Indications
FDA-Approved Indications
Hydrochlorothiazide is a medication approved by the US Food and Drug Administration (FDA) to treat hypertension and peripheral edema associated with congestive heart failure and cirrhosis. Hydrochlorothiazide is a thiazide-type diuretic that inhibits sodium resorption in the distal convoluted tubules (DCTs) of the kidney. For more than 60 years, thiazide diuretics have been a well-established class of antihypertensive diuretics that reduce sodium reabsorption and promote natriuresis and diuresis through direct inhibition of the sodium–chloride cotransporter.[1]
Hydrochlorothiazide is FDA-approved for the treatment of essential hypertension, either as a primary agent or an adjunct to other antihypertensive therapies.[2] Hydrochlorothiazide was initially approved for the treatment of hypertension in the 1960s.[3] According to some studies, thiazide-type diuretics and calcium channel blockers may be more effective at lowering blood pressure in Black patients than the renin-angiotensin system (RAS) inhibitors or beta-blockers.[4]
Hydrochlorothiazide is also FDA-approved for the treatment of peripheral edema related to heart failure, corticosteroids, nephrotic syndromes, or estrogen therapy. Loop diuretics are usually the first-line treatment for peripheral edema, and hydrochlorothiazide is utilized as an adjunctive therapy.[5] According to the 2025 American Heart Association and American College of Cardiology guidelines, hydrochlorothiazide is recommended as a first-line pharmacologic option for the management of hypertension.[6]
Single-pill (fixed-dose) combinations containing hydrochlorothiazide can improve blood pressure control and may reduce cardiovascular risk. The FDA has approved several single-pill combinations that include angiotensin II receptor blockers such as valsartan/hydrochlorothiazide, losartan/hydrochlorothiazide, and irbesartan/hydrochlorothiazide.[7] The FDA has also approved the angiotensin-converting enzyme (ACE) inhibitor combination lisinopril/hydrochlorothiazide. Additional approved single-pill combinations include hydrochlorothiazide+bisoprolol, hydrochlorothiazide+aliskiren (a direct renin inhibitor), and hydrochlorothiazide+triamterene (a potassium-sparing diuretic).[8]
Off-Label Uses
Hydrochlorothiazide can also be used to manage nephrogenic diabetes insipidus and to prevent calcium nephrolithiasis; however, these are not FDA-approved indications.[9][10][11]
Mechanism of Action
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Mechanism of Action
Hydrochlorothiazide selectively inhibits the Na+/Cl− cotransporter (NCC), the primary pathway for sodium reabsorption on the apical membrane of epithelial cells in the DCT, thereby reducing sodium and chloride reabsorption.[12] The DCT normally reabsorbs approximately 5% to 10% of filtered sodium.[13] This inhibition decreases sodium and chloride reabsorption, thereby increasing sodium delivery to the distal nephron and collecting duct.
Reduced intracellular sodium concentration within the DCT cells enhances the activity of the basolateral sodium-calcium exchanger, promoting calcium efflux into the interstitium and facilitating increased calcium reabsorption from the tubular lumen via apical calcium channels. This mechanism contributes to enhanced distal tubular calcium reabsorption, accounting for approximately 7% to 10% of total filtered calcium handling in this segment.[14] The resulting reduction in urinary calcium excretion underlies the therapeutic utility of thiazides in conditions such as calcium nephrolithiasis (see Images. Mechanism of Action of Hydrochlorothiazide and Hydrochlorothiazide Mechanism of Action and Physiologic Effects).
Increased sodium delivery to the collecting duct augments sodium reabsorption through epithelial sodium channels in principal cells under the influence of aldosterone. Aldosterone binds to intracellular mineralocorticoid receptors, increasing transcription of epithelial sodium channels and Na+/K+-ATPase pumps, thereby enhancing sodium reabsorption and potassium secretion.[15][16] This compensatory mechanism contributes to potassium wasting and the risk of hypokalemia observed with thiazide therapy.
The initial antihypertensive effect results from natriuresis and reduction in extracellular fluid volume, leading to decreased cardiac output.[17] With chronic therapy, plasma volume partially normalizes, yet blood pressure is reduced through decreased peripheral vascular resistance.[18] The precise mechanism underlying this sustained vasodilatory effect remains incompletely defined but is thought to involve alterations in sodium balance, vascular smooth muscle responsiveness, and possibly direct effects on ion transport within vascular tissue. Chlorthalidone and indapamide are thiazide-type diuretics, structurally belonging to the sulfonamide class, that share the same NCC inhibition mechanism in the DCT, despite lacking the benzothiadiazine ring.[19]
Pharmacokinetics (Adapted from PubChem) https://pubchem.ncbi.nlm.nih.gov/compound/Hydrochlorothiazide
Absorption: Hydrochlorothiazide is absorbed from the gastrointestinal tract, with an oral bioavailability of approximately 65% to 75%. In adults, the pharmacological effects of hydrochlorothiazide commence within 2 hours, peak after 4 hours, and persist for about 6 to 12 hours.[20] Food reduces bioavailability by about 10% and peak plasma concentration by about 20%, and delays the time to peak from about 1.6 to 2.9 hours.
Distribution: Hydrochlorothiazide has a volume of distribution ranging from approximately 0.83 to 4.19 L/kg. Plasma protein binding is about 40% to 68%, primarily to albumin. Hydrochlorothiazide crosses the placenta and is detectable in cord blood and breast milk, but does not significantly cross the blood-brain barrier.[21]
Metabolism: Hydrochlorothiazide is not metabolized.
Excretion: Hydrochlorothiazide is primarily eliminated by the kidney as an unchanged drug, with about 61% excreted in urine within 24 hours. The plasma elimination half-life ranges from about 5.6 to 15 hours.
Administration
Available Dosage Forms and Strengths
Hydrochlorothiazide is available in tablet and capsule forms for oral administration in strengths of 12.5 mg, 25 mg, and 50 mg. The drug is also widely available in fixed-dose combination products with other antihypertensive agents, as mentioned in the previous section.
