offering immediate insight into volume status and cardiac function without the need for invasive testing. The jugular venous examination is a key element of this assessment, requires careful observation and technique, and is an invaluable tool for assessing the patient's hemodynamic status.[1] When performed correctly, evaluation of the jugular venous pulse and waveform can aid in the diagnosis and prognostication of conditions such as heart failure, where elevated right atrial pressure is reflected in the jugular venous column.[2] Mastery of this examination enhances clinical decision-making and supports timely, patient-centered care.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Anatomy
Accurate assessment of jugular venous distention (JVD) requires an understanding of the anatomy of the jugular veins and their relationship to surrounding neck structures (see Image. Jugular Venous Distention). The jugular veins are central veins that serve as distensible conduits for venous return to the right atrium. Central veins are thin-walled, distensible reservoirs and act as a conduit of blood in continuity with the right atrium. They are divided into the internal jugular vein (IJV) and the external jugular vein (EJV).[3]
The IJV originates from the inferior petrosal and sigmoid sinuses at the base of the skull and exits through the jugular foramen. The IJV courses between the sternal and clavicular heads of the sternocleidomastoid muscle, where it may be identified within the triangular space between these landmarks. The IJV then descends within the carotid sheath, lateral to the carotid artery, and joins the subclavian vein to form the brachiocephalic vein at the base of the neck.[3]
The EJV forms from the posterior auricular vein and the posterior branch of the retromandibular vein behind the angle of the mandible. The EJV runs obliquely across the sternocleidomastoid muscle in the superficial fascia of the neck and drains into the subclavian vein. In contrast to IJV, EJV can be easily visualized but is often not used to measure central venous pressure.[4]
Physiology
The relationship between the IJV and the right atrium is significant because it provides healthcare professionals with a valuable tool during physical examination. The bedside examination of the jugular venous pulse can help assess central venous pressure (CVP), evaluate the contour of the venous pulse, and identify various cardiac pathologies.
Waveforms of jugular venous pulse signify the following:
- a
- Presystolic, produced by right atrial contraction
- c
- Isovolumic phase, bulging of the tricuspid valve into the right atrium during ventricular systole
- v
- Occurs in late systole; increased blood in the right atrium from venous return
- x
- A combination of atrial relaxation, downward movement of the tricuspid valve, and ventricular systole
- y
- The tricuspid valve opens, and the blood flows into the right ventricle.
When these are transmitted to the skin, flickers are visible throughout the overlying skin. Once we have identified the IJV, we must estimate the venous pressure. Normal venous pressure is 1 to 8 cm of water.
Indications
Measurement of jugular venous pressure is an integral component of the cardiovascular examination, although its use may vary across clinical settings and among examiners. This assessment is most commonly used to estimate right atrial pressure, particularly in patients with suspected or known heart failure, and to monitor response to diuretic therapy. Jugular venous pressure evaluation is also useful in assessing conditions such as superior vena cava obstruction, tricuspid valve disease, and pericardial disease.
Equipment
Assessment of jugular venous pressure is a bedside clinical skill that requires minimal equipment. Standard precautions should be observed, including the use of gloves when appropriate. Adequate lighting is essential, and a penlight may be used to visualize venous pulsations better. A centimeter ruler or measuring tape helps estimate the vertical height of the venous column relative to the sternal angle. Proper patient positioning on an adjustable examination bed or stretcher is also necessary to allow for accurate assessment at varying angles of elevation.
Technique or Treatment
Technique
Evaluation of jugular venous pressure involves observing the patient's jugular veins in the neck across varying positions and maneuvers, estimating right atrial pressure, and identifying abnormalities in the jugular venous column. The examiner stands at the right side of the table because the right-sided internal jugular vein connecting to the right brachiocephalic vein is in direct line with the superior vena cava. The left IJV can be used if the right-sided IJV is not visible. The left brachiocephalic vein, which connects the left IJV, crosses the mediastinal structures before draining into the superior vena cava and may be distended when there is partial obstruction of the mediastinal structures.
The patients are initially positioned supine on a bed bent at the hip, so that when the head of the bed is elevated, the head, neck, and thorax are on a similar plane. The head should be slightly tilted away from the examiner (left if examining from the right), and the neck should be in extension with the sternocleidomastoid relaxed. A penlight can help to enhance visualization.
