 Jessner Lymphocytic Infiltration of the Skin
Jessner Lymphocytic Infiltration of the Skin
Introduction
Jessner lymphocytic infiltration of the skin (JLIS) is a rare, benign cutaneous condition characterized by papular or plaque-like eruptions that typically involve sun-exposed areas, such as the face, neck, and trunk.[1] The eruptions are erythematous, non-scaly, and may also be annular. This disease has an indolent course, lasting weeks to months, and as the eruptions expand peripherally, they can sometimes exhibit central clearing or healing. The eruptions may resolve spontaneously or with medication, without sequelae, but they frequently recur. The lesions are typically asymptomatic, but some patients may experience burning sensations and pruritus.
JLIS is diagnosed by biopsy, which reveals perivascular and periadnexal clusters of plasmacytoid monocytes within the dermis, occasionally extending into the subcutaneous tissue. These cells, also known as plasmacytoid dendritic cells, are integral to the induction of autoimmune diseases and other dermatological conditions.[2] Although their presence, combined with an inappropriate CD8+ T-cell–predominant lymphoid infiltrate, provides a definitive diagnosis of JLIS, the etiology of this disorder remains unknown. Nonetheless, there exists a potential for hereditary and autoimmune components. JLIS, also recognized as benign lymphocytic infiltration of the skin, Jessner-Kanof syndrome, and benign chronic T-cell infiltrative disease, was first documented in 1953 by Max Jessner and Norman Kanof.
JLIS was previously classified under the overarching term "cutaneous lymphoid hyperplasia," which also encompassed lymphocytoma cutis and malignant lymphomas, all of which are skin conditions characterized by lymphocytic infiltrates. There remains debate regarding whether this disease constitutes a distinct entity or is part of a spectrum of cutaneous disorders, including discoid lupus erythematosus, polymorphous light eruption (PLE), and potentially malignant lymphoma.[3][4][5][6][7][8][9] Nonetheless, there is no definitive evidence indicating progression to any of the aforementioned conditions; however, case reports have documented patients with concurrent manifestations.[4]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The etiology of JLIS remains unknown, but numerous potential etiologies have been proposed. There may be a genetic component, as multiple familial cases of the disease have been reported.[10] Another possible etiology is autoimmunity. The presence of plasmacytoid dendritic cells in JLIS may suggest an autoimmune etiology, such as systemic lupus erythematosus (SLE).[2] One hypothesis is that JLIS may be an early cutaneous manifestation of SLE or even a progression of lupus erythematosus timidus.[1][2][3][6] These hypotheses are substantiated by the dermal manifestations of JLIS, erythema multiforme, tinea versicolor, and cutaneous lymphoma observed in patients with anti-HMGCR antibody-positive myopathy (HMGCR-IMNM).[11][12] Suppression of natural killer cell cytolytic activity suggests altered immunoregulatory pathways, similar to those in neoplastic and endocrine disorders.
Further studies report that photosensitivity is a trigger for JLIS, linking the disease to PLE. The typical distribution of eruptions in sun-exposed areas further supports this possible etiology. Drug-induced cases have also been reported, primarily associated with angiotensin-converting enzyme inhibitors and immunosuppressive therapies such as etanercept, ustekinumab, leflunomide, and glatiramer acetate.[13][14][15] Less commonly reported triggers include duloxetine, HIV, and Borrelia burgdorferi infection.[16]
Epidemiology
JLIS is an uncommon condition with unknown incidence and prevalence in the United States and worldwide. The onset of JLIS typically occurs in individuals aged between 30 and 50; however, cases have also been reported in children, albeit less frequently.[17] Although JLIS was initially believed to be more prevalent among males, recent studies indicate no gender bias, and there is no evidence suggesting racial predominance.
Pathophysiology
JLIS was historically regarded as a CD8+ polyclonal reactive skin disorder. The pathophysiology remains largely unknown; however, the prevailing hypothesis involves plasmacytoid dendritic cell–mediated migration of lymphocytes, resulting in an aberrant accumulation of CD8+ T lymphocytes within the dermis. The etiology of the formation of clusters of plasmacytoid dendritic cells in the affected perivascular and periadnexal regions is yet to be elucidated.
