Introduction
Pleural effusion is a common condition in emergency departments worldwide and a frequent reason for consultation with pulmonology. In the United States, nearly 1.5 million cases of pleural effusion are diagnosed each year. Congestive heart failure (CHF) is the most common cause, followed by pneumonia. Traditionally, pleural effusions are classified as transudates or exudates. Transudative effusions result from increased hydrostatic pressure with intact capillary membranes, whereas exudative effusions arise from capillary damage secondary to inflammatory or malignant processes.[1][2][3][4][5]
Most pleural effusions resolve following correction of the underlying cause and therapeutic thoracentesis. However, a substantial proportion recur rapidly or remain refractory, leading to repeated hospital visits, patient discomfort, and increased healthcare use. Malignant pleural effusions (MPEs) constitute the most common cause of recurrent pleural effusions, with lung cancer, breast cancer, and lymphoma being the predominant etiologies. Among nonmalignant pleural effusions, refractory CHF and hepatic hydrothorax are the leading causes.[6][7][8]
Recent literature has shifted the management paradigm from repeated thoracenteses to definitive pleural interventions for recurrent effusions. Indwelling pleural catheters (IPCs) have emerged as an effective strategy, providing durable symptom relief, reducing hospital stay, and enabling outpatient-based management (see Image. Indwelling Pleural Catheter System).[9][10][11][12] Although initially developed for MPEs, growing evidence supports the use of IPCs in selected nonmalignant pleural effusions, particularly refractory CHF and hepatic hydrothorax, with acceptable safety profiles.[13][14][15][16]
Results from randomized controlled trials have demonstrated symptom control comparable to talc pleurodesis, with the added advantages of shorter hospitalization and the potential for spontaneous pleurodesis.[10][11][12] Contemporary international guidelines now endorse IPCs as a first-line option for recurrent MPEs and a reasonable alternative in selected nonmalignant effusions, emphasizing shared decision-making and patient-centered care.[9][17][18] Additionally, they have also been found to cause less pain and are much better tolerated than the older chest tubes.[19]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The visceral pleura covers the lung surfaces and interlobar fissures, while the parietal pleura covers the mediastinum, chest wall, and diaphragm. Each lung has its own visceral and parietal pleurae. Therefore, a pneumothorax of 1 lung does not result in a bilateral pneumothorax. There is a "real" space between the visceral and parietal pleura. The pleural space surrounds the lung and is approximately 10 to 15 micrometers wide; it normally contains a small volume of lubricating fluid.[20][21]
Parietal Pleura
The parietal pleura consists of a mesothelial cell layer and a subpleural connective tissue layer, overlying the costal fascia and ribs. The mesothelial surface contains specialized lymphatic stomata, predominantly over the diaphragmatic and mediastinal pleura, which account for more than 90% of pleural fluid absorption and are the primary regulators of pleural fluid turnover.[20][21][22] This surface consists of a mesothelial cell layer and a subpleural layer and overlies the costal fascia and ribs. The mesothelial layer of the parietal pleura consists of stomata for lymphatic drainage.
Visceral Pleural
The visceral pleura consists of a layer of mesothelial cells and a subpleural layer. The visceral pleura is thin cranially and thick caudally due to changes in the density of the subpleural layer. This pleura also comprises mesothelial and subpleural layers and is thinner cranially and thicker caudally due to variation in subpleural tissue density. Unlike the parietal pleura, the visceral pleura has minimal absorptive capacity and plays a limited role in pleural fluid clearance.[21][22] Mesothelial cells lining both pleural surfaces are now recognized as metabolically active, contributing to inflammatory signaling, fibrinolysis, and fibrotic responses, with implications for pleural disease progression and pleurodesis outcomes.[23]
Indications
Indications include those listed below:
- Recurrent malignant pleural effusion causing dyspnea despite therapeutic thoracentesis [24][25]
- Malignant pleural effusion with nonexpandable (trapped) lung, where pleurodesis is unlikely to succeed
- Patients with poor performance status who are unsuitable for chemical or surgical pleurodesis
- Preference for outpatient, home-based palliation to minimize hospital stay
- Recurrent nonmalignant pleural effusions refractory to optimal medical therapy (eg, congestive heart failure, hepatic hydrothorax) [16][26][27]
- Recurrent postsurgical pleural effusions after lung resection requiring repeated therapeutic thoracocentesis [28]
- Need for rapid symptom control with minimal procedural invasiveness
- Patients in whom pleurodesis has failed or is contraindicated [29]
Contraindications
There are no absolute contraindications for IPC insertion. The common contraindications to minor surgical procedures also apply to IPC placement:
Equipment
