Introduction
Hypothermia is defined as a decrease in body temperature below 35 °C. The condition is common in cold geographic areas and during cooler months, though it can also develop in locations with milder climates.[1] Hypothermia affects all organ systems. Presenting symptoms depend on the severity of the condition.
The hypothalamus integrates signals from peripheral and central thermoreceptors and coordinates autonomic and behavioral responses to cold exposure. Early cold-defense mechanisms include peripheral vasoconstriction, increased sympathetic activity, and increased muscle tone. As cold stress intensifies, shivering thermogenesis substantially increases metabolic heat production, potentially several-fold above resting metabolic rate.[2]
Newborns lack the shivering mechanism due to incomplete development of the nervous system. However, brown fat helps generate heat in newborns' bodies. Brown fat's thermogenin (UCP1) increases proton permeability of the inner mitochondrial membrane. The resulting hydrogen-ion leak uncouples oxidative phosphorylation from ATP production, dissipating energy as heat.[3]
Thyroid, catecholamine, and adrenal hormones also increase in response to cold stress. Cold-induced, sympathetically mediated peripheral vasoconstriction reduces heat loss. Behavioral changes such as adding more clothing, seeking shelter, starting a fire, and exercising help retain or generate body heat.
Patients with mild hypothermia have a core body temperature ranging from 32 to 35 °C (90 to 95 °F). For moderate hypothermia, the core temperature falls between 28 and 32 °C (82-90 °F). Severe or profound hypothermia is defined as a core body temperature below 28 °C (82 °F). [4]
The Durrer et al. Swiss Staging System employs a hypothermia staging scheme for rescue operations to identify which patients may benefit from resuscitation.[5] As hypothermia progresses, the risk of morbidity and mortality increases significantly. Recently, the International Commission for Mountain Emergency Medicine recommended a revised Swiss staging system that focuses on responsiveness and the risk of cardiac arrest, rather than solely on estimated core temperature (see under "Staging" below). [6]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Hypothermia occurs when the body releases more heat than it absorbs or generates. Vital factors that help retain heat in the body include regulation by the central and peripheral nervous systems, as well as behavioral adaptations.[7][8]
Extremes of age, hypoglycemia, malnutrition, and various endocrine disorders are common reasons for inadequate heat production. Conditions resulting in heat loss include inflammatory skin disorders such as psoriasis and burns, as well as excessive peripheral vasodilation from nervous system injuries. Cerebrovascular accidents, neurodegenerative disorders, and drug abuse may disrupt the hypothalamic thermoregulation function. Hypothermia may also be iatrogenic, often from drugs like general anesthetics, beta-blockers, meperidine, clonidine, neuroleptics, and alcohol.
Accidental hypothermia may develop not only from conditions that impair heat production or increase heat loss, but also from factors that reduce an individual's ability to recognize or respond appropriately to cold exposure. Cognitive impairment associated with dementia, alcohol intoxication, sedative use, substance misuse, or metabolic encephalopathies can diminish protective behavioral responses. Social and environmental factors, including inadequate housing, insufficient clothing, homelessness, poverty, and prolonged outdoor exposure, may further increase risk. Individuals with limited mobility, such as neonates and patients with stroke, spinal cord injury, hip fracture, or other neuromuscular disorders, are particularly vulnerable because they may be unable to seek shelter, add clothing layers, or generate heat through activity. Among otherwise healthy young adults, alcohol intoxication remains one of the most frequently identified contributors to accidental hypothermia.[9][10]
Epidemiology
Accidental hypothermia remains an important cause of preventable morbidity and mortality. According to recent CDC data, 1,024 deaths in the United States were attributed to excessive cold or hypothermia in 2023, with most occurring during the colder months. [11] Although the true incidence is likely underestimated because mild cases may go unrecognized and reporting practices vary, population-based studies suggest that accidental hypothermia is associated with substantial mortality. A 2021 Danish nationwide cohort study reported an annual incidence of approximately 4.4 cases per 100,000 population and a one-year mortality rate of 27%, with alcohol intoxication identified as the most common associated diagnosis. [12]
Pathophysiology
The body's core temperature arises from the balance between heat produced by the body and heat lost to the surroundings. The normal value ranges from 36.5 °C to 37.5 °C. Four mechanisms are responsible for heat loss: radiation, conduction, convection, and evaporation.
Heat radiation occurs when the body emits electromagnetic energy into the surroundings. Heat conduction is the transfer of thermal energy between objects in contact. Heat loss by convection entails air molecules moving past a heated object. Evaporation happens when heat transforms liquid into gas, as when the thermal energy from the skin vaporizes sweat.
While normal body heat loss is most often due to radiation, hypothermia is more likely to result from exposure to cold air (convection), contact with cold water (conduction), and excessive sweating (evaporation).[13]
The body initially increases metabolism, ventilation, and cardiac output to maintain function when the ambient temperature drops. Heat loss can overwhelm the body and disrupt the shivering mechanism in the absence of external warming. Multiple organ systems, including neurologic, metabolic, and cardiac, will cease to function, ultimately leading to death.[14] Sinoatrial disturbances may result in atrial or ventricular fibrillation.
