Introduction
Hydrofluoric acid was first identified in 1771 by the Swedish chemist Carl Wilhelm Scheele during investigations of the mineral fluorite (calcium fluoride). Today, hydrofluoric acid is widely used in industrial processes, including the production of aluminum, stainless steel, hydrofluorocarbons, and fluorinated pharmaceuticals, as well as in glass etching, petroleum refining, mineral processing, chemical manufacturing, and metal cleaning. Occupational exposure may occur in industries such as transportation, HVAC maintenance, fire extinguisher manufacturing, and steel production. Hydrofluoric acid is also found in numerous consumer products, including rust removers, masonry and stone cleaners, toilet bowl cleaners, insecticides, automobile wheel cleaners, and air conditioner cleaning solutions.[1][2][3][4]
Hydrofluoric acid is primarily produced by treating fluorite with concentrated sulfuric acid at elevated temperatures, yielding hydrofluoric acid and calcium sulfate. Natural sources also exist, including volcanic emissions. Global production exceeds one million tons annually, and hydrofluoric acid is commonly transported and stored as a highly concentrated liquid under pressure.[5] In the United States, the Department of Transportation and the National Fire Protection Association (NFPA) classify hydrofluoric acid as a severe health hazard because of its potential to cause significant morbidity and mortality. Consumer products typically contain dilute concentrations, often around 0.5%, whereas industrial formulations may approach 100%.
In its anhydrous form, hydrofluoric acid exists as a diatomic gas composed of hydrogen and fluorine. In the liquid state, strong hydrogen bonding between molecules results in the formation of polymeric chains.[6] Both anhydrous and aqueous solutions are typically colorless but may appear slightly tinted depending on concentration and impurities. Hydrofluoric acid has a boiling point of approximately 20 °C (68 °F) at standard atmospheric pressure, a vapor density greater than that of air, and readily dissolves in water. Dilute solutions may appear indistinguishable from water. The compound has a pungent, irritating odor detectable at concentrations well below the Occupational Safety and Health Administration (OSHA) permissible exposure limit of 3 ppm. Hydrofluoric acid readily reacts with and dissolves many materials, particularly metal oxides.[4]
Due to its ability to penetrate deeply into tissues and cause both local and systemic toxicity, exposure to hydrofluoric acid remains an important occupational and environmental health concern.[4][7] Unintentional exposures may occur in occupational and nonoccupational settings due to equipment failure, transportation accidents, container ruptures, inadequate personal protective equipment, or accidental ingestion of household products containing hydrofluoric acid. Intentional ingestions associated with suicidal or homicidal intent have also been reported.[4][8][9][10][11]
Hydrofluoric acid causes toxicity through a unique dual mechanism. Hydrogen ions produce corrosive local tissue injury, while fluoride ions penetrate deeply into tissues, causing liquefactive necrosis and cellular destruction. Fluoride ions avidly bind calcium and magnesium, resulting in potentially severe electrolyte disturbances, particularly hypocalcemia. The primary manifestations of exposure include dermal burns, ocular injury, acute respiratory symptoms, pulmonary injury, gastrointestinal toxicity, severe electrolyte abnormalities, and cardiac complications. Systemic fluoride toxicity may affect the cardiovascular, pulmonary, renal, and neuromuscular systems and can lead to life-threatening dysrhythmias, cardiovascular collapse, and death.[3][9][12] In some cases, chronic symptoms may persist for months following significant ingestion or inhalational exposure.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Hydrofluoric acid toxicity results from dermal, ocular, inhalational, or gastrointestinal exposure to hydrofluoric acid-containing products. Although hydrofluoric acid is chemically classified as a weak acid compared with other hydrogen halides, it is highly toxic because fluoride ions readily penetrate tissues and are rapidly absorbed. Once absorbed, fluoride ions bind calcium and magnesium, resulting in local tissue destruction and potentially life-threatening systemic toxicity, including severe electrolyte abnormalities and cardiac dysrhythmias (see Image: Mechanism of Hydrofluoric Acid Burn Injury). The severity of injury depends on the concentration, duration, route, and extent of exposure. Dilute solutions may produce delayed symptoms because fluoride ions can penetrate deeply into tissues before causing significant pain or visible injury. In contrast, concentrated solutions typically cause immediate pain and tissue damage. Dermal exposure is the most common route of injury, with occupational burns to the fingers and hands occurring frequently.[13]
Epidemiology
Hydrofluoric acid exposure is relatively uncommon compared with other occupational and industrial injuries, although the true global incidence is unknown. Approximately 1,000 cases are estimated to occur annually worldwide. In one 15-year study, hydrofluoric acid exposure accounts for 35 (17%) of 204 cases of chemical burns.[2] A separate 10-year study from China reports 690 patients with chemical burns, with hydrofluoric acid and sulfuric acid responsible for more than half of all injuries.[14] Most chemical burns occur during the summer and autumn months. A 20-year survey from Taiwan identified 324 cases of hydrofluoric acid exposure, with dermal contact being the most common route.[1] The majority of affected patients are adult males, and the upper extremities, particularly the hands and fingers, are the most frequently involved anatomical sites.[2][15]
Pathophysiology
Hydrofluoric acid exposure occurs through 3 primary routes: cutaneous contact, inhalation, and ingestion. Cutaneous exposure involving the skin or mucous membranes is the most common route and is typically associated with occupational accidents involving aqueous hydrofluoric acid solutions. Gastrointestinal exposure may occur unintentionally through accidental ingestion or intentionally in cases of self-harm. Inhalational exposure results from hydrogen fluoride gas or vapors released from hydrofluoric acid-containing solutions.[4][16] Unlike most mineral acids, hydrofluoric acid readily penetrates tissues and can cause extensive local injury and systemic toxicity. Tissue damage occurs through 3 primary mechanisms:
- Corrosive injury: At higher concentrations, hydrofluoric acid produces immediate corrosive damage to the skin, eyes, respiratory tract, and gastrointestinal mucosa. This injury may result in ulceration, necrosis, and severe pain.