An IPC system consists of a 66-cm soft silicone catheter featuring a fenestrated intrapleural segment with multiple side holes extending up to 24 cm from the insertion end to facilitate uniform drainage and reduce obstruction compared with single end-hole designs. The catheter incorporates a subcutaneous tunneled segment that acts as a barrier to infection and enhances stability through tissue ingrowth. A polyester (Dacron) cuff positioned at the junction of the proximal two-thirds and distal one-third promotes local fibrosis, secures the catheter against accidental dislodgement, and further reduces the risk of infection. The external 1-way safety valve prevents air ingress and fluid leakage while allowing controlled connection to vacuum drainage bottles, which generate regulated negative pressure to enable gradual pleural fluid removal and minimize rapid lung reexpansion and discomfort. The procedure-specific insertion kit, typically including a metal introducer, dilators (standard and peel-away), scalpel, sutures, scissors, artery forceps, and local anesthetic, supports standardized, sterile bedside or outpatient placement.[29]
Technique or Treatment
Successful use of an IPC depends on meticulous technique, appropriate patient selection, and strict adherence to sterile procedural standards. The following section outlines the stepwise approach to IPC placement, tunneling, cuff positioning, and postprocedural management to optimize drainage efficacy, minimize complications, and promote patient-centered outpatient care (see Image. Indwelling Pleural Catheter Insertion Technique):
- Patient positioning
- The patient is positioned supine with the head end of the bed elevated to approximately 45 degrees. The ipsilateral arm is abducted and flexed over the head to expose the lateral chest wall; if required, the arm may be secured using a sling or adhesive tape to maintain position throughout the procedure.
- Ultrasound localization
- Bedside thoracic ultrasound is performed to confirm the presence, size, and depth of the pleural effusion and to identify a safe insertion site. The entry point is typically selected within the safety triangle, commonly in the mid-axillary line between the fourth and sixth intercostal spaces, to avoid underlying lung, diaphragm, and vascular structures.
- Aseptic preparation
- The skin is prepared with an appropriate antiseptic solution, and the procedure is performed under strict aseptic precautions, using sterile drapes, a gown, gloves, and a mask, as in central venous catheter insertion.
- Pleural access and guidewire placement
- Local anesthesia is infiltrated at the selected pleural entry site, extending from the skin through the subcutaneous tissues to the pleura. The pleural space is accessed with a needle, and free aspiration of pleural fluid confirms correct placement. A guidewire is then introduced into the pleural cavity, following which the needle is removed. A 1 to 1.5 cm skin incision is made with the guidewire positioned centrally within the incision.
- Creation of a subcutaneous tunnel
- A second skin entry point is selected approximately 5 cm inferior to the first site. After infiltration of local anesthetic, a 1-cm vertical incision is made. An additional local anesthetic is administered along the planned subcutaneous tunnel between the 2 incisions. The tunneling device is then attached to the distal end of the catheter.
- Catheter tunneling
- The tunneling device is advanced from the second incision toward the first incision using gentle pressure and rotational movements to create a subcutaneous tunnel. Once the tunneler exits at the first incision, the catheter is drawn through the tunnel. The polyester cuff is positioned within the subcutaneous tissue approximately 1 cm proximal to the second incision, after which the tunneler is detached.
- Tract dilation and catheter insertion
- Using the Seldinger technique, the pleural tract at the first incision is sequentially dilated over the guidewire. The peel-away sheath with its inner dilator is advanced until it reaches the pleural space. The inner dilator and guidewire are then removed, allowing pleural fluid to drain freely. The fenestrated end of the IPC is advanced through the sheath into the pleural cavity until all fenestrations lie intrapleurally. The peel-away sheath is then split and removed as the remaining catheter is advanced. Proper catheter position and absence of kinking are confirmed. Both skin incisions are secured with sutures and covered with sterile dressings; sutures are typically removed after 1 week.[32]
Complications
Infection
As with a long-term urinary catheter, bacteria can colonize an IPC. The pleural fluid culture will be positive, but there will be no signs or symptoms, nor a pathognomonic biochemical profile, characteristic of empyema. In some patients, diagnosing pleural infection can be challenging, as most MPEs have low pH, elevated lactate dehydrogenase, and low glucose. To date, the incidence of IPC-related pleural infection is unknown. Additionally, the diagnostic criteria for pleural infection are the same for patients with IPCs. Skin flora, most commonly Staphylococcus aureus, is reported in case reports, followed by Pseudomonas aeruginosa. Fsych et al reported that the results from a large multicenter trial involving 1021 patients showed an infection incidence of 4.8% and a mortality rate of 0.29%.[33]
Infection typically occurs 6 to 8 weeks post-insertion and is more likely attributable to post-insertion care than to arterial colonization during the procedure. Interestingly, IPC-related pleural infection often results in pleurodesis, particularly with staphylococcal infection. There is no documented increase in the risk of pleural infection with IPCs in immunocompromised patients. This is well documented in patients with hematological malignancies on chemotherapy.
