Introduction
The maxillary artery constitutes a terminal branch of the external carotid artery (ECA), supplying multiple deep structures of the face. This blood vessel is the largest terminal division of the ECA. Classically, the maxillary artery is divided into 3 segments and gives rise to 14 collateral branches, in addition to its terminal sphenopalatine branch.[1]
Originating posterior to the neck of the mandible, the artery courses through the parotid gland, advancing between the sphenomandibular ligament and the ramus of the mandible. The maxillary artery's trajectory is variable, passing either superficial, deep, or, less frequently, through the lateral pterygoid muscle before entering the pterygopalatine fossa (see Image. Dissection of the Maxillary Artery in the Head and Neck).[2] The maxillary artery perfuses the mandible, maxilla, muscles of mastication, nasal cavity, palate, and components of the pterygopalatine fossa.
The maxillary artery holds clinical significance due to its role in supplying vital deep facial structures and involvement in hemorrhage following facial trauma or maxillofacial fractures. Surgical procedures in the infratemporal and pterygopalatine regions necessitate careful consideration of the artery’s variable course to minimize the risk of inadvertent injury. Comprehensive knowledge of the maxillary artery’s anatomy and branching pattern enables clinicians to optimize surgical planning, improve hemostatic control, and enhance outcomes in both reconstructive and endovascular interventions.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The maxillary artery constitutes a terminal branch of the ECA, which originates from the common carotid artery at the C4 vertebral level, where the common carotid bifurcates into its external and internal divisions. The ECA provides arterial supply to superficial structures of the face and scalp. The branches of this blood vessel include the superior thyroid, ascending pharyngeal, lingual, facial, occipital, and posterior auricular arteries, with the maxillary and superficial temporal arteries serving as the terminal divisions.
The maxillary artery gives rise to multiple branches that supply structures of the face and cranium. The artery is classically divided into 3 segments based on its anatomical relationship with the lateral pterygoid muscle. The 1st part is the mandibular portion, which lies posterior to the lateral pterygoid and descends toward the mandible, emitting branches to the meninges and lower teeth. The 2nd segment, the pterygoid part, courses laterally, or less commonly medially, to the lateral pterygoid, supplying the muscles of mastication. The 3rd portion, the pterygopalatine segment, is situated within the pterygopalatine fossa and gives rise to terminal branches that provide arterial supply to the nasal cavity, palate, and maxillary teeth.[3][4] (see Images. Plan of the Maxillary Artery Branches; Maxillary Artery Branches in Lateral Facial View.)
The maxillary artery originates within the parotid gland and courses anteriorly between the neck of the mandible and the sphenomandibular ligament to reach the infratemporal fossa. The blood vessel subsequently traverses the pterygomaxillary fissure to enter the pterygopalatine fossa, a small, inverted pyramid-shaped cavity located deep within the facial skeleton, bounded anteriorly by the maxilla, medially by the palatine bone, and posteriorly by the pterygoid process of the sphenoid.[5]
The deep auricular artery, a branch of the mandibular part of the maxillary artery, enters the external acoustic meatus through the squamotympanic fissure, while the anterior tympanic artery passes through the same fissure to supply the tympanic membrane. The middle meningeal artery (MMA) ascends between the tensor veli palatini and the lateral pterygoid to enter the foramen spinosum, providing vascular supply to the dura mater of the middle cranial fossa. This branch divides into an anterior segment, which crosses the pterion toward the vertex, and a posterior section, which ascends posteriorly within the middle cranial fossa.
The accessory meningeal artery enters the cranial cavity via the foramen ovale. The inferior alveolar artery gives rise to the mylohyoid artery before entering the mandible, supplying the mylohyoid muscle, and then enters the mandibular foramen to supply the lower teeth and mandible. This branch terminates as the mental artery at the mental foramen, providing arterial supply to the skin, muscles of the chin, and surrounding gingivae.[6]
The pterygoid part of the maxillary artery gives rise to the deep temporal arteries—anterior, middle, and posterior—which ascend between the temporalis muscle and the pericranium, providing its primary vascular supply. The buccal artery courses anteriorly along the buccinator muscle, supplying both the muscle and the mucosa of the cheek. The masseteric artery passes laterally through the mandibular notch to vascularize the masseter muscle, while small pterygoid branches supply the medial and lateral pterygoid muscles.