- Deep tissue penetration: At lower concentrations, symptoms may be delayed because undissociated hydrofluoric acid penetrates deeply into tissues before dissociating. Once released, fluoride ions continue to diffuse through soft tissues, causing progressive cellular injury, liquefactive necrosis, and destruction of nerves, blood vessels, and underlying structures.[4][12]
- Systemic fluoride toxicity: Fluoride ions are rapidly absorbed and avidly bind to calcium and magnesium, forming insoluble salts that produce hypocalcemia and hypomagnesemia. Cellular injury and electrolyte disturbances may also contribute to hyperkalemia. These abnormalities can result in life-threatening cardiac dysrhythmias, including QT interval prolongation, polymorphic ventricular tachycardia, ventricular fibrillation, and conduction abnormalities. Severe systemic toxicity may lead to cardiovascular collapse and death.[4][12]
The severity of injury depends on the concentration of hydrofluoric acid, the duration of exposure, the total body surface area involved, and the route of exposure.
History and Physical
The clinical presentation of hydrofluoric acid toxicity varies with the route of exposure, acid concentration, duration of contact, and extent of tissue involvement. Patients often report severe pain that is disproportionate to visible tissue injury, a hallmark feature of hydrofluoric acid exposure. Symptoms may occur immediately following exposure to concentrated solutions, whereas lower-concentration solutions may produce delayed manifestations. Dermal exposure to solutions greater than 14.5% typically causes immediate pain and tissue injury, while symptoms may be delayed for up to 1 hour with 12% solutions and several hours with concentrations below 7%. A history of occupational or household exposure to products containing hydrofluoric acid, such as rust removers, wheel cleaners, masonry cleaners, or industrial chemicals, is common.
Information on the solution concentration, exposure duration, and use of personal protective equipment may help characterize the severity of exposure.Patients with systemic fluoride toxicity may develop perioral numbness, paresthesias, muscle cramps, weakness, tetany, and altered mental status. Physical findings associated with hypocalcemia include the Chvostek and Trousseau signs, carpopedal spasm, and generalized tetany. Severe toxicity may result in seizures, paralysis, cardiovascular collapse, or cardiac arrest.
Cardiovascular manifestations are primarily related to fluoride-induced electrolyte disturbances, including hypocalcemia, hypomagnesemia, and hyperkalemia. Patients may present with palpitations, syncope, hemodynamic instability, or cardiac arrest. Electrocardiographic abnormalities may include QT interval prolongation, peaked T waves, QRS widening, ventricular tachycardia, torsades de pointes, ventricular fibrillation, and other life-threatening dysrhythmias.
Dermal Exposure
Dermal exposure is the most common route of hydrofluoric acid injury. Patients typically present with intense pain, erythema, blistering, ulceration, or necrosis. The hands and fingers are most frequently affected, followed by the upper extremities, head and neck, and lower extremities. Tissue injury may initially appear mild despite extensive underlying damage. Exposure to highly concentrated solutions can result in rapid tissue penetration, progressive liquefactive necrosis, and severe pain.[4][16][17][18][19]
Ocular Exposure
Patients with ocular exposure typically present with immediate eye pain, tearing, photophobia, conjunctival injection, and blepharospasm. Physical findings may include conjunctival edema, corneal epithelial defects, corneal ulceration, stromal opacification, and decreased visual acuity.[4][5] Severe or prolonged exposures may result in corneal scarring, globe destruction, and permanent vision loss.