Adult Dosages
Dosing varies by indication, patient characteristics, and therapeutic response. Early administration is recommended to minimize nocturia.
Hypertension: The typical initial dosage of hydrochlorothiazide for the treatment of hypertension is 12.5 to 25 mg once daily. Dose titration may occur after 2 to 4 weeks based on blood pressure response, with a usual maximum of 50 mg daily. Dosages above 25 mg daily generally provide minimal additional antihypertensive benefit while increasing the risk of metabolic adverse effects.[2]
Peripheral edema: The typical initial dosage of hydrochlorothiazide for the treatment of peripheral edema is 25 to 50 mg once daily or in divided doses. In refractory cases, dosages up to 200 mg daily may be used; however, higher doses are associated with increased electrolyte disturbances and are less commonly used in contemporary practice.[22]
Nephrogenic diabetes insipidus: An initial dosage of hydrochlorothiazide for the treatment of nephrogenic diabetes insipidus is 25 mg twice daily, with subsequent titration based on clinical response.[23]
Calcium nephrolithiasis prevention: The usual starting dosage of hydrochlorothiazide is 25 mg once daily. Depending on urinary calcium excretion and tolerance, the dosage may be increased to 25 mg twice daily or 50 mg daily in equally divided doses.[24] Renal function should be assessed prior to initiation and periodically thereafter. Thiazide diuretics are less effective in advanced renal impairment.
Cardiovascular Outcomes
Untreated hypertension is associated with adverse cardiac remodeling, endothelial dysfunction, and increased risk of major adverse cardiovascular events. Selection of antihypertensive therapy should be individualized, taking into account comorbid conditions, baseline cardiovascular risk, and tolerability.
The 2025 hypertension guidelines provide a Class I, Level A recommendation for thiazide-type diuretics, calcium channel blockers, ACE inhibitors, or angiotensin receptor blockers as initial therapy in most adults with primary hypertension.[6] In patients with chronic kidney disease or specific cardiovascular comorbidities, RAS inhibition is often preferred as foundational therapy due to cardiorenal protective effects.
Thiazide-type diuretics are frequently used as part of combination therapy, including with RAS inhibitors, calcium channel blockers, beta-blockers, mineralocorticoid receptor antagonists, or additional diuretics when clinically indicated. The 2008 ACCOMPLISH trial demonstrated that combination therapy with benazepril-amlodipine was superior to benazepril–hydrochlorothiazide in reducing cardiovascular events among high-risk patients with hypertension.[25] These findings suggest that antihypertensive efficacy alone does not necessarily translate into equivalent reductions in cardiovascular outcomes across all combination regimens.
Most large randomized trials evaluating hydrochlorothiazide have examined it as monotherapy rather than as part of multiple drug regimens tailored to contemporary risk-based treatment strategies. Future research may better define the role of hydrochlorothiazide as a second- or third-line agent in specific patient populations, particularly those with coexisting cardiovascular or metabolic disease.
Specific Patient Populations
Hepatic impairment: Hydrochlorothiazide should be used with caution in patients with impaired hepatic function, as minor alterations of fluid and electrolyte balance can precipitate hepatic coma.
Renal impairment: Hydrochlorothiazide is primarily eliminated unchanged by the kidneys. Although specific dose adjustments are not universally recommended for mild to moderate renal impairment, thiazide diuretics are less effective in severe renal dysfunction, particularly when creatinine clearance falls below approximately 10 mL/min.[26][27][26]
Pregnancy considerations: According to the product labeling for hydrochlorothiazide, edema during pregnancy may arise from pathologic causes or from the physiologic and mechanical consequences of pregnancy. Thiazide diuretics are indicated in pregnancy when edema is due to pathologic causes. However, dependent edema during pregnancy, caused by the gravid uterus restricting venous return, can be effectively treated by elevating the lower extremities and using support stockings. The use of diuretics in this setting to reduce intravascular volume is illogical and unnecessary.
Preferred treatment according to the 2025 American Heart Association/American College of Cardiology Foundation guidelines and the American College of Obstetricians and Gynecologists is labetalol and nifedipine. Hydrochlorothiazide may be used as an alternative.[28][29]
Breastfeeding considerations: Thiazides are excreted into breast milk. Because of the risk of serious adverse effects in nursing infants, a decision should be made to either discontinue breastfeeding or stop the medication, considering the importance of the medication to the mother and a shared risk–benefit assessment. High doses that produce aggressive diuresis may also reduce breast milk production.[21]
Pediatric patients: Hydrochlorothiazide dosing for pediatric patients is highly individualized. No controlled clinical trials exist; dosing guidance relies on empirical pediatric use and literature on hypertension treatment in children. As per product labeling for diuresis in blood pressure control, the usual pediatric dosage is 1 to 2 mg/kg/d, which is administered as a single or divided dose. Hydrochlorothiazide doses should not exceed 37.5 mg/d in infants up to age 2 or 100 mg/d in children aged 2 to 12. In infants younger than 6 months, hydrochlorothiazide doses up to 3 mg/kg/d, divided into 2 equal doses, may be required.
Older patients: According to the 2023 American Geriatrics Society Beers Criteria 2023, diuretics may precipitate or exacerbate syndrome of inappropriate antidiuretic hormone secretion (SIADH) or hyponatremia; therefore, sodium levels should be monitored closely when initiating therapy or adjusting doses in older adults.[30]
Adverse Effects
Hydrochlorothiazide is generally well tolerated at low to moderate doses; however, adverse effects are dose-dependent and occur more frequently when daily doses exceed 25 mg.[31]
Electrolyte Derangements
Hypokalemia, hyponatremia, hypomagnesemia, hypercalcemia, and hyperchloremic alkalosis may result from hydrochlorothiazide blocking the sodium-chloride cotransporter in the DCTs, as described earlier.[5] Hyponatremia may be particularly pronounced in older adults, individuals with low solute intake, or those receiving concomitant diuretics.[5][31] Electrolyte abnormalities are more common with higher doses or combination diuretic therapy.