History and Physical
Hypothermia may result in cardiorespiratory arrest. A quick primary survey—assessing the airway, breathing, circulation, disability, and exposure (ABCDE)—should reveal the need for immediate resuscitation. Patients presenting with unconsciousness, pulselessness, and apnea must be given resuscitative care immediately, regardless of the cause. Once stabilized or if emergency conditions have been ruled out, a more detailed investigation may be started.
People who have suffered hypothermia typically have a history of recent significant cold exposure. The presenting symptoms depend on the core body temperature, which must be obtained accurately to diagnose and manage the condition effectively. When used correctly, epitympanic thermistor probes reflect the carotid artery temperature and can be reasonably reliable.
Rectal and bladder temperature measurements are reasonable in conscious individuals with mild to moderate hypothermia. However, these approaches may not be appropriate for critically ill patients during rewarming, as they lag behind the true core temperature. In the prehospital setting, rectal and bladder temperature monitoring may further expose the patient and worsen hypothermia. Esophageal temperature measurement is most accurate when the probe is in the lower third of the esophagus, but it should only be performed in patients with an advanced airway in place.
Oral temperature is only useful in ruling out hypothermia, as most commercially available thermometers cannot read under 35 °C. Standard tympanic infrared thermometers are also unreliable.
Core body temperature must be obtained immediately, as it is critical for determining appropriate management. This parameter correlates significantly with the symptoms of each stage of hypothermia, though it can be challenging to obtain in the prehospital setting.[15]
In mild hypothermia, the core body temperature ranges from 32 to 35 °C (90-95 °F). The symptoms are often subtle and nonspecific, including hunger, nausea, fatigue, shivering, and pale, dry skin. Patients may also have increased muscle tone, blood pressure, heart rate, and respiration as the body attempts to promote thermogenesis. Shivering is usually present unless the patient's energy stores have been depleted, as in cases of malnutrition or underlying endocrinopathy. Potential neurologic symptoms include cognitive decline, memory and judgment impairment, ataxia, and dysarthria. "Cold diuresis" may occur due to peripheral vasoconstriction, leading to increased diuresis and subsequent volume depletion.
Patients with moderate hypothermia have a core body temperature of 28 to 32 °C (82-90 °F). Cognitive decline and lethargy are common. CNS depression may lead to hyporeflexia, with the pupils being less responsive and dilated. Hypotension, bradycardia, and bradypnea may ensue. Shivering typically ceases when the core temperature reaches 30 to 32 °C, at which point, paradoxical undressing may be observed. Susceptibility to dysrhythmias increases, with atrial fibrillation being the most common.
Individuals with severe hypothermia have a core body temperature of less than 28 °C (82 °F). Cerebral blood flow continues to decline until patients become unresponsive. Blood pressure, heart rate, and cardiac output also continue to decrease. Atrial and junctional dysrhythmias may be present. Pulmonary congestion, oliguria, and areflexia may occur. The condition may result in cardiorespiratory failure.[16]
All patients with suspected hypothermia should undergo a comprehensive history and physical examination to identify local cold-related injuries, associated trauma, and underlying medical conditions that may have contributed to heat loss or impaired thermoregulation. Clinicians should consider alternative or concurrent diagnoses when the patient's presentation appears disproportionate to the degree of hypothermia, including sepsis, hypothyroidism, adrenal insufficiency, hypoglycemia, carbon monoxide poisoning, malnutrition, intoxication, and drug overdose. Numerous medications and substances, including beta-blockers, clonidine, antipsychotic agents, sedative-hypnotics, ethanol, and anesthetic medications, may impair thermoregulation, blunt physiologic responses to cold stress, or alter behavior, thereby increasing the risk of hypothermia.[17][4]
Evaluation
Again, for all potentially unstable patients, the trauma ABCs should be the clinician's initial focus of evaluation. Remove all clothing after completing the primary survey and place dry, warm blankets over the patient's fully exposed chest. Standard laboratory evaluation should include finger-stick glucose, complete blood count, and a basic metabolic panel.
A rise in hemoglobin and hematocrit may be due to cold diuresis from impaired antidiuretic hormone secretion. Glucose levels do not follow a specific pattern unless hypo- or hyperglycemia is triggered in patients with diabetes mellitus. Electrolytes and other laboratory abnormalities should be monitored serially during resuscitation and rewarming, with testing frequency guided by the patient's clinical condition and severity of hypothermia.
A coagulation panel must be obtained when invasive procedures are deemed necessary. However, this test generally requires the patient's in vivo temperature to be 37 °C to be reliable. Fibrinogen should also be checked to rule out disseminated intravascular coagulation (DIC). Serum lactate, creatinine kinase, troponin, thyroid-stimulating hormone (TSH), cortisol, toxicology screen, fibrinogen, lipase, and magnesium may be obtained to find non-environmental causes of hypothermia.