Inhalational Exposure
Inhalation of hydrogen fluoride gas or HF-containing vapors may cause nasal irritation, throat irritation, cough, dyspnea, chest tightness, wheezing, or respiratory distress. Findings may include mucosal inflammation, epistaxis, laryngitis, bronchospasm, tracheobronchitis, pulmonary edema, pneumonitis, or acute respiratory failure. Chronic or repeated inhalational exposure may result in persistent respiratory symptoms and chronic dyspnea.[4][16]
Ingestion Exposure
Hydrofluoric acid ingestion produces corrosive injury to the oropharynx, esophagus, and gastrointestinal tract. Patients commonly report oral pain, odynophagia, dysphagia, nausea, vomiting, diarrhea, and severe abdominal pain. Findings may include oral and pharyngeal burns, hematemesis, melena, hemorrhagic gastritis, and gastrointestinal perforation. Ingestion carries the greatest risk of severe systemic fluoride toxicity and death.[4][16]
Neurologic and Neuromuscular Manifestations
Individuals exposed through all routes can develop neurologic and muscular disorders. Neurologic and neuromuscular symptoms are primarily related to fluoride-induced electrolyte abnormalities. Patients may experience anxiety, confusion, headaches, paresthesia, seizures or paralysis, carpopedal and generalized tetany, and coma secondary to cerebral edema.[4][16]
Evaluation
The evaluation of hydrofluoric acid toxicity should begin with an assessment of the route of exposure, acid concentration, duration of contact, extent of tissue involvement, and evidence of systemic toxicity. Initial evaluation should focus on identifying life-threatening complications, including airway compromise, respiratory distress, severe electrolyte abnormalities, and cardiac dysrhythmias.
Physical examination findings vary according to the route of exposure. Dermal injuries should be assessed for location, total body surface area involved, pain severity, erythema, blistering, ulceration, necrosis, and involvement of deeper structures such as tendons, joints, or bone. Ocular exposures require evaluation of visual acuity, conjunctival injury, corneal involvement, and the extent of ocular surface damage. Patients with inhalational exposure should be assessed for upper- and lower-airway injury, including stridor, wheezing, bronchospasm, hypoxemia, and signs of pulmonary edema. Following ingestion, examination should evaluate for oropharyngeal burns, abdominal tenderness, gastrointestinal bleeding, and evidence of perforation. All patients should be assessed for manifestations of systemic fluoride toxicity, including paresthesias, muscle cramps, tetany, altered mental status, seizures, hemodynamic instability, and signs of hypocalcemia such as Chvostek and Trousseau signs.
Electrolyte abnormalities are among the hallmark findings of systemic hydrofluoric acid toxicity and may occur following exposure through any route. Initial laboratory evaluation should include serum calcium, magnesium, potassium, and bicarbonate, as well as renal function tests. Hypocalcemia, hypomagnesemia, and hyperkalemia are the most clinically significant abnormalities and may develop even after isolated dermal exposure. Patients with significant exposures may require serial laboratory monitoring, with severe cases warranting hourly assessment until electrolyte abnormalities stabilize.
Electrocardiography and continuous cardiac monitoring are essential in patients with moderate to severe exposures or evidence of systemic toxicity. ECG abnormalities may include QT interval prolongation secondary to hypocalcemia, peaked T waves, and QRS widening associated with hyperkalemia, and ventricular dysrhythmias resulting from combined electrolyte disturbances. Severe toxicity may manifest as torsades de pointes, ventricular fibrillation, wide-complex tachycardia, or cardiovascular collapse (see Image: ECG Prolonged QTc).
Additional diagnostic testing should be guided by the route of exposure and clinical findings. Patients with inhalational exposure should undergo chest radiography to evaluate for pulmonary edema, chemical pneumonitis, or other pulmonary complications. End-tidal carbon dioxide monitoring may be useful in patients with significant respiratory involvement. Patients with ocular exposure require ophthalmologic evaluation to assess the extent of corneal injury and visual impairment. Renal function studies and urinalysis should be considered in patients with significant exposures, as hematuria, proteinuria, or worsening renal function may indicate renal injury or, rarely, renal cortical necrosis.
Treatment / Management
Management of hydrofluoric acid toxicity begins with rapid assessment and stabilization of life-threatening conditions, including airway compromise, respiratory failure, severe electrolyte abnormalities, and cardiac dysrhythmias.[4] Contaminated clothing, jewelry, and other items that can retain hydrofluoric acid should be removed immediately and placed in appropriate containers to prevent secondary exposure among healthcare personnel and caregivers.
Prompt decontamination is essential and should not be delayed. Exposed areas should be irrigated copiously with water, saline, or soap and water to dilute and remove residual acid from the skin and mucous membranes. Using a soft brush and moving downward (from head to toe) may aid decontamination efforts. Although irrigation reduces the concentration of hydrofluoric acid through mechanical dilution and removal, it does not bind fluoride ions that have already penetrated tissues. Consequently, additional therapy to neutralize fluoride ions is often required.
Calcium gluconate is the cornerstone of treatment for hydrofluoric acid toxicity.[4] Calcium ions bind free fluoride ions to form insoluble calcium fluoride, thereby limiting ongoing tissue destruction and systemic fluoride absorption. Calcium gluconate may be administered repeatedly, depending on the severity of exposure and persistence of symptoms. Additional fluoride-binding agents used in selected circumstances include benzalkonium chloride, magnesium-containing compounds, and other topical neutralizing preparations.
