Introduction
A myocardial infarction (MI) occurs when a coronary atherosclerotic plaque ruptures, resulting in platelet aggregation and thrombus formation. The thrombus occludes blood flow, causing myocardial ischemia and potentially infarction. There are 3 main coronary arteries: the left anterior descending artery (LAD), the left circumflex artery (LCx)(both branch from the left main coronary artery), and the right coronary artery (RCA). In right-dominant circulation (75%-80%), the RCA supplies the right atrium, right ventricle, and the inferior wall of the left ventricle via the posterior descending artery (PDA), as well as the sinoatrial (SA) and atrioventricular (AV) nodes. The most common conduction disorder is complete AV block, which requires immediate intervention to prevent complications and mortality.[1]
Inferior wall MI typically results from an acute coronary artery occlusion (often following plaque rupture), leading to decreased perfusion of the inferior wall. Without emergency intervention, myocardial ischemia can lead to infarction. In most patients, the RCA supplies the inferior myocardium. In approximately 6% to 10% of cases, the left coronary artery system is dominant, and the LCx supplies the inferior wall via the PDA. Approximately 40% of all MIs involve the inferior wall. Inferior MIs generally have a better prognosis than anterior MIs, with a mortality rate of less than 10%. However, complications that increase mortality include right ventricular infarction, hypotension, bradycardia, AV nodal block, and cardiogenic shock.[2][3][4]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Atherosclerosis is characterized by the accumulation of fatty deposits (plaque) within the arterial intima. Atherosclerosis can begin in childhood with the development of fatty streaks that progress with age into fibrous cholesterol plaques. When this process involves the coronary arteries, it is called coronary artery disease. The portion of the plaque adjacent to the vessel's lumen is the fibrous cap, and thinner, inflamed caps have a higher risk of rupture. When coronary artery plaques rupture, highly thrombogenic substances inside the plaque are released into the blood, leading to rapid thrombus formation, sudden occlusion of the coronary artery, ischemia, and possible infarction (death of myocardial tissue). Acute coronary syndrome results from the loss of integrity of the protective covering over an atherosclerotic plaque. Rupture of a plaque within a coronary artery that perfuses the inferior wall of the heart results in an inferior MI.[5]
Epidemiology
Myocardial infarction is a leading cause of global morbidity and mortality. Due to advances in medical care, patient education, and risk factor management, the incidence of MI has declined in the United States. Modifiable risk factors include hypertension, hyperlipidemia, tobacco use, diabetes mellitus, obesity, physical inactivity, and psychosocial stress. The nonmodifiable risk factors are age and family history. The risk of MI increases with age, and men have a higher risk than women. Black individuals have higher mortality rates from MI than White individuals, reflecting disparities in patient care. Inferior wall MIs account for 40% to 50% of all MIs and have a better prognosis than other anatomic territories, with a mortality rate of 2% to 9%. However, up to 40% of inferior wall MIs involve the right ventricle, which is associated with worse outcomes.[1][6][7]
Pathophysiology
The pathophysiology of MI involves rupture of a coronary artery plaque, platelet aggregation and thrombus formation, and distal occlusion of the vessel lumen resulting in diminished flow. This narrowing or occlusion of a vessel can progress to myocardial ischemia and necrosis. The RCA runs in the AV groove and continues to the posterior interventricular groove, where it gives rise to the PDA and supplies the inferior wall in right-dominant circulation. In left-dominant circulation, the PDA arises from the LCx. A lesion in the RCA usually causes inferior wall infarction.