Imaging should be dictated by clinical need, as some patients may have had an inciting incident like trauma or cerebrovascular accident that led to a significant body temperature drop. Chest x-ray may be normal in the absence of trauma or an underlying thoracic condition. Bedside ultrasound may be used to confirm cardiac activity and volume status. Head computed tomography (CT) may benefit individuals with altered mental status not proportional to the severity of hypothermia, especially if trauma or stroke is suspected.[16]
Electrocardiography (ECG) should be obtained in all patients with hypothermia because cardiac conduction abnormalities and dysrhythmias are common. Hypothermia slows myocardial conduction and repolarization, resulting in prolongation of the PR, QRS, and QT intervals. An elevated J point may also be present, producing the characteristic Osborn (J) wave (see Image. Osborn Wave). Osborn waves are most commonly observed in the precordial leads, and their amplitude generally increases as core temperature decreases. However, this finding is not specific to hypothermia and may occur in other clinical conditions. Atrial fibrillation is the most common dysrhythmia associated with hypothermia, while severe hypothermia increases bradycardia and susceptibility to ventricular arrhythmias, including ventricular fibrillation. [4]
Treatment / Management
Management of hypothermia focuses on preventing further heat loss, supporting the airway, breathing, and circulation, and initiating rewarming appropriate to the severity of illness. Wet clothing should be removed promptly and replaced with dry insulation or warming blankets.[18][19] After immediate threats have been addressed, clinicians should obtain a focused history, assess mental status, perform a physical examination, and measure core temperature. Measure core temperature using a thermometer capable of accurately measuring temperatures below 35°C, such as a low-reading esophageal, bladder, rectal, or epitympanic thermistor probe when available. (B3)
Patients with moderate or severe hypothermia should be handled gently because rough movement may increase myocardial irritability and precipitate fatal dysrhythmias.[20] Clinicians should evaluate for trauma, intoxication, infection, endocrine disorders, hypoglycemia, and other conditions that may contribute to or mimic hypothermia. Documented or strongly suspected hypoglycemia should be treated with oral glucose if the patient can safely swallow or with intravenous dextrose when indicated. (B3)
Rewarming strategies include passive external rewarming, active external rewarming, and active internal rewarming. Passive external rewarming with removal of wet clothing, insulation, and a warm environment is appropriate for many patients with mild hypothermia who are alert, hemodynamically stable, and able to generate heat through shivering.[21] Shivering can substantially increase metabolic heat production but requires adequate energy stores and may increase oxygen demand in patients with limited cardiopulmonary reserve. (B3)
Active external rewarming is used for moderate hypothermia, severe hypothermia with preserved circulation, and mild hypothermia that does not improve with passive measures. Forced-air warming systems and heat packs applied to the trunk, axillae, chest, and back can reduce heat loss and transfer heat by convection or conduction. Care should be taken to avoid burns and to maintain continuous clinical and cardiac monitoring.[22]
Warm-water immersion may be considered in selected, stable patients, but is often difficult to perform safely in clinical settings because monitoring, vascular access, and resuscitation may be limited. Extremity warming may be useful in mild hypothermia, but rapid peripheral vasodilation in more severe hypothermia can contribute to hemodynamic instability.
Active internal rewarming techniques include warmed humidified oxygen, warmed intravenous fluids, and warm lavage of body cavities such as the bladder, stomach, thorax, or peritoneum. Warmed intravenous fluids, typically 38 to 42 °C, are useful for preventing additional heat loss and treating volume depletion, although they provide only modest rewarming when used alone. Pleural or peritoneal lavage may be considered in selected patients with severe hypothermia when less invasive methods are insufficient, but these procedures require specialized expertise and careful monitoring.[4]
Extracorporeal and intravascular rewarming techniques may be considered for patients with severe accidental hypothermia, particularly when there is cardiac arrest, severe hemodynamic instability, ventricular dysrhythmia, or failure to respond to less invasive rewarming. Available methods include renal replacement therapy, cardiopulmonary bypass, and extracorporeal membrane oxygenation (ECMO), although local availability and transfer logistics often determine which option is feasible.