Hyperglycemia
Hydrochlorothiazide has been associated with mild elevations in fasting plasma glucose. Although the mechanism is not fully elucidated, hypokalemia may impair pancreatic β-cell insulin secretion, contributing to dysglycemia.[32] The effect is generally modest and appears to be dose-related, necessitating monitoring in patients with diabetes mellitus or impaired glucose tolerance.
Hyperuricemia and Gout
Hydrochlorothiazide can increase serum uric acid levels and precipitate gout flares, particularly in predisposed individuals. The mechanism involves volume contraction and enhanced proximal tubular urate reabsorption.[33] Hyperuricemia typically develops within the first weeks of therapy initiation and is dose-dependent.
Dyslipidemia
Thiazide therapy has been associated with modest, dose-related increases in total cholesterol and triglyceride levels. These changes are generally small and may attenuate with long-term therapy.[34]
Sulfa Allergy
Hydrochlorothiazide contains a sulfonamide moiety. Severe hypersensitivity reactions, including rash, urticaria, Stevens-Johnson syndrome, toxic epidermal necrolysis, and anaphylaxis, are rare but reported adverse effects.[35] Although cross-reactivity between sulfonamide antibiotics and nonantibiotic sulfonamides, such as hydrochlorothiazide, is considered low, caution is advised in patients with a history of severe sulfonamide reactions. The absolute contraindication is generally limited to patients with a prior serious hypersensitivity to hydrochlorothiazide itself.[36]
Ocular Disturbance
Rare cases of acute myopia and secondary angle-closure glaucoma have been reported, typically within days of therapy initiation. These events are thought to be related to idiosyncratic sulfonamide-associated choroidal effusion leading to anterior displacement of the lens–iris diaphragm. Immediate drug discontinuation is required if ocular symptoms develop.[37]
Special Considerations
In patients with advanced liver disease, hydrochlorothiazide may precipitate severe hyponatremia, hypokalemia, or hepatic encephalopathy due to fluid and electrolyte shifts. Careful monitoring is required in this population.[38]
Clinicians should also exercise caution during the perioperative period, as diuretic-induced volume depletion may increase the risk of intraoperative hypotension or postoperative acute kidney injury.
Drug-Drug Interactions
- Antidiabetic drugs: When hydrochlorothiazide is administered with antidiabetic drugs, including oral agents and insulin, dosage adjustment of the antidiabetic therapy may be required.
- Alcohol or narcotics: Concomitant use of alcohol, barbiturates, or narcotics with hydrochlorothiazide may potentiate orthostatic hypotension.
- Cholestyramine and colestipol resins: Cholestyramine or colestipol binds hydrochlorothiazide in the gastrointestinal tract, reducing its systemic absorption.
- Steroids or adrenocorticotropic hormone: Concomitant use of corticosteroids or adrenocorticotropic hormone with hydrochlorothiazide may lead to electrolyte depletion, increasing the risk of hypokalemia.
- Lithium: Lithium should not be given with diuretics, including hydrochlorothiazide. Diuretic therapy can reduce the renal clearance of lithium and markedly increase the risk of lithium toxicity.[39][40] Clinicians should consult the prescribing information for lithium preparations before using these agents concomitantly with hydrochlorothiazide.
- Nonsteroidal anti-inflammatory drugs: In some patients, concomitant use of nonsteroidal anti-inflammatory drugs (NSAIDs) with thiazide, loop, or potassium-sparing diuretics may reduce the diuretic, natriuretic, and antihypertensive effects of these diuretics. When hydrochlorothiazide and NSAIDs are used together, patients should be monitored closely to ensure that the desired diuretic and antihypertensive effects are achieved.[41]
Drug-Laboratory Interactions
Thiazide diuretics reduce urinary calcium excretion and may cause transient, mild increases in serum calcium levels, even in the absence of underlying disorders of calcium metabolism. Marked hypercalcemia may unmask underlying hyperparathyroidism; therefore, thiazides should be discontinued before evaluation of parathyroid function.[42]
Contraindications
Hydrochlorothiazide is contraindicated in patients with anuria and in those with a known hypersensitivity to hydrochlorothiazide or other components of the formulation.
Warnings and Precautions
- Severe hepatic impairment: Hydrochlorothiazide should be used cautiously in patients with severe hepatic impairment due to the potential risk of developing hepatic coma.[43]
- Adrenal insufficiency: In individuals with underlying adrenal insufficiency, hydrochlorothiazide therapy should be avoided.[44]
- Non-melanoma skin cancer: The FDA has stated that hydrochlorothiazide is linked with a small increased risk of non-melanoma skin cancer, particularly squamous cell carcinoma in White patients with high cumulative exposure. No clear association has been observed with basal cell carcinoma or melanoma.[45][46][47] The FDA notes that treatment for non-melanoma skin cancer is typically local, effective, and associated with very low mortality. In contrast, uncontrolled hypertension carries substantial risk, including life-threatening myocardial infarction and stroke. Given this risk–benefit profile, patients should continue hydrochlorothiazide and adopt sun protection and other skin care measures to reduce the risk of non-melanoma skin cancer, unless their healthcare professional advises otherwise.https://www.fda.gov/drugs/drug-safety-and-availability/fda-approves-label-changes-hydrochlorothiazide-describe-small-risk-non-melanoma-skin-cancer.
- Prescribing cascade: The use of hydrochlorothiazide for peripheral edema caused by calcium channel blockers, such as amlodipine, is often ineffective and represents a prescribing cascade in which a thiazide is mistakenly added to treat an adverse effect of calcium channel blocker–induced peripheral edema. Calcium channel blocker-induced edema results from precapillary vasodilation rather than volume overload, making diuretics largely ineffective in this setting.[48]
Monitoring
Patients receiving hydrochlorothiazide should undergo regular clinical and laboratory monitoring to ensure safety and optimize therapeutic outcomes. Monitoring should be individualized based on patient comorbidities, dose, and duration of therapy. Early detection of adverse effects allows prompt intervention and dose adjustment, optimizing both efficacy and safety.