Hexafluorine is an amphoteric, hypertonic solution specifically developed for decontamination following hydrofluoric acid exposure. In addition to providing mechanical irrigation, Hexafluorine can bind both hydrogen and fluoride ions, theoretically reducing the corrosive and cytotoxic effects of hydrofluoric acid. Although experimental studies suggest potential benefits, clinical evidence demonstrating superiority over prompt and thorough water irrigation remains limited.[4][20] Therefore, water irrigation should never be delayed while awaiting the availability of Hexafluorine or other specialized decontamination solutions.(B3)
Further treatment is guided by the route of exposure, extent of tissue injury, and presence of systemic toxicity.
Dermal Exposure
Dermal exposure is the most common form of hydrofluoric acid injury. Following removal of contaminated clothing and copious irrigation, calcium gluconate is the primary treatment for fluoride-ion neutralization. Topical 2.5% calcium gluconate gel should be applied liberally to the affected area and continuously massaged into the skin for 15 to 30 minutes. The gel may be reapplied every 10 to 15 minutes until pain improves. As calcium binds fluoride ions, the gel may develop a white discoloration due to the formation of calcium fluoride. For ongoing treatment, topical calcium gluconate may be applied 4 to 6 times daily for several days.[4]
Persistent pain despite topical therapy suggests ongoing fluoride penetration and may warrant subcutaneous calcium gluconate infiltration. A 5% calcium gluconate solution may be injected at a dose of 0.5 mL/cm² of affected tissue, extending slightly beyond the visible margins of injury.[21] Relief of pain is a possible sign of treatment efficacy.[12][13][22] Injections into the digits should be used cautiously because of the risk of increased compartment pressure and vascular compromise; volumes are generally limited to 0.5 mL per phalanx, with repeat administration as needed.[23](B3)
Additional topical therapies include benzalkonium chloride (0.13%) soaks. Potential adverse effects include local irritation, allergic reactions, urticaria, pruritus, dyspnea, chest tightness, and angioedema.[12][13][22][24](B3)
Ocular Exposure
Hydrofluoric acid readily penetrates ocular tissues and may cause severe injury. Initial management consists of immediate irrigation with copious amounts of water or sterile isotonic saline for at least 15 to 30 minutes. Topical ophthalmic anesthetics may facilitate adequate irrigation. Additional therapy may include intermittent irrigation with 1% calcium gluconate solution administered through a Morgan lens. Hexafluorine irrigation has also been utilized in selected cases.[5] Because hydrofluoric acid can rapidly penetrate the cornea and damage deeper ocular structures, urgent ophthalmologic consultation is recommended.
Inhalational Exposure
Inhalation of hydrogen fluoride gas or vapors may result in upper airway irritation, chemical pneumonitis, noncardiogenic pulmonary edema, acute respiratory distress syndrome (ARDS), and respiratory failure. Supplemental oxygen should be administered as needed. Nebulized calcium gluconate (2.5% to 3%) may help neutralize fluoride ions within the respiratory tract and improve symptoms. Patients with pulmonary edema may require noninvasive positive-pressure ventilation, while severe respiratory compromise may necessitate endotracheal intubation and mechanical ventilation. Surgical airway management may be required in rare cases of severe upper airway obstruction.
Ingestion Exposure
Hydrofluoric acid ingestion is a medical emergency because of the risk of severe corrosive injury and rapid systemic fluoride absorption. Management includes aggressive supportive care, correction of electrolyte abnormalities, continuous cardiac monitoring, and consultation with a poison center or medical toxicologist. Endoscopic evaluation may be indicated following stabilization to assess the extent of gastrointestinal injury. Patients are at high risk for severe hypocalcemia, hypomagnesemia, hyperkalemia, ventricular dysrhythmias, and cardiovascular collapse.
Management of Systemic Fluoride Toxicity
Patients with significant exposures require close monitoring for systemic toxicity. Individuals with burns involving more than 5% TBSA (or >1% TBSA if hydrofluoric acid concentration is higher than 50%), significant inhalational exposure, ingestion, or evidence of electrolyte abnormalities should be admitted for continuous cardiac monitoring and serial laboratory evaluation. Severe exposures often warrant intensive care unit admission for 24 to 48 hours or longer.
Intravenous calcium gluconate or calcium chloride is the primary therapy for hypocalcemia and ongoing fluoride binding. Associated electrolyte abnormalities should be corrected aggressively. Hyperkalemia may require treatment with intravenous insulin and dextrose (5 to 10 units IV with 250 ml of 10% dextrose), sodium bicarbonate (0.5 to 1 meq/kg), nebulized high-dose albuterol (10 to 20 mg nebulized), or emergent hemodialysis in refractory cases. The use of antiarrhythmic medication such as amiodarone, lidocaine, and procainamide is relatively contraindicated as they are largely ineffective and can worsen cardiac instability. Severe systemic fluoride toxicity with persistent electrolyte abnormalities may also require hemodialysis to enhance fluoride removal. Cardiac dysrhythmias should be managed with aggressive correction of the underlying electrolyte disturbances. Continuous cardiac monitoring is essential. Patients who develop torsades de pointes should be treated according to Advanced Cardiovascular Life Support (ACLS) protocols, including intravenous magnesium (0.05 to 0.1 mL/kg) and overdrive pacing when clinically indicated.