Histopathology
Histopathological examination of skin biopsies reveals a normal epidermis without atrophy, follicular plugging, basal vacuolar change, or basement membrane thickening. There are dense superficial and deep perivascular and periadnexal CD8+ T-cell lymphocytic infiltrates within the dermis that sometimes extend into the subcutaneous tissue and can also be perifollicular (see Image. Inflammatory Infiltrate in Jessner's Dermatitis, Mostly of Small Mature Lymphocytes). T cells are typically located more peripherally, whereas B cells expressing follicular center differentiation are found near superficial vessels.[18][19] Perivascular and periadnexal clusters of plasmacytoid monocytes are also present within the dermis.[2]
Plasmacytoid monocytes, also known as plasmacytoid dendritic cells, are larger than lymphocytes with a pale nucleus and a relatively large single nucleolus. These cells are typically scattered throughout the dermis. During active eruptions, circulating immune complex levels increase, but they generally return to normal as the eruption resolves. In addition, natural killer cell cytolytic function is often depressed.[20]
History and Physical
Patients with JLIS typically report asymptomatic, non-scaly, erythematous, solitary or multiple plaques or papules in sun-exposed regions, such as the face, neck, and trunk, persisting for weeks to months.[1] The history may reveal the onset or aggravation of these lesions following sun exposure. The lesions may resolve spontaneously without sequelae and subsequently recur at the same or at previously unaffected sites. Although lesions are generally asymptomatic, some patients may experience burning sensations or pruritus. Given that some case reports suggest a hereditary pattern, a comprehensive history should include inquiry into similar lesions in family members. Additionally, given the suspected autoimmune component, both personal and family histories of autoimmune disease should be evaluated.[5]
On physical examination, lesions are well demarcated and may appear annular or demonstrate peripheral expansion. The surface is non-scaly, showing no evidence of follicular plugging or atrophy. Lesions are typically arranged in crescent-shaped rings, ranging from 2 mm to 2 cm in diameter. A meticulous skin examination is essential because multiple lesions may be present. Commonly affected areas include the malar region of the face and the upper back; however, lesions may also occur on other parts of the body, including the forehead, neck, mastoid region, arms, legs, and trunk.
Evaluation
Basic laboratory investigations, including a complete blood count and urinalysis, are recommended.
Autoimmune Workup
The initial evaluation should include antinuclear antibody (ANA) testing and an erythrocyte sedimentation rate. If results are positive, further assessment for SLE is recommended, including anti-Smith (anti-Sm) and anti–double-stranded DNA (anti-dsDNA) antibodies. Testing for antiphospholipid syndrome should include lupus anticoagulant, anti-cardiolipin, and anti-apolipoprotein antibodies. Assessment for Sjögren syndrome should include anti-Ro and anti-La antibodies. Rheumatoid arthritis assessment should include rheumatoid factor and anti-citrullinated protein antibodies. Evaluation for anti-HMGCR myopathy should include anti-HMGCR antibody testing (antibodies against HMG-CoA reductase), creatine kinase measurement, and liver enzyme testing.[12]
Additional Tests
UVA- and UVB-provocative phototoxicity testing should be considered.[21]
Diagnostic Procedures
Skin biopsy with hematoxylin and eosin staining, direct immunofluorescence, Alcian blue staining (at pH 2.5) for dermal mucin evaluation, and cytological examination.
Treatment / Management
Currently, no definitive therapeutic intervention for JLIS exists. Current management primarily consists of topical corticosteroids such as hydrocortisone, triamcinolone, and betamethasone. In more severe or refractory cases, systemic corticosteroids such as prednisone or antimalarial agents, including hydroxychloroquine, may be used.[4][22] Nonetheless, many patients choose not to pursue treatment for a benign condition, given the significant adverse effects associated with the main pharmacological options.[18](B3)
The initial line of treatment involves topical and intralesional corticosteroids.[22] In cases where photosensitivity is a concern, antimalarial medications may be more effective.[18] Additional therapies reported to be beneficial in case reports include tacrolimus, thalidomide, etretinate, methotrexate, oral auranofin, and proquazone.[17][23][24](B3)
Cosmetic camouflage, photoprotection, and surgical excision of small lesions may help conceal or eliminate the clinical manifestations of the condition. Less frequently used modalities include laser therapy, photodynamic therapy, and cryotherapy.