- Electrolytes: Serum sodium, potassium, calcium, and magnesium levels should be monitored at baseline and periodically during therapy, particularly in patients receiving higher doses, combination diuretics, or those at risk for electrolyte disturbances.
- Volume status: Volume status should be assessed for signs of dehydration or volume overload, with therapy adjusted as clinically indicated.
- Blood pressure: Regular measurement is essential to confirm achievement and maintenance of target blood pressure and to minimize risks associated with hypotension or uncontrolled hypertension.
- Gout risk: Patients with a personal or family history of gout should be monitored for signs of acute gout flares, especially during the early weeks of therapy.[49]
- Glucose metabolism: Fasting blood glucose should be monitored in patients with diabetes mellitus or impaired glucose tolerance, as hydrochlorothiazide may induce mild hyperglycemia.
- Renal and hepatic function: Periodic assessment of kidney and liver function is recommended in patients with preexisting renal or hepatic disease, as diuretic response and electrolyte handling may be altered.[50]
Toxicity
Signs and Symptoms of Overdose
The most common signs and symptoms observed are hypovolemia and hypotension. Patients may have electrolyte depletion, hypokalemia, hypochloremia, hyponatremia, and excessive diuresis.[54] A rare case of non-cardiogenic pulmonary edema induced by hydrochlorothiazide has been described.[55]
Management of Overdose
In the event of hydrochlorothiazide overdose, symptomatic and supportive measures should be implemented. Airway patency, respiration, and circulation should be maintained. Dehydration, electrolyte disturbances, and hypotension should be corrected as clinically indicated. The extent of hydrochlorothiazide removal by hemodialysis has not been established.
Enhancing Healthcare Team Outcomes
Hydrochlorothiazide is commonly prescribed for hypertension and peripheral edema. Despite the long-standing use of thiazide diuretics, patients require careful monitoring for electrolyte disturbances, blood pressure changes, and other adverse effects. Achieving optimal outcomes requires a multidisciplinary, patient-centered approach, with coordinated oversight of fluid balance, vital signs, and laboratory parameters.
Effective management relies on collaboration among an interprofessional healthcare team, including clinicians, specialists, nurses, and pharmacists, with clear communication regarding monitoring, reassessment, and therapy adjustments. This coordinated approach facilitates early identification of adverse effects and supports individualized, evidence-based care.
Effective hydrochlorothiazide therapy requires a coordinated interprofessional healthcare team operating within the Team Strategies and Tools to Enhance Performance and Patient Safety (TeamSTEPPS) framework.[56] Physicians and advanced practice providers initiate and adjust therapy based on clinical indication, renal function, and comorbid conditions. In contrast, clinical pharmacists perform prospective prescription verification, screen for clinically significant drug-drug interactions (with agents such as lithium, NSAIDs, and digoxin), and provide structured patient counseling on adherence and adverse drug reaction recognition.
Registered nurses are the most proximate caregivers, and they monitor vital signs, fluid intake and output, and clinical signs of electrolyte disturbances, including hypokalaemia, hyponatremia, and hypomagnesemia, and escalate concerns to the prescribing clinician using the Situation, Background, Assessment, Recommendation (SBAR) structured communication tool. Verbal orders and medication changes, such as the addition of oral potassium (K+) supplementation or dose adjustment of hydrochlorothiazide, should be confirmed through the check-back technique, in which the receiver reads back the instruction and the sender explicitly verifies receipt, thereby closing the communication loop and minimizing medication error. Regular polypharmacy review is particularly critical in older adults, in whom cumulative diuretic burden compounds the risk of volume depletion and falls.
Hydrochlorothiazide is one of the 3 commonly used thiazide-type diuretics, along with chlorthalidone and chlorothiazide, all of which share a benzothiadiazine-based chemical structure.[57] While most historical trials have evaluated hydrochlorothiazide or chlorthalidone, few have directly compared these agents. One large multicenter study found no statistically significant difference in the incidence of major cardiovascular events between hydrochlorothiazide and chlorthalidone.[58]
Although hydrochlorothiazide is rarely used as monotherapy in contemporary practice, successful antihypertensive management requires individualized treatment plans informed by patient comorbidities, preferences, and shared decision-making. Interprofessional collaboration is key to optimizing both safety and long-term cardiovascular outcomes.