Differential Diagnosis
The differential diagnoses for hydrofluoric acid toxicity include the following:
- Chemical burns
- Chlorine toxicity
- Fluoride toxicity
- Hyperkalemia from other etiologies, including rhabdomyolysis, crush injury, and renal failure
- Ocular burns and chemical injuries
- Other causes of hypocalcemia including ethylene glycol poisoning, pancreatitis, and tumor lysis syndrome
Prognosis
Large volume or concentrated hydrofluoric acid ingestions have a poor prognosis, particularly if not treated early, due to significant caustic effects and systemic fluorosis. Small, accidental, dermal exposures to dilute solutions may result in pain but are rarely life-threatening.
Complications
Complications of hydrofluoric acid exposure may vary by route of exposure. In addition to severe electrolyte disturbances, ingestion of hydrofluoric acid solutions may result in esophageal injury, including risk of perforation or strictures. Inhalational exposures may result in severe pulmonary injury and risk of long-term respiratory insufficiency.
Consultations
Consultation with a regional poison center or medical toxicologist is recommended for all significant hydrofluoric acid exposures. The route and severity of exposure should guide additional specialty consultation. They may include burn surgery for extensive dermal injuries, ophthalmology for ocular exposures, gastroenterology for significant ingestions, pulmonology or critical care for severe inhalational injuries, and nephrology when hemodialysis is required for refractory electrolyte abnormalities or severe systemic fluoride toxicity.
Deterrence and Patient Education
Hydrofluoric acid toxicity is a potentially life-threatening chemical exposure that can cause severe burns, deep tissue injury, electrolyte abnormalities, cardiac dysrhythmias, and systemic organ toxicity. Unlike many other acids, hydrofluoric acid readily penetrates tissues and may cause progressive injury even when the initial skin findings appear mild. Prompt recognition and treatment are critical to reducing morbidity and mortality.
Prevention of hydrofluoric acid exposure is paramount. Individuals who work with hydrofluoric acid should receive comprehensive education regarding its toxic properties, safe handling practices, appropriate storage and transportation procedures, waste disposal requirements, decontamination methods, and emergency medical management following exposure. Hydrofluoric acid should be used only in industrial facilities and laboratories that are appropriately equipped to handle the chemical and maintain exposure-control programs, including immediate access to decontamination supplies and antidotal therapies before transport to a healthcare facility. Household products containing hydrofluoric acid should be stored securely and kept out of children's reach.
Strict adherence to personal and environmental safety measures is essential whenever hydrofluoric acid is handled. Recommended personal protective equipment includes a laboratory coat, long pants, an acid-resistant apron, closed-toed shoes, a full-face shield used in conjunction with tightly fitting chemical safety goggles, chemical-resistant gloves made of nitrile, butyl rubber, or neoprene, and appropriate respiratory protection when airborne exposure is possible. Work areas should be equipped with engineering controls such as chemical fume hoods, adequate ventilation and exhaust systems, clearly visible hazard signage, readily accessible running water, emergency safety showers, eyewash stations, and written standard operating procedures.
Hydrofluoric acid should be stored only in compatible containers, such as polyethylene or Teflon containers, that are clearly labeled, tightly sealed, secured against tipping, and protected from heat sources and direct sunlight. Facilities that utilize hydrofluoric acid should maintain readily available first-aid supplies, including 2.5% calcium gluconate gel, 1% calcium gluconate ophthalmic irrigation solution, or 0.13% benzalkonium chloride (Zephiran chloride), to facilitate immediate treatment following accidental exposure while awaiting definitive medical care.
Pearls and Other Issues
Dermal hydrofluoric acid exposures may present with pain out of proportion to the physical examination, where skin appears normal, but deeper injury is occurring. Topical and intravenous calcium and magnesium salts may be urgently required to reduce injury and prevent complications of systemic toxicity.
Enhancing Healthcare Team Outcomes
Hydrofluoric acid toxicity is a potentially life-threatening chemical exposure that can result in severe local tissue injury, electrolyte abnormalities, cardiac dysrhythmias, respiratory failure, and death. Because the clinical manifestations may initially appear mild despite significant underlying tissue penetration and systemic fluoride absorption, prompt recognition, early intervention, and coordinated multidisciplinary management are essential to optimizing patient outcomes. The management of hydrofluoric acid toxicity requires an interprofessional approach that emphasizes patient-centered care, effective communication, and coordinated treatment strategies.
Physicians and advanced practice clinicians are responsible for rapidly identifying the route and severity of exposure, initiating decontamination and antidotal therapy, assessing for systemic toxicity, and coordinating specialty consultations. Medical toxicologists and regional poison centers provide valuable expertise regarding exposure assessment, calcium-based therapies, electrolyte management, and the treatment of severe or unusual presentations.