Jugular venous pressure is ideally measured in different planes. The degree of upper body elevation (0°–90°) is the angle at which the venous meniscus can be best appreciated in the neck. When a patient is supine, low venous pressure is apparent; high venous pressure is readily visible when the patient is upright (90°). Recommendations include changing the head of the bed to various angles to assess jugular venous pressure. If venous pressure is seen at the clavicle when the patient is upright, it suggests an elevated jugular venous pressure; when the pressure is very high, it can sometimes be appreciated below the ear.[5]
Jugular venous pressure varies with respiration, with inspiration generally decreasing the pressure. In some patients, it might not decrease or may even increase (eg, a finding called the "Kussmaul sign"). This finding can occur in patients with constructive or effusive pericarditis, restrictive pericarditis, right ventricular infarction, severe right ventricular dysfunction, massive pulmonary embolism, severe tricuspid regurgitation, tricuspid stenosis, and cardiac tamponade.[6]
EJV vs IJV
The EJV is an option when the IJV is inappropriate. After identifying the EJV, the forefinger should be placed above the clavicle on the vein; the venous column gets distended because of the blood coming from cerebral circulation. At this point, a second finger should be used to occlude the vein superiorly to prevent overdistension, and the finger at the clavicle should be released.
Venous pressure is now measured because it approximates the vertical distance between the upper level of the fluid column and the right atrium, which is estimated to be 5 to 6 cm behind the angle of Louis. The IJV can be differentiated from the carotid artery by palpating the radial pulse, where the single upstroke systole coincides. Unlike the carotid pulse, the IJV is not palpable and varies with respiration. The IJV impulse has 3 upstrokes (a, c, and v) and 2 descents (x and y).[4]
Pathological Conditions Associated With Abnormal Waveforms
The 'a' wave is absent in patients with atrial fibrillation because of loss of atrial contraction. A large 'a' wave is present in patients with resistance to atrial contraction, such as pulmonary hypertension, tricuspid stenosis, or right atrial mass or thrombus. Cannon 'a' wave is when the right atrium contracts against a closed tricuspid valve, such as in patients with complete atrioventricular block, premature atrial/ventricular/junctional beat, or ventricular tachycardia.
A large 'v' wave is seen in tricuspid regurgitation when the right ventricle contracts and the tricuspid valve does not completely close, which results in the shooting of blood back to the right atrium. Jugular venous pressure is 1 of the most common and readily available tools for measuring right atrial pressure and can be used to assess volume status, especially in hypervolemic states due to cardiac etiologies. Right atrial pressure is measured by adding the height of the venous column above the angle of Louis to the vertical distance between the sternal angle and the mid-right atrium.
The vertical distance between the sternal angle and the mid-right atrium varies with the patient's position: 5 cm, 8 cm, and 10 cm at 0° (supine), 30°, and 45°, respectively.[7] Generally, 5 cm is used as an approximate measurement, though it may be underestimated when applied to all patients across all head-elevation levels.[7] Hence, right atrial pressure is estimated with the formula: Estimated right atrial pressure (in cm of water) = (jugular venous pressure height) + 5 cm. Some causes of elevated right atrial pressure include right ventricular failure (cardiomyopathy), cor pulmonale, pulmonary hypertension, tricuspid valve disease, constrictive pericarditis, tricuspid valve incompetence, and tricuspid valve stenosis or obstruction.
Clinical Significance
With rapid advances in diagnostic technology, clinicians may place less emphasis on bedside physical examination. Assessment of jugular venous pressure requires careful observation and clinical skill.[8] Jugular venous pressure assessment offers valuable insight into cardiac hemodynamics, particularly in conditions such as heart failure exacerbation, where elevated right atrial pressure is reflected in the jugular venous column.
Jugular venous pressure remains 1 of the most accessible and repeatable methods for estimating CVP. Although measurement can vary between patients, diagnostic accuracy improves with clinical experience. Proficiency in bedside assessment allows for timely diagnosis and prognostication while potentially reducing reliance on invasive testing.
Enhancing Healthcare Team Outcomes
Jugular venous pressure assessment is a key component of the cardiovascular examination and provides a noninvasive estimate of central venous pressure and right atrial hemodynamics. Despite advances in diagnostic technology, reliance on imaging may lead to underuse of this high-yield bedside skill. Elevated jugular venous pressure reflects increased right atrial pressure and is clinically significant in conditions such as heart failure, pulmonary hypertension, and pericardial disease. Careful observation of jugular venous waveforms and height, along with appropriate patient positioning, allows clinicians to assess volume status, guide therapy, and monitor response to treatment. Proficiency in jugular venous pressure evaluation supports timely diagnosis and may reduce reliance on invasive testing.
Interprofessional collaboration enhances the accuracy and application of jugular venous pressure assessment in clinical care. Physicians and advanced practice providers integrate findings into diagnostic and management decisions, while primary care clinicians ensure longitudinal monitoring and follow-up. Nurses play a critical role in patient positioning, observation, and early identification of changes in volume status. Pharmacists assist in optimizing therapies, such as diuretic therapy, and in managing medication-related risks. Effective communication, shared decision-making, and coordinated care improve diagnostic accuracy, guide treatment adjustments, and reduce complications, ultimately supporting patient-centered, high-quality care.