Renal replacement therapy, including hemodialysis or continuous renal replacement therapy, may provide active internal rewarming in patients who have adequate circulation and blood pressure. The mean rewarming rate for this method has been reported as 1.9 °C per hour and has the benefit of widespread availability. These methods do not provide full cardiopulmonary support and are therefore not appropriate as the primary rewarming strategy for hypothermic cardiac arrest. Older techniques such as continuous arteriovenous rewarming are now much less commonly used and have largely been replaced by modern extracorporeal life support and renal replacement approaches.[23](A1)
Cardiopulmonary bypass surgery and veno-arterial (VA) ECMO are the most effective but highly invasive rewarming methods. These procedures are reserved for patients in hypothermic cardiac arrest, hemodynamically unstable individuals, and people unresponsive to less invasive rewarming techniques. Reports vary on the extent to which cardiopulmonary bypass and ECMO can raise core temperature, with some studies citing up to 6 °C per hour. These methods can simultaneously improve oxygenation and circulatory support. However, not all facilities can offer these methods, and the transfer of highly unstable patients can be difficult and risky. Cardiopulmonary bypass and ECMO also require systemic anticoagulation, predisposing patients (who may have concomitant trauma) to spontaneous bleeding.[23] (A1)
The ICE-CRASH published in 2023 showed that ECMO improved survival and neurological outcomes in accidental hypothermia patients with cardiac arrest, but not in accidental hypothermia patients without cardiac arrest. In non-cardiac arrest patients, ECMO was found to increase bleeding complications and decrease the number of event-free days.[24] (B2)
Prognostication in hypothermic cardiac arrest should not be based on core temperature alone. The Hypothermia Outcome Prediction after Extracorporeal Life Support (HOPE) score can help estimate the survival probability for patients with hypothermic cardiac arrest who are resuscitated with Extracorporeal Life Support (ECLS) rewarming. The HOPE score incorporates age, sex, mechanism of hypothermia, core temperature, serum potassium, and duration of cardiopulmonary resuscitation. Proceeding with ECLS is recommended if the HOPE score is ≥10%. Current reviews and resuscitation guidance recommend using validated prognostic tools such as the HOPE score, along with clinical judgment, to guide ECLS decisions rather than excluding patients solely because of prolonged arrest time or very low body temperature.[25]
Differential Diagnosis
An abnormally low body temperature may result from primary environmental exposure or secondary hypothermia due to impaired thermoregulation, decreased heat production, increased heat loss, or impaired behavioral response to cold.[17]
Table. Common Causes of Hypothermia
|
Etiologic Category |
Representative Causes |
Mechanism or Clinical Impact |
|
Neurologic or central thermoregulatory failure |
Cerebrovascular accident, CNS trauma, hypothalamic dysfunction, spinal cord injury |
May impair central temperature regulation, mobility, or behavioral response to cold |
|
Endocrine or metabolic disorders |
Hypoglycemia, diabetic or alcoholic ketoacidosis, adrenal insufficiency, hypopituitarism, hypothyroidism, lactic acidosis |
May reduce heat production, alter mental status, or contribute to hemodynamic instability |
|
Infection and systemic illness |
Sepsis, major infection, shock, multisystem trauma, cardiopulmonary disease, malignancy |
May cause secondary hypothermia and worsen prognosis |
|
Toxicologic or medication-related causes |
Alcohol intoxication, sedatives, opioids, neuroleptics, beta-blockers, clonidine, anesthetic agents, and other drug overdoses |
May impair shivering, vasoconstriction, cognition, mobility, or exposure avoidance |
|
Peripheral or dermatologic heat loss |
Burns, exfoliative skin disease, acute spinal cord transection, neuropathy |
May increase heat loss or impair protective responses |
|
Iatrogenic or situational causes |
Cold fluid infusion, heat-stroke treatment, emergency childbirth, inadequate shelter or clothing, immobility, extremes of age |
May cause or worsen hypothermia and should be addressed during management |
A thorough evaluation should identify the underlying cause of hypothermia, detect associated trauma or cold-related injury, and guide targeted treatment in addition to rewarming.
Staging
The Swiss Staging System was originally developed by Durrer et al. to estimate hypothermia severity based on clinical findings and approximate core temperature when direct temperature measurement is unavailable. The Revised Swiss Staging System (RSS) places greater emphasis on neurologic responsiveness and the risk of hypothermic cardiac arrest, using the AVPU (Alert, Verbal, Pain, Unresponsive) scale rather than shivering and estimated temperature alone. The table below compares the original and revised staging systems and their associated risk of hypothermic cardiac arrest[6]
Table. Comparison of Original and Revised Swiss Hypothermia Staging Systems
|
Original Swiss Staging System (Durrer et al, 2003) |
Clinical Findings (Estimated Core Temperature) |
Revised Swiss Staging System (RSS) |
Cardiac Arrest Risk |
|
Stage 1 (Mild Hypothermia) |
Patient is awake and responds appropriately with shivering (35–32°C) |
"Alert" on AVPU scale
|
Low |
|
Stage 2 (Moderate Hypothermia) |
Patient is not fully alert, responds to voice, without shivering (32–28°C) |
"Verbal" response on the AVPU scale |
Moderate |
|
Stage 3 (Severe hypothermia) |
Not responding to voice but with vital signs present (28–24°C) |
"Pain" response or "Unresponsive" on AVPU scale with detectable vital signs |
High |
|
Stage 4 (Severe/Profound hypothermia) |
Unresponsive and no pulse or respirations (<24°C) |
"Unresponsive" on the AVPU scale with no detectable vital signs |
Hypothermic cardiac arrest |
Table adapted from Musi ME, Sheets A, Zafren K, et al. Clinical staging of accidental hypothermia: recommendations of the International Commission for Mountain Emergency Medicine (ICAR MEDCOM). Wilderness Environ Med. 2021;32(4):571-573. Modified for educational purposes.[6]
Prognosis