The RCA perfuses the SA and AV node, so bradycardia, AV nodal block, and arrhythmias are associated with inferior wall MIs.[8] Sinus bradycardia is common in early inferior ST-segment elevation myocardial infarction. For example, results from a study demonstrated that sinus bradycardia was 3 times more common in inferior MIs than in anterior MIs. Furthermore, proximal RCA occlusion caused sinus bradycardia more often than mid- or distal RCA occlusion, and LCx occlusion was not associated with sinus bradycardia.[9]
AV nodal block is common in inferior wall MIs because the posterolateral RCA supplies part of the AV node in right-dominant circulation. RCA occlusion causes the inferior myocardial wall to release acetylcholine, contributing to bradycardia and AV nodal block.[8][9] Transient, second-degree, Mobitz type I AV nodal block is more common in inferior MI caused by RCA occlusion. Second-degree, Mobitz type II AV nodal block carries a worse prognosis when present.[9] The Bezold-Jarisch reflex is a triad of hypotension, bradycardia, and peripheral vasodilation, often caused by an inferior wall MI. This reflex is caused by stimulation of cardiopulmonary mechanoreceptors associated with unmyelinated, vagal nerve afferent C fibers.[9]
Histopathology
Atherosclerosis involving the coronary arteries is known as coronary artery disease (CAD). The histopathologic features of CAD evolve and can be divided into several stages. The initial lesions of atherosclerosis often begin in childhood as fatty streaks. These lesions do not disrupt the arterial architecture and commonly occur in adolescents and young adults. Over time, these fatty streaks can develop into atherosclerotic plaques. Characteristics of atheromatous plaques include a fibrous cap and a necrotic lipid core. Eventually, these fibrous caps can rupture, releasing the contents of the necrotic lipid core into the blood, which can result in thrombus formation. Depending on the size and magnitude of the thrombus, occlusion of the coronary artery can occur, leading to ischemia and potential infarction.[10]
History and Physical
The history should elicit the onset and character of symptoms, including chest pain or shortness of breath. A past medical history of diabetes mellitus, CAD, prior MI, and hypertension is pertinent. Family history of CAD and social history of tobacco use are also important factors. Medication history, including the recent use of phosphodiesterase type 5 inhibitors, can uncover contraindications to the use of nitroglycerin. Physical examination should include vital signs (heart rate, blood pressure, oxygen saturation) and evaluation for jugular venous distension (suggestive of right ventricular infarction), assessment of heart rhythm, and auscultation for murmurs and gallops. Evidence of volume overload, such as peripheral edema or pulmonary crackles (rales) on lung examination, should also be noted.
Evaluation
Evaluation should include an electrocardiogram (ECG) for detecting ST-segment changes, including ST-segment elevation in the inferior leads (II, III, aVF) with reciprocal change in other leads. Serial troponin levels, a complete blood count, a basic metabolic panel, and coagulation studies should be performed in all patients in anticipation of percutaneous coronary intervention or thrombolytic therapy. Patients presenting with typical chest pain symptoms and an ECG revealing ST-segment elevation should proceed directly to the cardiac catheterization lab for primary percutaneous coronary intervention if available.[11]
The ECG remains the initial test of choice. Traditionally, reciprocal ST-segment depression is observed in leads electrically opposite to the infarct location; however, ST-segment depression can occur in any lead, with the infarct area acting as the negative pole.[11] Inferior MI is associated with ST-segment elevations in the inferior leads (II, III, and aVF). (See Image. Electrocardiogram With Pardee Waves).