The pterygopalatine part of the maxillary artery gives rise to several branches that supply the pharynx, palate, nasal cavity, and maxillary teeth. The pharyngeal artery descends medially, providing vascular supply to the roof of the pharynx, the soft palate, and the pharyngotympanic (Eustachian) tube. The descending (greater) palatine artery courses through the greater palatine canal to reach the hard palate, giving rise to lesser palatine branches that supply the soft palate. The artery of the pterygoid canal, also referred to as the "Vidian artery," passes posteriorly through the pterygoid canal alongside the Vidian nerve, supplying the upper pharynx, auditory tube, and structures within the pterygoid canal.
The sphenopalatine artery enters the nasal cavity through the sphenopalatine foramen and gives rise to the posterior lateral nasal arteries and posterior septal branches. The posterior superior alveolar artery provides arterial supply to the maxillary molars, premolars, and adjacent gingiva, while the infraorbital artery passes through the inferior orbital fissure into the infraorbital canal, giving rise to the anterior superior alveolar artery for the upper incisors and canines.[7]
Embryology
The maxillary artery arises from the remnant of the 1st aortic arch. Regression of the 1st and 2nd aortic arches occurs during embryogenesis, leaving the maxillary artery among the limited number of permanent derivatives.
Blood Supply and Lymphatics
Mandibular Branches
The deep auricular and anterior tympanic arteries provide arterial supply to the external acoustic meatus and the deep surface of the tympanic membrane, respectively. The MMA, a principal branch of the maxillary artery, supplies the dura mater, cranial bones, and structures of the middle cranial fossa, remaining adherent to the periosteal layer of the dura.[8] The accessory meningeal artery contributes to the vascularization of the dura mater, trigeminal ganglion, and adjacent muscles of the infratemporal region, including the medial and lateral pterygoid, tensor veli palatini, and, occasionally, the tensor tympani muscles.[9] The inferior alveolar artery supplies the lower teeth, lower lip, and chin through its terminal mental branch, while the mylohyoid artery provides arterial supply to the mylohyoid muscle.
Pterygoid Branches
The deep temporal arteries provide vascular supply to the temporalis muscle, which also receives contributions from the superficial temporal artery, a branch of the ECA. The buccal artery supplies the buccinator muscle, while the masseteric artery provides arterial supply to the masseter muscle. Small pterygoid branches supply the medial and lateral pterygoid muscles, ensuring comprehensive vascularization of the muscles of mastication.
Pterygopalatine Branches
The pharyngeal artery provides arterial supply to the posterior roof of the nasal cavity, the sphenoid sinus, and the auditory (Eustachian) tube. The greater palatine artery supplies the hard palate, while its lesser palatine branches vascularize the soft palate. The sphenopalatine artery terminates as the posterior lateral nasal and posterior septal branches, with the posterior septal branches forming anastomoses with the greater palatine artery. The posterior superior alveolar artery supplies the maxillary molars, premolars, and adjacent gingiva, whereas the infraorbital artery provides vascular supply to the lower eyelid, upper lip, cheek, and anterior maxillary teeth.
Venous Drainage
Venous return from regions supplied by the maxillary artery occurs primarily via the pterygoid venous plexus, situated between the medial and lateral pterygoid muscles and between the lateral pterygoid and temporalis muscles. This plexus facilitates drainage from the infratemporal and pterygopalatine fossae and establishes communication with the cavernous sinus through small emissary veins traversing the foramen ovale, foramen lacerum, and sphenoidal emissary foramina.