Catheter Tract Metastasis
Patients treated with IPC for MPEs can develop painful nodules near the insertion site or the point of entry into the parietal pleura. Treatment is analgesia and radiotherapy. Mesothelioma is notorious for causing catheter tract metastasis. The cause of this complication remains unknown.[19]
Residual Loculated Effusions
The presence of an IPC is postulated to promote fibrin deposition, which can lead to the formation of loculations, thereby rendering the IPC nonfunctional. This complication usually happens at least 8 weeks postinsertion. Treatment is fibrinolytic therapy with tissue plasminogen activator through the IPC. This is usually very successful but carries a small risk of significant pleural hemorrhage.
Malnutrition
Cachexia is very common in those with cancer. Because pleural fluid is rich in protein, the risk of malnutrition is thought to be substantial. A prospective trial followed patients with IPC for 1 year, but the results showed no significant risk of malnutrition.
Blockage
Fibrous tissue grows around and within the IPC, obstructing several openings. This tissue seldom affects drainage. A complete blockage is rare, occurring in fewer than 5% of cases. A mild blockage usually responds to saline flushes.[34]
Catheter Fracture
This usually happens when an IPC is removed. The polyester cuff promotes inflammation and fibrosis, thereby leading to tight catheter anchoring. The risk is estimated at approximately 10%. This is usually managed by surgical exploration or by leaving the catheter fragments in situ. No complications have been reported with retained IPC fragments.[34]
Clinical Significance
IPCs have significantly altered the management paradigm for recurrent and refractory pleural effusions, particularly MPEs. Historically, repeated thoracentesis was the primary strategy, but this approach was associated with procedural discomfort, frequent hospital visits, diminished quality of life, and cumulative complication risk. Pleurodesis subsequently emerged as a method to obliterate the pleural space, achieved chemically through instillation of sclerosing agents such as talc, bleomycin, or doxycycline via chest tube, or surgically via thoracoscopic mechanical abrasion.[35][36]
However, pleurodesis requires complete lung re-expansion for effective pleural apposition and succeeds in only 60% to 70% of patients. Many individuals with MPEs, particularly those with endobronchial obstruction, interstitial fibrosis, or trapped lung, are not candidates for successful pleurodesis. Following United States Food and Drug Administration approval in 1997, IPCs have become the treatment of choice for MPEs and are increasingly supported by evidence in select non-malignant effusions.[37]
IPCs offer several clinically meaningful advantages. Placement is typically performed under local anesthesia in an outpatient setting, resulting in a shorter length of stay compared with pleurodesis (which commonly requires 2 to 5 days of hospitalization) and improved procedural tolerance. Unlike chemical pleurodesis, IPC insertion avoids pleural and systemic inflammatory responses that may precipitate hypoxemia or respiratory failure, particularly with talc.[35][36] While dyspnea relief is comparable within the first 6 months, IPCs demonstrate superior long-term symptom control and quality-of-life outcomes beyond 6 months.
Additionally, IPCs show higher sustained success rates (>90%) compared with chemical pleurodesis, which may require repeat procedures in approximately 32% of patients and demonstrates reduced efficacy with prolonged cancer survival. Spontaneous pleurodesis can occur with IPCs at a median of 11 weeks, particularly in patients with favorable factors such as breast or gynecologic malignancy, complete lung re-expansion after catheter placement, positive pleural cytology, and no prior chest wall irradiation. From a health economics perspective, IPCs are more cost-effective than talc pleurodesis when anticipated survival is less than 3 months, though this advantage diminishes with longer life expectancy.[37] Collectively, IPCs provide durable symptom palliation, procedural flexibility, and improved patient-centered outcomes in appropriately selected patients.
Enhancing Healthcare Team Outcomes
Effective management of IPCs requires procedural expertise, strategic patient selection, and coordinated interdisciplinary care. Physicians and advanced practitioners must assess candidacy, particularly in patients with malignant pleural effusion or trapped lung, while evaluating performance status, expected survival, and goals of care. Technical competence in sterile placement, tunneling technique, and complication avoidance is essential to minimize pneumothorax, infection, and catheter malfunction. Strategic planning includes determining drainage schedules, monitoring for spontaneous pleurodesis, and identifying early signs of infection or loculation. Clear documentation of catheter type, placement date, and drainage protocol supports safe longitudinal management across care settings.