The relative magnitude of ST elevation in lead II versus lead III can sometimes help distinguish whether the RCA or the LCx is involved. If ST-segment elevation in lead III is higher than in lead II, the RCA is likely involved. When the ST-segment elevation magnitude is greater in lead II compared with lead III, the LCx is more likely to be involved. Reciprocal ST-segment depression is most common in the lateral leads I and aVL. RCA involvement may also produce ST-segment elevation in the right-sided leads.[12][13] The most common ECG finding associated with an inferior wall myocardial infarction is ST-segment elevation in leads II, III, and aVF, accompanied by reciprocal ST-segment depression in leads I and aVL. Results from a large meta-analysis found that the most sensitive and specific findings for inferior MI were ST-segment elevation in lead III, along with concurrent ST-segment depression in lead I.[7]
Treatment / Management
If ST-segment elevation is present on the ECG, the patient should receive emergent coronary angiography with primary percutaneous coronary intervention; the goal door-to-balloon time is less than 90 minutes. If the facility does not have a cardiac catheterization lab or transport times are outside this time window, thrombolysis should be considered. If right ventricular infarction is suspected, nitrates should be avoided due to the risk of hypotension, and intravenous crystalloids should be provided to optimize preload. The right ventricle contains less myocardium than the left ventricle and depends on adequate preload to maintain cardiac output. If there is damage to the right ventricle, preload reduction from nitrates could result in significant hypotension. Treatment with intravenous crystalloids and, if necessary, vasopressors is required in the setting of hypotension. Other treatments include an oral aspirin dose of 162 mg to 325 mg, intravenous unfractionated heparin, and additional antiplatelet agents such as clopidogrel or prasugrel.[14][15][16](A1)
High-grade conduction abnormalities are associated with higher mortality. Temporary transvenous pacing is recommended in cases of complete AV nodal block that does not improve with reperfusion. When pacing is not available, intravenous isoproterenol, dopamine, or epinephrine has been used temporarily.[1] (B3)
Differential Diagnosis
The differential diagnosis of acute chest pain can be extensive. Symptoms that indicate an increased likelihood of cardiac disease include exertional chest pain, diaphoresis, nausea and vomiting, and radiation of pain to the arm or jaw. Other life-threatening illnesses to consider include pulmonary embolism, acute aortic dissection, pneumothorax, esophageal rupture, and cardiac tamponade. Atypical symptoms may occur, especially in women, older adults, and individuals with diabetes mellitus. Because myocardial ischemia symptoms include nausea, vomiting, epigastric pain, and fatigue, it is imperative to consider the cardiac causes of these symptoms and not dismiss them as gastrointestinal tract illnesses.
Pertinent Studies and Ongoing Trials
The recently reported Fractional Flow Reserve Versus Optical Coherence Tomography to Guide Revascularization of Intermediate Coronary Stenoses (FORZA) trial and the OCT-Features Of moRphology, coMposItion anD instABility of culprit and not culprit coronary pLaquE in ACS patient (OCT-FORMIDABLE) have evaluated the use of fractional flow reserve and optical coherence tomography to help risk-stratify patients for interventional cardiac procedures.[17]
Prognosis
The mortality rate of inferior wall MI is approximately 2% to 9%.[7] While inferior wall MIs usually have a favorable prognosis, a few factors may increase mortality. Approximately 40% of inferior wall infarctions also involve the right ventricle. Right ventricular infarctions are very preload-dependent, and nitrates may precipitate hypotension. Obtaining an ECG using right-sided leads and noting ST-segment elevations in V4R may suggest the diagnosis. If timely treatment does not occur, myocyte death increases, and there is a risk of cardiogenic shock. Additionally, AV nodal block and bradycardia may occur because the RCA supplies blood to the SA and AV nodes. A high-grade AV nodal block (defined as a second-degree, Mobitz type II or third-degree AV nodal block) occurs in 19% of patients with acute inferior wall myocardial infarction. The amount of collateral circulation to the AV node impacts the incidence of heart block. If there are concomitant perfusion abnormalities in other coronary arteries, collateral circulation to the AV node is reduced, and the likelihood of AV nodal block increases.
Complications
The complications of inferior myocardial infarctions include:
- Cardiogenic shock
- AV nodal block
- Bradyarrhythmias
- Ventricular fibrillation
Postoperative and Rehabilitation Care
Secondary prevention and rehabilitation for inferior myocardial infarctions include:
- Cardiac rehabilitation
- Blood pressure management
- Cholesterol and blood glucose management
- Maintenance of a healthy body weight
Deterrence and Patient Education
Important points of patient education for secondary prevention in inferior MIs include:
- Balanced diet
- Regular exercise
- Smoking cessation
Pearls and Other Issues
AV nodal block is present initially in approximately 9% of patients, and high-degree AV nodal block occurs in two-thirds of patients in the first 24 hours after onset. While AV nodal blocks are a primary contributor to morbidity and mortality, most high-degree AV nodal blocks are treatable with atropine. Temporary transvenous pacing is used when the nodal block is unresponsive to medical therapy, and permanent pacemakers are rarely required. Myocardial necrosis can predispose to potentially lethal arrhythmias such as ventricular tachycardia and ventricular fibrillation (See Image. Ischemic Ventricular Tachycardia in a Patient With Previous Inferior Myocardial Infarction). Patients with arrhythmias should be monitored in an intensive care unit during the acute phase. When potentially lethal arrhythmias occur, immediate defibrillation is lifesaving.
