Introduction
Intussusception occurs when a segment of bowel telescopes into an adjacent segment, causing an obstruction and, in severe cases, intestinal ischemia (see Image. Intussusception of Small Bowel). This process can lead to multiple complications such as bowel obstruction, bowel necrosis, and sepsis. The disease process is much more common in the pediatric population and often resolves with nonoperative management. This condition is characterized by the triad of abdominal pain, a palpable mass, and "red currant jelly" stool." Intussusception is less common in adults, accounting for only 1% to 5% of bowel obstructions. When present in adults, it is likely due to a pathological lead point such as a neoplasm.[1][2]
Intussusception in adults is a challenging diagnosis that requires a high index of suspicion, as symptoms are nonspecific. Assessment and management of abdominal pain primarily depend on the severity of signs and symptoms during evaluation. History, physical examination, and laboratory values can aid the process, but imaging is usually required to establish the diagnosis. Intussusception is also challenging in adults because it can mimic many other diagnoses.[3] If not diagnosed properly, this condition can cause severe complications that can lead to poor patient outcomes. Definitive treatment is surgical intervention, and patient outcomes depend on timely diagnosis and the recruitment of an interprofessional team comprising clinicians, nurses, and technicians. This activity focuses on an in-depth understanding of this rare yet life-threatening emergency.[4]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Intussusceptions are classified as benign or malignant based on their etiology. In adults, more than 90% of cases have a pathological lead point, most commonly a neoplasm.[5][6] Benign causes are typically in the small intestine and include a Meckel diverticulum, lipomas, lymphoid hyperplasia, hemangiomas, adhesions, or adenomas associated with Peutz-Jeghers syndrome. Malignant causes include metastasis, adenocarcinoma, gastrointestinal stromal tumor, lymphoma, leiomyosarcoma, and neuroendocrine tumors. Other etiologies include iatrogenic causes such as catheter placement or gastrojejunostomy.[7]
Epidemiology
Intussusception in adults is extremely rare, found in less than 1 in 1300 abdominal operations. Children are affected more than adults, with an approximate 20:1 ratio. Intussusception represents 1% of small bowel obstructions in adults, with the most common cause being a tumor.[8]
Pathophysiology
Intussusception is a condition involving part of the intestine folding into the section adjacent to it. Part of the proximal bowel (intussusceptum) slides into the adjacent distal section (intussuscipiens) and can cause bowel obstruction as well as intestinal ischemia. The mesentery may or may not be involved. The blood supply to the affected bowel is compressed due to impaired peristalsis, leading to bowel obstruction and gangrene if not treated. Perforation and sepsis can occur from a segment of intestine becoming necrotic secondary to ischemia.[1]
Nonspecific abdominal pain is the most common symptom in adults. Patients may also present with vomiting (can be bilious), bloating, or even bloody stool.[9][10][11] This condition may also result in small- or large-bowel obstruction. In adults, symptoms can be acute, intermittent, or chronic, which complicates diagnosis.[12] The most common site of an intussusception is the ileocecal junction and involves a freely moving segment of bowel with a fixed retroperitoneal structure. The adult intussusception is generally divided into four main categories based on the site of the origin:
- Enteroenteric: involving the small bowel
- Ileocolic: terminal ileum telescoping into the ascending colon
- Ileocecal: the ileocecal valve is the lead point
- Colocolic: involving the large bowel [1]
Histopathology
Histopathology does not play a role in the diagnosis of intussusception. However, histopathology is important in determining the etiology in cases with a pathological lead point, such as a neoplasm.