Nurses play a pivotal role in patient education, aseptic drainage technique, symptom monitoring, and reinforcement of home-care instructions, which are critical for preventing infection and maintaining catheter patency. Pharmacists contribute by optimizing analgesia, guiding antimicrobial therapy when infection is suspected, and reviewing anticoagulation management around placement. Interprofessional communication, particularly during discharge planning and transitions to outpatient or hospice care, ensures continuity of drainage supplies, follow-up imaging, and timely evaluation of complications. Collaboration among pulmonology, thoracic surgery, oncology, interventional radiology, palliative care, and home health services enhances patient-centered outcomes, improves symptom control, reduces hospital utilization, and strengthens overall team performance in the management of pleural effusions.
Media
(Click Image to Enlarge)
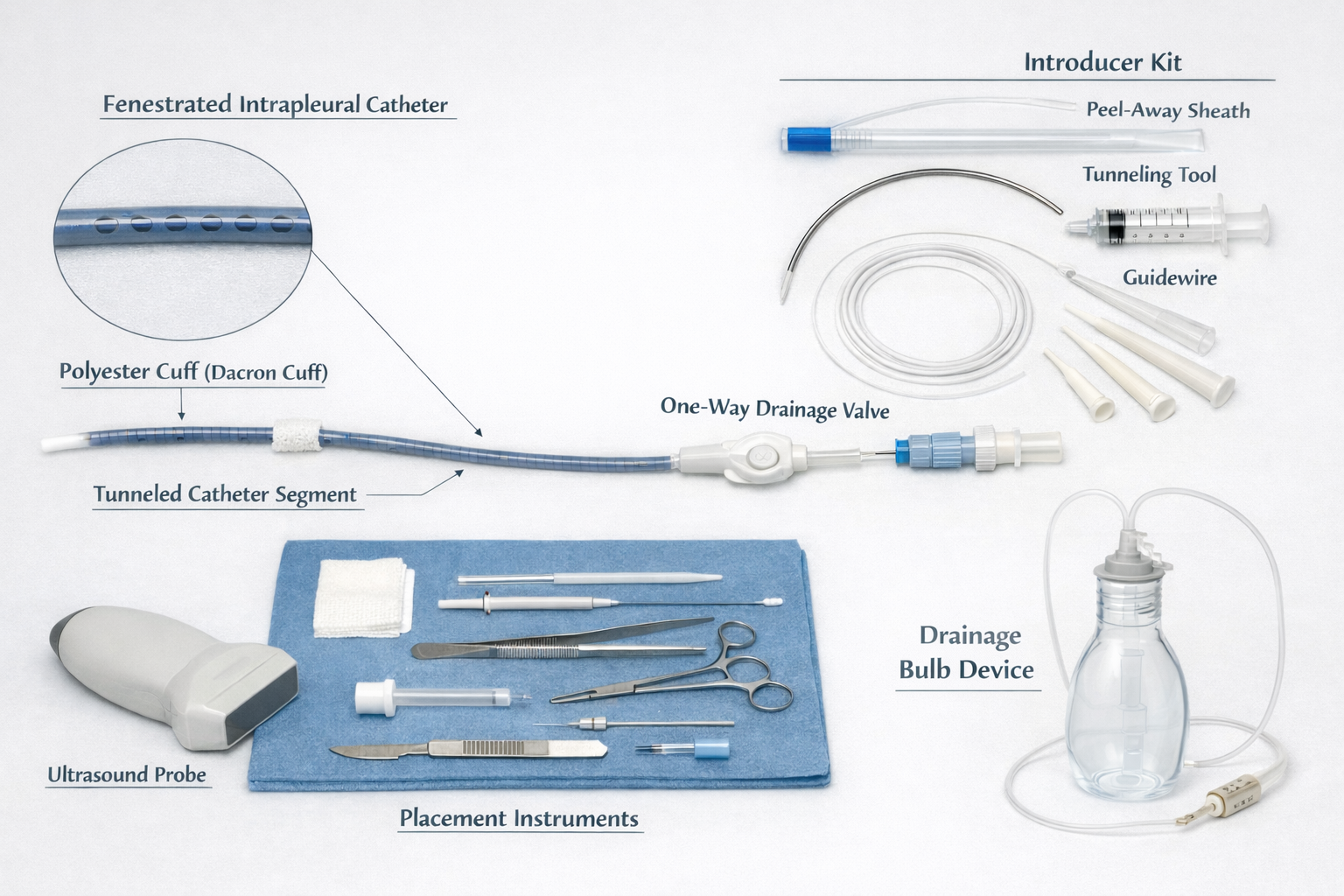
Indwelling Pleural Catheter System. Shown are the fenestrated intrapleural catheter with a polyester (Dacron) cuff and subcutaneous tunneled segment, an external 1-way drainage valve, and the introducer kit comprising a peel-away sheath, tunneling device, guidewire, and dilators. Also depicted are the ultrasound probe used for image-guided insertion, sterile placement instruments, and a drainage bulb device employed for intermittent controlled pleural fluid evacuation in the outpatient or home setting.