Enhancing Healthcare Team Outcomes
Managing an inferior wall MI requires an interprofessional team of nurses, clinicians, cardiac surgeons, and cardiologists. These patients risk life-threatening complications, so prevention is the best approach. At discharge, nurses should educate patients about the potential need for cardiac pacing in the future should a high-grade AV nodal block occur. The dietitian should recommend a diet low in salt and fat. Patients should be enrolled in a cardiac rehabilitation program. The pharmacist should encourage smoking cessation, medication adherence, and the regulation of blood cholesterol and glucose levels.[18][19][20]
Outcomes
Right ventricular infarction is an independent predictor of major complications and prolonged hospitalization in inferior MI. Additionally, ischemia of the cardiac conduction system disrupts its function, leading to a high degree of AV blockade that often requires temporary pacing. Mortality with right ventricular involvement often exceeds 25%. Additionally, even after discharge, many patients require permanent pacing within 3 years.[21][22][23]
A strategic approach is equally crucial, involving evidence-based strategies to optimize treatment plans and minimize adverse effects. Ethical considerations must guide decision-making, ensuring informed consent and respecting patient autonomy in treatment choices. Each healthcare professional must know their responsibilities and contribute their unique expertise to the patient's care plan, fostering an interdisciplinary approach. Effective interprofessional communication is paramount, allowing seamless information exchange and collaborative decision-making among the team members. Care coordination plays a pivotal role in ensuring that patients' journey from diagnosis to treatment and follow-up is well-managed, minimizing errors and enhancing patient safety. By embracing these principles of skill, strategy, ethics, responsibilities, interprofessional communication, and care coordination, healthcare professionals can deliver patient-centered care, ultimately improving patient outcomes and enhancing team performance in the management of inferior wall MIs.
Media
(Click Image to Enlarge)
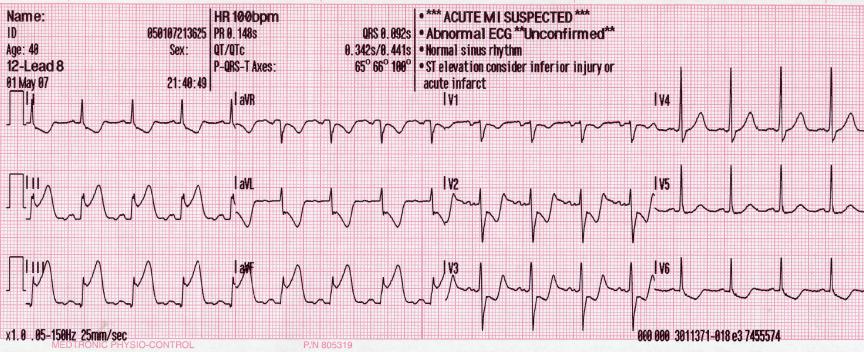
Electrocardiogram With Pardee Waves. Pardee waves indicate acute myocardial infarction in the inferior leads II, III, and augmented voltage foot with reciprocal changes in the anterolateral leads.