Differential Diagnosis
JLIS is among a group of histologically characterized conditions characterized by a lymphocytic infiltrate in the dermis. The conditions below, in conjunction with JLIS, are collectively referred to as the 5 L's.[8][20]
- Polymorphous light eruption: The presence of active lesions during the winter months or in regions with limited sun exposure may aid in differentiating JLIS from PLE.
- Discoid lupus erythematosus/lupus erythematosus tumidus: ANA, anti-Sm, and anti-dsDNA antibody testing can help differentiate JLIS from lupus erythematosus tumidus (LET). Due to its autoimmune etiology, LET exhibits a predominance in females. Compared to JLIS, LET demonstrates less truncal involvement. In addition, JLIS may demonstrate a higher proportion of B lymphocytes on biopsy.[7]
- Well-differentiated lymphocytic lymphoma: Lymphoma can involve the bone marrow, whereas JLIS is restricted to the skin.
- Lymphocytoma cutis: Lymphocytoma cutis typically demonstrates a polyclonal B-cell infiltrate.[25]
Other differential diagnoses include:
Prognosis
As a benign condition that may resolve spontaneously without residual sequelae, JLIS has an excellent prognosis and is not associated with increased mortality.
Complications
Misdiagnosis
JLIS may be misdiagnosed because it can resemble other dermatological conditions, particularly benign entities such as LET or PLE. JLIS may also be erroneously diagnosed as a malignancy, such as cutaneous lymphoma, which is a more serious condition requiring distinct therapeutic interventions.
Ectropion
Lesions surrounding the eyes may lead to ectropion, defined as the outward rotation of the lower eyelid. This condition can increase the risk of surgical failure in patients undergoing corrective procedures.[28][29]
Adverse Effects of Treatment
Therapeutic interventions for JLIS may entail adverse effects; for instance, the use of topical steroids may cause skin atrophy. Additionally, sunscreen use is recommended for patients with JLIS, as photosensitivity may be a trigger.
Co-occurrence With Other Conditions
A subset of patients may concurrently develop JLIS and PLE, along with other skin conditions such as psoriasis, or may experience alternating periods of both conditions.[24] Furthermore, patients with anti-HMGCR antibody-positive myopathy (HMGCR-IMNM) may present with multiple dermal manifestations, including JLIS, erythema multiforme, tinea versicolor, and cutaneous lymphoma.[11][12][19]
Consultations
JLIS may benefit from a multidisciplinary approach. A dermatologist is recommended, and a plastic surgeon should be involved for cosmetic camouflage. If autoimmune testing yields positive results, consultation with a rheumatologist is advisable.
Deterrence and Patient Education
As the etiology remains unknown, there are no established preventive measures for JLIS. Nonetheless, given that photosensitivity may be a trigger for JLIS, patients are strongly advised to avoid sun exposure and to use effective photoprotection measures. Given the risk of ectropion, patients presenting with periorbital lesions should be subjected to close clinical monitoring.
Finally, patients receiving medical therapy, including topical steroids and antimalarials, should attend regular follow-up appointments to enable early detection and management of adverse effects, such as skin atrophy.