Media
(Click Image to Enlarge)
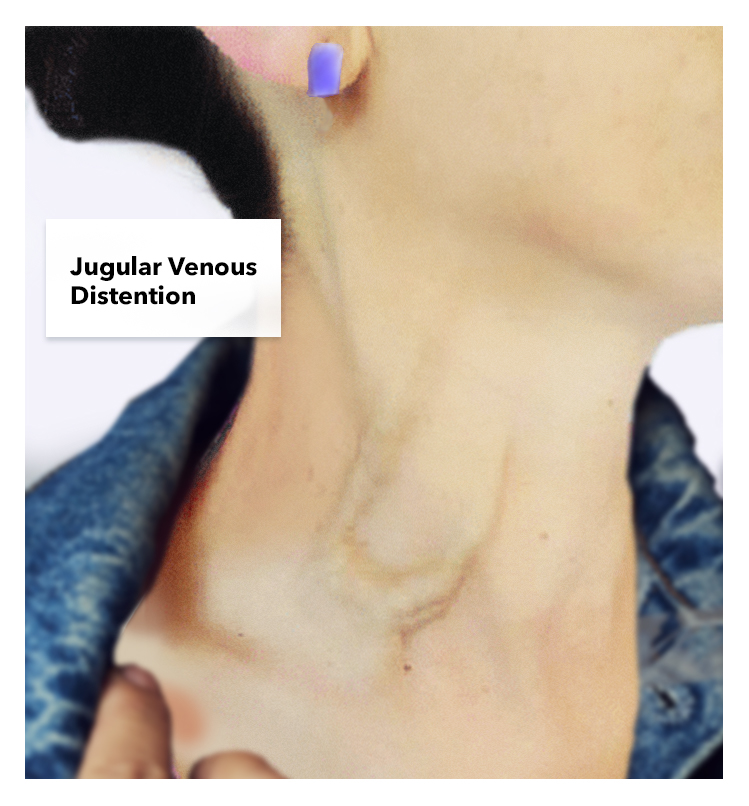
Jugular Venous Distention.
Contributed by K Humphreys
References
Senthelal S, Maingi M. Physiology, Jugular Venous Pulsation. StatPearls. 2026 Jan:(): [PubMed PMID: 30480931]
Kolupoti A, Fudim M, Pandey A, Kucharska-Newton A, Hall ME, Vaduganathan M, Mentz RJ, Caughey MC. Temporal Trends and Prognosis of Physical Examination Findings in Patients With Acute Decompensated Heart Failure: The ARIC Study Community Surveillance. Circulation. Heart failure. 2021 Dec:14(12):e008403. doi: 10.1161/CIRCHEARTFAILURE.121.008403. Epub 2021 Oct 27 [PubMed PMID: 34702047]
Jeon JC, Choi WI, Lee JH, Lee SH. Anatomical Morphology Analysis of Internal Jugular Veins and Factors Affecting Internal Jugular Vein Size. Medicina (Kaunas, Lithuania). 2020 Mar 18:56(3):. doi: 10.3390/medicina56030135. Epub 2020 Mar 18 [PubMed PMID: 32197519]
Rusu MC, Tudose RC, Vrapciu AD, Toader C, Popescu ŞA. Anatomical Variations of the External Jugular Vein: A Pictorial and Critical Review. Medicina (Kaunas, Lithuania). 2023 Mar 21:59(3):. doi: 10.3390/medicina59030622. Epub 2023 Mar 21 [PubMed PMID: 36984623]
Sinisalo J, Rapola J, Rossinen J, Kupari M. Simplifying the estimation of jugular venous pressure. The American journal of cardiology. 2007 Dec 15:100(12):1779-81 [PubMed PMID: 18082526]
Noguchi M, Kasai K, Honda S, Sakai C, Harimoto K, Kawasaki T. Jugular Venous Response for Risk Stratification in Heart Failure. Cureus. 2024 Apr:16(4):e58423. doi: 10.7759/cureus.58423. Epub 2024 Apr 16 [PubMed PMID: 38765383]
Devine PJ, Sullenberger LE, Bellin DA, Atwood JE. Jugular venous pulse: window into the right heart. Southern medical journal. 2007 Oct:100(10):1022-7; quiz 1004 [PubMed PMID: 17943049]
Metkus TS, Kim BS. Bedside Diagnosis in the Intensive Care Unit. Is Looking Overlooked? Annals of the American Thoracic Society. 2015 Oct:12(10):1447-50. doi: 10.1513/AnnalsATS.201505-271OI. Epub [PubMed PMID: 26389653]