Media
(Click Image to Enlarge)
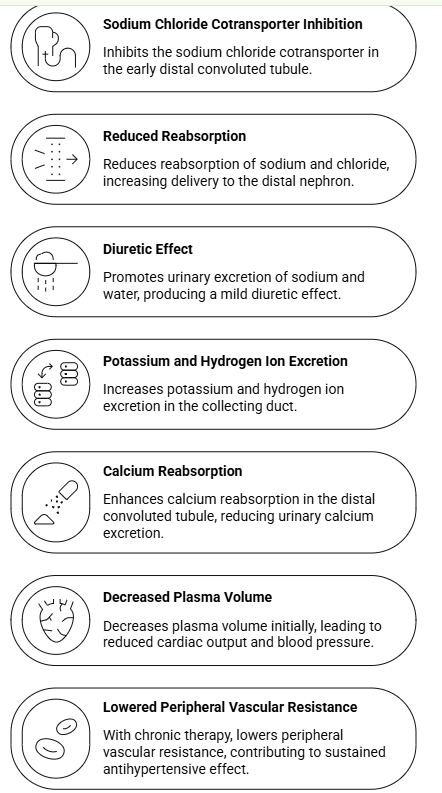
Hydrochlorothiazide Mechanism of Action and Physiologic Effects
Contributed by Preeti Patel, PharmD
(Click Image to Enlarge)
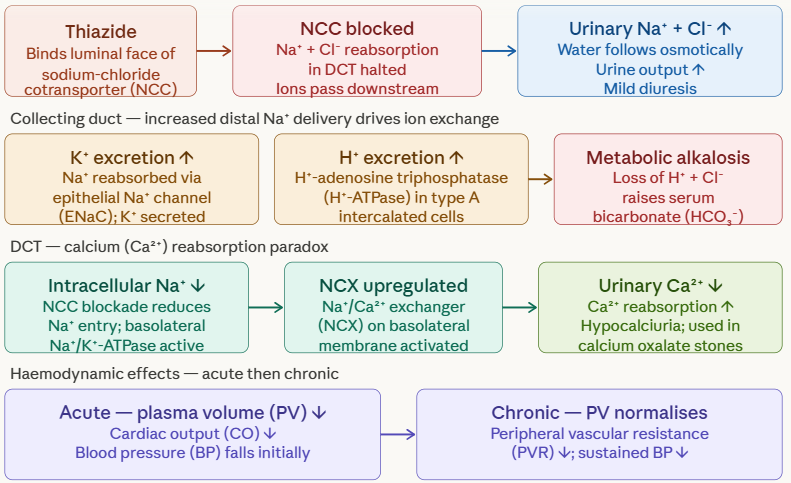
Mechanism of Action of Hydrochlorothiazide
Contributed by Preeti Patel, PharmD
References
Ernst ME, Fravel MA. Thiazide and the Thiazide-Like Diuretics: Review of Hydrochlorothiazide, Chlorthalidone, and Indapamide. American journal of hypertension. 2022 Jul 1:35(7):573-586. doi: 10.1093/ajh/hpac048. Epub [PubMed PMID: 35404993]
Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, DePalma SM, Gidding S, Jamerson KA, Jones DW, MacLaughlin EJ, Muntner P, Ovbiagele B, Smith SC Jr, Spencer CC, Stafford RS, Taler SJ, Thomas RJ, Williams KA Sr, Williamson JD, Wright JT Jr. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension (Dallas, Tex. : 1979). 2018 Jun:71(6):e13-e115. doi: 10.1161/HYP.0000000000000065. Epub 2017 Nov 13 [PubMed PMID: 29133356]
Level 1 (high-level) evidenceHOLLANDER W, WILKINS RW. Chlorothiazide: a new type of drug for the treatment of arterial hypertension. BMQ; the Boston medical quarterly. 1957 Sep:8(3):69-75 [PubMed PMID: 13471453]
Ojji DB, Mayosi B, Francis V, Badri M, Cornelius V, Smythe W, Kramer N, Barasa F, Damasceno A, Dzudie A, Jones E, Mondo C, Ogah O, Ogola E, Sani MU, Shedul GL, Shedul G, Rayner B, Okpechi IG, Sliwa K, Poulter N, CREOLE Study Investigators. Comparison of Dual Therapies for Lowering Blood Pressure in Black Africans. The New England journal of medicine. 2019 Jun 20:380(25):2429-2439. doi: 10.1056/NEJMoa1901113. Epub 2019 Mar 18 [PubMed PMID: 30883050]
Sica DA, Carter B, Cushman W, Hamm L. Thiazide and loop diuretics. Journal of clinical hypertension (Greenwich, Conn.). 2011 Sep:13(9):639-43. doi: 10.1111/j.1751-7176.2011.00512.x. Epub 2011 Jul 27 [PubMed PMID: 21896142]
Writing Committee Members*, Jones DW, Ferdinand KC, Taler SJ, Johnson HM, Shimbo D, Abdalla M, Altieri MM, Bansal N, Bello NA, Bress AP, Carter J, Cohen JB, Collins KJ, Commodore-Mensah Y, Davis LL, Egan B, Khan SS, Lloyd-Jones DM, Melnyk BM, Mistry EA, Ogunniyi MO, Schott SL, Smith SC Jr, Talbot AW, Vongpatanasin W, Watson KE, Whelton PK, Williamson JD. 2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2025 Sep 16:152(11):e114-e218. doi: 10.1161/CIR.0000000000001356. Epub 2025 Aug 14 [PubMed PMID: 40811497]
Level 1 (high-level) evidenceMa L, Zheng K, Yan J, Cheng W. Efficacy of ARB/HCTZ Combination Therapy in Uncontrolled Hypertensive Patients Compared with ARB Monotherapy: A Meta-Analysis. International journal of hypertension. 2021:2021():6670183. doi: 10.1155/2021/6670183. Epub 2021 Apr 27 [PubMed PMID: 33996152]
Level 1 (high-level) evidenceGong H, Li Y, Zheng C, Du TT, Luo BQ, Pang M. Modulatory effects of hydrochlorothiazide and triamterene on resistant hypertension patients. Experimental and therapeutic medicine. 2017 Jun:13(6):3217-3222. doi: 10.3892/etm.2017.4412. Epub 2017 Apr 28 [PubMed PMID: 28588673]
Dhayat NA, Bonny O, Roth B, Christe A, Ritter A, Mohebbi N, Faller N, Pellegrini L, Bedino G, Venzin RM, Grosse P, Hüsler C, Koneth I, Bucher C, Del Giorno R, Gabutti L, Mayr M, Odermatt U, Buchkremer F, Ernandez T, Stoermann-Chopard C, Teta D, Vogt B, Roumet M, Tamò L, Cereghetti GM, Trelle S, Fuster DG. Hydrochlorothiazide and Prevention of Kidney-Stone Recurrence. The New England journal of medicine. 2023 Mar 2:388(9):781-791. doi: 10.1056/NEJMoa2209275. Epub [PubMed PMID: 36856614]
Kim GH, Lee JW, Oh YK, Chang HR, Joo KW, Na KY, Earm JH, Knepper MA, Han JS. Antidiuretic effect of hydrochlorothiazide in lithium-induced nephrogenic diabetes insipidus is associated with upregulation of aquaporin-2, Na-Cl co-transporter, and epithelial sodium channel. Journal of the American Society of Nephrology : JASN. 2004 Nov:15(11):2836-43 [PubMed PMID: 15504936]
Level 3 (low-level) evidenceEarley LE, Orloff J. THE MECHANISM OF ANTIDIURESIS ASSOCIATED WITH THE ADMINISTRATION OF HYDROCHLOROTHIAZIDE TO PATIENTS WITH VASOPRESSIN-RESISTANT DIABETES INSIPIDUS. The Journal of clinical investigation. 1962 Nov:41(11):1988-97 [PubMed PMID: 16695887]
Lee CL, Feng L. Transport and thiazide-inhibition mechanisms of the Na-Cl cotransporter: a structural perspective. Current opinion in nephrology and hypertension. 2025 Sep 1:34(5):440-449. doi: 10.1097/MNH.0000000000001099. Epub 2025 Jul 3 [PubMed PMID: 40575829]