Enhancing Healthcare Team Outcomes
The most critical aspects of managing JLIS are accurate diagnosis and treatment. Although JLIS is a rare, benign condition with a generally favorable prognosis, identification of a lesion requires careful evaluation to rule out more serious conditions, such as lymphoma.[5] Diagnosis begins with a dermatologist performing a biopsy, after which the tissue specimen is processed and analyzed by a pathologist, laboratory technologists, and supporting staff using immunohistologic techniques to confirm the condition.[25]
Comprehensive care requires close collaboration among the patient, caregivers, and a multidisciplinary healthcare team. This team may include a rheumatologist if an autoimmune component is suspected. Moreover, when multiple family members are affected, it is advisable to counsel the entire family regarding the potential genetic predisposition to the disease.[10]
Once JLIS is diagnosed, it is essential to educate the patient about available treatment options, taking into account risk factors such as photosensitivity, and to encourage shared decision-making in developing a treatment strategy tailored to their individual needs. Patients should also be informed that treatment may not be effective for all individuals and that outcomes can vary.[4][21]
Depending on the treatment plan, consultation with a plastic surgeon may be warranted. Effective management of this condition requires clear communication among all members of the interprofessional team. For patients receiving medical therapy, close monitoring for adverse effects is recommended. Furthermore, patients diagnosed with JLIS should undergo regular skin examinations coordinated among the patient, caregivers, primary care providers, dermatologists, and other relevant healthcare professionals involved in patient care. Particular attention should be given to periorbital lesions, as these may progress to ectropion.[28]
Media
(Click Image to Enlarge)
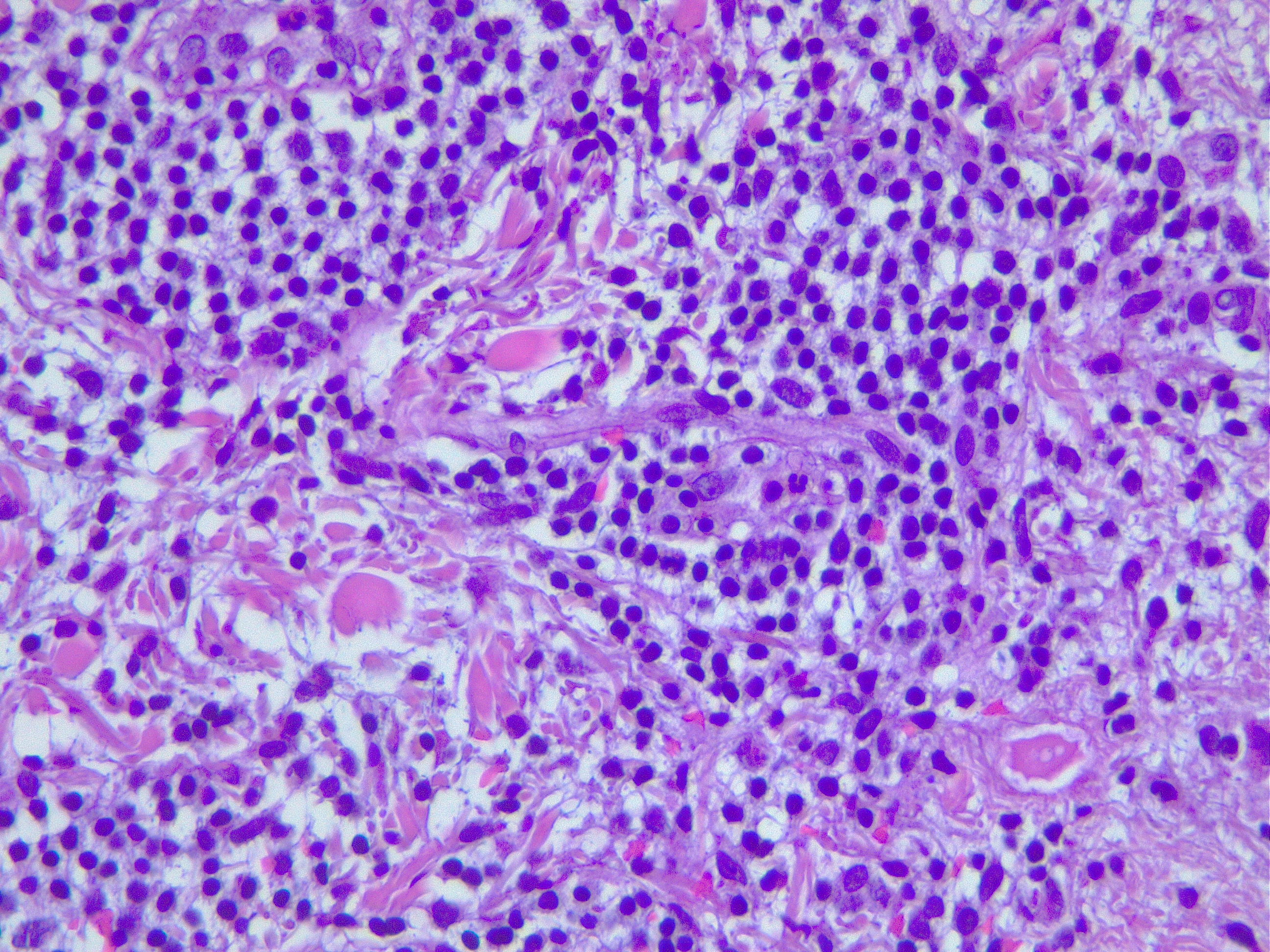
Inflammatory infiltrate in Jessner's dermatitis, mostly of small mature lymphocytes. Contributed by Fabiola Farci, MD
References
Poenitz N, Dippel E, Klemke CD, Qadoumi M, Goerdt S. Jessner's lymphocytic infiltration of the skin: a CD8+ polyclonal reactive skin condition. Dermatology (Basel, Switzerland). 2003:207(3):276-84 [PubMed PMID: 14571070]
Level 2 (mid-level) evidenceTomasini D, Mentzel T, Hantschke M, Cerri A, Paredes B, Rütten A, Schärer L, Kutzner H. Plasmacytoid dendritic cells: an overview of their presence and distribution in different inflammatory skin diseases, with special emphasis on Jessner's lymphocytic infiltrate of the skin and cutaneous lupus erythematosus. Journal of cutaneous pathology. 2010 Nov:37(11):1132-9. doi: 10.1111/j.1600-0560.2010.01587.x. Epub [PubMed PMID: 20659210]