Severe hypothermia can be fatal, but favorable neurologic recovery is possible, particularly in patients with primary accidental hypothermia who receive prompt recognition, appropriate rewarming, and treatment of reversible causes. Prognosis is influenced by the mechanism of hypothermia, duration of arrest or low-flow state, presence of asphyxia or trauma, underlying illness, serum potassium, core temperature, and response to resuscitation. Hemodynamically stable patients with primary hypothermia generally have excellent outcomes when treated with active external or minimally invasive rewarming. In selected patients with hypothermic cardiac arrest, extracorporeal life support, particularly VA-ECMO, is associated with survival and favorable neurologic recovery in a substantial proportion of cases. Full neurological recovery has been reported in accidental hypothermia reaching 14 °C.[17]
Recent outcome data suggest that advanced age and coexisting medical conditions are important predictors of mortality. In one study, non-survivors were, on average, 6.3 years older than survivors, and increasing age was significantly associated with decreased 30-day survival. Additionally, at least one comorbid illness was present in 78% of patients. [26]
Hypothermia-related dysrhythmias may be refractory to standard advanced cardiac life support until rewarming has progressed. Ventricular fibrillation and asystole should prompt continued resuscitation and active rewarming when the clinical scenario is compatible with survivable accidental hypothermia. Serum potassium may provide important prognostic information in patients with hypothermic cardiac arrest. Markedly elevated potassium levels, particularly values exceeding 12 mEq/L, are generally associated with extensive cellular injury and poor outcomes; however, potassium concentration should not be used as the sole criterion for terminating resuscitative efforts. Validated tools such as the HOPE score, combined with clinical judgment and the overall clinical context, can help estimate survival probability and guide decisions regarding extracorporeal rewarming. Patients who survive may experience complications such as frostbite, rhabdomyolysis, acute kidney injury, or neurologic injury, requiring ongoing monitoring and follow-up.
Complications
Frostbite is a complication of hypothermia that may potentially lead to limb loss if not treated in a timely fashion. This lesion is a form of dry gangrene. A secondary infection can lead to wet gangrene. Infection by the anaerobic species Clostridium perfringens produces gas, manifesting as crepitus in the skin. Frostbite infection may lead to amputation if refractory to medical treatment.
Other complications of hypothermia include the following:[14]
- Cold diuresis
- Rhabdomyolysis
- Aspiration
- Hyperkalemia
- Frostbite
- Acute kidney injury
- Pulmonary edema
- Ataxia
- Ventricular and atrial arrhythmias, frequently atrial or ventricular fibrillation, and pulseless electrical activity
- Coma
- Pancreatitis
- Death
Rewarming also produces complications, which include the following:[27][28][29][30][31]
- Takotsubo cardiomyopathy
- Systemic inflammation
- Electrical abnormalities like hyperkalemia, hypophosphatemia, hypomagnesemia, and hypocalcemia
- Rhabdomyolysis
- Ventricular and atrial arrhythmias (A. fibrillation, ventricular arrhythmia, PEA)
- Infections like pneumonia
- Platelet dysfunction from thrombocytopenia to platelet aggregation and thrombosis.
- Alterations in glucose homeostasis from reduced glucose utilization to insulin resistance
Prompt recognition and appropriate treatment help reduce the likelihood of complications.
Deterrence and Patient Education
Many cases of accidental hypothermia are preventable through patient education and risk-factor modification. Clinicians should counsel patients to limit unnecessary exposure during extreme cold weather and to wear appropriate layered clothing that provides insulation while protecting against wind and moisture. Individuals participating in outdoor activities such as hiking, skiing, mountaineering, or snowboarding should monitor weather conditions, carry emergency supplies, remain adequately nourished and hydrated, and avoid traveling alone when possible.
Particular attention should be directed toward populations at increased risk, including older adults, young children, individuals experiencing homelessness, and patients with cognitive impairment, psychiatric illness, substance use disorders, or chronic medical conditions that affect thermoregulation. Caregivers should ensure that vulnerable individuals have access to appropriate clothing, shelter, heating, and regular wellness checks during periods of cold weather.
Clinicians should also educate patients about the effects of alcohol and certain medications on thermoregulation and judgment, as these factors may increase the risk of accidental hypothermia. Counseling regarding substance misuse, medication safety, and recognition of early symptoms such as shivering, confusion, impaired coordination, and excessive fatigue may facilitate earlier intervention and reduce complications. Community measures, including access to warming centers, safe housing, and adequate home heating, play an important role in preventing cold-related illness and death.
Pearls and Other Issues
The most important points to remember about hypothermia management are the following:
1. Hypothermia arises from inadequate heat retention or excessive heat loss due to environmental exposure, impaired thermoregulation, metabolic disorders, intoxication, trauma, or medication effects. Symptoms range from mild to severe. Severe hypothermia may result in death if not treated promptly.
2. Patients with hypothermia may present with unconsciousness, pulselessness, and lack of respiration. Resuscitation should be initiated immediately in such individuals, as survival with good neurologic outcomes is possible even after prolonged cardiac arrest in selected patients.
3. Most commercial thermometers can only read to a minimum of approximately 34 °C, making a special low-reading thermometer necessary during patient evaluation.
4. The esophageal thermometer is the most accurate method of determining core temperature in critically ill and intubated patients.
5. Rectal temperatures may lag behind true core temperature changes and can take up to 1 hour to reflect changes during rewarming.