Muscles
The infratemporal and pterygopalatine fossae contain several muscles, many of which receive vascular supply from branches of the maxillary artery. Among these muscles, the lateral and medial pterygoids are of particular significance due to their anatomical relationships, as they are critical for understanding the divisions of the artery.
The lateral pterygoid muscle comprises upper and lower heads, with the upper head originating from the roof of the infratemporal fossa and the lower head arising from the lateral surface of the lateral pterygoid plate. Both heads insert into the capsule of the temporomandibular joint, and their nearly horizontal fibers facilitate jaw protrusion and lateral movements. The medial pterygoid muscle consists of deep and superficial heads, with the deep head arising from the medial surface of the lateral pterygoid plate and the superficial head originating from the maxillary tuberosity. Both heads insert on the medial surface of the mandible near its angle, functioning to elevate the jaw and assist in side-to-side movements.[10]
Physiologic Variants
Variations in the course of the maxillary artery are frequent. The artery runs lateral to the lateral pterygoid muscle in about 2/3 of cases and medially in the remainder. Additional variations include the presence of common trunks between the deep auricular and anterior tympanic arteries, or between the MMA and accessory meningeal arteries. Evidence suggests that a medially coursing artery is more likely to exhibit separate meningeal branches, while a laterally coursing artery often originates from a common meningeal trunk. Rarely, the artery may course laterally on one side and medially on the contralateral side.
Surgical Considerations
Posterior epistaxis is frequently difficult to control, and anterior nasal packing is typically insufficient. Endovascular embolization of the sphenopalatine and anterior ethmoidal arteries may be required in refractory cases.[11] In recent years, extracranial-to-intracranial (EC-IC) bypass procedures utilizing the maxillary artery have been developed for the treatment of skull base tumors and complex cerebral aneurysms. Traditional approaches involve a zygomatic osteotomy to access the vessel. However, newer techniques achieve exposure through the deep temporal vessels after reflection of the temporalis muscle, eliminating the need for osteotomy.[12][13][14]
Bleeding originating from the deeper branches of the nasal cavity, referred to as "posterior epistaxis," is typically more severe and less responsive to conservative management than bleeding from the anterior nasal region. Standard nasal packing, which applies pressure within the nasal passage to promote clot formation, often fails to control hemorrhage when the source is located in the posterior vasculature. Endovascular embolization may be undertaken in such cases. A fine catheter is advanced through the arterial system to the target vessels, most commonly the sphenopalatine and anterior ethmoidal arteries, where embolic materials, such as coils or microparticles, are deployed to obstruct blood flow and achieve hemostasis.
The maxillary artery provides an essential vascular route for advanced cranial and skull base procedures. An EC-IC bypass may be performed in selected cases of cerebral aneurysm or skull base tumor.[15] This procedure involves creating a surgical connection between an artery located outside the skull and one within the cranial cavity, establishing an alternative channel for cerebral blood flow when normal circulation is compromised.
Historically, exposure of the maxillary artery for EC-IC bypass required a zygomatic osteotomy, involving temporary removal of part of the zygomatic bone to access the vessel. Less invasive approaches have been developed more recently. The artery may be approached by reflecting the temporalis muscle to identify the deep temporal branches, providing direct access to the maxillary artery. This technique eliminates the need for bone removal, shortens operative time, and reduces tissue trauma while maintaining sufficient visualization of the artery for microvascular reconstruction.
The pterygoid venous plexus is clinically significant due to its communication with the cavernous sinus via valveless emissary veins. This connection allows the potential spread of odontogenic or facial infections into the intracranial space, which may result in cavernous sinus thrombosis.