Contributed by P Sharma, MD
(Click Image to Enlarge)
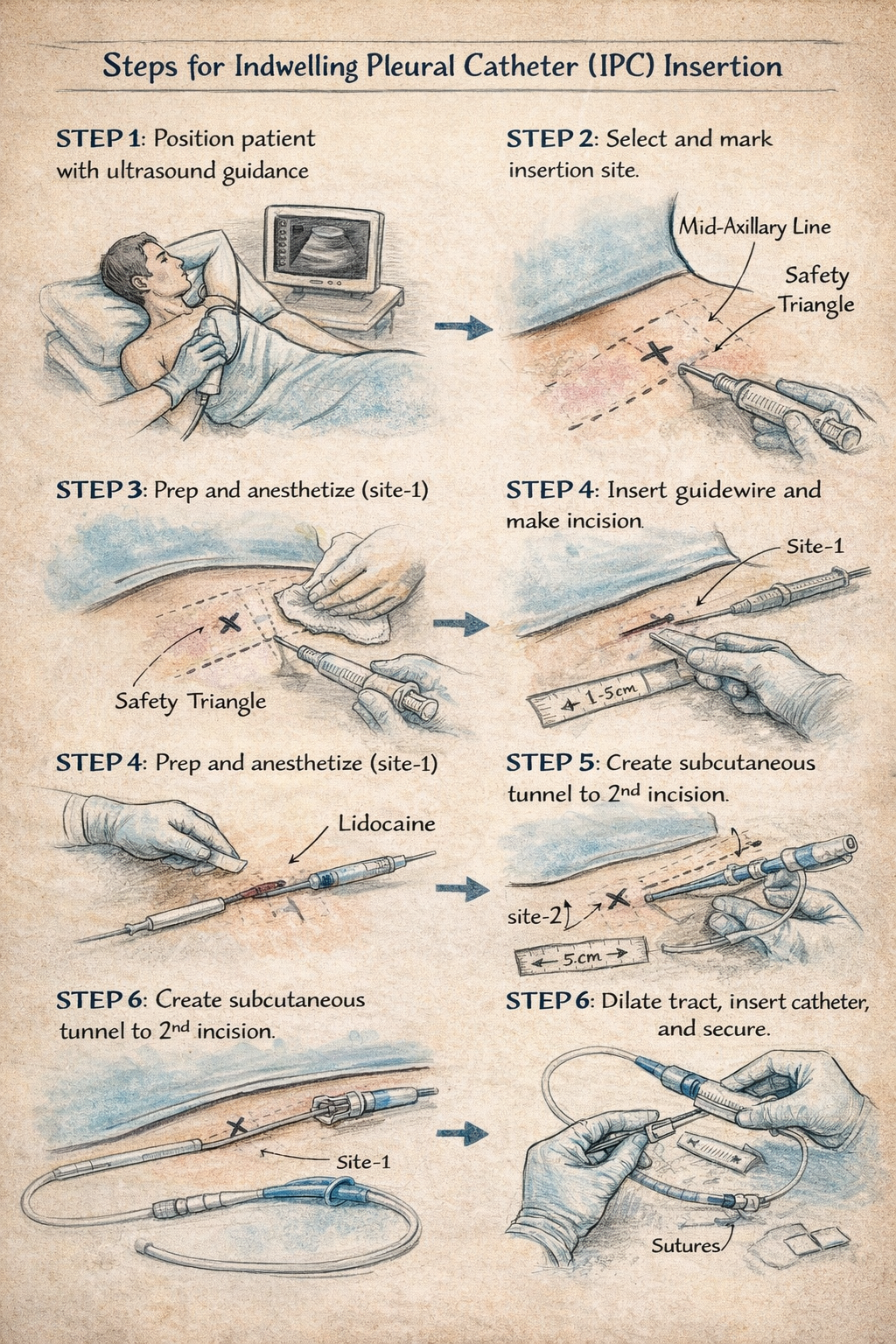
Indwelling Pleural Catheter Insertion Technique. This illustration shows the steps in the insertion technique of an intrapleural catheter.