Glenlarson, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
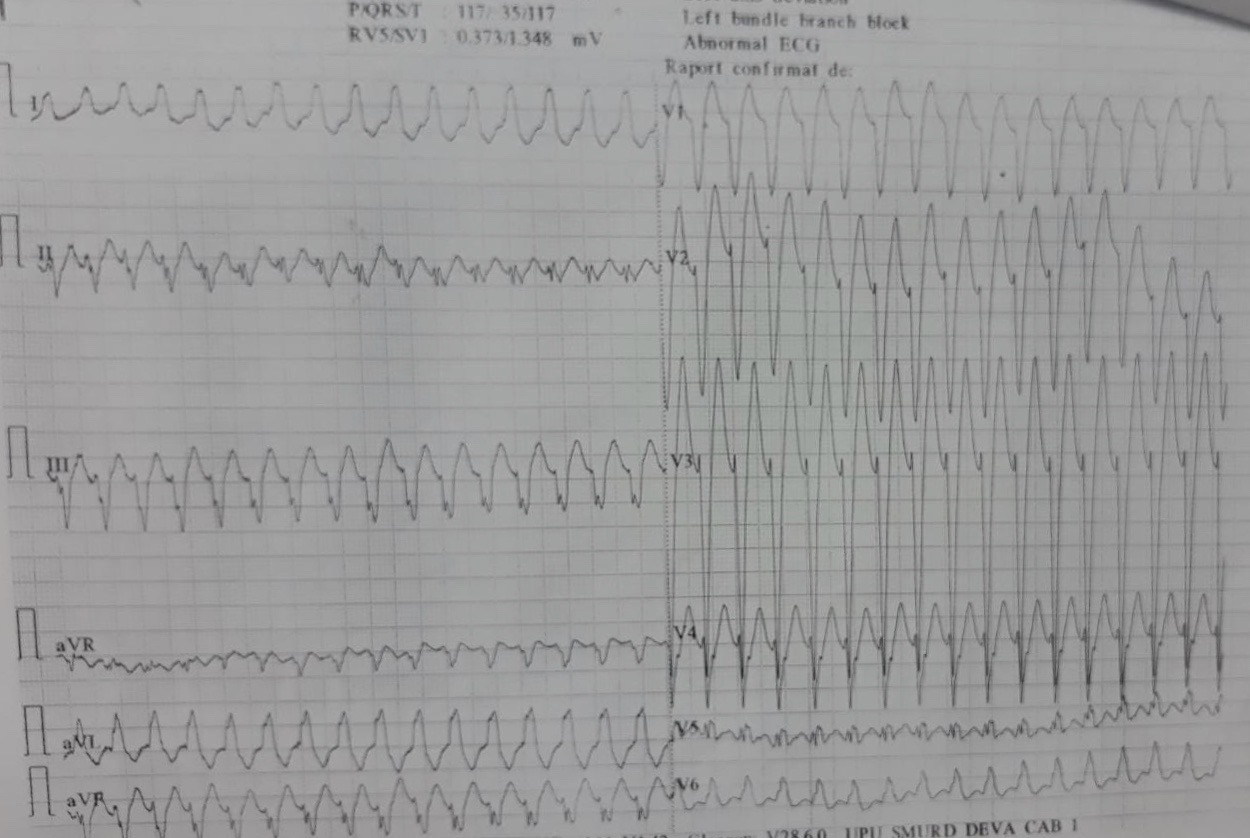
Ischemic Ventricular Tachycardia in a Patient With a Previous Inferior Myocardial Infarction. Life-threatening arrhythmias may occur in inferior myocardial infarction due to ischemia, release of acetylcholine, and reduced blood flow to the atrioventricular node.
Contributed by A Negru, MD
References
Sandjojo E, Jaury VA, Astari YK, Sukmana M, Haeruman RA, Kloping YP. Dopamine and epinephrine for managing complete atrioventricular block due to nonreperfused acute inferior wall myocardial infarction in a rural hospital: A case report. SAGE open medical case reports. 2021:9():2050313X21996113. doi: 10.1177/2050313X21996113. Epub 2021 Mar 15 [PubMed PMID: 33796312]
Level 3 (low-level) evidenceAydin F, Turgay Yildirim O, Dagtekin E, Huseyinoglu Aydin A, Aksit E. Acute Inferior Myocardial Infarction Caused by Lightning Strike. Prehospital and disaster medicine. 2018 Dec:33(6):658-659. doi: 10.1017/S1049023X18000705. Epub 2018 Aug 29 [PubMed PMID: 30156178]
Lévy S. Bundle branch blocks and/or hemiblocks complicating acute myocardial ischemia or infarction. Journal of interventional cardiac electrophysiology : an international journal of arrhythmias and pacing. 2018 Aug:52(3):287-292. doi: 10.1007/s10840-018-0430-3. Epub 2018 Aug 22 [PubMed PMID: 30136134]
Balasubramanian K, Ramachandran B, Subramanian A, Balamurugesan K. Combined ST Elevation in a Case of Acute Myocardial Infarction: How to Identify the Infarct-related Artery? International journal of applied & basic medical research. 2018 Jul-Sep:8(3):184-186. doi: 10.4103/ijabmr.IJABMR_365_16. Epub [PubMed PMID: 30123751]
Level 3 (low-level) evidenceBouhuijzen LJ, Stoel MG. Inferior acute myocardial infarction with anterior ST-segment elevations. Netherlands heart journal : monthly journal of the Netherlands Society of Cardiology and the Netherlands Heart Foundation. 2018 Oct:26(10):515-516. doi: 10.1007/s12471-018-1147-8. Epub [PubMed PMID: 30105594]
Aguiar Rosa S, Timóteo AT, Ferreira L, Carvalho R, Oliveira M, Cunha P, Viveiros Monteiro A, Portugal G, Almeida Morais L, Daniel P, Cruz Ferreira R. Complete atrioventricular block in acute coronary syndrome: prevalence, characterisation and implication on outcome. European heart journal. Acute cardiovascular care. 2018 Apr:7(3):218-223. doi: 10.1177/2048872617716387. Epub 2017 Jun 15 [PubMed PMID: 28617040]