History and Physical
Although relevant, the history and physical examination are variable in adults. The most common presenting symptom is abdominal pain in over 80% of affected adults.[1] However, the classic triad of abdominal pain, bloody currant-jelly stools, and a palpable, tender abdominal mass seen in children is uncommon in adults. Adults may present with chronic and intermittent abdominal cramping associated with nonspecific abdominal symptoms such as nausea, vomiting, gastrointestinal bleeding, abdominal distention, or constipation.[13]
Evaluation
Abdominal computed tomography (CT) appears to be the most sensitive diagnostic method in making a preoperative diagnosis of adult intussusception, especially in patients presenting with nonspecific abdominal pain.[14][15] However, plain abdominal radiography is often the first diagnostic imaging modality, as most patients present with obstructive symptoms. Upper gastrointestinal studies may demonstrate a "stacked coin" or "coil-spring" appearance. On barium enema, a "cup-shaped" filling defect, "spiral" appearance, or "coil-spring" appearance is characteristically seen in patients with colocolic or ileocolic intussusceptions.[11]
Ultrasonography of the abdomen has lower sensitivity for detecting adult intussusception than abdominal CT. Still, this modality can identify the characteristic "target" sign in the transverse view or the "pseudo-kidney" sign in the longitudinal view, especially in patients presenting with a palpable abdominal mass, where it is more than 90% sensitive.[4][5][11][15] Ultrasound has several disadvantages, including the masking of identifiable features by gas-filled bowel loops and operator dependency.[16][17][18]
The cardinal features on abdominal CT include a "target"- or "sausage"-shaped soft-tissue mass with a layering effect. Visualization of mesenteric vessels within the bowel lumen may also be seen. Abdominal CT can define the location and nature of the mass, its proximity to surrounding structures, and staging in cases of suspected malignancy. Abdominal CT can also determine whether there is a lead point (features suggestive of proximal bowel obstruction).[11] Endoscopy plays a limited role in the diagnosis of adult intussusception. In patients presenting with subacute or chronic large bowel obstruction, lower endoscopy can confirm the intussusception, localize the disease, and identify the lead point.[11]
Treatment / Management
Adult intussusception typically necessitates surgical intervention because of the high incidence of an associated malignancy.[19] However, spontaneous resolution of intussusception without lead points has been reported. A selective approach to resection in adult intussusception has been recommended. Due to the high association with a malignancy, resection without reduction has been recommended whenever possible in ileocolic, colocolic, and ileocecal intussusception. A formal resection using appropriate oncologic techniques should be performed.[15] (B2)
Manipulation and reduction of intussuscepted bowel carry risks, including intraluminal seeding and dissemination of tumor cells, perforation and release of microorganisms into the peritoneal cavity, and an increased risk of anastomotic complications. Reduction should not be attempted in cases of inflammation or bowel ischemia.[11][15][20] In small bowel intussusceptions, reduction should be attempted unless bowel ischemia is present.[15] Laparoscopy can be successfully used in selected cases, depending on the patient's clinical condition and the availability of laparoscopic expertise.[11](B3)
Differential Diagnosis
In adults, the nonspecific symptoms and clinical presentation lead to a wide differential diagnosis. Differential diagnoses include:
- Volvulus
- Small bowel obstruction
- Large bowel obstruction
- Peptic ulcer disease
- Mesenteric ischemia
- Constipation
- Inflammatory bowel disease
- Irritable bowel syndrome
- Diverticulitis
- Diverticulosis
- Appendicitis
- Crohn disease
- Cystic fibrosis
- Ovarian torsion
- Tubo-ovarian abscess
- Fibroids
- Pelvic inflammatory disease
- Pyelonephritis
- Ileus
- Meckel diverticulum
- Foreign bodies [18][21]
Surgical Oncology
Adult intussusception is associated with an identifiable cause in approximately 90% of cases. Benign or malignant neoplasms account for two-thirds of all cases, with more than 50% malignant.[21] The presence of anemia and colonic intussusception is an independent predictor of malignancy.[21][22]
Malignancy is a leading cause of intussusception, with metastatic disease the most common cause. Malignant causes of small bowel intussusception include leiomyosarcomas, adenocarcinoma, gastrointestinal stromal tumors, carcinoid tumors, neuroendocrine tumors, and lymphomas. Colonic intussusception is more likely to have a malignant lead point. Common malignant causes of malignant colonic intussusception include adenocarcinoma, sarcoma, and lymphoma.[21]
Due to the increased incidence of an underlying malignancy in colonic intussusception and the inability to distinguish a malignant from a benign etiology preoperatively or intraoperatively, primary resection without reduction of the intussusception is recommended. Reduction of intussusceptions with a malignant lead point has a theoretical risk of intraluminal seeding of malignant cells and venous embolization.[21][22][18] Standard oncological principles should be applied to resect an unreduced intussusception, including lymphadenectomy of major draining vessels and resection of at least 12 lymph nodes to facilitate accurate diagnosis and future chemotherapeutic intervention.[21]
Prognosis
The prognosis is generally favorable, depending on the etiology of the intussusception. The rarity of this disease, diagnostic delays, and the prevalence of malignancy can lead to severe complications that can have high mortality rates.[23] Prognosis is worse in small bowel intussusceptions associated with metastatic disease.[13]
Transient cases of adult intussusception have been reported. The results of a retrospective analysis demonstrated that intussusceptions less than 4 cm in length were more likely to respond to conservative management. Intussusceptions greater than 9.6 cm were more likely to require surgical exploration.[24]
Complications
Given the high probability of a delay in diagnosis due to vague complaints and an extensive differential diagnosis, intussusception has the potential for life-threatening complications. Complications include superficial wound infections, bowel obstruction, bowel necrosis, perforation, septic shock, pneumonia, and severe organ failure.[13][18][23] Mortality rates are more severe depending on the etiology of the intussusception and when the diagnosis is delayed.[23] Mortality rates range from 0% to 5%.[18][23][25]
Deterrence and Patient Education
Deterrence and patient education for adult intussusception emphasize early symptom recognition, risk mitigation, and strict follow-up to prevent delayed diagnosis and serious complications. Because adult intussusception is uncommon and frequently associated with a pathological lead point—such as malignancy, benign tumors, postoperative adhesions, or inflammatory bowel disease—patients should be counseled that recurrent or intermittent crampy abdominal pain, nausea, vomiting, gastrointestinal bleeding, or obstructive symptoms require prompt medical evaluation rather than observation. Education should reinforce that even episodic symptoms may represent a surgically significant condition, as delays in care increase the risk of bowel ischemia, perforation, and sepsis.