Level 3 (low-level) evidenceHierholzer K, Wiederholt M. Some aspects of distal tubular solute and water transport. Kidney international. 1976 Feb:9(2):198-213 [PubMed PMID: 940262]
Level 3 (low-level) evidenceSubramanya AR, Ellison DH. Distal convoluted tubule. Clinical journal of the American Society of Nephrology : CJASN. 2014 Dec 5:9(12):2147-63. doi: 10.2215/CJN.05920613. Epub 2014 May 22 [PubMed PMID: 24855283]
Cheng L, Poulsen SB, Wu Q, Esteva-Font C, Olesen ETB, Peng L, Olde B, Leeb-Lundberg LMF, Pisitkun T, Rieg T, Dimke H, Fenton RA. Rapid Aldosterone-Mediated Signaling in the DCT Increases Activity of the Thiazide-Sensitive NaCl Cotransporter. Journal of the American Society of Nephrology : JASN. 2019 Aug:30(8):1454-1470. doi: 10.1681/ASN.2018101025. Epub 2019 Jun 28 [PubMed PMID: 31253651]
Yin J, Wagner DJ, Prasad B, Isoherranen N, Thummel KE, Wang J. Renal secretion of hydrochlorothiazide involves organic anion transporter 1/3, organic cation transporter 2, and multidrug and toxin extrusion protein 2-K. American journal of physiology. Renal physiology. 2019 Oct 1:317(4):F805-F814. doi: 10.1152/ajprenal.00141.2019. Epub 2019 Jul 19 [PubMed PMID: 31322418]
Rapoport RM, Soleimani M. Mechanism of Thiazide Diuretic Arterial Pressure Reduction: The Search Continues. Frontiers in pharmacology. 2019:10():815. doi: 10.3389/fphar.2019.00815. Epub 2019 Aug 27 [PubMed PMID: 31543812]
Duarte JD, Cooper-DeHoff RM. Mechanisms for blood pressure lowering and metabolic effects of thiazide and thiazide-like diuretics. Expert review of cardiovascular therapy. 2010 Jun:8(6):793-802. doi: 10.1586/erc.10.27. Epub [PubMed PMID: 20528637]
Level 3 (low-level) evidenceLee CL, Zhang J, Feng L. Molecular mechanisms of thiazide-like diuretics-mediated inhibition of the human Na-Cl cotransporter. Nature communications. 2025 Aug 20:16(1):7740. doi: 10.1038/s41467-025-62714-w. Epub 2025 Aug 20 [PubMed PMID: 40830368]
Beermann B, Groschinsky-Grind M. Pharmacokinetics of hydrochlorothiazide in man. European journal of clinical pharmacology. 1977 Dec 2:12(4):297-303 [PubMed PMID: 590315]
. Hydrochlorothiazide. Drugs and Lactation Database (LactMed®). 2006:(): [PubMed PMID: 30000024]
Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, Deswal A, Drazner MH, Dunlay SM, Evers LR, Fang JC, Fedson SE, Fonarow GC, Hayek SS, Hernandez AF, Khazanie P, Kittleson MM, Lee CS, Link MS, Milano CA, Nnacheta LC, Sandhu AT, Stevenson LW, Vardeny O, Vest AR, Yancy CW, ACC/AHA Joint Committee Members. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022 May 3:145(18):e895-e1032. doi: 10.1161/CIR.0000000000001063. Epub 2022 Apr 1 [PubMed PMID: 35363499]
Level 1 (high-level) evidenceVaz de Castro PAS, Bitencourt L, de Oliveira Campos JL, Fischer BL, Soares de Brito SBC, Soares BS, Drummond JB, Simões E Silva AC. Nephrogenic diabetes insipidus: a comprehensive overview. Journal of pediatric endocrinology & metabolism : JPEM. 2022 Apr 26:35(4):421-434. doi: 10.1515/jpem-2021-0566. Epub 2022 Feb 11 [PubMed PMID: 35146976]
Level 3 (low-level) evidenceArrabal-Martín M, González-Torres S, Cano-García MD, De Haro-Muñoz T, Abad-Menor F, Arrabal-Polo MÁ, Cózar-Olmo JM. Urine Calcium and Bone Mineral Density in Calcium Stone-Forming Patients Treated with Alendronate and Hydrochlorothiazide. Urologia internationalis. 2016:97(3):292-298 [PubMed PMID: 26800461]
Jamerson K, Weber MA, Bakris GL, Dahlöf B, Pitt B, Shi V, Hester A, Gupte J, Gatlin M, Velazquez EJ, ACCOMPLISH Trial Investigators. Benazepril plus amlodipine or hydrochlorothiazide for hypertension in high-risk patients. The New England journal of medicine. 2008 Dec 4:359(23):2417-28. doi: 10.1056/NEJMoa0806182. Epub [PubMed PMID: 19052124]
Level 1 (high-level) evidenceSinha AD, Agarwal R. Clinical Pharmacology of Antihypertensive Therapy for the Treatment of Hypertension in CKD. Clinical journal of the American Society of Nephrology : CJASN. 2019 May 7:14(5):757-764. doi: 10.2215/CJN.04330418. Epub 2018 Nov 13 [PubMed PMID: 30425103]
Huh W, Oh HY, Han JS, Jang IJ, Yim DS. Hydrochlorothiazide does not increase furosemide's effects in end-stage renal disease. Translational and clinical pharmacology. 2017 Mar:25(1):28-33. doi: 10.12793/tcp.2017.25.1.28. Epub 2017 Mar 15 [PubMed PMID: 32095456]