Level 3 (low-level) evidenceKonttinen YT, Reitamo S, Ranki A, Segerberg-Konttinen M. T lymphocytes and mononuclear phagocytes in the skin infiltrate of systemic and discoid lupus erythematosus and Jessner's lymphocytic infiltrate. The British journal of dermatology. 1981 Feb:104(2):141-5 [PubMed PMID: 6971117]
Toonstra J, Wildschut A, Boer J, Smeenk G, Willemze R, van der Putte SC, Boonstra H, van Vloten WA. Jessner's lymphocytic infiltration of the skin. A clinical study of 100 patients. Archives of dermatology. 1989 Nov:125(11):1525-30 [PubMed PMID: 2684021]
Lipsker D, Mitschler A, Grosshans E, Cribier B. Could Jessner's lymphocytic infiltrate of the skin be a dermal variant of lupus erythematosus? An analysis of 210 cases. Dermatology (Basel, Switzerland). 2006:213(1):15-22 [PubMed PMID: 16778421]
Level 2 (mid-level) evidenceRémy-Leroux V, Léonard F, Lambert D, Wechsler J, Cribier B, Thomas P, Adamski H, Marguery MC, Aubin F, Leroy D, Bernard P. Comparison of histopathologic-clinical characteristics of Jessner's lymphocytic infiltration of the skin and lupus erythematosus tumidus: Multicenter study of 46 cases. Journal of the American Academy of Dermatology. 2008 Feb:58(2):217-23 [PubMed PMID: 18083273]
Level 2 (mid-level) evidenceAkasu R, Kahn HJ, From L. Lymphocyte markers on formalin-fixed tissue in Jessner's lymphocytic infiltrate and lupus erythematosus. Journal of cutaneous pathology. 1992 Feb:19(1):59-65 [PubMed PMID: 1556268]
Pereira A, Ferrara G, Calamaro P, Cota C, Massone C, Boggio F, Prieto-Torres L, Cerroni L. The Histopathological Spectrum of Pseudolymphomatous Infiltrates in Cutaneous Lupus Erythematosus. The American Journal of dermatopathology. 2018 Apr:40(4):247-253. doi: 10.1097/DAD.0000000000000942. Epub [PubMed PMID: 28654469]
Camisa C Sr, Papavero V. Lupus Erythematosus Tumidus as a Distinct Uncommon Subtype of Cutaneous Lupus Erythematosus: A Case Report and Review. Cureus. 2024 Apr:16(4):e59140. doi: 10.7759/cureus.59140. Epub 2024 Apr 27 [PubMed PMID: 38803774]
Level 3 (low-level) evidenceAshworth J, Morley WN. Jessner and Kanof's lymphocytic infiltration of the skin: a familial variant. Dermatologica. 1988:177(2):120-2 [PubMed PMID: 3169334]
Level 3 (low-level) evidenceKurashige T, Nakamura R, Murao T, Mine N, Sato M, Katsumata R, Kanaya Y, Dodo Y, Sugiura T, Ohshita T. Atypical skin conditions of the neck and back as a dermal manifestation of anti-HMGCR antibody-positive myopathy. BMC immunology. 2024 May 11:25(1):30. doi: 10.1186/s12865-024-00622-2. Epub 2024 May 11 [PubMed PMID: 38734636]