Injury to the MMA constitutes a classic cause of epidural hematoma following trauma to the temporal bone at the pterion. The artery lies within the periosteal layer of the dura, and hemorrhage occurs under high pressure, separating the dura from the skull and producing a biconvex (lens-shaped) hematoma on computed tomography. Patients may present with an initial loss of consciousness, followed by a lucid interval and subsequent neurological deterioration. This condition represents a neurosurgical emergency requiring immediate evacuation, most commonly via craniotomy or, when indicated, burr hole decompression.[16]
Clinical Significance
The maxillary artery is of considerable clinical importance due to its complex anatomy and involvement in multiple pathologic and surgical conditions. The sphenopalatine artery, a terminal branch, constitutes a major source of posterior epistaxis, which is often resistant to anterior nasal packing and may require endovascular embolization for definitive management. In neurosurgical and skull base procedures, the maxillary artery can serve as a donor vessel for EC-IC bypass, reestablishing cerebral perfusion when native intracranial vessels are compromised. Contemporary techniques that utilize the deep temporal branches have reduced operative morbidity by avoiding zygomatic osteotomy.
The pterygoid venous plexus provides a potential route for the spread of odontogenic or facial infections to the cavernous sinus, while trauma to the MMA remains a recognized cause of epidural hematoma following temporal bone injury. Comprehensive knowledge of these vascular relationships is essential for minimizing complications in maxillofacial, otolaryngologic, and neurosurgical interventions.
Media
(Click Image to Enlarge)
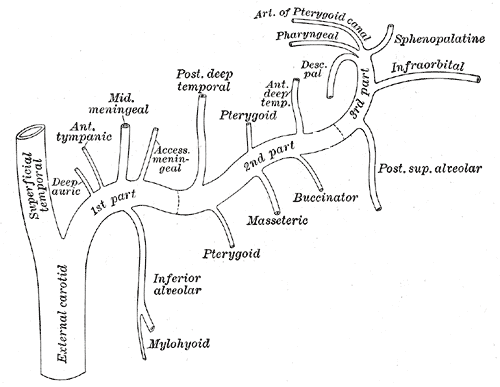
Plan of the Maxillary Artery Branches. The mandibular segment (proximal portion) of the maxillary artery gives rise to the middle meningeal and inferior alveolar arteries. The pterygoid segment (second portion) produces multiple branches, including the buccal artery, which supplies the buccinator musculomucosal flap. The pterygopalatine segment (terminal portion) traverses the pterygopalatine fossa, giving rise to the sphenopalatine, infraorbital, superior alveolar, and descending palatine arteries.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
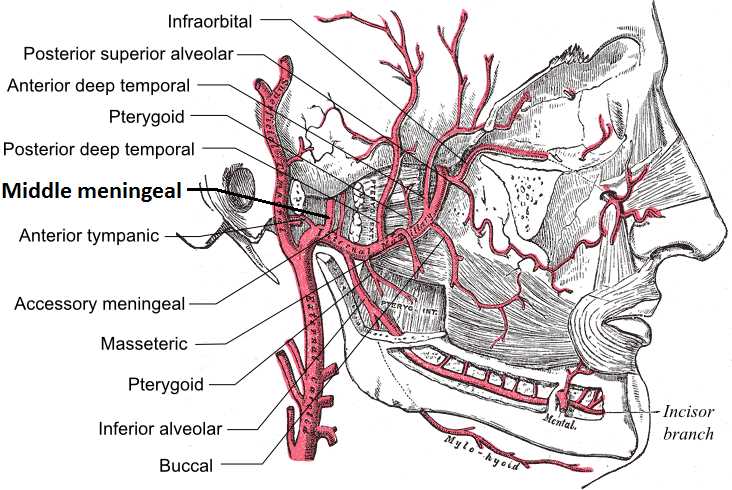
Maxillary Artery Branches in Lateral Facial View. The image depicts the maxillary artery and its major branches as they traverse the infratemporal fossa and lateral face. Key arteries, including the middle meningeal and inferior alveolar branches, are identified with respect to surrounding muscles and bone.