Countouris M, Mahmoud Z, Cohen JB, Crousillat D, Hameed AB, Harrington CM, Hauspurg A, Honigberg MC, Lewey J, Lindley K, McLaughlin MM, Sachdev N, Sarma A, Shapero K, Sinkey R, Tita A, Wong KE, Yang E, Cho L, Bello NA. Hypertension in Pregnancy and Postpartum: Current Standards and Opportunities to Improve Care. Circulation. 2025 Feb 18:151(7):490-507. doi: 10.1161/CIRCULATIONAHA.124.073302. Epub 2025 Feb 17 [PubMed PMID: 39960983]
American College of Obstetricians and Gynecologists' Committee on Practice Bulletins—Obstetrics. ACOG Practice Bulletin No. 203: Chronic Hypertension in Pregnancy. Obstetrics and gynecology. 2019 Jan:133(1):e26-e50. doi: 10.1097/AOG.0000000000003020. Epub [PubMed PMID: 30575676]
By the 2023 American Geriatrics Society Beers Criteria® Update Expert Panel. American Geriatrics Society 2023 updated AGS Beers Criteria® for potentially inappropriate medication use in older adults. Journal of the American Geriatrics Society. 2023 Jul:71(7):2052-2081. doi: 10.1111/jgs.18372. Epub 2023 May 4 [PubMed PMID: 37139824]
Palmer BF. Metabolic complications associated with use of diuretics. Seminars in nephrology. 2011 Nov:31(6):542-52. doi: 10.1016/j.semnephrol.2011.09.009. Epub [PubMed PMID: 22099511]
Zhang X, Zhao Q. Association of Thiazide-Type Diuretics With Glycemic Changes in Hypertensive Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Clinical Trials. Journal of clinical hypertension (Greenwich, Conn.). 2016 Apr:18(4):342-51. doi: 10.1111/jch.12679. Epub 2015 Sep 23 [PubMed PMID: 26395424]
Level 1 (high-level) evidenceChoi HK, Soriano LC, Zhang Y, Rodríguez LA. Antihypertensive drugs and risk of incident gout among patients with hypertension: population based case-control study. BMJ (Clinical research ed.). 2012 Jan 12:344():d8190. doi: 10.1136/bmj.d8190. Epub 2012 Jan 12 [PubMed PMID: 22240117]
Level 2 (mid-level) evidencePrice AL, Lingvay I, Szczepaniak EW, Wiebel J, Victor RG, Szczepaniak LS. The metabolic cost of lowering blood pressure with hydrochlorothiazide. Diabetology & metabolic syndrome. 2013 Jul 9:5(1):35. doi: 10.1186/1758-5996-5-35. Epub 2013 Jul 9 [PubMed PMID: 23837919]
Minakawa S, Matsuzaki Y, Hashimoto T, Ishii N, Koga H, Sawamura D, Akasaka E. Lichenoid Drug Eruption due to Telmisartan-Hydrochlorothiazide Combination Progressing to Bullous Pemphigoid: A Case Report. The Journal of dermatology. 2026 Jan:53(1):e65-e67. doi: 10.1111/1346-8138.70068. Epub 2025 Nov 24 [PubMed PMID: 41277794]
Level 3 (low-level) evidenceSullivan TJ. Cross-reactions among furosemide, hydrochlorothiazide, and sulfonamides. JAMA. 1991 Jan 2:265(1):120-1 [PubMed PMID: 1984112]
Chen SH, Karanjia R, Chevrier RL, Marshall DH. Bilateral acute angle closure glaucoma associated with hydrochlorothiazide-induced hyponatraemia. BMJ case reports. 2014 Dec 4:2014():. doi: 10.1136/bcr-2014-206690. Epub 2014 Dec 4 [PubMed PMID: 25477363]
Level 3 (low-level) evidenceRunyon BA, AASLD. Introduction to the revised American Association for the Study of Liver Diseases Practice Guideline management of adult patients with ascites due to cirrhosis 2012. Hepatology (Baltimore, Md.). 2013 Apr:57(4):1651-3. doi: 10.1002/hep.26359. Epub [PubMed PMID: 23463403]
Level 1 (high-level) evidenceHandler J. Lithium and antihypertensive medication: a potentially dangerous interaction. Journal of clinical hypertension (Greenwich, Conn.). 2009 Dec:11(12):738-42. doi: 10.1111/j.1751-7176.2009.00181.x. Epub [PubMed PMID: 20021532]
Finley PR. Drug Interactions with Lithium: An Update. Clinical pharmacokinetics. 2016 Aug:55(8):925-41. doi: 10.1007/s40262-016-0370-y. Epub [PubMed PMID: 26936045]
Moore N, Pollack C, Butkerait P. Adverse drug reactions and drug-drug interactions with over-the-counter NSAIDs. Therapeutics and clinical risk management. 2015:11():1061-75. doi: 10.2147/TCRM.S79135. Epub 2015 Jul 15 [PubMed PMID: 26203254]
Mifsud S, Montanaro G, Craus S, Mifsud EL, Gruppetta M. Thiazide diuretics and primary hyperparathyroidism. British journal of hospital medicine (London, England : 2005). 2023 Dec 2:84(12):1-8. doi: 10.12968/hmed.2023.0228. Epub 2023 Dec 20 [PubMed PMID: 38153014]
Jo W, Koh ES, Chung S. Therapeutic roles of thiazides and loop diuretics in blood pressure control and renal protection against chronic kidney disease. Clinical hypertension. 2023 May 15:29(1):14. doi: 10.1186/s40885-023-00238-5. Epub 2023 May 15 [PubMed PMID: 37183259]