Prenner J, Choi E, Kim YJ, Zheng L, Nguyen CV. Jessner Lymphocytic Infiltrate in Anti-HMGCR Myopathy. JAMA dermatology. 2025 Feb 1:161(2):227-228. doi: 10.1001/jamadermatol.2024.5266. Epub [PubMed PMID: 39714826]
Abbad N, Lanal T, Brenuchon C, Morel G, Deprez X. Etanercept-Induced Lymphocytic Infiltration of Jessner-Kanof. Arthritis & rheumatology (Hoboken, N.J.). 2018 Mar:70(3):449. doi: 10.1002/art.40347. Epub 2018 Jan 10 [PubMed PMID: 29024536]
Guarneri C, Lentini M, Polimeni G, Giuffrida R, Cannavò SP. Ustekinumab-induced drug eruption resembling lymphocytic infiltration (of Jessner-Kanof) and lupus erythematosus tumidus. British journal of clinical pharmacology. 2016 Apr:81(4):792-4. doi: 10.1111/bcp.12837. Epub 2015 Dec 29 [PubMed PMID: 26616890]
Sparsa L, Afif N, Goetz J, Sordet C, Chatelus E, Lipsker D, Sibilia J. Jessner-Kanof disease induced by leflunomide: a dermal variant of cutaneous lupus? Rheumatology international. 2011 Feb:31(2):255-8. doi: 10.1007/s00296-009-1169-z. Epub 2009 Oct 13 [PubMed PMID: 19823837]
Level 3 (low-level) evidenceDemirbaş A, Çelik ZE. Jessner's lymphocytic infiltration as a symptom of Immune Reconstitution Inflammatory Syndrome in an HIV-infected patient: A case report. Dermatologic therapy. 2020 Jul:33(4):e13637. doi: 10.1111/dth.13637. Epub 2020 Jun 2 [PubMed PMID: 32436645]
Level 3 (low-level) evidencePetersen MP, Vestergaard V, Bygum A. Jessner lymphocytic infiltration - rare in childhood. Dermatology online journal. 2017 Oct 15:23(10):. pii: 13030/qt04f7b3xq. Epub 2017 Oct 15 [PubMed PMID: 29469790]
Higgins CR, Wakeel RA, Cerio R. Childhood Jessner's lymphocytic infiltrate of the skin. The British journal of dermatology. 1994 Jul:131(1):99-101 [PubMed PMID: 8043427]
Level 3 (low-level) evidenceKurashige T. Anti-HMGCR myopathy: clinical and histopathological features, and prognosis. Current opinion in rheumatology. 2021 Nov 1:33(6):554-562. doi: 10.1097/BOR.0000000000000832. Epub [PubMed PMID: 34456255]
Level 3 (low-level) evidenceBraddock SW, Kay HD, Maennle D, McDonald TL, Pirruccello SJ, Masih A, Klassen LW, Sawka AR. Clinical and immunologic studies in reticular erythematous mucinosis and Jessner's lymphocytic infiltrate of skin. Journal of the American Academy of Dermatology. 1993 May:28(5 Pt 1):691-5 [PubMed PMID: 8496412]