6. The Revised Swiss Staging System emphasizes neurologic responsiveness and the risk of hypothermic cardiac arrest rather than estimated core temperature alone and may help guide management decisions.
7. Coagulation studies may appear normal despite clinically significant coagulopathy because laboratory testing is typically performed at 37 °C.
8. Electrocardiography may demonstrate Osborn (J) waves, bradycardia, atrial fibrillation, QT prolongation, and other conduction abnormalities in patients with hypothermia.
9. Passive and active external rewarming are effective for most patients. Active internal and extracorporeal rewarming techniques should be considered for patients with moderate-to-severe hypothermia, hemodynamic instability, or cardiac arrest.
10. Cardiopulmonary bypass and venoarterial extracorporeal membrane oxygenation (ECMO) are the most invasive but effective methods for rewarming patients with severe hypothermia and can provide both circulatory and respiratory support.
11. The HOPE score may assist clinicians in identifying appropriate candidates for extracorporeal life support and should be used alongside clinical judgment when evaluating patients with hypothermic cardiac arrest.
12. If the patient fails to rewarm despite appropriate therapy, underlying causes such as hypoglycemia, infection, hypothyroidism, adrenal insufficiency, intoxication, or ongoing environmental exposure should be investigated.
Importantly, hypothermia is often preventable. Patient education regarding cold-weather precautions, appropriate clothing, alcohol avoidance during exposure, and early recognition of symptoms is particularly important for vulnerable populations.
Enhancing Healthcare Team Outcomes
Hypothermia is defined as a core body temperature below 35°C and can result from environmental exposure, impaired thermoregulation, metabolic disorders, trauma, intoxication, or medication effects. Clinical manifestations range from mild symptoms such as shivering and cognitive impairment to severe hypothermia with cardiac dysrhythmias, hemodynamic instability, and cardiorespiratory arrest. Accurate core temperature assessment, appropriate staging, identification of underlying causes, and prompt rewarming are essential for reducing morbidity and mortality. Management strategies include passive and active rewarming techniques, while extracorporeal life support may be indicated for selected patients with severe hypothermia or hypothermic cardiac arrest. Contemporary prognostic tools, such as the HOPE score, can assist in identifying candidates for extracorporeal rewarming.
Optimal outcomes require coordinated interprofessional care. Emergency physicians, primary care clinicians, and advanced practitioners evaluate severity, direct treatment, and identify underlying etiologies. Nurses provide continuous monitoring, administer therapies, and communicate changes in patient status. Pharmacists assist with medication management and recognition of drug-related causes of hypothermia. Critical care, cardiology, nephrology, and cardiothoracic specialists collaborate when advanced monitoring, renal replacement therapy, ECMO, or management of complications is required. Effective communication, timely referral, shared decision-making, and coordinated follow-up help reduce complications, improve patient safety, and support recovery and prevention strategies.
Media
(Click Image to Enlarge)
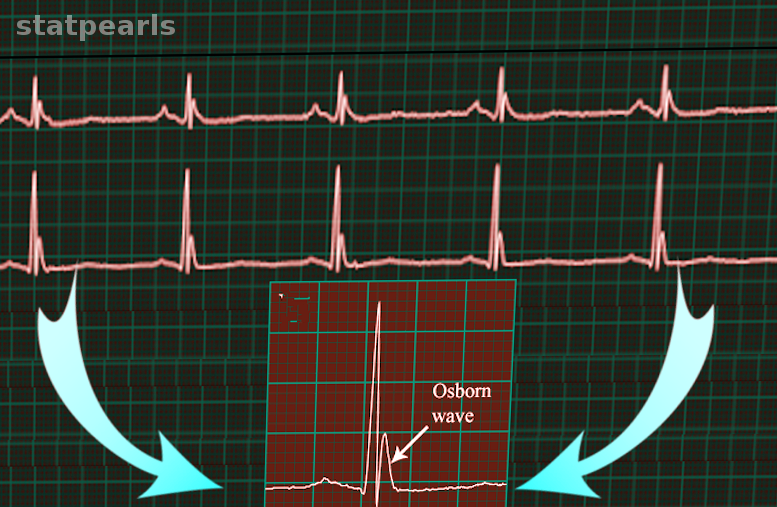
Osborn Wave On Electrocardiography. This electrocardiogram (ECG) strip shows Osborn waves.