Nurses play a critical role in performing decontamination procedures, administering medications, monitoring pain control, obtaining serial vital signs and laboratory studies, identifying clinical deterioration, and communicating changes in patient status to the healthcare team.
Pharmacists contribute by ensuring the timely availability and preparation of calcium gluconate formulations, reviewing medication regimens, assisting with the management of electrolyte abnormalities, and providing guidance regarding antidotal therapies and drug administration. Respiratory therapists may assist with oxygen therapy, nebulized calcium gluconate administration, airway management, and ventilatory support for patients with inhalational injuries.
Additional collaboration with burn, ophthalmology, gastroenterology, nephrology, and surgical specialists may be necessary depending on the route and severity of exposure. Burn specialists assist in managing extensive dermal injuries; ophthalmologists evaluate and treat ocular exposures; gastroenterologists may perform endoscopic evaluations following significant ingestions; and nephrologists may facilitate hemodialysis in patients with severe systemic fluoride toxicity or refractory electrolyte abnormalities.
Effective interprofessional communication is essential throughout the continuum of care. Clear communication regarding the concentration and route of exposure, timing of decontamination, laboratory results, electrocardiographic findings, and response to therapy helps ensure timely interventions and reduces the risk of complications. Standardized communication tools, accurate documentation, and coordinated transitions of care promote patient safety and improve team performance.
A collaborative, evidence-based approach enables healthcare professionals to rapidly identify hydrofluoric acid toxicity, initiate appropriate treatment, monitor for systemic complications, and provide ongoing supportive care. Through effective teamwork, communication, and care coordination, the interprofessional healthcare team can improve clinical outcomes, reduce morbidity and mortality, enhance patient safety, and deliver high-quality patient-centered care.
Media
(Click Image to Enlarge)
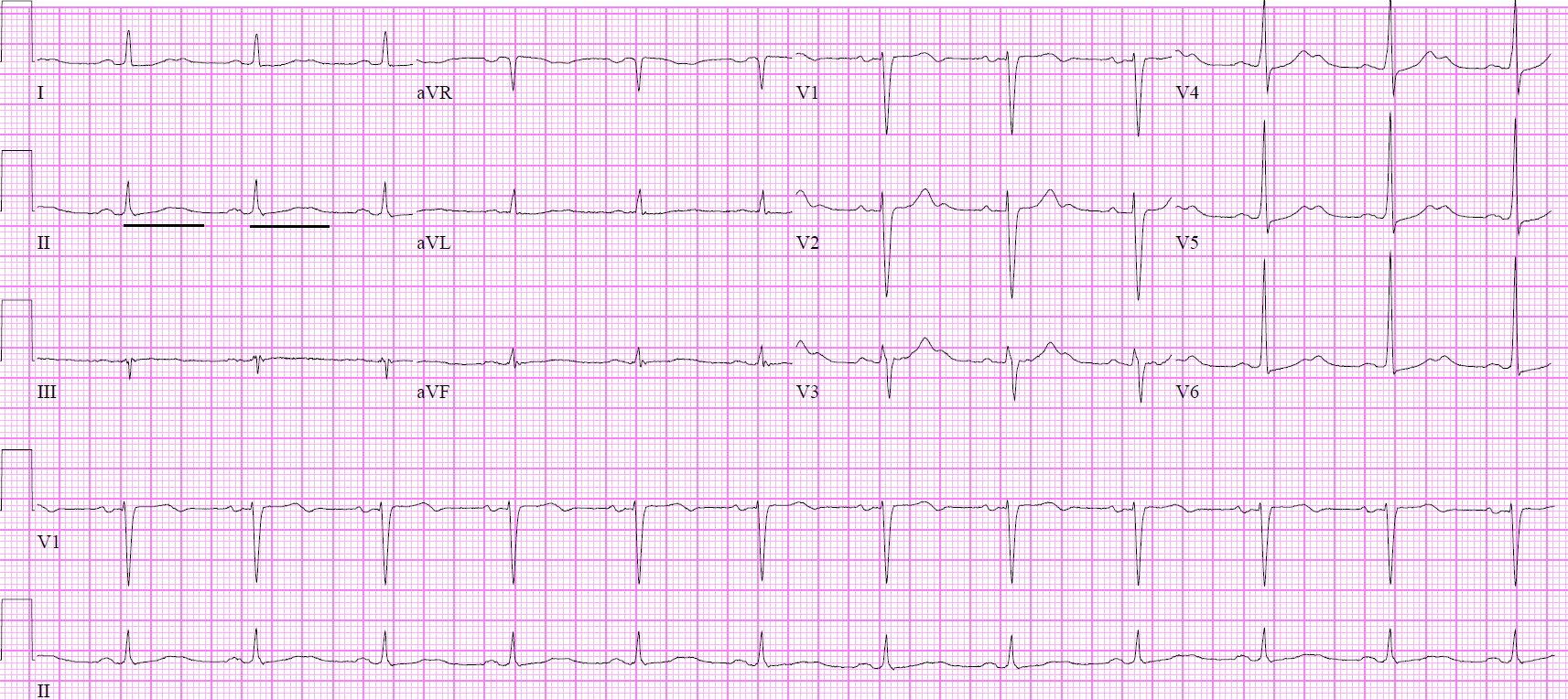
ECG Prolonged QTc.