Mikael Häggström, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
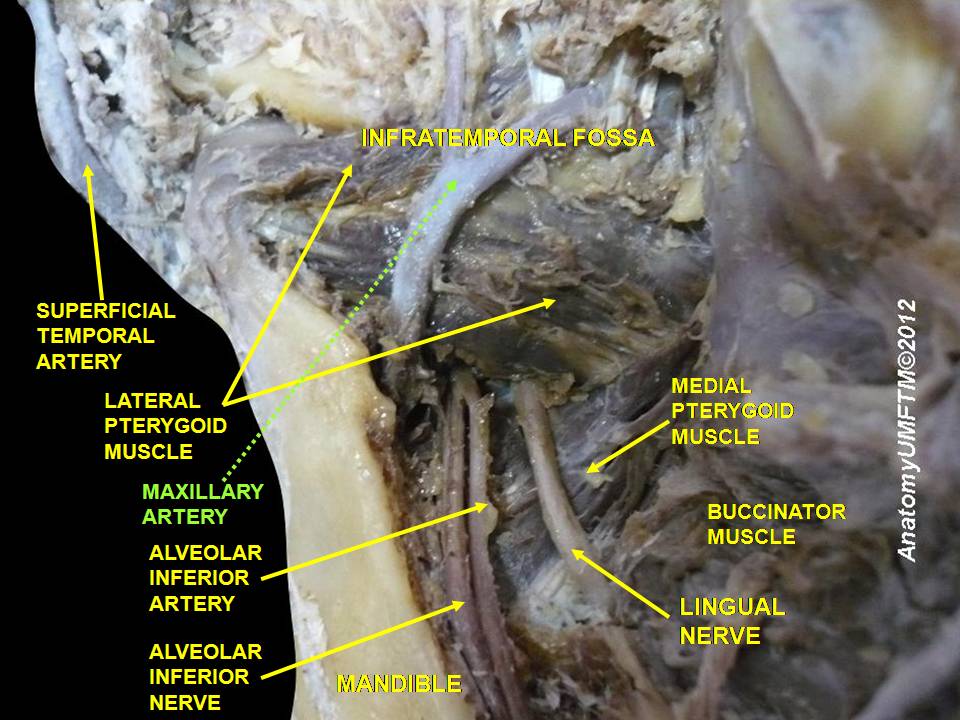
Dissection of the Maxillary Artery in the Head and Neck. This image shows a dissection of the lateral side of the head and neck, demonstrating the course of the maxillary artery and its relation to adjacent structures. The artery is depicted passing lateral to the lateral pterygoid muscle, giving rise to the inferior alveolar artery near the inferior alveolar nerve, with surrounding structures including the superficial temporal artery, medial pterygoid and buccinator muscles, and lingual nerve.
Contributed by Anatomist90 - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=19784978 Public Domain
References
Ottone NE, Sandoval C, Cid-Gutierrez P, Vásquez-Balboa ML, Tubbs RS, Fuentes R. Systematic review and meta-analysis of the anatomy of the maxillary artery using the Anatomical Quality Assurance (AQUA) checklist. Surgical and radiologic anatomy : SRA. 2021 Nov:43(11):1875-1886. doi: 10.1007/s00276-021-02825-3. Epub 2021 Sep 4 [PubMed PMID: 34480213]
Level 1 (high-level) evidencePiagkou M, Triantafyllou G, Papadopoulos-Manolarakis P, Demetriou F, Tsakotos G, Olewnik Ł, Duparc F. Mapping the Maxillary Artery and Lateral Pterygoid Muscle Relationship: Insights from Radiological and Meta-Analytic Evidence. Medicina (Kaunas, Lithuania). 2025 Jun 30:61(7):. doi: 10.3390/medicina61071201. Epub 2025 Jun 30 [PubMed PMID: 40731831]
Casale J, Bordoni B. Anatomy, Head and Neck: Infratemporal Fossa. StatPearls. 2025 Jan:(): [PubMed PMID: 30725719]
Cappello ZJ, Arbor TC, Potts KL. Anatomy, Pterygopalatine Fossa. StatPearls. 2025 Jan:(): [PubMed PMID: 30020641]
Lovász K, Magyar P, Szalóki T, Maurovich-Horvat P, Altdorfer K, Tamás L, Alpár A. A radioanatomical study of 3rd segment terminal branches of the maxillary artery in the pterygopalatine fossa. Scientific reports. 2023 Feb 28:13(1):3401. doi: 10.1038/s41598-023-29975-1. Epub 2023 Feb 28 [PubMed PMID: 36854685]
White HJ, Reddy V, Mesfin FB. Anatomy, Head and Neck: Foramen Spinosum. StatPearls. 2025 Jan:(): [PubMed PMID: 30571053]
Alvernia JE, Hidalgo J, Sindou MP, Washington C, Luzardo G, Perkins E, Nader R, Mertens P. The maxillary artery and its variants: an anatomical study with neurosurgical applications. Acta neurochirurgica. 2017 Apr:159(4):655-664. doi: 10.1007/s00701-017-3092-5. Epub 2017 Feb 13 [PubMed PMID: 28191601]