Image courtesy S. Bhimji MD
References
Kempainen RR, Brunette DD. The evaluation and management of accidental hypothermia. Respiratory care. 2004 Feb:49(2):192-205 [PubMed PMID: 14744270]
Tan CL, Knight ZA. Regulation of Body Temperature by the Nervous System. Neuron. 2018 Apr 4:98(1):31-48. doi: 10.1016/j.neuron.2018.02.022. Epub [PubMed PMID: 29621489]
Crichton PG, Lee Y, Kunji ER. The molecular features of uncoupling protein 1 support a conventional mitochondrial carrier-like mechanism. Biochimie. 2017 Mar:134():35-50. doi: 10.1016/j.biochi.2016.12.016. Epub 2017 Jan 3 [PubMed PMID: 28057583]
Paal P, Pasquier M, Darocha T, Lechner R, Kosinski S, Wallner B, Zafren K, Brugger H. Accidental Hypothermia: 2021 Update. International journal of environmental research and public health. 2022 Jan 3:19(1):. doi: 10.3390/ijerph19010501. Epub 2022 Jan 3 [PubMed PMID: 35010760]
Durrer B, Brugger H, Syme D, International Commission for Mountain Emergency Medicine. The medical on-site treatment of hypothermia: ICAR-MEDCOM recommendation. High altitude medicine & biology. 2003 Spring:4(1):99-103 [PubMed PMID: 12713717]
Level 1 (high-level) evidenceMusi ME, Sheets A, Zafren K, Brugger H, Paal P, Hölzl N, Pasquier M. Clinical staging of accidental hypothermia: The Revised Swiss System: Recommendation of the International Commission for Mountain Emergency Medicine (ICAR MedCom). Resuscitation. 2021 May:162():182-187. doi: 10.1016/j.resuscitation.2021.02.038. Epub 2021 Mar 3 [PubMed PMID: 33675869]
Epstein E, Anna K. Accidental hypothermia. BMJ (Clinical research ed.). 2006 Mar 25:332(7543):706-9 [PubMed PMID: 16565126]
Paal P, Brugger H, Strapazzon G. Accidental hypothermia. Handbook of clinical neurology. 2018:157():547-563. doi: 10.1016/B978-0-444-64074-1.00033-1. Epub [PubMed PMID: 30459025]
Petrone P, Asensio JA, Marini CP. Management of accidental hypothermia and cold injury. Current problems in surgery. 2014 Oct:51(10):417-31. doi: 10.1067/j.cpsurg.2014.07.004. Epub 2014 Jul 29 [PubMed PMID: 25242454]
Davis PR, Byers M. Accidental hypothermia. Journal of the Royal Army Medical Corps. 2005 Dec:151(4):223-33 [PubMed PMID: 16548338]
. QuickStats: Percentage Distribution of Deaths Attributed to Excessive Cold or Hypothermia,* by Month - United States, 2023. MMWR. Morbidity and mortality weekly report. 2025 Feb 27:74(6):107. doi: 10.15585/mmwr.mm7406a6. Epub 2025 Feb 27 [PubMed PMID: 40014663]
Wiberg S, Mortensen AF, Kjaergaard J, Hassager C, Wanscher M. Accidental hypothermia in Denmark: A nationwide cohort study of incidence and outcomes. BMJ open. 2021 May 31:11(5):e046806. doi: 10.1136/bmjopen-2020-046806. Epub 2021 May 31 [PubMed PMID: 34059513]
Zafren K. Out-of-Hospital Evaluation and Treatment of Accidental Hypothermia. Emergency medicine clinics of North America. 2017 May:35(2):261-279. doi: 10.1016/j.emc.2017.01.003. Epub [PubMed PMID: 28411927]
Danzl DF, Pozos RS. Accidental hypothermia. The New England journal of medicine. 1994 Dec 29:331(26):1756-60 [PubMed PMID: 7984198]
Dow J, Giesbrecht GG, Danzl DF, Brugger H, Sagalyn EB, Walpoth B, Auerbach PS, McIntosh SE, Némethy M, McDevitt M, Schoene RB, Rodway GW, Hackett PH, Zafren K, Bennett BL, Grissom CK. Wilderness Medical Society Clinical Practice Guidelines for the Out-of-Hospital Evaluation and Treatment of Accidental Hypothermia: 2019 Update. Wilderness & environmental medicine. 2019 Dec:30(4S):S47-S69. doi: 10.1016/j.wem.2019.10.002. Epub 2019 Nov 15 [PubMed PMID: 31740369]
Level 1 (high-level) evidenceLloyd EL. Accidental hypothermia. Resuscitation. 1996 Sep:32(2):111-24 [PubMed PMID: 8896051]
Brown DJ, Brugger H, Boyd J, Paal P. Accidental hypothermia. The New England journal of medicine. 2012 Nov 15:367(20):1930-8. doi: 10.1056/NEJMra1114208. Epub [PubMed PMID: 23150960]
Haverkamp FJC, Giesbrecht GG, Tan ECTH. The prehospital management of hypothermia - An up-to-date overview. Injury. 2018 Feb:49(2):149-164. doi: 10.1016/j.injury.2017.11.001. Epub 2017 Nov 4 [PubMed PMID: 29162267]
Level 3 (low-level) evidenceAvellanas Chavala ML, Ayala Gallardo M, Soteras Martínez Í, Subirats Bayego E. Management of accidental hypothermia: A narrative review. Medicina intensiva. 2019 Dec:43(9):556-568. doi: 10.1016/j.medin.2018.11.008. Epub 2019 Jan 22 [PubMed PMID: 30683520]