Bornstein SR, Allolio B, Arlt W, Barthel A, Don-Wauchope A, Hammer GD, Husebye ES, Merke DP, Murad MH, Stratakis CA, Torpy DJ. Diagnosis and Treatment of Primary Adrenal Insufficiency: An Endocrine Society Clinical Practice Guideline. The Journal of clinical endocrinology and metabolism. 2016 Feb:101(2):364-89. doi: 10.1210/jc.2015-1710. Epub 2016 Jan 13 [PubMed PMID: 26760044]
Level 1 (high-level) evidenceRouette J, Yin H, Pottegård A, Nirantharakumar K, Azoulay L. Use of Hydrochlorothiazide and Risk of Melanoma and Nonmelanoma Skin Cancer. Drug safety. 2021 Feb:44(2):245-254. doi: 10.1007/s40264-020-01015-1. Epub 2020 Oct 26 [PubMed PMID: 33104975]
Asante R, Yao Z, Dzaye O, Berning P, Jelwan Y, Burka S, Blumenthal RS, Blaha MJ. Prescription Trends of Hydrochlorothiazide vs. Chlorthalidone in the United States (2019-2024). American journal of hypertension. 2026 Mar 1:39(3):459-465. doi: 10.1093/ajh/hpaf190. Epub [PubMed PMID: 40985615]
Kappelin J, Ahnlide I, Christensen GB, Ingvar Å, Nielsen K. Antihypertensive Medication as a Risk Factor For Basal Cell Carcinoma: A Nationwide Registry-based Case-control Study. Acta dermato-venereologica. 2025 Sep 23:105():adv42749. doi: 10.2340/actadv.v105.42749. Epub 2025 Sep 23 [PubMed PMID: 40985575]
Level 2 (mid-level) evidenceVouri SM, van Tuyl JS, Olsen MA, Xian H, Schootman M. An evaluation of a potential calcium channel blocker-lower-extremity edema-loop diuretic prescribing cascade. Journal of the American Pharmacists Association : JAPhA. 2018 Sep-Oct:58(5):534-539.e4. doi: 10.1016/j.japh.2018.06.014. Epub 2018 Jul 20 [PubMed PMID: 30033126]
Bargagli M, Trelle S, Bonny O, Fuster DG. Thiazides for kidney stone recurrence prevention. Current opinion in nephrology and hypertension. 2024 Jul 1:33(4):427-432. doi: 10.1097/MNH.0000000000000990. Epub 2024 Apr 12 [PubMed PMID: 38606682]
Level 3 (low-level) evidence. Thiazide Diuretics. LiverTox®: Clinical and Research Information on Drug-Induced Liver Injury. 2012:(): [PubMed PMID: 31643991]
Pedersen SA, Gaist D, Schmidt SAJ, Hölmich LR, Friis S, Pottegård A. Hydrochlorothiazide use and risk of nonmelanoma skin cancer: A nationwide case-control study from Denmark. Journal of the American Academy of Dermatology. 2018 Apr:78(4):673-681.e9. doi: 10.1016/j.jaad.2017.11.042. Epub 2017 Dec 4 [PubMed PMID: 29217346]
Level 2 (mid-level) evidencePottegård A, Hallas J, Olesen M, Svendsen MT, Habel LA, Friedman GD, Friis S. Hydrochlorothiazide use is strongly associated with risk of lip cancer. Journal of internal medicine. 2017 Oct:282(4):322-331. doi: 10.1111/joim.12629. Epub 2017 Jun 6 [PubMed PMID: 28480532]
Hohl M, Götzinger F, Jäger S, Wagmann L, Tokcan M, Tschernig T, Reichrath J, Federspiel JM, Boor P, Meyer MR, Mahfoud F, Böhm M. Assessing phototoxic drug properties of hydrochlorothiazide using human skin biopsies. Communications biology. 2025 May 6:8(1):705. doi: 10.1038/s42003-025-08064-1. Epub 2025 May 6 [PubMed PMID: 40328921]
Klhůfek J, Vodička M, Ponížil P, Ryšavý I, Fojtík P, Kojecký V, Šálek T. Thiazide-Associated Hyponatremia: A Retrospective Cohort Study Comparing Hydrochlorothiazide Versus Indapamide Versus Chlorthalidone. Journal of clinical hypertension (Greenwich, Conn.). 2025 May:27(5):e70060. doi: 10.1111/jch.70060. Epub [PubMed PMID: 40346873]
Level 2 (mid-level) evidenceChen EJ, Hayrapetian L, Frishe K. A Rare Case of Pulmonary Edema Secondary to Hydrochlorothiazide Use. Case reports in critical care. 2024:2024():9423545. doi: 10.1155/2024/9423545. Epub 2024 Nov 7 [PubMed PMID: 39544450]
Level 3 (low-level) evidenceMatzke CM, DeGennaro R, Howie-Esquivel J. Incorporating TeamSTEPPS training to improve staff collaboration in an academic level I emergency and trauma center. International emergency nursing. 2021 Mar:55():100959. doi: 10.1016/j.ienj.2020.100959. Epub 2021 Feb 1 [PubMed PMID: 33540238]
Novak JE, Ellison DH. Diuretics in States of Volume Overload: Core Curriculum 2022. American journal of kidney diseases : the official journal of the National Kidney Foundation. 2022 Aug:80(2):264-276. doi: 10.1053/j.ajkd.2021.09.029. Epub 2022 Feb 19 [PubMed PMID: 35190215]
Ishani A, Cushman WC, Leatherman SM. Chlorthalidone vs. Hydrochlorothiazide for Hypertension-Cardiovascular Events. Reply. The New England journal of medicine. 2023 Apr 6:388(14):1342. doi: 10.1056/NEJMc2301922. Epub [PubMed PMID: 37018506]