Contributed by P Sharma, MD
References
Miller C, Bridges E, Laxmanan B, Cox-North P, Thompson H. Tunneled Pleural Catheter: Treatment for Recurrent Pleural Effusion. AACN advanced critical care. 2018 Winter:29(4):432-441. doi: 10.4037/aacnacc2018806. Epub [PubMed PMID: 30523014]
. . :(): [PubMed PMID: 30362967]
Villano AM, Caso R, Marshall MB. Open window thoracostomy as an alternative approach to secondarily infected malignant pleural effusion and failure of intrapleural catheter drainage: a case report. AME case reports. 2018:2():12. doi: 10.21037/acr.2018.03.05. Epub 2018 Apr 13 [PubMed PMID: 30264008]
Level 3 (low-level) evidenceGuinde J, Georges S, Bourinet V, Laroumagne S, Dutau H, Astoul P. Recent developments in pleurodesis for malignant pleural disease. The clinical respiratory journal. 2018 Oct:12(10):2463-2468. doi: 10.1111/crj.12958. Epub [PubMed PMID: 30252207]
Shen-Wagner J, Gamble C, MacGilvray P. Pleural Effusion: Diagnostic Approach in Adults. American family physician. 2023 Nov:108(5):464-475 [PubMed PMID: 37983698]
Demmy TL. Optimizing the study of tunneled intrapleural catheters for malignant pleural effusions. The Journal of thoracic and cardiovascular surgery. 2018 Sep:156(3):1255-1259.e1. doi: 10.1016/j.jtcvs.2018.04.112. Epub 2018 May 24 [PubMed PMID: 29935793]
Fysh ETH, Thomas R, Tobin C, Kuok YJ, Lee YCG. Air in the Pleural Cavity Enhances Detection of Pleural Abnormalities by CT Scan. Chest. 2018 Jun:153(6):e123-e128. doi: 10.1016/j.chest.2018.02.038. Epub [PubMed PMID: 29884273]
Martin GA, Tsim S, Kidd AC, Foster JE, McLoone P, Chalmers A, Blyth KG. Pre-EDIT: protocol for a randomised feasibility trial of elastance-directed intrapleural catheter or talc pleurodesis (EDIT) in malignant pleural effusion. BMJ open respiratory research. 2018:5(1):e000293. doi: 10.1136/bmjresp-2018-000293. Epub 2018 May 29 [PubMed PMID: 29862030]
Level 1 (high-level) evidenceRoberts ME, Neville E, Berrisford RG, Antunes G, Ali NJ, BTS Pleural Disease Guideline Group. Management of a malignant pleural effusion: British Thoracic Society Pleural Disease Guideline 2010. Thorax. 2010 Aug:65 Suppl 2():ii32-40. doi: 10.1136/thx.2010.136994. Epub [PubMed PMID: 20696691]
Davies HE, Mishra EK, Kahan BC, Wrightson JM, Stanton AE, Guhan A, Davies CW, Grayez J, Harrison R, Prasad A, Crosthwaite N, Lee YC, Davies RJ, Miller RF, Rahman NM. Effect of an indwelling pleural catheter vs chest tube and talc pleurodesis for relieving dyspnea in patients with malignant pleural effusion: the TIME2 randomized controlled trial. JAMA. 2012 Jun 13:307(22):2383-9. doi: 10.1001/jama.2012.5535. Epub [PubMed PMID: 22610520]
Level 1 (high-level) evidenceThomas R, Fysh ETH, Smith NA, Lee P, Kwan BCH, Yap E, Horwood FC, Piccolo F, Lam DCL, Garske LA, Shrestha R, Kosky C, Read CA, Murray K, Lee YCG. Effect of an Indwelling Pleural Catheter vs Talc Pleurodesis on Hospitalization Days in Patients With Malignant Pleural Effusion: The AMPLE Randomized Clinical Trial. JAMA. 2017 Nov 21:318(19):1903-1912. doi: 10.1001/jama.2017.17426. Epub [PubMed PMID: 29164255]
Level 1 (high-level) evidenceBhatnagar R, Kahan BC, Morley AJ, Keenan EK, Miller RF, Rahman NM, Maskell NA. The efficacy of indwelling pleural catheter placement versus placement plus talc sclerosant in patients with malignant pleural effusions managed exclusively as outpatients (IPC-PLUS): study protocol for a randomised controlled trial. Trials. 2015 Feb 12:16():48. doi: 10.1186/s13063-015-0563-y. Epub 2015 Feb 12 [PubMed PMID: 25880969]