Level 3 (low-level) evidenceSmith TM, Berk AS, Upadhyay H. Severe hypothermia in a patient with spinal cord injury without radiological abnormality. Journal of emergencies, trauma, and shock. 2011 Jul:4(3):421-4. doi: 10.4103/0974-2700.83878. Epub [PubMed PMID: 21887040]
Level 3 (low-level) evidenceSavioli G, Ceresa IF, Bavestrello Piccini G, Gri N, Nardone A, La Russa R, Saviano A, Piccioni A, Ricevuti G, Esposito C. Hypothermia: Beyond the Narrative Review-The Point of View of Emergency Physicians and Medico-Legal Considerations. Journal of personalized medicine. 2023 Dec 5:13(12):. doi: 10.3390/jpm13121690. Epub 2023 Dec 5 [PubMed PMID: 38138917]
Level 3 (low-level) evidencevan Veelen MJ, Brodmann Maeder M. Hypothermia in Trauma. International journal of environmental research and public health. 2021 Aug 18:18(16):. doi: 10.3390/ijerph18168719. Epub 2021 Aug 18 [PubMed PMID: 34444466]
Mendrala K, Kosiński S, Podsiadło P, Pasquier M, Paal P, Mazur P, Darocha T. The Efficacy of Renal Replacement Therapy for Rewarming of Patients in Severe Accidental Hypothermia-Systematic Review of the Literature. International journal of environmental research and public health. 2021 Sep 13:18(18):. doi: 10.3390/ijerph18189638. Epub 2021 Sep 13 [PubMed PMID: 34574562]
Level 1 (high-level) evidenceTakauji S, Hayakawa M, Yamada D, Tian T, Minowa K, Inoue A, Fujimoto Y, Isokawa S, Miura N, Endo T, Irie J, Otomo G, Sato H, Bando K, Suzuki T, Toyohara T, Tomita A, Iwahara M, Murata S, Shimazaki J, Matsuyoshi T, Yoshizawa J, Nitta K, Sato Y. Outcome of extracorporeal membrane oxygenation use in severe accidental hypothermia with cardiac arrest and circulatory instability: A multicentre, prospective, observational study in Japan (ICE-CRASH study). Resuscitation. 2023 Jan:182():109663. doi: 10.1016/j.resuscitation.2022.12.001. Epub 2022 Dec 9 [PubMed PMID: 36509361]
Level 2 (mid-level) evidenceCools E, Swol J, Wanscher M, Brugger H, Pasquier M, McIntosh S, Musi M, Oshiro K, Gordon L, Walpoth B, Hoffman JRH, Follis F, Zafren K, Paal P, Giraud R, Podsiadlo P, Martucci G, Darocha T. ELSO 2025 Narrative Guideline on the Use of ECMO for Accidental Hypothermia. ASAIO journal (American Society for Artificial Internal Organs : 1992). 2025 Nov 1:71(11):865-874. doi: 10.1097/MAT.0000000000002557. Epub 2025 Oct 22 [PubMed PMID: 41128452]
Pirnes J, Nyländen J, Karjalainen TM, Sälkiö S, Ohtonen P, Hoikka M, Ala-Kokko T. Factors related to 30-day survival rate following accidental hypothermia - a retrospective single-center study from Northern Finland. Scandinavian journal of trauma, resuscitation and emergency medicine. 2025 Nov 7:33(1):179. doi: 10.1186/s13049-025-01491-3. Epub 2025 Nov 7 [PubMed PMID: 41204240]
Level 2 (mid-level) evidenceKakizaki R, Bunya N, Uemura S, Odagiri A, Kasai T, Narimatsu E. Takotsubo cardiomyopathy developed during rewarming of accidental hypothermia with extracorporeal membrane oxygenation. Acute medicine & surgery. 2019 Apr:6(2):201-205. doi: 10.1002/ams2.399. Epub 2019 Mar 1 [PubMed PMID: 30976450]
Kirkegaard H, Grejs AM, Gudbjerg S, Duez C, Jeppesen A, Hassager C, Laitio T, Storm C, Taccone FS, Skrifvars MB, Søreide E. Electrolyte profiles with induced hypothermia: A sub study of a clinical trial evaluating the duration of hypothermia after cardiac arrest. Acta anaesthesiologica Scandinavica. 2022 May:66(5):615-624. doi: 10.1111/aas.14053. Epub 2022 Mar 28 [PubMed PMID: 35218019]
Polderman KH, Peerdeman SM, Girbes AR. Hypophosphatemia and hypomagnesemia induced by cooling in patients with severe head injury. Journal of neurosurgery. 2001 May:94(5):697-705 [PubMed PMID: 11354399]
Metz C, Holzschuh M, Bein T, Woertgen C, Frey A, Frey I, Taeger K, Brawanski A. Moderate hypothermia in patients with severe head injury: cerebral and extracerebral effects. Journal of neurosurgery. 1996 Oct:85(4):533-41 [PubMed PMID: 8814152]
Escolar JC, Hoo-Paris R, Castex C, Sutter BC. Effect of low temperatures on glucose-induced insulin secretion and glucose metabolism in isolated pancreatic islets of the rat. The Journal of endocrinology. 1990 Apr:125(1):45-51 [PubMed PMID: 2187049]
Level 3 (low-level) evidence