Zhou P, Wu Y, Wang M, Zhao Y, Yu Y, Waresi M, Li H, Jin B, Luo X, Li J. Identifying the culprit artery via 12-lead electrocardiogram in inferior wall ST-segment elevation myocardial infarction: A meta-analysis. Annals of noninvasive electrocardiology : the official journal of the International Society for Holter and Noninvasive Electrocardiology, Inc. 2023 Jan:28(1):e13016. doi: 10.1111/anec.13016. Epub 2022 Nov 1 [PubMed PMID: 36317727]
Level 1 (high-level) evidenceRoshdy HS, El-Dosouky II, Soliman MH. High-risk inferior myocardial infarction: Can speckle tracking predict proximal right coronary lesions? Clinical cardiology. 2018 Jan:41(1):104-110. doi: 10.1002/clc.22859. Epub 2018 Jan 29 [PubMed PMID: 29377172]
Nikus K, Birnbaum Y, Fiol-Sala M, Rankinen J, de Luna AB. Conduction Disorders in the Setting of Acute STEMI. Current cardiology reviews. 2021:17(1):41-49. doi: 10.2174/1573403X16666200702121937. Epub [PubMed PMID: 32614749]
Isailă OM, Ion OM, Luta R, Catinas R, Ionita A, Haisan D, Hostiuc S. Postmortem Immunohistochemical Findings in Early Acute Myocardial Infarction: A Systematic Review. International journal of molecular sciences. 2024 Jul 11:25(14):. doi: 10.3390/ijms25147625. Epub 2024 Jul 11 [PubMed PMID: 39062865]
Level 1 (high-level) evidenceGao Q, Bie F, Hu Y, Chen Y, Yang B. Characteristics and mechanism of reciprocal ST-segment depression in acute ST segment elevation myocardial infarction: Reciprocal ST-segment depression and ST segment elevation myocardial infarction. Medicine. 2022 Nov 4:101(44):e31238. doi: 10.1097/MD.0000000000031238. Epub [PubMed PMID: 36343047]
Bischof JE, Worrall C, Thompson P, Marti D, Smith SW. ST depression in lead aVL differentiates inferior ST-elevation myocardial infarction from pericarditis. The American journal of emergency medicine. 2016 Feb:34(2):149-54. doi: 10.1016/j.ajem.2015.09.035. Epub 2015 Oct 3 [PubMed PMID: 26542793]
Glancy DL, Doghmi W. Use of indicative and reciprocal electrocardiographic changes to help localize the site of coronary occlusion. Proceedings (Baylor University. Medical Center). 2001 Jan:14(1):104-5 [PubMed PMID: 16369596]
Albaghdadi A, Teleb M, Porres-Aguilar M, Porres-Munoz M, Marmol-Velez A. The dilemma of refractory hypoxemia after inferior wall myocardial infarction. Proceedings (Baylor University. Medical Center). 2018 Jan:31(1):67-69. doi: 10.1080/08998280.2017.1401347. Epub 2018 Feb 1 [PubMed PMID: 29686558]
Sibbing D, Aradi D, Jacobshagen C, Gross L, Trenk D, Geisler T, Orban M, Hadamitzky M, Merkely B, Kiss RG, Komócsi A, Dézsi CA, Holdt L, Felix SB, Parma R, Klopotowski M, Schwinger RHG, Rieber J, Huber K, Neumann FJ, Koltowski L, Mehilli J, Huczek Z, Massberg S, TROPICAL-ACS Investigators. Guided de-escalation of antiplatelet treatment in patients with acute coronary syndrome undergoing percutaneous coronary intervention (TROPICAL-ACS): a randomised, open-label, multicentre trial. Lancet (London, England). 2017 Oct 14:390(10104):1747-1757. doi: 10.1016/S0140-6736(17)32155-4. Epub 2017 Aug 28 [PubMed PMID: 28855078]