Level 1 (high-level) evidenceBaig MA, Majeed MB, Attar BM, Khan Z, Demetria M, Gandhi SR. Efficacy and Safety of Indwelling Pleural Catheters in Management of Hepatic Hydrothorax: A Systematic Review of Literature. Cureus. 2018 Aug 6:10(8):e3110. doi: 10.7759/cureus.3110. Epub 2018 Aug 6 [PubMed PMID: 30338185]
Level 1 (high-level) evidencePu CY, Avendano CA, Durant M, Ospina-Delgado D, Burbano AV, Swenson KE, Beattie J, Parikh M, Majid A. Rapid Pleurodesis in Patients With Chronic Noninfectious Pleural Effusion: Twenty Years of Real-world Performance Data. Journal of bronchology & interventional pulmonology. 2025 Jan 1:32(1):. pii: e0993. doi: 10.1097/LBR.0000000000000993. Epub 2024 Oct 30 [PubMed PMID: 39475863]
Shah R, Succony L, Gareeboo S. Use of tunneled pleural catheters for the management of refractory hepatic hydrothorax. BMJ case reports. 2011 Aug 17:2011():. doi: 10.1136/bcr.05.2011.4213. Epub 2011 Aug 17 [PubMed PMID: 22688936]
Level 3 (low-level) evidencePorcel JM. Nonmalignant Pleural Effusions. Seminars in respiratory and critical care medicine. 2022 Aug:43(4):570-582. doi: 10.1055/s-0042-1748186. Epub 2022 Sep 14 [PubMed PMID: 36104027]
Feller-Kopman DJ, Reddy CB, DeCamp MM, Diekemper RL, Gould MK, Henry T, Iyer NP, Lee YCG, Lewis SZ, Maskell NA, Rahman NM, Sterman DH, Wahidi MM, Balekian AA. Management of Malignant Pleural Effusions. An Official ATS/STS/STR Clinical Practice Guideline. American journal of respiratory and critical care medicine. 2018 Oct 1:198(7):839-849. doi: 10.1164/rccm.201807-1415ST. Epub [PubMed PMID: 30272503]
Level 1 (high-level) evidenceFrost N, Ruwwe-Glösenkamp C, Raspe M, Brünger M, Temmesfeld-Wollbrück B, Suttorp N, Witzenrath M. Indwelling pleural catheters for non-malignant pleural effusions: report on a single centre's 10 years of experience. BMJ open respiratory research. 2020 Jan:7(1):. doi: 10.1136/bmjresp-2019-000501. Epub [PubMed PMID: 31958272]
Lui MM, Thomas R, Lee YC. Complications of indwelling pleural catheter use and their management. BMJ open respiratory research. 2016:3(1):e000123. doi: 10.1136/bmjresp-2015-000123. Epub 2016 Feb 5 [PubMed PMID: 26870384]
Ferreiro L, Toubes ME, Suárez-Antelo J, Rodríguez-Núñez N, Valdés L. Clinical overview of the physiology and pathophysiology of pleural fluid movement: a narrative review. ERJ open research. 2024 Sep:10(5):. pii: 00050-2024. doi: 10.1183/23120541.00050-2024. Epub 2024 Sep 30 [PubMed PMID: 39351376]
Level 3 (low-level) evidenceLight RW. Pleural diseases. Disease-a-month : DM. 1992 May:38(5):266-331 [PubMed PMID: 1572232]
Solari E, Marcozzi C, Ottaviani C, Negrini D, Moriondo A. Draining the Pleural Space: Lymphatic Vessels Facing the Most Challenging Task. Biology. 2022 Mar 10:11(3):. doi: 10.3390/biology11030419. Epub 2022 Mar 10 [PubMed PMID: 35336793]
Bhatnagar R, Maskell N. The modern diagnosis and management of pleural effusions. BMJ (Clinical research ed.). 2015 Sep 8:351():h4520. doi: 10.1136/bmj.h4520. Epub 2015 Sep 8 [PubMed PMID: 26350935]
Kamil HG, AbiMusaAsa'ari A, Asaduzzaman M, Su J, Haris M. Clinical Factors Influencing Spontaneous Pleurodesis Success in Malignant Pleural Effusion in Patients With Indwelling Pleural Catheter. Cureus. 2026 Jan:18(1):e100854. doi: 10.7759/cureus.100854. Epub 2026 Jan 5 [PubMed PMID: 41646594]
Westley R, De Fonseka D, Bedawi EO. Updates in the management of malignant pleural effusion: a clinical practice review. Journal of thoracic disease. 2025 Aug 31:17(8):6283-6295. doi: 10.21037/jtd-2025-113. Epub 2025 Jul 28 [PubMed PMID: 40950873]