Postoperatively, patients must receive clear education on reporting new or worsening abdominal symptoms, adhering to lifestyle and dietary modifications appropriate to their underlying condition, and performing proper wound care when indicated. When bowel resection is not undertaken, clinicians should stress the importance of mandatory, close postoperative follow-up with interval evaluation and imaging as indicated, given a documented recurrence rate of up to 6.5%.[26] Counseling should also include adherence to surveillance strategies for underlying gastrointestinal disease, including malignancy screening when appropriate. This comprehensive, proactive education strategy supports early detection of recurrence, improves patient safety, and reduces morbidity through timely reintervention.
Pearls and Other Issues
Pearls and other issues on intussusception include the following:
- Adult intussusception is a rare diagnosis that requires strong clinical suspicion. Delay in management can have severe consequences for the patient.
- Early diagnosis and treatment are essential to reducing poor patient outcomes.
- CT imaging is the modality of choice for diagnosis.
- Most cases of adult intussusception involve a pathological lead point.
- Surgical intervention is the definitive treatment, as most cases have a pathological lead point and are associated with a malignancy.
Enhancing Healthcare Team Outcomes
Optimal management of adult intussusception requires a coordinated, interprofessional approach that integrates diagnostic precision, timely surgical decision-making, and longitudinal patient engagement. Clinicians (particularly emergency clinicians), general surgeons, and gastroenterologists must maintain a high index of suspicion for intussusception in adults presenting with nonspecific or intermittent abdominal symptoms, recognizing the strong association with an underlying pathological lead point, frequently malignancy. Radiologists play a pivotal role by promptly interpreting contrast-enhanced computed tomography scans to confirm the diagnosis, assess bowel viability, and identify potential lead points, thereby directly informing the operative strategy. Advanced practitioners support early risk stratification, ensure rapid surgical consultation, and assist with perioperative planning, while reinforcing adherence to evidence-based pathways that prioritize patient safety and timely intervention.
Nurses and pharmacists are essential to optimizing perioperative and postoperative outcomes through vigilant monitoring, patient education, and medication management. Nursing staff contribute to the early detection of clinical deterioration, bowel ischemia, or postoperative complications, and provide clear education on symptom reporting, wound care, dietary modifications, and the importance of close follow-up, given the documented recurrence risk. Pharmacists enhance safety by guiding appropriate analgesia, antimicrobial stewardship, venous thromboembolism prophylaxis, and medication reconciliation, particularly in older patients with complex comorbidities. Effective interprofessional communication, through structured handoffs, multidisciplinary rounds, and shared documentation, ensures alignment on operative findings, pathology results, and follow-up plans. Coordinated team performance across the continuum of care supports patient-centered decision-making, reduces delays in diagnosis or treatment, and improves outcomes in this uncommon but high-risk surgical condition.