Contributed by DL Schwerin, MD, FACEP, FAEMS, FAAEM
(Click Image to Enlarge)
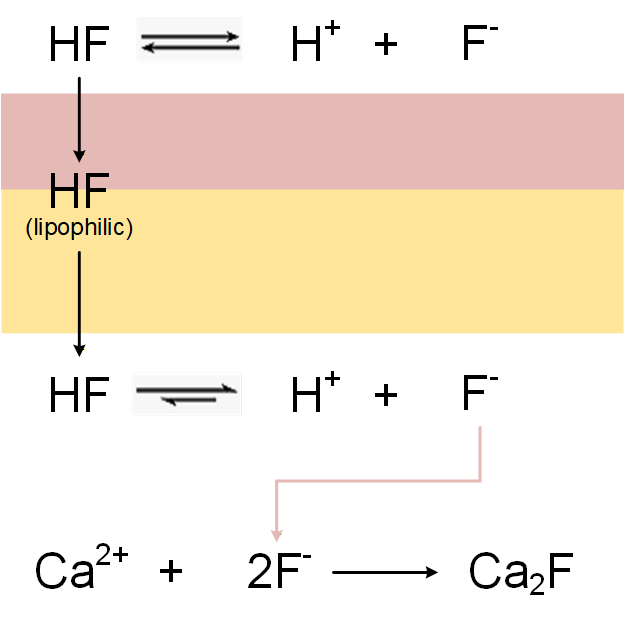
Mechanism of Hydrofluoric Acid Burn Injury. The image depicts dermal penetration and fluoride ion dissociation, with the fluoride ion binding to calcium to form a calcium fluoride salt.
Contributed by DL Schwerin, MD, FACEP, FAEMS, FAAEM
References
Wu ML, Yang CC, Ger J, Tsai WJ, Deng JF. Acute hydrofluoric acid exposure reported to Taiwan Poison Control Center, 1991-2010. Human & experimental toxicology. 2014 May:33(5):449-54. doi: 10.1177/0960327113499165. Epub 2013 Jul 25 [PubMed PMID: 23892993]
Level 2 (mid-level) evidenceStuke LE, Arnoldo BD, Hunt JL, Purdue GF. Hydrofluoric acid burns: a 15-year experience. Journal of burn care & research : official publication of the American Burn Association. 2008 Nov-Dec:29(6):893-6. doi: 10.1097/BCR.0b013e31818b9de6. Epub [PubMed PMID: 18849854]
Level 2 (mid-level) evidenceKim Y, Shin J, Kang S, Kyung S, Park JW, Lee S, Lee S, Jeong SH. Pulmonary alveolar proteinosis induced by hydrofluoric acid exposure during fire extinguisher testing. Journal of occupational medicine and toxicology (London, England). 2015:10():6. doi: 10.1186/s12995-015-0048-7. Epub 2015 Feb 25 [PubMed PMID: 25737738]
Level 3 (low-level) evidenceBajraktarova-Valjakova E, Korunoska-Stevkovska V, Georgieva S, Ivanovski K, Bajraktarova-Misevska C, Mijoska A, Grozdanov A. Hydrofluoric Acid: Burns and Systemic Toxicity, Protective Measures, Immediate and Hospital Medical Treatment. Open access Macedonian journal of medical sciences. 2018 Nov 25:6(11):2257-2269. doi: 10.3889/oamjms.2018.429. Epub 2018 Nov 20 [PubMed PMID: 30559898]
Atley K, Ridyard E. Treatment of hydrofluoric acid exposure to the eye. International journal of ophthalmology. 2015:8(1):157-61. doi: 10.3980/j.issn.2222-3959.2015.01.28. Epub 2015 Feb 18 [PubMed PMID: 25709926]
Smędra-Kaźmirska A, Kędzierski M, Barzdo M, Jurczyk A, Szram S, Berent J. Accidental intoxication with hydrochloric acid and hydrofluoric acid mixture. Archiwum medycyny sadowej i kryminologii. 2014 Jan-Mar:64(1):50-8 [PubMed PMID: 25184427]
Franzblau A, Sahakian N. Asthma following household exposure to hydrofluoric acid. American journal of industrial medicine. 2003 Sep:44(3):321-4 [PubMed PMID: 12929153]
Level 3 (low-level) evidenceOzsoy G, Kendirli T, Ates U, Perk O, Azapagasi E, Ozcan S, Baran C, Goktug A, Dindar H. Fatal Refractory Ventricular Fibrillation Due to Ingestion of Hydrofluoric Acid. Pediatric emergency care. 2019 Nov:35(11):e201-e202. doi: 10.1097/PEC.0000000000001548. Epub [PubMed PMID: 30020244]
Gradinger R, Jung C, Reinhardt D, Mall G, Figulla HR. Toxic myocarditis due to oral ingestion of hydrofluoric acid. Heart, lung & circulation. 2008 Jun:17(3):248-50 [PubMed PMID: 17822953]
Level 3 (low-level) evidenceVohra R, Velez LI, Rivera W, Benitez FL, Delaney KA. Recurrent life-threatening ventricular dysrhythmias associated with acute hydrofluoric acid ingestion: observations in one case and implications for mechanism of toxicity. Clinical toxicology (Philadelphia, Pa.). 2008 Jan:46(1):79-84 [PubMed PMID: 17906993]
Level 3 (low-level) evidenceWhiteley PM, Aks SE. Case files of the Toxikon Consortium in Chicago: survival after intentional ingestion of hydrofluoric acid. Journal of medical toxicology : official journal of the American College of Medical Toxicology. 2010 Sep:6(3):349-54. doi: 10.1007/s13181-010-0088-4. Epub [PubMed PMID: 20661686]