Level 1 (high-level) evidenceBahramali E, Askari A, Zakeri H, Farjam M, Dehghan A, Zendehdel K. Fasa Registry on Acute Myocardial Infarction (FaRMI): Feasibility Study and Pilot Phase Results. PloS one. 2016:11(12):e0167579. doi: 10.1371/journal.pone.0167579. Epub 2016 Dec 1 [PubMed PMID: 27907128]
Level 2 (mid-level) evidenceD'Ascenzo F, Caranzano I, De Filippo O, Giacobbe F, Leone AM, Sanavia T, Ravetti E, Ugo F, Trani C, Amabile N, Sandrone S, Aurigemma C, Souteyrand G, Capodanno D, Borzillo I, Bruno F, Boccuzzi G, Fariselli P, De Ferrari GM, Iannaccone M, Burzotta F. Phenomapping-derived selection of fractional flow reserve or optical coherence tomography to personalise percutaneous coronary intervention. Open heart. 2025 Sep 17:12(2):. doi: 10.1136/openhrt-2025-003453. Epub 2025 Sep 17 [PubMed PMID: 40967674]
Udroiu CA, Cotoban A, Ursulescu A, Siliste C, Vinereanu D. Interdisciplinary Approach in a Complex Case of STEMI. Maedica. 2014 Dec:9(4):382-6 [PubMed PMID: 25705309]
Level 3 (low-level) evidenceMartin D, Bekiaris B, Hansen G. Mobile emergency simulation training for rural health providers. Rural and remote health. 2017 Jul-Sep:17(3):4057. doi: 10.22605/RRH4057. Epub 2017 Oct 17 [PubMed PMID: 29040811]
Kiani F, Hesabi N, Arbabisarjou A. Assessment of Risk Factors in Patients With Myocardial Infarction. Global journal of health science. 2015 May 28:8(1):255-62. doi: 10.5539/gjhs.v8n1p255. Epub 2015 May 28 [PubMed PMID: 26234995]
Li H, Guo W, Dai W, Li L. Short-versus long-term dual antiplatelet therapy after second-generation drug-eluting stent implantation: a systematic review and meta-analysis of randomized controlled trials. Drug design, development and therapy. 2018:12():1815-1825. doi: 10.2147/DDDT.S165435. Epub 2018 Jun 22 [PubMed PMID: 29970956]
Level 1 (high-level) evidenceGinanjar E, Yulianto Y. ST Elevation in Lead aVR and Its Association with Clinical Outcomes. Acta medica Indonesiana. 2017 Oct:49(4):347-350 [PubMed PMID: 29348386]
Level 2 (mid-level) evidenceAltıntaş B, Yaylak B, Ede H, Altındağ R, Baysal E, Bilge Ö, Çiftçi H, Adıyaman MŞ, Karahan MZ, Kaya I, Çevik K. Impact of right ventricular diastolic dysfunction on clinical outcomes in inferior STEMI. Herz. 2019 Apr:44(2):155-160. doi: 10.1007/s00059-017-4631-9. Epub 2017 Oct 9 [PubMed PMID: 28993840]
Level 2 (mid-level) evidence