Media
(Click Image to Enlarge)
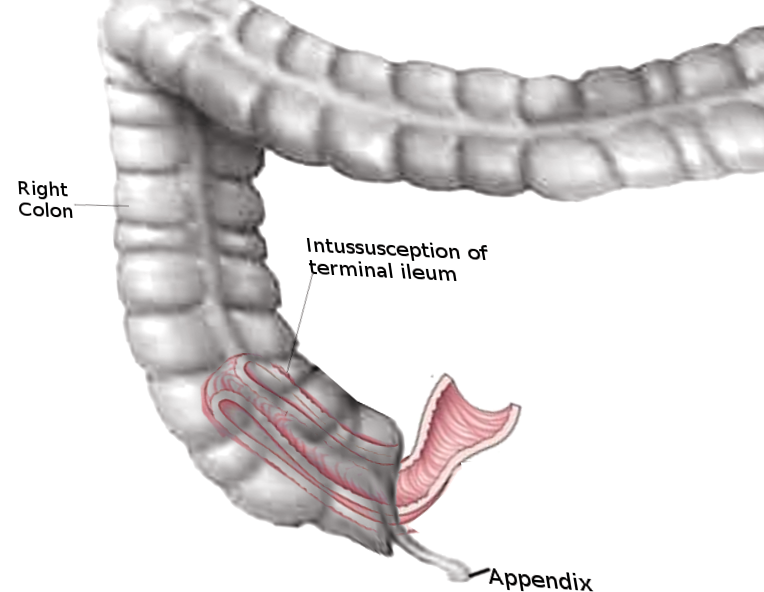
Intussusception of Small Bowel. Intussusception occurs when a segment of bowel telescopes into an adjacent segment, causing an obstruction and, in severe cases, intestinal ischemia.
Contributed by O Chaigasame, MD
References
T Chand J, R R, Ganesh MS. Adult intussusception: a systematic review of current literature. Langenbeck's archives of surgery. 2024 Jul 31:409(1):235. doi: 10.1007/s00423-024-03429-2. Epub 2024 Jul 31 [PubMed PMID: 39085533]
Level 1 (high-level) evidenceHeersche S, Hirt J, Butti F, Hübner M, Hahnloser D, Joliat GR, Grass F. Intestinal Intussusception in Adults: A Systematic Review. World journal of surgery. 2025 Oct:49(10):2706-2716. doi: 10.1002/wjs.70055. Epub 2025 Aug 19 [PubMed PMID: 40831154]
Level 1 (high-level) evidenceMatulich J, Thurston K, Galvan D, Misra S. A case of carcinoid likely causing jejunal intussusception. Case reports in surgery. 2014:2014():949020. doi: 10.1155/2014/949020. Epub 2014 Mar 16 [PubMed PMID: 24757572]
Level 3 (low-level) evidenceAydin N, Roth A, Misra S. Surgical versus conservative management of adult intussusception: Case series and review. International journal of surgery case reports. 2016:20():142-6. doi: 10.1016/j.ijscr.2016.01.019. Epub 2016 Jan 22 [PubMed PMID: 26859872]
Level 2 (mid-level) evidenceEisen LK, Cunningham JD, Aufses AH Jr. Intussusception in adults: institutional review. Journal of the American College of Surgeons. 1999 Apr:188(4):390-5 [PubMed PMID: 10195723]
Level 2 (mid-level) evidenceLotfollahzadeh S, Kashyap S, Tsoris A, Recio-Boiles A, Babiker HM. Rectal Cancer. StatPearls. 2025 Jan:(): [PubMed PMID: 29630254]
González-Carreró Sixto C, Baleato-González S, García Palacios JD, Sánchez Bernal S, Junquera Olay S, Bravo González M, García Figueiras R. Intestinal intussusception in adults: Location, causes, symptoms, and therapeutic management. Radiologia. 2023 May-Jun:65(3):213-221. doi: 10.1016/j.rxeng.2022.10.005. Epub [PubMed PMID: 37268363]
Jain S, Haydel MJ. Child Intussusception. StatPearls. 2025 Jan:(): [PubMed PMID: 28613732]
Yalamarthi S, Smith RC. Adult intussusception: case reports and review of literature. Postgraduate medical journal. 2005 Mar:81(953):174-7 [PubMed PMID: 15749793]
Level 3 (low-level) evidenceWang LT, Wu CC, Yu JC, Hsiao CW, Hsu CC, Jao SW. Clinical entity and treatment strategies for adult intussusceptions: 20 years' experience. Diseases of the colon and rectum. 2007 Nov:50(11):1941-9 [PubMed PMID: 17846839]
Level 2 (mid-level) evidenceMarinis A, Yiallourou A, Samanides L, Dafnios N, Anastasopoulos G, Vassiliou I, Theodosopoulos T. Intussusception of the bowel in adults: a review. World journal of gastroenterology. 2009 Jan 28:15(4):407-11 [PubMed PMID: 19152443]
Lianos G, Xeropotamos N, Bali C, Baltoggiannis G, Ignatiadou E. Adult bowel intussusception: presentation, location, etiology, diagnosis and treatment. Il Giornale di chirurgia. 2013 Sep-Oct:34(9-10):280-3 [PubMed PMID: 24629817]