Level 3 (low-level) evidenceAdamski H, Labrousse AL, Sparsa A, Leonard F, Le Gall F, Labrousse F, Ollivier I, Bonnetblanc JM, Chevrant-Breton J, Bedane C, Bernard P. [Positive photobiological investigation in Jessner's lymphocytic infiltration of the skin]. Annales de dermatologie et de venereologie. 2002 Dec:129(12):1370-3 [PubMed PMID: 12536173]
Level 3 (low-level) evidenceSánchez CE, Cabezas MDC, Narváez S, Jaramillo H, Miño C. Jessner's Lymphocytic Infiltration of the Skin in a 73-Year-Old Woman: A Case Report. The American journal of case reports. 2023 Apr 24:24():e938969. doi: 10.12659/AJCR.938969. Epub 2023 Apr 24 [PubMed PMID: 37088972]
Level 3 (low-level) evidenceChen J, Kerkemeyer KLS, Ross C, Ly H. A case of treatment-resistant Jessner's lymphocytic infiltrate responsive to oral auranofin. The Australasian journal of dermatology. 2022 Nov:63(4):e390-e392. doi: 10.1111/ajd.13899. Epub 2022 Jul 25 [PubMed PMID: 35877178]
Level 3 (low-level) evidenceTabanelli M, Baraldi C, Zago S, Patrizi A, Savoia F. A case of psoriasis associated with lymphocytic infiltration of Jessner-Kanof successfully treated with methotrexate monotherapy and subsequently with etanercept monotherapy. Italian journal of dermatology and venereology. 2022 Aug:157(4):384-385. doi: 10.23736/S2784-8671.21.07175-9. Epub [PubMed PMID: 35916187]
Level 3 (low-level) evidenceRalfkiaer E, Lange Wantzin G, Mason DY, Stein H, Thomsen K. Characterization of benign cutaneous lymphocytic infiltrates by monoclonal antibodies. The British journal of dermatology. 1984 Dec:111(6):635-45 [PubMed PMID: 6391533]
Yi LG, Gru AA. Primary Cutaneous CD4-Positive Small/Medium T-Cell Lymphoproliferative Disorder Mimicking Jessner Lymphocytic Infiltrate and Tumid Lupus-A Report of Two Cases. The American Journal of dermatopathology. 2021 Dec 1:43(12):e293-e297. doi: 10.1097/DAD.0000000000001982. Epub [PubMed PMID: 34001748]
Level 3 (low-level) evidenceLi L, Wang Y, Gu H. Mimicking Rosacea? Jessner's Lymphocytic Infiltration of the Skin: A Case Report. Clinical, cosmetic and investigational dermatology. 2024:17():847-851. doi: 10.2147/CCID.S452008. Epub 2024 Apr 13 [PubMed PMID: 38633469]
Level 3 (low-level) evidenceAwotesu S, Dubois V, El-Hindy N, Watts M. Jessner's lymphocytic infiltrate: a rare cause of lid ectropion. BMJ case reports. 2010:2010():. pii: bcr07.2009.2064. doi: 10.1136/bcr.07.2009.2064. Epub 2010 Feb 19 [PubMed PMID: 22347890]
Level 3 (low-level) evidenceSugioka K, Hayashi A, Ichishi M, Sugimoto Y, Habe K, Yamanaka K. Three Cases of Lymphocytic Infiltration of the Eyelid. Dermatopathology (Basel, Switzerland). 2021 May 8:8(2):124-129. doi: 10.3390/dermatopathology8020018. Epub 2021 May 8 [PubMed PMID: 34066876]
Level 3 (low-level) evidence