Level 3 (low-level) evidenceMcKee D, Thoma A, Bailey K, Fish J. A review of hydrofluoric acid burn management. Plastic surgery (Oakville, Ont.). 2014 Summer:22(2):95-8 [PubMed PMID: 25114621]
Alper N, Desai K, Rabinowitz S. Management of hydrofluoric Acid burns. Eplasty. 2014:14():ic42 [PubMed PMID: 25525489]
Level 3 (low-level) evidenceYe C, Wang X, Zhang Y, Ni L, Jiang R, Liu L, Han C. Ten-year epidemiology of chemical burns in western Zhejiang Province, China. Burns : journal of the International Society for Burn Injuries. 2016 May:42(3):668-74. doi: 10.1016/j.burns.2015.12.004. Epub 2016 Jan 20 [PubMed PMID: 26803372]
Meaney C, Perdue M, Umar M, Walker J. Hydrofluoric Acid, an Unexpected Surprise. Military medicine. 2023 Jul 22:188(7-8):e2793-e2796. doi: 10.1093/milmed/usac179. Epub [PubMed PMID: 35748498]
Wang X, Zhang Y, Ni L, You C, Ye C, Jiang R, Liu L, Liu J, Han C. A review of treatment strategies for hydrofluoric acid burns: current status and future prospects. Burns : journal of the International Society for Burn Injuries. 2014 Dec:40(8):1447-57. doi: 10.1016/j.burns.2014.04.009. Epub 2014 Jun 16 [PubMed PMID: 24946967]
Zhang Y, Zhang J, Jiang X, Ni L, Ye C, Han C, Sharma K, Wang X. Hydrofluoric acid burns in the western Zhejiang Province of China: a 10-year epidemiological study. Journal of occupational medicine and toxicology (London, England). 2016:11():55 [PubMed PMID: 27980604]
Level 2 (mid-level) evidencePu Q, Qian J, Tao W, Yang A, Wu J, Wang Y. Extracorporeal membrane oxygenation combined with continuous renal replacement therapy in cutaneous burn and inhalation injury caused by hydrofluoric acid and nitric acid. Medicine. 2017 Dec:96(48):e8972. doi: 10.1097/MD.0000000000008972. Epub [PubMed PMID: 29310404]
Level 2 (mid-level) evidenceDennerlein K, Kiesewetter F, Kilo S, Jäger T, Göen T, Korinth G, Drexler H. Dermal absorption and skin damage following hydrofluoric acid exposure in an ex vivo human skin model. Toxicology letters. 2016 Apr 25:248():25-33. doi: 10.1016/j.toxlet.2016.02.015. Epub 2016 Feb 27 [PubMed PMID: 26930472]
Level 3 (low-level) evidenceHultén P, Höjer J, Ludwigs U, Janson A. Hexafluorine vs. standard decontamination to reduce systemic toxicity after dermal exposure to hydrofluoric acid. Journal of toxicology. Clinical toxicology. 2004:42(4):355-61 [PubMed PMID: 15461243]
Level 3 (low-level) evidenceDibbell DG, Iverson RE, Jones W, Laub DR, Madison MS. Hydrofluoric acid burns of the hand. The Journal of bone and joint surgery. American volume. 1970 Jul:52(5):931-6 [PubMed PMID: 5479482]
Robinson EP, Chhabra AB. Hand chemical burns. The Journal of hand surgery. 2015 Mar:40(3):605-12; quiz 613. doi: 10.1016/j.jhsa.2014.07.056. Epub 2015 Feb 1 [PubMed PMID: 25653184]
Edelman P. Hydrofluoric acid burns. Occupational medicine (Philadelphia, Pa.). 1986 Jan-Mar:1(1):89-103 [PubMed PMID: 3299779]
Ohtani M, Nishida N, Chiba T, Muto H, Yoshioka N. Pathological demonstration of rapid involvement into the subcutaneous tissue in a case of fatal hydrofluoric acid burns. Forensic science international. 2007 Mar 22:167(1):49-52 [PubMed PMID: 16426786]
Level 3 (low-level) evidence