Lu T, Chng YM. Adult intussusception. The Permanente journal. 2015 Winter:19(1):79-81. doi: 10.7812/TPP/14-125. Epub [PubMed PMID: 25663210]
Level 3 (low-level) evidenceGayer G, Zissin R, Apter S, Papa M, Hertz M. Pictorial review: adult intussusception--a CT diagnosis. The British journal of radiology. 2002 Feb:75(890):185-90 [PubMed PMID: 11893645]
Takeuchi K, Tsuzuki Y, Ando T, Sekihara M, Hara T, Kori T, Kuwano H. The diagnosis and treatment of adult intussusception. Journal of clinical gastroenterology. 2003 Jan:36(1):18-21 [PubMed PMID: 12488701]
Hurwitz LM, Gertler SL. Colonoscopic diagnosis of ileocolic intussusception. Gastrointestinal endoscopy. 1986 Jun:32(3):217-8 [PubMed PMID: 3721141]
Level 3 (low-level) evidenceFujii Y, Taniguchi N, Itoh K. Intussusception induced by villous tumor of the colon: sonographic findings. Journal of clinical ultrasound : JCU. 2002 Jan:30(1):48-51 [PubMed PMID: 11807856]
Level 3 (low-level) evidenceYakan S, Caliskan C, Makay O, Denecli AG, Korkut MA. Intussusception in adults: clinical characteristics, diagnosis and operative strategies. World journal of gastroenterology. 2009 Apr 28:15(16):1985-9 [PubMed PMID: 19399931]
Level 2 (mid-level) evidenceAzar T, Berger DL. Adult intussusception. Annals of surgery. 1997 Aug:226(2):134-8 [PubMed PMID: 9296505]
Level 2 (mid-level) evidenceWeilbaecher D, Bolin JA, Hearn D, Ogden W 2nd. Intussusception in adults. Review of 160 cases. American journal of surgery. 1971 May:121(5):531-5 [PubMed PMID: 5557762]
Level 3 (low-level) evidenceMarsicovetere P, Ivatury SJ, White B, Holubar SD. Intestinal Intussusception: Etiology, Diagnosis, and Treatment. Clinics in colon and rectal surgery. 2017 Feb:30(1):30-39. doi: 10.1055/s-0036-1593429. Epub [PubMed PMID: 28144210]
Goh BK, Quah HM, Chow PK, Tan KY, Tay KH, Eu KW, Ooi LL, Wong WK. Predictive factors of malignancy in adults with intussusception. World journal of surgery. 2006 Jul:30(7):1300-4 [PubMed PMID: 16773257]
Traoré D, Sissoko F, Ongoïba N, Traoré I, Traoré AK, Koumaré AK. Adult intussusception: diagnostic pitfalls, morbidity and mortality in a developing country. Journal of visceral surgery. 2012 Jun:149(3):e211-4. doi: 10.1016/j.jviscsurg.2012.03.005. Epub 2012 May 24 [PubMed PMID: 22633569]
Rea JD, Lockhart ME, Yarbrough DE, Leeth RR, Bledsoe SE, Clements RH. Approach to management of intussusception in adults: a new paradigm in the computed tomography era. The American surgeon. 2007 Nov:73(11):1098-105 [PubMed PMID: 18092641]
Lief K, Janakan G, Clark C, Coffey D. Diagnostic challenge of the non-specific presentation of adult intussusception. BMJ case reports. 2019 Nov 5:12(11):. doi: 10.1136/bcr-2019-229931. Epub 2019 Nov 5 [PubMed PMID: 31694825]
Level 3 (low-level) evidenceHong KD, Kim J, Ji W, Wexner SD. Adult intussusception: a systematic review and meta-analysis. Techniques in coloproctology. 2019 Apr:23(4):315-324. doi: 10.1007/s10151-019-01980-5. Epub 2019 Apr 22 [PubMed PMID: 31011846]
Level 1 (high-level) evidence