Shojaee S, Rahman N, Haas K, Kern R, Leise M, Alnijoumi M, Lamb C, Majid A, Akulian J, Maldonado F, Lee H, Khalid M, Stravitz T, Kang L, Chen A. Indwelling Tunneled Pleural Catheters for Refractory Hepatic Hydrothorax in Patients With Cirrhosis: A Multicenter Study. Chest. 2019 Mar:155(3):546-553. doi: 10.1016/j.chest.2018.08.1034. Epub 2018 Aug 29 [PubMed PMID: 30171863]
Level 2 (mid-level) evidenceChalhoub M, Harris K, Castellano M, Maroun R, Bourjeily G. The use of the PleurX catheter in the management of non-malignant pleural effusions. Chronic respiratory disease. 2011:8(3):185-91. doi: 10.1177/1479972311407216. Epub 2011 Jun 2 [PubMed PMID: 21636653]
Reinoso J, Aftab G, Vijayan K, Mehta HJ. Indwelling pleural catheters for persistent pleural effusions secondary to post lung resection for malignancies. Journal of thoracic disease. 2023 May 30:15(5):2469-2474. doi: 10.21037/jtd-22-1517. Epub 2023 Mar 27 [PubMed PMID: 37324077]
Lazarus DR. Extending the indications for indwelling pleural catheters: a tube for all seasons. Journal of thoracic disease. 2023 Jul 31:15(7):3501-3504. doi: 10.21037/jtd-23-765. Epub 2023 Jun 30 [PubMed PMID: 37559635]
Petrov R, Bakhos C, Abbas AE. Management of Malignant Lung Entrapment, the Oncothorax. Thoracic surgery clinics. 2018 Feb:28(1):81-90. doi: 10.1016/j.thorsurg.2017.08.009. Epub [PubMed PMID: 29150040]
Faiz SA, Pathania P, Song J, Li L, Balachandran DD, Ost DE, Morice RC, Shannon VR, Bashoura L, Eapen GA, Jimenez CA. Indwelling Pleural Catheters for Patients with Hematologic Malignancies. A 14-Year, Single-Center Experience. Annals of the American Thoracic Society. 2017 Jun:14(6):976-985. doi: 10.1513/AnnalsATS.201610-785OC. Epub [PubMed PMID: 28326798]
Delaca GB, Titu IM, Teterea F, Ciulic SA, Palade E. Indwelling pleural catheter insertion technique. Multimedia manual of cardiothoracic surgery : MMCTS. 2023 Aug 24:2023():. doi: 10.1510/mmcts.2023.045. Epub 2023 Aug 24 [PubMed PMID: 37615545]
Fysh ETH, Tremblay A, Feller-Kopman D, Mishra EK, Slade M, Garske L, Clive AO, Lamb C, Boshuizen R, Ng BJ, Rosenstengel AW, Yarmus L, Rahman NM, Maskell NA, Lee YCG. Clinical outcomes of indwelling pleural catheter-related pleural infections: an international multicenter study. Chest. 2013 Nov:144(5):1597-1602. doi: 10.1378/chest.12-3103. Epub [PubMed PMID: 23828305]
Level 2 (mid-level) evidenceSidhu C, Davies HE, Muruganandan S, Lui MMS, Lau EPM, Lee YCG. Indwelling Pleural Catheter: Management of Complications. Seminars in respiratory and critical care medicine. 2023 Aug:44(4):454-461. doi: 10.1055/s-0043-1769093. Epub 2023 May 31 [PubMed PMID: 37257836]
Skalski JH, Pannu J, Sasieta HC, Edell ES, Maldonado F. Tunneled Indwelling Pleural Catheters for Refractory Pleural Effusions after Solid Organ Transplant. A Case-Control Study. Annals of the American Thoracic Society. 2016 Aug:13(8):1294-8. doi: 10.1513/AnnalsATS.201601-080BC. Epub [PubMed PMID: 27243620]
Level 2 (mid-level) evidenceClive AO, Jones HE, Bhatnagar R, Preston NJ, Maskell N. Interventions for the management of malignant pleural effusions: a network meta-analysis. The Cochrane database of systematic reviews. 2016 May 8:2016(5):CD010529. doi: 10.1002/14651858.CD010529.pub2. Epub 2016 May 8 [PubMed PMID: 27155783]
Level 1 (high-level) evidenceMunavvar M, Bodtger U, Carus A, Cordovilla R, Naik S, Salud A, Porcel JM. Current Trends in Treating Malignant Pleural Effusion: Evidence, Guidelines, and Best Practice Recommendations. JCO oncology practice. 2025 Jun:21(6):759-765. doi: 10.1200/OP.24.00387. Epub 2024 Dec 17 [PubMed PMID: 39689269]