Natali AL, Reddy V, Leo JT. Neuroanatomy, Middle Meningeal Arteries. StatPearls. 2025 Jan:(): [PubMed PMID: 30137830]
Ikezawa M, Maeda K, Takasu S, Takemoto M, Nishihori M, Choo J, Sago F, Somiya D, Doba K, Ikeda A. Rare Dilated Collateral Circulation from Accessory Meningeal Artery to Inferolateral Trunk: A Case Report. NMC case report journal. 2023:10():47-50. doi: 10.2176/jns-nmc.2022-0308. Epub 2023 Mar 15 [PubMed PMID: 37020745]
Level 3 (low-level) evidenceCorcoran NM, Goldman EM. Anatomy, Head and Neck, Masseter Muscle. StatPearls. 2025 Jan:(): [PubMed PMID: 30969691]
Iimura J, Hatano A, Ando Y, Arai C, Arai S, Shigeta Y, Kojima H, Otori N, Wada K. Study of hemostasis procedures for posterior epistaxis. Auris, nasus, larynx. 2016 Jun:43(3):298-303. doi: 10.1016/j.anl.2015.09.015. Epub 2015 Oct 31 [PubMed PMID: 26527519]
Wang L, Cai L, Lu S, Qian H, Lawton MT, Shi X. The History and Evolution of Internal Maxillary Artery Bypass. World neurosurgery. 2018 May:113():320-332. doi: 10.1016/j.wneu.2018.02.158. Epub 2018 Mar 7 [PubMed PMID: 29524709]
Level 2 (mid-level) evidenceAkiyama O, Güngör A, Middlebrooks EH, Kondo A, Arai H. Microsurgical anatomy of the maxillary artery for extracranial-intracranial bypass in the pterygopalatine segment of the maxillary artery. Clinical anatomy (New York, N.Y.). 2018 Jul:31(5):724-733. doi: 10.1002/ca.22926. Epub 2017 Nov 29 [PubMed PMID: 28556192]
Yağmurlu K, Kalani MYS, Martirosyan NL, Safavi-Abbasi S, Belykh E, Laarakker AS, Nakaji P, Zabramski JM, Preul MC, Spetzler RF. Maxillary Artery to Middle Cerebral Artery Bypass: A Novel Technique for Exposure of the Maxillary Artery. World neurosurgery. 2017 Apr:100():540-550. doi: 10.1016/j.wneu.2016.12.130. Epub 2017 Jan 9 [PubMed PMID: 28089839]
Matsuo S, Komune N, Akiyama O, Amano T, Nakamizo A. Surgical Anatomy of the Donor Arteries for Extracranial-Intracranial Bypass Surgery: An Anatomic and Radiologic Study. World neurosurgery. 2020 Apr:136():e447-e459. doi: 10.1016/j.wneu.2020.01.033. Epub 2020 Jan 14 [PubMed PMID: 31953092]
Khairat A, Margetis K, Waseem M. Epidural Hematoma. StatPearls. 2025 Jan:(): [PubMed PMID: 30085524]